
Abstract
Burn injuries are severe traumas causing serious complications and high mortality. Managing burns is especially challenging in resource-limited settings. This study explores burn care challenges from the perspectives of both patients and healthcare providers. This qualitative descriptive study was conducted in Iran (2024–2025) with 41 hospitalized burn patients and healthcare providers, including physicians, nurses, psychologists, physiotherapists, and nutritionists. Participants were purposively sampled, and data were collected through semi-structured interviews until saturation. Data were analyzed concurrently using Graneheim and Lundman’s content analysis method with MAXQDA 2020 for data management. An inductive data analysis process revealed two main categories and nine subcategories. The categories identified were: “Structural and Professional Barriers in Burn Management” and “Challenges Related to Burn Patients and their Families”. Key structural barriers include inadequate interprofessional collaboration, limited resources and specialized expertise in non-specialized centers, insufficient burn care education in health profession curricula, and a lack of attention to burn injuries in health policy. Patient- and family-related challenges include cultural and economic factors, insufficient post-discharge follow-up, and low public awareness about burn injuries. This study highlights the multifaceted challenges in burn management from both healthcare providers’ and patients’ perspectives. Addressing these interconnected challenges requires comprehensive strategies encompassing healthcare system reforms, enhanced education and training, culturally sensitive care approaches, and supportive policies. Such efforts are essential to improve patient outcomes, reduce long-term complications, and alleviate the substantial burden of burn injuries on individuals and the healthcare system.
Similar content being viewed by others

Introduction
Burn injuries are among the most devastating and life-altering forms of trauma, often resulting in complex clinical scenarios that demand immediate and sustained multidisciplinary intervention. These injuries impact virtually all organ systems, leading to a wide range of acute and chronic complications, including infections, fluid and electrolyte imbalances, respiratory distress, and systemic inflammatory responses, which collectively contribute to high rates of morbidity and mortality1,2. According to estimates by the World Health Organization (WHO), approximately 180,000 people lose their lives to burn injuries each year, with the actual burden likely being underestimated due to underreporting in many regions3. Burns are characterized as damage to the skin and underlying tissues caused by exposure to thermal, chemical, electrical, or radiation sources. The severity of the injury depends on various factors, including the depth, extent, and location of the burn, as well as the patient’s age and comorbid conditions4.
Beyond the physical damage, burn injuries are often accompanied by significant psychological trauma. Survivors frequently experience long-term mental health issues such as post-traumatic stress disorder (PTSD), anxiety, depression, and body image disturbances, all of which contribute to a diminished quality of life and hinder rehabilitation and reintegration5. Moreover, the burden of care extends to the patient’s family, who often endure emotional, social, and economic hardship, especially in prolonged treatment and recovery scenarios6. These cascading effects place considerable strain not only on the patient and their support system but also on national healthcare infrastructures, particularly in countries where resources are limited7.
Burn injuries are widely acknowledged as a form of complex trauma that necessitates a highly coordinated, interprofessional approach to treatment and rehabilitation8. The intricate interplay between the physical, psychological, social, and economic dimensions of burn care highlights the importance of teamwork among physicians, nurses, psychologists, physiotherapists, nutritionists, and social workers9,10. The primary objectives in managing burn injuries include improving the quality and safety of care, reducing mortality and disability, preventing complications, and ultimately enabling patients to return to a functional life within their families and communities11. Although major advancements in burn treatment—such as early excision and grafting, improved wound care protocols, and enhanced nutritional and psychological support—have led to substantial reductions in mortality rates, burn patients and their caregivers continue to face a wide range of persistent and emerging challenges throughout the care continuum12,13. Addressing these challenges effectively requires sustained attention, innovation, and policy development across healthcare systems at both national and international levels14.
Importantly, the burden of burn injuries is not confined to any single geographic or economic region. While burn injuries pose serious challenges in both developed and developing countries, the incidence and outcomes are disproportionately worse in low- and middle-income countries (LMICs), where access to timely and effective burn care remains limited15,16. In such contexts, lack of specialized facilities, insufficiently trained personnel, inadequate infection control, and poor access to rehabilitation services are among the many barriers that exacerbate patient outcomes17. Despite the fact that more than 90% of global burn injuries occur in LMICs18, the majority of scholarly research and policy initiatives to date have focused on high-income settings19,20. This disparity has led to significant knowledge and practice gaps, which in turn hinder the development of contextually appropriate strategies for burn prevention, treatment, and long-term care in resource-constrained environments.
In light of this critical need, the present study was conducted in Iran, a developing country classified as lower-middle-income according to World Bank criteria, with the aim of exploring the real-world challenges of burn care management. Despite these advancements, there remains a paucity of qualitative research exploring the lived experiences of burn patients and healthcare providers to better understand these challenges and identify context-specific solutions21. By capturing the lived experiences and perspectives of both healthcare providers and burn patients across different stages of the treatment process during the years 2024–2025, this research seeks to generate locally relevant insights that can inform future clinical practices, training programs, and health policy reforms aimed at improving burn care outcomes in similar socio-economic contexts.
