
Abstract
In this regard, the main goal of the current research was to determine the effect of educational intervention based on the protection motivation theory on the promotion of preventive behaviors against brucellosis among ranchers of Khodabandeh city through health care providers. This quasi -experimental study was conducted in two groups of intervention and control in the before, immediately and 2 months after intervention. A total of 126 ranchers were investigated with the multi-stage sampling method and were included in two control (n = 64) and intervention groups (n = 62). The standard motivational theory questionnaire was used to collect data. The data collected in SPSS-22 software was analyzed using the independent sample t-test, Mann–Whitney and Friedman test. The results in the intervention group showed a significant difference in the general knowledge score during the three stages before, immediately, and 2 months after the intervention (P = 0.007). The results in the intervention group showed a significant difference in perceived susceptibility, perceived severity, perceived self-efficacy, response efficacy, perceived reward, fear, protection motivation, perceived response cost and preventive behavior during the three stages before, immediately, and 2 months after the intervention (P < 0.001). The results indicate the high impact of education by the area and the importance of paying attention to the culture and customs of the areas in education. Also, given the stability of the effects in most cases, it can be of interest to experts.
Similar content being viewed by others

Introduction
Brucellosis is one of the most common zoonotic diseases of humans around the world1. According to the World Health Organization data, there are about 50 human brucellosis reports in the world2. Brucellosis is a job disease and is most commonly found in ranchers, farmers, veterinarians and slaughterhouse workers who deal with their contaminated animals or tissues3. The cause of the disease is brucella, which is one of the obligate parasites of animals and humans4. In humans, and especially in children, it can cause complications such as meningitis, endocarditis, nephritis and pan-cytopenia5. Also, it is more common among men and those who use non -pasteurized dairy products3.
The prevalence of the disease varies from country to country and is more prevalent in countries around the Mediterranean (South Europe, North and East Africa), Middle East, India, and Central Asia6. The prevalence of disease in countries such as Australia and Canada is rare. However developing countries such as Syria and Iran classified as high prevalence countries7. The disease is scattered throughout all parts of Iran, and the highest prevalence of the disease is in the Zanjan, Hamedan, Markazi and East Azerbaijan provinces (98–130 per hundred thousand)4.
The most common way to transmit brucella is through the consumption of raw milk and unpasteurized dairy products, fresh meat, and raw liver. It is also possible to transmit the disease by contact with the placenta and aborted fetus of animals. Since early diagnosis and treatment of the disease does not have much effect on the control of the disease, the importance of prevention and teaching people to control the disease has been highly emphasized8. Evidence showed that the prevalence of the disease can be prevented by providing the necessary training to those at risk1. Although the prevalence of disease in humans is reduced by vaccination and reduced disease in ranchers, preventive behaviors are one of the most important factors in protecting human health7,9.
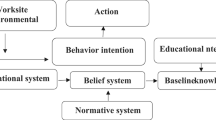
In numerous studies, the impact of health education on awareness in various fields, especially healthy behaviors, has been proven. To have effective and scientific evidence-based interventions, it is necessary to plan and implement educational programs based on the theories that have been proven9,10,11,12,13,14. In this regard, some studies recommended that interventions must have a motivational component15. A theory used to examine the factors affecting motivation and ultimately one’s behavior is the protection motivation theory (PMT). This theory was developed in 1975 by Rogers to explain the effects of fear of health risk on health attitudes and behaviors and whether the arousal of fear has an important effect on choosing behaviors. In this theory, it is assumed that accepting the recommended health behavior against a health risk can be considered as a motivational concept to behavior changing intentions. Based on this theory three factor can shape behavior protection motivation: (1) Threat appraisal that is both the Perceived severity and susceptibility of the situation that can change possibility of adopting maladaptive behaviors, (2) Coping appraisal that contain the response efficacy (the confidence that the educated action is effective in reducing the threat), self-efficacy (the belief that one can successfully adopt the recommended actions, and the response costs (are the expenses of the endorsed behavior), and (3) Fear that is a motivational power determined by perceived threats16 (Fig. 1).