Methods
Design
This descriptive qualitative study was conducted from 2024 to 2025 at Imam Mousa Kazem (AS) Hospital in Isfahan Province, Iran—a major referral center for burn patients in central and southern Iran with 120 beds and monthly admissions of 70–80 patients. The study was approved by the Ethics Committee of Isfahan University of Medical Sciences (Ethical Code: IR.MUI.NUREMA.REC.1403.124). All participants provided informed written and verbal consent prior to participation, including permission to record the interviews. Interviews adhered to ethical guidelines ensuring participants’ privacy and confidentiality. Numeric codes were used in place of personal names to secure confidentiality, and all data—including names, recordings, and transcripts—were kept strictly confidential. All methods were performed in accordance with the relevant guidelines and regulations.
Participants
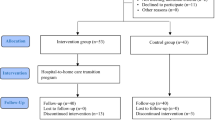
Using purposive sampling, the study included 18 hospitalized burn patients and 23 healthcare providers (physicians, nurses, psychologists, physiotherapists, nutritionists, and spiritual care providers). Burn patients were eligible if they: (1) were willing to participate, (2) were Iranian, (3) could understand and speak Persian, and (4) were currently hospitalized. Healthcare providers needed at least 2 years of burn unit experience and willingness to participate. Healthcare providers possessing extensive expertise and in-depth knowledge in burn care were purposively selected to ensure the provision of credible and comprehensive information. Burn patients were recruited following the principle of maximum variation, encompassing a wide range of ages, gender, diverse etiologies of injury, and burn surface areas ranging from 20 to 100%. Data collection continued until data saturation was achieved, defined as the point when no new themes emerged from the interviews22.
Data collection
Data were collected through individual semi-structured interviews conducted by the first author. Interview timing and location were arranged based on participant preferences. Healthcare provider interviews were typically held privately in their workrooms in Imam Mousa Kazem (AS) Hospital, while patient interviews took place in the hospital ward when participants were physically and mentally ready. Each interview lasted approximately 30–45 min. After a brief explanation of the study’s objectives, participants were invited to share their experiences and challenges related to burn care management. Interviews began with general questions to build rapport, such as: “Can you describe your experience with the treatment process from the time of injury until now?” and “What challenges have you faced during care and treatment?” Providers were also asked: “What is your experience as a burn care provider?” and “What challenges do you encounter in treating burn patients?” Probing questions like “Why?”, “How?”, and “Can you elaborate?” were used to deepen the responses (Supplementary file 1).
Data analysis
Data were analyzed using Graneheim and Lundman’s23 approach. Interviews were transcribed verbatim and reviewed for a shared understanding of participants’ perspectives. Meaning units—segments of text reflecting a single idea—were identified, condensed, and coded to represent abstract concepts. Through inductive analysis involving constant comparison and interpretation, similar codes were grouped into subcategories and broader categories, leading to the emergence of key themes (Fig. 1). MAXQDA 2020 was used to facilitate the analysis.

Data analysis process based on Graneheim and Lundman.
Trustworthiness
Trustworthiness was established using the criteria of confirmability, credibility, dependability, and transferability24. To ensure confirmability, all research steps were transparently documented to create an audit trail. Credibility was enhanced through peer review of data, codes, and categories, and member checking, where selected transcripts and codes were returned to participants for validation. Dependability was supported by collaboration between the first and second authors during analysis, along with review of coded samples by a qualitative research expert. To improve transferability, participants with diverse demographic backgrounds were included to ensure broader applicability of the findings. The quality appraisal of the study was conducted using the COREQ checklist (Supplementary file 2).
Results
This study is part of the results of a larger research project (Ph.D. Dissertation in Nursing). The age of burn patients ranged from 16 to 80 years (mean age: 37 years), with the total body surface area (TBSA) burned varying from 30 to 90%. The most common cause of burns was accidents, with flame burns being the predominant factor (Table 1). The age range of healthcare providers was 30–64 years (mean age: 46 years), with an average of 29 years of work experience (Table 2). Through the inductive data analysis process, two main categories and nine subcategories were identified (Table 3). The identified categories were “Structural and Professional Barriers in Burn Management” and “Challenges Related to Burn Patients and their Families”.
Structural and professional barriers in burn management
This category refers to the interconnected network of systemic and professional challenges that directly or indirectly limit the efficiency, timeliness, and quality of burn care. It reflects how the organization of services, allocation of resources, and professional preparedness influence treatment outcomes. Key issues include insufficient interprofessional and intraprofessional collaboration, which disrupts the continuity of care and creates delays in decision-making. There is also a shortage of specialized burn units and trained personnel, particularly in non-specialized centers, leading to uneven standards of care between urban and rural areas. Inadequate integration of burn-specific content into medical and nursing curricula results in healthcare providers entering practice without the skills needed for comprehensive burn care. Furthermore, the absence of clear national strategies and burn-specific policies at the health system level results in poor prioritization of burn care within the broader health agenda. Collectively, these barriers reveal a healthcare infrastructure that is reactive rather than proactive, lacking both the specialized capacity and coordinated teamwork essential for optimal burn injury management.
Poor interprofessional collaboration
Effective burn injury management requires ongoing collaboration among healthcare professionals, including physicians, nurses, physiotherapists, psychologists, and nutritionists. However, a lack of coordination and communication among these disciplines hinders the delivery of integrated care. Misalignment among providers complicates treatment, challenges teamwork, and can compromise the quality and efficiency of burn care:
… One of the biggest ongoing challenges we face is the lack of effective team communication in the hospital. This really impacts the quality of our work and ultimately harms the patient. (P 33)
Inappropriate delegation of physicians’ responsibilities to nurses can disrupt treatment and introduce legal risks. This issue increases nurses’ workload, raises the likelihood of errors, and compromises care quality. Additionally, it creates a disconnect between responsibilities and decision-making authority, undermining team efficiency and negatively affecting patient outcomes.One participant highlighted this concern, stating:
… According to standards, the physician is supposed to visit the patient before surgery, introduce themselves, and explain the procedure. Unfortunately, these duties are often assigned to nurses. Even the informed consent form, which should be completed and signed by the physician, is left to the nurse. The nurse already has a heavy workload and may be caring for multiple patients, including critical ones, and cannot always provide these explanations properly — this is a serious issue. (P 19)
Professional challenges affecting the quality of care
Structural and professional challenges within healthcare settings can undermine decision-making in burn patient care. Issues such as neglecting healthcare workers’ psychological well-being, insufficient rest, high burnout, low compensation, and an imbalance between workload and remuneration compromise the quality and continuity of care. The lack of institutional support for staff mental and physical health exacerbates fatigue, reducing the ability to deliver compassionate, effective care and negatively impacting patient outcomes. One participant raised these concerns, stating:
… Working in such an environment severely affects the mental health of the staff, and they can’t perform their duties the way they should. Personally, I became depressed from constantly hearing patients cry and scream in pain. On top of that, I developed persistent ear ringing. After seeing a specialist, I was told there was no physical problem with my hearing—it was due to stress and job-related anxiety. None of the treatments worked. This is clearly a result of the working conditions and the emotional toll of working in a burn center. (P 39)
Another significant professional challenge that critically impacts the quality of care is the low wages and the disproportionate workload faced by burn care providers. Participants consistently highlighted this issue as a primary concern:
…My salary is significantly low in relation to the demands of the work and the challenges inherent in this job. It drains all my energy, leading to a decrease in my work efficiency. I remind myself to work diligently for the sake of God for one month, but as time goes on, I lose the strength and motivation to maintain high performance. These issues are all interrelated. (P 21)
Lack of facilities and expertise in non-specialized centers
The initial hours following a burn injury are critical, and the availability of appropriate facilities and expertise in non-specialized burn centers can significantly mitigate the severity of complications. Participants reported that the absence of specialized skills and adequate facilities in these centers often leads to severe consequences for patients. These deficiencies not only delay treatment but also increase the likelihood of complications, ultimately compromising the patient’s quality of life. As one participant stated:
…When patients are transferred from rural areas or non-specialized centers, we face challenges such as thermal loss, leading to hypothermia. Additionally, a significant bacterial presence is often noted on the wound, as sterilization practices are not followed in rural areas, and a simple dry bandage is applied. Furthermore, fluid resuscitation is frequently inadequate, and by the time the patient arrives at a specialized facility, it is often too late for proper compensation. These are some of the gaps that exist. (P 27)
In many instances, burn patients are transferred to centers that lack the necessary facilities and expertise to manage such injuries promptly. The unpreparedness of non-specialized centers to receive and properly manage burn patients can lead to significant challenges and the loss of critical initial hours following the injury. This issue not only complicates the treatment process but also increases the likelihood of long-term complications. As one participant recounted:
…After the explosion at home, we quickly went to the nearest hospital in the city. We spent an hour or two going back and forth, but everywhere we went, they said it wasn’t their responsibility. I asked them to at least provide some pain relief until I could reach a hospital with a burn unit, but they told me it wasn’t their job and that I needed to go to a center with a burn department. Several hours were lost, and nothing was done for me. (P 8)
Lack of attention to burn education in health professions curricula
A significant challenge in burn care in low-income countries is the limited focus on specialized burn education within health professions curricula. The lack of comprehensive burn care training, particularly in medical and nursing programs, leaves healthcare professionals underprepared to address the unique challenges of treating burn patients. This educational gap directly impacts care quality, as insufficient knowledge and skills hinder effective treatment and management of burn injuries. As one participant pointed out:
…The biggest challenge right now is that only a few specific universities offer short-term training courses, such as two-week or one-month internships or clerkships for medical interns and residents. However, smaller universities either don’t offer burn courses, or they are inactive or non-educational, so students don’t become familiar with the subject. (P 30)
Furthermore, Inexperienced primary care providers without specialized burn care qualifications can significantly undermine burn patient treatment. Their difficulty in diagnosing, managing, and performing initial interventions often leads to delays or incorrect decisions, increasing the risk of complications and adverse outcomes. Continuous, specialized education for primary care providers is essential to ensure safe and effective burn care, preventing serious complications. As one participant noted:
…The first line of burn treatment is provided by staff working in health houses, health centers, and district hospitals, and the incorrect treatments they administer are disastrous. This is a direct result of neglect in providing specialized burn education. (P 28)
Insufficient attention to burns in health policy
The inadequate allocation of resources and lack of clear policies at the managerial and policy levels have resulted in neglecting burn patients’ needs and insufficient support for burn care. This deficiency can delay treatment and compromise care quality, as one participant noted:
…The Ministry of Health does not provide the attention that burn centers require, and it seems that the importance and priority of burn treatment and care are not well understood by health policymakers. (P 36)
Overcoming the fundamental challenges in burn management is achievable through the development and revision of policies at the policymaking level. One participant emphasized this point:
…Because our resources are very limited and the Ministry of Health does not provide adequate attention to this issue, we are forced to continue treatment using outdated methods. A reference book has defined the standard of care, but we are unable to implement the standard methods due to a lack of financial resources. (P 27)
Challenges related to burn patients and their families
This category encompasses the complex mix of financial, social, cultural, and psychological obstacles experienced by patients and their families during and after the treatment process. Burn care is not only medically intensive but also financially demanding, often placing a severe burden on households, especially those from lower-income backgrounds. Limited public awareness about appropriate burn first aid and modern treatment options means that many patients arrive at hospitals after receiving inadequate or harmful initial care. Cultural beliefs, language barriers, and social stigmas can further complicate interactions between patients and healthcare providers, sometimes reducing trust and adherence to medical advice. Post-discharge challenges, such as lack of structured follow-up and limited access to rehabilitation services, hinder recovery and increase the risk of complications like contractures, infections, and permanent disability. The emotional toll on families, including psychological stress, caregiver burnout, and social isolation, further exacerbates the recovery process. These challenges demonstrate that burn care extends far beyond the hospital setting, requiring sustained support systems, community-based education, and culturally sensitive approaches to care. This category includes four subcategories.
Financial limitations and the economic burden of burn treatment
Limited financial resources and the high cost of burn treatment significantly impede access to effective care, particularly in developing countries where many burn victims come from low-income backgrounds. Financial constraints often prevent patients from completing their treatment, leading to long-term complications. Burn survivors commonly face ongoing physical, psychological, and social challenges due to inadequate care, as one participant noted:
…One challenge we face in the hospital is the economic issue, which is one of our barriers. Since the costs are high and only a small portion is covered by insurance, patients, due to financial difficulties, do not follow up with their treatment. After a while, they face complications such as deformities and contractures. (P 40)
In this context, another participant shared:
…One issue that burn patients are particularly concerned about is the cost. For instance, the individual who suffers an injury often loses their job and comes to the hospital, now burdened with significant financial expenses. Although food is provided within the hospital, we still ask them to go outside to buy juice and other food items, which adds an additional financial strain on the patient. I recall one case where the father of a family, who was in poor financial condition, would sleep in his car outside the hospital so he could make kebabs and bring them to his hospitalized child. (P 19)
Cultural challenges and complexities in providing care
Given the cultural and social diversity of burn patients, providing quality care that accounts for these factors is a significant challenge. In the inpatient setting, patients from various cities, cultures, and social backgrounds have different needs and expectations, complicating communication and the delivery of care. Healthcare providers must effectively communicate with diverse patients to understand their individual needs and provide appropriate care. This requires specialized training in cultural sensitivity to improve care quality and treatment outcomes, as one participant noted:
…The problem we face with patients is with those who are culturally different. Communication with them is very difficult, especially with those with whom we have a language barrier. Providing care becomes very challenging until we, as service providers and patients, reach a common understanding and a shared language of communication. (P 38)
In this regard, one of the care providers in the burn emergency department shared:
…One of the challenges we face in the emergency department, which can significantly disrupt the treatment process, is that taking medical histories, performing initial assessments, inquiring about the details of the incident, and so on, is very slow, time-consuming, and even prone to errors when dealing with patients from different cultural and linguistic backgrounds. (P 24)
Discontinuation of post-discharge follow-up
Contrary to common belief, burn treatment extends beyond hospitalization into the crucial rehabilitation phase after discharge. This phase is essential for physical, psychological, and social recovery. A major challenge identified by nearly all healthcare providers was the discontinuation of post-discharge follow-up by patients and their families. This lack of follow-up can lead to complications, slower recovery, and prolonged rehabilitation. As many burn patients require long-term care, neglecting this phase can negatively impact their quality of life and increase the caregiving burden, as one participant explained:
…Because the cost of treating a burn patient can sometimes exceed that of treating cancer patients, and when we cannot provide complete treatment, surviving patients develop numerous complications that require multiple interventions after discharge, such as physical therapy, tissue release surgeries, and so on, to mitigate the severity of these complications. However, since patients are either unaware of the consequences of not following up, or in many cases come from distant cities, they completely abandon their post-discharge care. (P 27)