Also, given the community’s trust in health care providers and their important role in promoting community health, this group can properly promote preventive behaviors. Accordingly, this study aimed to determine the effectiveness of an educational intervention based on the PMT in promoting brucellosis preventive behaviors in ranchers of Khodabandeh city (Zanjan province, Iran).

Protection motivation theory diagram.
Methods
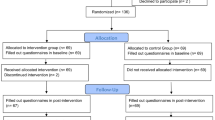
This semi-experimental study was designed with the intervention and control groups. The studied persons were selected using the multi-stage sampling method. In this way, in the first stage, 3 centers of 25 Khodabandeh city comprehensive rural health service centers were selected. In the second stage, 2 villages were randomly selected from each center (6 villages in total), and in the third stage, one village was randomly selected as the control group and one village was randomly selected as the intervention group. Finally, the samples of qualified ranchers were selected from each village.
According to the results of a similar study4 and taking into account the confidence interval of 95% and the power of 90%, the sample size was calculated as 59 persons in each group and increased to 64 persons with a 10% drop rate. The inclusion criteria were being a rancher, not having brucellosis, and having at least minimal literacy. The study exclusion criteria were absence of more than one session in the educational phase and unwillingness to continue participating in the study. Data were collected before, immediately, and 2 months after the educational intervention in both the intervention and control groups.
In order to collect data, the validated questionnaire of the PMT was used17. The first part of the questionnaire was the demographic variables. The second part included questions related to knowledge, which consists of 5 questions related to the knowledge of the general causes and symptoms of the brucellosis, 8 questions about the knowledge of the brucellosis transmission, and 7 questions about the ways of prevention and treatment of brucellosis (each correct answer scored 2 points, don’t knowing the answer also negative answer scored 1 and 0 point respectively). The maximum score in this section was 20 and 0 points is considered the minimum). The third part of the questionnaire included; 66 items to measure 9 constructs of PMT. Which contained the perceived susceptibility construct with 6 items, perceived severity 6 items, perceived self-efficacy 7 items, response efficacy 7 items, perceived reward 7 items, fear construct 5 items, protection motivation 10 items, perceived response 9 items. The questions related to the constructs were measured using a five-point Likert scale from completely agree (score 5) to completely disagree (score 1). Also, 9 questions related to the construct of preventive behavior were measured with a four-choice scale: always (score 4), most of the time (score 3), sometimes (score 2), and never (score 1). The maximum and the minimum score of this section were 321 and 66 score, respectively. The validity of this questionnaire was determined by the content validity ratio of the questionnaire (0.62) and the content validity index 0.79. To determine the reliability of the questionnaire, the test-retest method and Cronbach’s alpha were used. For this purpose, the questionnaire was completed by 15 members of the target population at a time interval of 10 days, and the results showed a correlation of over 70%. Also, the internal reliability of the questionnaire showed that all the constructs Cronbach’s alpha are more than 0.70.
The educational content of the study was prepared based on the constructs of the PMT. Educational intervention was provided to ranchers through health care providers who’s oriented by the research team. The educational intervention program was implemented in 7 sessions that took 45 min for 5 weeks. Lectures, brainstorming and forum method were used in the educational sessions. Also 6 educational clips were made based on PMT in the local language and in accordance with the cultural customs of the region. A summary of the educational activity is presented in Table 1. In order to comply with ethical points, after ending the study, the educational intervention was implemented for the control group. Data analysis was done using SPSS 22 software using Chi Square test, independent sample t-test, Mann–Whitney test, and Friedman test.
Results
In this quasi -experimental study, 126 ranchers were present, and the mean (± standard deviation) age in the intervention and control groups was 44.74 (± 12.01) and 42.45 (± 13.28), respectively, and based on the results of independent sample t-test the two groups were homogeneous in terms of age (p = 0.313). Also, based on the Chi Square test in Table 2, there was no significant difference between the two groups before the intervention in term of demographic characteristics (P > 0.05).