Low financial capacity and high costs associated with the post-discharge period significantly contribute to treatment discontinuation. Burn patients often require long-term medical care, physical therapy, psychotherapy, and other rehabilitation services, which can be financially burdensome. For many patients and their families, covering these costs is a challenge, leading to incomplete post-discharge care. This can result in long-term complications, decreased quality of life, increased caregiving burden, and higher healthcare costs, as one participant noted:
…In my opinion, one of the reasons patients do not continue their treatment after discharge is that our insurance systems do not provide adequate support for these patients, and many medications, dressings, and other expenses are charged privately. Most often, those affected by this issue come from the weaker sectors of society, who, due to their lower economic status, likely have lower job security. These costs prevent them from completing their treatment or following up as they should. (P 32)
Lack of awareness at various levels of burn prevention and treatment
This subcategory highlights the lack of awareness and knowledge among patients and their families throughout burn prevention, treatment, and rehabilitation, leading to inefficiencies in care. A key factor is the insufficient public education on burn prevention and treatment, exacerbated by the absence of media campaigns, cultural awareness initiatives, and health policy efforts. This lack of awareness often results in inadequate burn prevention, delays in treatment initiation, and poor rehabilitation management, as one participant pointed out:
…Another issue that I believe is greatly overlooked in society is the public’s lack of awareness about the risks associated with working with tools and materials. Many workers and people don’t know how safe the tool or material they are working with is, or how to protect themselves from it. Or, as I mentioned before, they don’t know how to respond to an injury in order to minimize harm. In general, there is a strong need for public awareness and education to prevent and reduce complications. (P 33)
The participants’ experiences revealed that, in addition to a lack of awareness, there was a prevalent misconception about burn injuries among patients and their families even before the incident occurred. Many believed that a burn injury was always minor and could be treated on an outpatient basis. One participant shared:
…When I got burned, I thought it wasn’t anything serious and that just a little skin was damaged, and with a simple dressing, it would heal. But now, I’ve been hospitalized for 28 days. I’ve had several surgeries, my body has become weak, I can’t walk, I can’t eat properly, I’ve developed digestive problems, breathing has become difficult, and many other issues. I never thought that one moment of injury could incapacitate me like this. (P 1)
Discussion
This study aimed to explore the challenges in burn management, focusing on both the perspectives of burn care providers and patients. Burn injuries necessitate complex and costly care, and if not properly managed, can lead to long-term complications, negative health outcomes, and substantial burdens on both families and the healthcare system. The experiences shared by participants in this study underscored the multifaceted nature of these challenges, which range from systemic issues within healthcare providers and the healthcare system to concerns within patients and their families. These findings highlight that burn care is not merely a technical or clinical process, but rather a multifactorial challenge influenced by organizational readiness, professional competency, socio-economic conditions, and cultural dynamics, all of which require an integrated and context-specific approach.
One of the key findings of the present study was the identification of structural and professional barriers in burn management. Participants noted the lack of coordination among different specialties and the insufficient interprofessional collaboration, which hinders the delivery of integrated, effective treatment for burn patients. Furthermore, professional issues among healthcare providers can lead to delays in treatment decisions and a failure to address the specific needs of burn patients. Ma et al.25 emphasize that burn care is a complex, interconnected process requiring communication, coordination, and joint decision-making among burn care specialists. To enhance care quality, attention must be directed toward overcoming both interprofessional and intraprofessional barriers25,26. Additionally, Butler27 highlights that modern burn care revolves around integrated, interprofessional care. The physical, psychological, and social needs of burn victims necessitate close collaboration among various healthcare professionals27. In light of the present findings, it becomes evident that such collaborative frameworks are often fragmented or absent in many healthcare settings, particularly in resource-limited environments. Strengthening communication channels and establishing structured interprofessional protocols could directly enhance treatment efficiency, reduce redundancy in care, and improve patient satisfaction. Indeed, interprofessional and intraprofessional challenges are fundamental barriers that significantly hinder effective care delivery. Identifying and analyzing these barriers at multiple levels can offer health policymakers crucial insights, enabling the development of effective strategies to improve healthcare quality and treatment outcomes. From a policy perspective, addressing these gaps demands not only professional training but also systemic reforms aimed at fostering a culture of collaboration across all levels of burn care.
Moreover, the study by Soltani Goki et al.28 on Iranian nurses’ perceptions of core competencies required for disaster risk management highlights the indispensable role of communication, teamwork, ethical responsibility, and psychological resilience among healthcare providers during complex emergencies, including burn injuries. This finding supports the current study’s results, emphasizing that systematic training in these core competencies not only improves provider preparedness but also fosters effective collaboration and ethical decision-making, which are critical for delivering high-quality burn care under pressure. The alignment between these competencies and the challenges identified in the present research reinforces the urgent need for embedding targeted interprofessional education programs into formal healthcare curricula and ongoing professional development initiatives.
Another significant challenge identified in this study is the lack of specialized facilities and expertise in non-specialized centers, which often leads to suboptimal treatment outcomes in burn injury management. Improper injury management and the use of unscientific or unreliable methods can exacerbate these issues. Collier et al.29 highlight that in Asia, the absence of access to safe, affordable surgery, a shortage of trained manpower, and limited specialized facilities are key barriers to effective burn care. This challenge is particularly acute in resource-limited countries. The situation in Iran mirrors this broader regional problem, where referral delays and the absence of specialized units in peripheral areas can significantly worsen patient prognosis. Investing in capacity-building for non-specialized centers—through telemedicine support, standardized treatment protocols, and targeted training—could bridge part of this gap while long-term infrastructural development is pursued. Equipping non-specialized centers with essential resources and enhancing specialized skills among healthcare providers are crucial steps in mitigating risks and improving treatment outcomes.
Another structural barrier to effective burn care is the insufficient emphasis on burn education within relevant training curricula. Allorto et al.30 observe that in South Africa, efforts to address burn education for specialists have been limited, and the training provided to healthcare providers has been inadequate for managing burn injuries effectively. The lack of burn care education in health professions curricula results in the preparation of doctors and nurses who are unqualified to provide adequate care for burn patients. This gap is particularly concerning in countries with high burn incidence rates, where the absence of structured education not only limits clinical competency but also perpetuates preventable complications and mortality. Revising educational programs to include practical, case-based burn management modules could significantly improve both acute and long-term patient outcomes. This lack of preparedness can have detrimental consequences for both the patient and the healthcare system.
The study also highlighted a lack of attention to resource allocation and the absence of specific policies at the managerial and policy-making levels for burn treatment and prevention. Despite the high incidence of burn injuries in resource-limited settings, burn-related issues are often overlooked in health policy-making. Barbosa et al.31 note that significant gaps in infrastructure, management, and policy-making hinder effective burn care and stress the need for greater attention from health policymakers. Addressing these challenges at the policy level is essential. Revisiting health and cultural policies at a macro level could improve care quality and lead to increased resource allocation, particularly for prevention initiatives. Such measures could reduce the incidence of burn injuries and improve treatment outcomes. Additionally, fostering cultural awareness and focusing on effective policies at the community level could significantly reduce burn injury rates and increase public awareness. The integration of burn prevention into broader public health strategies—similar to campaigns for road safety or tobacco cessation—could provide a sustainable framework for long-term impact, especially when coupled with community-driven initiatives.
One of the key sections of the present study explores “Challenges Related to Burn Patients and their Families”. The financial constraints faced by victims, coupled with the high costs associated with burn care and treatment, are regarded as some of the most significant challenges. Bayu32 emphasizes that, in addition to concerns about the injury itself, the financial burdens related to hospitalization impose additional pressure on both the patient and their family. Nearly all participants highlighted the substantial cost of treatment, indicating the importance of this issue. Many victims come from low-income backgrounds, which exacerbates the challenge of affording treatment. In such contexts, the absence of comprehensive health insurance coverage or government-subsidized burn care programs amplifies the inequity in access to treatment, creating a cycle where socio-economic status becomes a determinant of survival and recovery. Furthermore, cultural challenges arising from the diverse cultural and social backgrounds of burn patients complicate the provision of care by healthcare providers. In this regard, Coombs and colleagues33 note that linguistic and cultural differences between patients and healthcare providers create obstacles to delivering quality care. These findings underline the necessity of incorporating cultural competence training into healthcare systems, ensuring that professionals can navigate diverse patient backgrounds with sensitivity and efficacy.
Furthermore, the treatment of burn injuries extends beyond hospitalization, with a substantial portion of recovery occurring post-discharge. One major challenge identified by healthcare providers in this study is the lack of follow-up care after discharge. Burn patients and their families often struggle with adherence to post-discharge treatment plans, exacerbating long-term complications and hindering survivors’ ability to return to normal life34. This failure to follow up is often attributed to financial constraints and limited access to specialized burn care centers, undermining healthcare providers’ efforts and resulting in deformities, infections, and disabilities. Given the pivotal role of rehabilitation in functional recovery, establishing structured post-discharge care pathways—supported by community health workers and telehealth interventions—could substantially improve patient adherence and reduce preventable complications. This underscores the urgent need for financial support strategies and programs to assist burn patients during the post-discharge phase.