According to the Table 3, there was no significant difference between the two groups before the intervention (P > 0.05) in most constructs of the PMT (except knowledge of the prevention methods and perceived severity), but immediately after the intervention and 2 months later, the score difference between the two groups in all variables were significant (P < 0.05).
In the intervention group, the results obtained from the Friedman test showed a significant difference in the scores of the constructs of the PMT (except for two constructs) during the three periods before, immediately and 2 months after the intervention, and the score in this group compared to before the intervention had increased (P < 0.05). The score of perceived cost-response constructs and perceived reward in this group had decreased compared to before the intervention (P < 0.05).
In the control group, the score of the constructs of the PMT, immediately after of the intervention and 2 months later had significantly decreased compared to before the intervention (P < 0.05), except the score of the constructs Perceived cost-response and perceived reward increased compared to before the intervention (P < 0.05).
Discussion
Because of brucellosis importance, it is essential to investigate the factors related to the transmission of this disease and provide solutions for its prevention. These measures can help reduce the spread of disease and maintain the health of animals and humans. This study was conducted to determine the effect of education based on the theory of protected motivation on the promotion of preventive behaviors against brucellosis in Khodabandeh city ranchers using health care providers.
The results of the present study showed that after the implementation of the educational intervention, there was a significant difference in the knowledge about the general aspects of human brucellosis between the two groups. Also, after the implementation of the educational program, the awareness of ranchers about the ways of brucellosis transmission increased, and this difference was also significant. The results of Ramezankhani et al.‘s study4 showed that educational programs could significantly increase the level of awareness about Malaria disease in the intervention group compared to the control group. Which is consistent with the results of the present study. The results of the semi-experimental study by Allahverdipour18 and colleagues showed that the educational program was able to significantly improve the level of awareness about brucellosis in the intervention group, compared to the control group, which is in line with the results of this study. Therefore, it can be claimed that the implementation of the educational program can lead to an increase in people’s awareness of brucellosis and the importance of knowledge and prevention in disease control will be revealed.
It was observed that after the implementation of the educational intervention, there was a significant difference in the perceived susceptibility score between the two Intervention and control groups. Also, study results showed that the perceived severity constructs in the intervention group increased significantly immediately and 2 months after the intervention19. The study of Khosravi et al.20 and Khazaian study et al.21 showed that an increase in perceived susceptibility can lead ranchers to imagine the fact that they are at risk of contracting brucellosis and then adopt preventive behaviors.
There was a significant difference in the perceived severity scores between the intervention and control groups at different phases of data collection. Then, using the PMT can be effective for increasing the perceived severity of the brucellosis. The study of Farzadmehr et al., also showed that after the implementation of the educational intervention, the mean scores of perceived severity in the intervention group increased significantly compared to the control group22. Also, results a study showed that implementation of the educational intervention increased the perceived severity between the intervention and the control group1. In general, education can increase the severity perceived by ranchers and improve understanding of the risk of brucellosis, leading to the reduction of risky behaviors.
It was observed that there was no significant difference in self-efficacy between the two groups before the intervention, but after the intervention and 2 months later, the difference between the two groups was significant. Self-efficacy is one of the most important constructs of PMT, which was investigated based on this study. The results of this research showed that emphasizing self-efficacy can have a positive effect on a person’s final behavior, and increasing confidence in people’s ability to use protective behaviors increases the likelihood of their compliance. In addition, other studies have shown that educational programs based on self-efficacy can improve people’s confidence in their abilities and increase disease prevention behavior1,19.
There was no significant difference in the response efficiency scores between the two groups before the intervention, but after the implementation of the intervention and 2 months later, a significant difference was observed between the two groups. Response efficacy refers to a person’s expectation that adaptive responses and protective behaviors against a health hazard can eliminate the hazard. According to the research findings of Matlabi et al., after an educational intervention based on response efficiency, performing preventive behaviors against Corona significantly increased23. This finding is in agreement with the results of other studies that show that the response efficiency increased after the intervention. However, some studies have shown that there was no statistical difference in the mean response efficiency scores between the intervention and control groups, which may be due to the short duration of the intervention to change the attitude24,25. In general, education increases the adoption of protective behaviors by ranchers and increases the effectiveness of the response.
According to the findings, it was observed that there was no significant difference in the preventive behavior scores between the two groups before the intervention, but after the intervention and 2 months later, a significant difference was observed between the two groups. The results show that using the PMT can be effective for increasing preventive behaviors. Studies have shown that education as an effective factor can be effective in reducing diseases. This study also shows that the implementation of educational programs has increased preventive behaviors by ranchers.
According to the findings, it was observed that there was no significant difference in protection motivation between the two groups before the intervention, but after the implementation of the intervention and 2 months later, a significant difference between the two groups was clearly observed. According to the findings of Matlabi et al., the protection motivation scores increased after the implementation of the educational program in the intervention group. This may be due to the educational programs provided23. On the other hand, the results from Magai et al.‘s research showed that after the educational intervention based on this model, protection motivation in women increased significantly26, which is consistent with the findings of the present study and shows that education may have a positive effect on the motivation of ranchers.
Before the intervention, there was no significant difference in the perceived response cost between the two groups. However, after the intervention and after 2 months of follow-up, a significant difference was observed between the two groups. Based on studies, the higher the perceived response efficacy and self-efficacy and the lower the perceived response costs, the more likely the protective behaviors. In agreement with the findings of a study, the educational program significantly decreased the perceived response cost in the intervention group compared to the control group27. Helmes’ research also found that lower perceived response costs can increase the motivation to undergo genetic testing. These findings recommended that if people rationalize the costs associated with prevention behaviors, they are likely to perform these behaviors28.
According to the information, it was observed that there was no significant difference in the perceived reward between the two groups before the intervention, but after the implementation of the intervention and 2 months follow-up, a significant difference was observed between the two groups. As the study of Matlabi et al., this study showed, after the implementation of the educational program, the perceived reward decreased in the intervention group23. The lower the internal and external rewards of maladaptive behavior (lack of self-protection), can cause more likely to protective behaviors.
Regarding the construct of fear, it was observed that there was no significant difference in the scores of this construct between the two groups before the intervention, but after the implementation of the intervention and 2 months follow-up, a significant difference was observed between the groups. Fear acts through protection motivation and can influence health behaviors. The conformity of the results of this research with the reports of other studies26,29,30 shows that the increase in the mean score of fear after the implementation of the educational intervention indicates the positive relationship between education and the increase of fear and finally, the increase of protective behaviors. The analysis of the results of the present study concludes that raising the level of awareness and the constructs of the PMT through education may have positive effects in improving the preventive behaviors of brucellosis.
In present study confounding variables among ranchers affected the results as other studies that deal with this problem31,32, so in order to reducing this problem, after selecting the intervention group, an attempt was made to select the control group background variables in such a way that no significant difference was observed between two groups.
The most important limitation of this study was difficulty of objective observation of preventive behaviors that lead to using a self-report questionnaire. It suggests that future studies find more objective ways for measure preventive behaviors of brucellosis in ranchers.
Conclusions
The results of the present study showed the positive and significant effect of the educational intervention on the awareness and improvement of the preventive behaviors of brucellosis among the traditional ranchers in the rural areas of Khodabandeh city. This positive effect included improved perceived self-efficacy, decreased perceived response cost, and significant changes in perceived reward scores, fear construct, perceived sensitivity, and perceived severity. Therefore, the results confirmed that the PMT can be effective in improving the preventive behaviors of brucellosis in ranchers. In addition to the fact that this knowledge can be used in the development of effective interventions to improve preventive behaviors, it can facilitate the process of raising awareness and changing behavior in the rancher’s population.
Data availability
All data generated or analyzed during this study are included in this published article.
References
Babaei, V. et al. The effectiveness of an educational intervention based on the health belief model in the empowerment of stockbreeders against high-risk behaviors associated with brucellosis. J. Educ. Community Health. 1 (3), 12–19 (2014).
Taleski, V. et al. An overview of the epidemiology and epizootology of brucellosis in selected countries of central and Southeast Europe. Vet. Microbiol. 90 (1), 147–155 (2002).