Another patient and family-related barrier is the widespread lack of adequate awareness and knowledge at all stages of burn prevention, treatment, and rehabilitation. Denekew et al.35 emphasize that many individuals still rely on unscientific traditional methods, such as applying pastes or oils to burn injuries, highlighting a significant public knowledge gap regarding proper burn care. Public education campaigns, particularly through mass media, alongside prioritizing burn-related policy-making, could serve as effective strategies to address these challenges. By integrating burn prevention messages into school curricula, workplace safety programs, and community workshops, such initiatives could achieve long-term behavioral change, reducing both the incidence and severity of burn injuries.
Future research should investigate the effects of interprofessional ethics education on collaboration and care quality in burn management. Additionally, studies exploring financial support models and culturally sensitive interventions to improve patient adherence and post-discharge outcomes are needed to enhance comprehensive burn care.
Strengths and limitations
This study explored the experiences healthcare providers involved in burn injury management and patients with burn, identifying various barriers and challenges. A key strength was its focus on firsthand accounts from those directly engaged in burn care, providing valuable insights into the complexities of the issue. However, a primary limitation was the physical and psychological condition of hospitalized burn patients, which could have affected data accuracy and reliability. To mitigate this potential bias, interviews were scheduled when patients’ conditions had stabilized, enhancing data quality and study credibility.
Conclusion
This study highlights the multifaceted challenges in burn management from both healthcare providers’ and patients’ perspectives. Structural and professional barriers—including inadequate interprofessional collaboration, lack of specialized resources, insufficient education, and limited policy attention—significantly hinder the delivery of high-quality burn care. Additionally, economic burdens, cultural complexities, discontinuity in post-discharge follow-up, and widespread lack of burn-related awareness among patients and families further complicate treatment outcomes. Addressing these interconnected challenges requires comprehensive strategies encompassing healthcare system reforms, enhanced education and training, culturally sensitive care approaches, and supportive policies. Such efforts are essential to improve patient outcomes, reduce long-term complications, and alleviate the substantial burden of burn injuries on individuals and the healthcare system.
Data availability
All data are available from the corresponding author upon reasonable request via email: Sedighehfarzi@nm.mui.ac.ir.
References
You, Z., Jain, S., Shen, S., Mao, J. & Martyn, J. J. Pathophysiology and management of burn injury-induced pain. Burns Open 10, 1–7 (2025).
Carey, M. G., Valcin, E. K., Lent, D. & White, M. Nursing care for the initial resuscitation of burn patients. Crit. Care Nurs. Clin. 33(3), 275–285 (2021).
Wang, Y. et al. Burn injury: Challenges and advances in burn wound healing, infection, pain and scarring. Adv. Drug Deliv. Rev. 123, 3–17 (2018).
Hamza Hermis, A. et al. RETRACTED: Prevalence of non-accidental burns and related factors in children: A systematic review and meta-analysis. Int. Wound J. 20(9), 3855–3870 (2023).
Zabihi, M. R., Rashtiani, S., Akhoondian, M. & Farzan, R. The role of nursing care in the management of post-burn epidermal cancer: A narrative review. J. Nurs. Rep. Clin. Pract. 2(3), 172–179 (2024).
Zare-Kaseb, A., Beigee, A. M., Doustahadi, A., Shahabi, M. & Ghazanfari, M. J. Social support against suicide in burn survivors: A vital but overlooked protective factor. J. Nurs. Rep. Clin. Pract. 2(1), 45–46 (2023).
Jeschke, M. G. et al. Burn injury. Nat. Rev. Dis. Primers 6(1), 11 (2020).
Rodrigues, M. A. C., Tanita, M. T., Alfaro, A. J. Y. & Grion, C. M. C. Patient care for burn victims in Brazil: A national survey. Burns 50(9), 1–9 (2024).
Costa, P. C. P. et al. Nursing care directed to burned patients: A scoping review. Rev. Bras. Enfermagem. 76, 1–8 (2023).
Caminati, G. et al. Emotional impact of clinical practice in Burns Unit among nursing students: A qualitative study. Acta Bio Med. Atenei Parmensis 92(Suppl 2), 1–8 (2021).
Kettering, C. E., Erpenbeck, S. P., Stofman, G. M., Ziembicki, J. A. & Egro, F. M. Interdisciplinary representation of burn surgery journal and society leadership. J. Burn Care Res. 42(3), 459–464 (2021).
Ray, D. E. et al. Care of the critically ill burn patient. An overview from the perspective of optimizing palliative care. Ann. Am. Thorac. Soc. 14(7), 1094–1102 (2017).
Griggs, C., Goverman, J., Bittner, E. & Levi, B. Sedation and pain management in burn patients. Clin. Plast. Surg. 44(3), 1–10 (2017).
Stapelberg, F. Challenges in anaesthesia and pain management for burn injuries. Anaesth. Intensive Care 48(2), 101–113 (2020).
Gerstl, J. V. et al. The global macroeconomic burden of burn injuries. Plast. Reconstr. Surg. 153, 743–752 (2023).
Hendriks, T. et al. Acute burn care in resource-limited settings: A cohort study on treatment and outcomes in a rural regional referral hospital in Tanzania. Burns 48(8), 1966–1979 (2022).