Eskandari, Z., Bashirian, S., Barati, M., Soltanian, A. R. & Hazavehi, S. M. M. The effect of educational program based on the health belief model on brucellosis preventive behaviors among traditional ranchers in rural areas of Hamadan Province. J. Educ. Community Health. 3 (4), 16–23 (2017).
Ramezankhani, A., Jahani, H., Hatami, H., Sharifzadeh, G. H. & Hosseini, S. H. Determine the effect of intervention on the adoption of preventive behaviours of the brucellosis was based on the health belief model. nkums-journal 8 (1), 33–45 (2016).
Shahnavazi, M., Gholamreza, M., Ansari-Moghadam, A., Raeisy, D. & Varnamkhasti Khashei, F. Preventive behaviors of brucellosis in Khash City ranchers based on health belief model. Iran-J-Health-Educ-Health-Promot. ;4 (4):281–288. (2017).
Roushan, M. R. H., Baiani, M., Asnafi, N. & Saedi, F. Outcomes of 19 pregnant women with brucellosis in babol, Northern Iran. Trans. R. Soc. Trop. Med. Hyg. 105 (9), 540–542 (2011).
Pappas, G., Papadimitriou, P., Akritidis, N., Christou, L. & Tsianos, E. V. The new global map of human brucellosis. Lancet. Infect. Dis. 6 (2), 91–99 (2006).
Petkova, A. S., Zhelyazkov, C. B. & Kitov, B. D. Spontaneous Spondylodiscitis - Epidemiology, clinical features, diagnosis and treatment. Folia Med. (Plovdiv). 59 (3), 254–260 (2017).
Khunti, K. & Millar-Jones, D. Clinical inertia to insulin initiation and intensification in the UK: a focused literature review. Prim. Care Diabetes. 11 (1), 3–12 (2017).
Eshete, A., Mohammed, S., Deresse, T., Kifleyohans, T. & Assefa, Y. Association of stress management behavior and diabetic self-care practice among diabetes type II patients in North Shoa zone: a cross-sectional study. BMC Health Serv. Res. 23 (1), 767 (2023).
Paudel, G. et al. Self-care behaviours among people with type 2 diabetes mellitus in South asia: A systematic review and meta-analysis. J. Global Health ;12. (2022).
Kontoangelos, K. et al. Burnout Related To Diabetes Mellitus: a Critical Analysis18 (CP & EMH, 2022).
Kaveh, M. H., Layeghiasl, M., Nazari, M., Ghahremani, L. & Karimi, M. What are the determinants of a workplace health promotion? Application of a social marketing model in identifying determinants of physical activity in the workplace (a qualitative study). Front. Public. Health. 8, 614631 (2021).
Mobasheri, N., Ghahremani, L., Fallahzadeh Abarghooee, E. & Hassanzadeh, J. Lifestyle intervention for patients with nonalcoholic fatty liver disease: A randomized clinical trial based on the theory of planned behavior. Biomed. Res. Int. 2022 (1), 3465980 (2022).
Diao, D. Y. & Lee, T. K. Sun-protective behaviors in populations at high risk for skin cancer. Psychol. Res. Behav. Manage. :9–18. (2013).
Rogers, R. W. A protection motivation theory of fear appeals and attitude change1. J. Psychol. 91 (1), 93–114 (1975).
Hossein Abadi, S. S. et al. Effectiveness of educational intervention based on protection motivation theory to promotion of preventive behaviors from brucellosis among ranchers of farmer. J. Educ. Community Health. 8 (1), 11–19 (2021).
Allahverdipour, H. & Bashirian, S. Brucellosis prevention program: applying child to family health education method. Avicenna J. Clin. Med. 17 (1), 46–51 (2010).
Abadi, S. S. H. et al. Effectiveness of educational intervention based on protection motivation theory to promotion of preventive behaviors from brucellosis among ranchers of farmer. J. Educ. Community Health. 8 (1), 11–19 (2021).