Hendriks, T. C. C. Think Global, Act Local: Burn Care in a Resource-Limited Setting, 1–268 (2021).
Sarbazi, E. et al. Epidemiology and the survival rate of burn-related injuries in Iran: A registry-based study. Ann. Burns Fire Disasters 32(1), 1–7 (2019).
Abubakar, A. I. & Sabo, V. Y. Modifying burn care in a low-and middle-income countries (LMIC) to meet global best practice: A burn unit or burn isolation ward?. Burns 50(9), 1–9 (2024).
Jordan, K. C., Di Gennaro, J. L., von Saint André-von Arnim, A. & Stewart, B. T. Global trends in pediatric burn injuries and care capacity from the World Health Organization Global Burn Registry. Front. Pediatr. 10, 1–9 (2022).
Flannery, E., Halcomb, E., Peters, K., Murphy, G. & Ramjan, L. M. The experiences of ‘significant others’ supporting people with severe burn injury: An integrative literature review. Aust. Crit. Care 35(3), 321–329 (2022).
Guest, G., Bunce, A. & Johnson, L. How many interviews are enough? An experiment with data saturation and variability. Field Methods 18(1), 59–82 (2006).
Graneheim, U. H. & Lundman, B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today 24(2), 105–112 (2004).
Guba, E. G. Criteria for assessing the trustworthiness of naturalistic inquiries. Ectj 29(2), 75–91 (1981).
Ma, Y., Stewart, G., Chipp, E. & Bache, S. World burn care and the multidisciplinary team. Burns 51, 1–10 (2025).
Schoenbrunner, A., Banda, W. & Gosman, A. A. Global burn care: Education and research. Clin. Plast. Surg. 44(3), 485–493 (2017).
Butler, D. P. The 21st century burn care team. Burns 39(3), 375–379 (2013).
Soltani Goki, F., Farahmandnia, H., Sabzi, A., Taskiran Eskici, G. & Farokhzadian, J. Iranian nurses’ perceptions of core competencies required for disaster risk management. BMC Emerg. Med. 23(1), 84 (2023).
Collier, Z. J., McCool, K., Magee, W. P. III., Potokar, T. & Gillenwater, J. 58 Burn injuries in Asia: A global burden of disease study. J. Burn Care Res. 43(Supplement_1), 40–41 (2022).
Allorto, N. L. & Clarke, D. L. Merits and challenges in the development of a dedicated burn service at a regional hospital in South Africa. Burns 41(3), 454–461 (2015).
dos Santos, B. A. et al. Evolution and challenges in pre-hospital care for burn injury victims in Brazil. Res. Soc. Dev. 13(10), 1–10 (2024).
Bayuo, J. & Wong, F. K. Y. Issues and concerns of family members of burn patients: A scoping review. Burns 47(3), 503–524 (2021).
Coombs, N. C., Campbell, D. G. & Caringi, J. A qualitative study of rural healthcare providers’ views of social, cultural, and programmatic barriers to healthcare access. BMC Health Serv. Res. 22(1), 1–16 (2022).
Ahmadi, H., Attari, A. M. A., Ajoudani, F. & Lotfi, M. Family-based education and follow-up program for patients with burns: A mixed assessment study. Burns 50(6), 1671–1681 (2024).
Denekew, B. et al. Investigating burn cases, knowledge, attitudes and practices to burn care and prevention in Ethiopia: A community-survey. J. Glob. Health Rep. 5, 1–10 (2021).
Acknowledgements
The researchers would like to express their gratitude to the Vice Chancellor for Research of Isfahan University of Medical Sciences for the financial support of this study (Project Number: 3403448) and all participants.
Funding
This work was supported by the Vice Chancellor for Research of Isfahan University of Medical Sciences grant number 3403448.
Author information
Authors and Affiliations
Contributions
Hossein Ghasemi: Conceptualization, investigation, analysis, writing original draft. Sedigheh Farzi : Conceptualization, investigation, analysis, writing—review and editing, project administration, supervision. Maryam Moghimian: Analysis, review and editing. Masoud Bahrami: Review and editing, supervision. Mahmood Omranifard: Analysis, supervision, review and editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study was approved by the Ethics Committee of Isfahan University of Medical Sciences (Ethics Code: IR.MUI.NUREMA.REC.1403.124). All research procedures were conducted in accordance with ethical standards, and participant confidentiality was rigorously maintained. Written informed consent was obtained from all participants after a comprehensive explanation of the study objectives and procedures.
Consent to participate
Informed consent was obtained from all individual participants included in the All research procedures were conducted in accordance with ethical standards, and participant confidentiality was rigorously maintained. Written informed consent was obtained from all participants after a comprehensive explanation of the study objectives and procedures.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ghasemi, H., Omranifard, M., Bahrami, M. et al. Challenges in burn care management: a qualitative study of health professionals’ and patients’ perspectives. Sci Rep 15, 33401 (2025). https://doi.org/10.1038/s41598-025-18722-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-18722-3