Khosravi, V., Barati, M., Moeini, B. & Mohammadi, Y. The effect of an educational intervention based on protection motivation theory on prostate cancer prevention behaviors in men 50 to 75 years old. HAYAT 24 (4), 342–354 (2019).
Khazaeian, S., Sanavi, F. S., Ansari, H. & Mirshekari, F. Promotion of osteoporosis-preventive behaviors in adolescents: Application of protection motivation theory. J. Educ. Health Promotion. 10 (1), 469 (2021).
Farzadmehr, M., Ghorbani, M., Sadeghi, M. & Mosavi Bazzaz, S. The effect of education based on the health belief model in reducing the risk factors of the brucellosis in Torbat Haydariyeh. J. Torbat Heydariyeh Univ. Med. Sci. 6 (4), 47–56 (2019).
Matlabi, M., Esmaeili, R., Mohammadzadeh, F. & Hassanpour-Nejad, H. The effect of educational intervention based on the protection motivation theory in promotion of preventive behaviors against COVID-19. Health Syst. Res. 18 (1), 30–38 (2022).
Dehdari, T. et al. Effects of an educational intervention based on the protection motivation theory and implementation intentions on first and second pap test practice in Iran. Asian Pac. J. Cancer Prevention: APJCP. 15 (17), 7257–7261 (2014).
Ghahremani, L., Harami, Z. K., Kaveh, M. H. & Keshavarzi, S. Investigation of the role of training health volunteers in promoting pap smear test use among Iranian women based on the protection motivation theory. Asian Pac. J. Cancer Prev. 17 (3), 1157–1162 (2016).
Magai, C., Consedine, N., Conway, F., Neugut, A. & Culver, C. Diversity matters: Unique populations of women and breast cancer screening. Cancer: Interdisciplinary Int. J. Am. Cancer Soc. 100 (11), 2300–2307 (2004).
Khiyali, Z., Ghahremani, L., Kaveh, M. H. & Keshavarzi, S. The effect of an educational program based on protection motivation theory on pap smear screening behavior among women referring to health centers in Fasa. J. Educ. Community Health. 3 (4), 31–37 (2017).
Helmes, A. W. Application of the protection motivation theory to genetic testing for breast cancer risk. Prev. Med. 35 (5), 453–462 (2002).
Conner, M. & Norman, P. Predicting and Changing Health Behaviour: Research and Practice with Social Cognition Models (McGraw-hill education (UK), 2015).
Kunkel, E. J. et al. Behaviors used by men to protect themselves against prostate cancer. Cancer Epidemiol. Biomarkers Prev. 13 (1), 78–86 (2004).
Johnson, A. et al. Agricultural injuries among farmers and ranchers in the central united States during 2011–2015. J. Agromed. 26 (1), 62–72 (2021).
Carbonero, A. et al. Seroprevalence and risk factors associated with Brucella seropositivity in dairy and mixed cattle herds from Ecuador. Trop. Anim. Health Prod. 50 (1), 197–203 (2018).
Acknowledgements
We would like to thank the Social Development and Health Promotion Research Center, Gonabad University of Medical Sciences. We would like to thank all the people who assisted the authors in running this research project.
Funding
This study received financial support from the Social Development and Health Promotion Research Center, Gonabad University of Medical Sciences.
Author information
Authors and Affiliations
Contributions
H. R.: Design, Idea of research, Article writing. J.O.: Design, Idea of research. M.M.: Design of study, critical review. A.M.: Analyze, Article writing. A.J.: Design, Idea of research, Article writingAll authors have approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study is based on a research project approved by the Ethics Committee of Gonabad University of Medical Sciences with the code of ethics IR.GMU.REC.1402.092. All procedures performed in this study were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable. Written Informed Consent was obtained from all subjects.
Consent for publication
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Rohani, H., Osanloo, J., Moshki, M. et al. Effectiveness of educational intervention based on the protection motivation theory in promoting brucellosis preventive behaviors in ranchers. Sci Rep 15, 32334 (2025). https://doi.org/10.1038/s41598-025-17974-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-17974-3
