
Abstract
The growing reliance on online communities has reshaped how individuals articulate, validate, and navigate psychological distress. However, the value of online peer support spaces remains insufficiently studied, particularly in the context of underrecognized conditions such as Premenstrual Dysphoric Disorder (PMDD). Here we investigated r/PMDD, a Reddit-based peer support community comprising 17,332 participants over a 12-year period (2012–2024), contextualized by their activity across 112 other mental health subreddits. We found a substantial decrease in the association of PMDD with depression and anxiety, evident both in general cross-community activity trends and at the individual level shortly after users become active in r/PMDD. Despite PMDD’s clinical classification as an affective disorder, users frequently discussed both psychological and physical symptoms. These discussions largely aligned with DSM-5-TR diagnostic criteria, though substantial heterogeneity was evident across individuals. Users clustered around distinct treatment types, with SSRI antidepressants, contraceptives, and complementary medicine as the most prominent. These three medication types were negatively associated between each other, indicating a compartmentalized approach to treatment. Moreover, users posting about SSRI antidepressants in r/PMDD exhibited higher cross-community activity across most disorders compared to those posting about contraceptives. The findings underscore the value of online peer support communities as a complement to clinical understanding of diagnostically complex conditions like PMDD, particularly in relation to comorbidity patterns, symptomatology, and treatment.
Similar content being viewed by others

Introduction
There is growing recognition of the relationship between hormonal fluctuations and mental health, particularly the impact of the menstrual cycle on psychological well-being, as evidenced by several recent initiatives, such as the Menarche, Menstruation, Menopause and Mental Health (4M) consortium1 and the journal special issue Menstruation Matters2. Among menstrual-related disorders, Premenstrual Dysphoric Disorder (PMDD) has received particular attention due to its significant psychological and functional impairments3,4. PMDD is a severe, cyclical mood disorder characterized by emotional, cognitive, and physical symptoms that occur during the luteal phase of the menstrual cycle and resolve shortly after menstruation begins5,6,7,8,9. Prevalence varies by diagnostic method and cultural context, ranging from 1.6% (95% CI 1.0–2.5%) for confirmed DSM diagnoses to 7.7% (95% CI 5.3–11.0%) for provisional cases10,11,12,13, with the highest rates reported in African samples and the lowest in North America.
Although the impact of menstruation on mental health has been documented in academic literature as early as 193114, Premenstrual Dysphoric Disorder (PMDD) was not formally recognized until the Fifth Edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5, 2013)15 and later included in the International Classification of Diseases (ICD-11, 2019)16. Since then, several key initiatives have specifically aimed to advance PMDD research, diagnosis, and support, including the UK PMDD Research Agenda17 and the iHera Project (EUniWell, 2023)18. Collectively, these efforts highlight the growing momentum in PMDD research.
Despite its recognition, PMDD remains a contentious diagnosis19. A central challenge lies in the reliance on self-reported symptom tracking, which requires individuals to document symptoms over multiple menstrual cycles to ascertain a cyclical pattern. This process is particularly difficult for those experiencing acute distress or irregular menstrual cycles, as well as for individuals struggling to communicate their experiences in a way that aligns with clinical criteria20. The complexity of diagnosis is further compounded by the substantial symptom overlap between PMDD and other mental health conditions, including Bipolar Disorder, Anxiety, and Depression, often leading to misdiagnoses before PMDD is correctly identified19. Since symptoms occur only in the luteal phase, tracking temporal patterns is crucial for diagnosis. However, research indicates that affected individuals may struggle to access appropriate care, highlighting systemic gaps in menstrual health services9,19,21.
Platforms such as Reddit have become vital spaces for anonymous mental health discussions, enabling online peer support and collective knowledge exchange22,23,24. In the context of menstrual health disorders, limited institutional recognition and support often drive individuals to these communities in search of alternative resources, whether to navigate healthcare systems, advocate for their needs, or manage their condition independently19,21. User-generated content has fueled a growing body of research that investigates large-scale social media data to study mental health conditions such as suicidality, depression, and eating disorders25,26,27. These studies have advanced to early detection models, improved symptom identification, and contributed to understanding online peer support dynamics28,29,30. While such findings have yet to be fully integrated into clinical guidelines, they increasingly inform risk assessment tools, digital mental health interventions, and personalized support systems31,32. Given the diagnostic challenges surrounding PMDD, these platforms offer a valuable opportunity to extend research beyond traditional clinical settings, capturing the lived experiences of individuals who self-manage the condition, encounter barriers to care, or find existing support insufficient. Despite this potential, no prior work has examined PMDD-related discussions on Reddit or other social media platforms.
Building on the recognition of online peer support communities as meaningful sources of mental health support, this study investigates PMDD-related discussions on Reddit as a contemporary resource for accessing firsthand accounts that often go unreported in clinical research. We conducted a large-scale analysis of the r/PMDD subreddit, an active peer support community focused on PMDD, spanning twelve years of user engagement. To examine challenges in diagnosis and treatment, we analyzed how individuals describe their symptoms, conceptualize their condition, and navigate treatment options, both within r/PMDD and across adjacent mental health communities. Our investigation focused on two main questions: (1) How frequently do users of r/PMDD engage with other mental health communities, and what patterns of participation emerge following their involvement in r/PMDD? (2) What symptoms and treatments are most frequently discussed, and how do they co-occur in reported experiences? While r/PMDD may not fully represent the population of individuals affected by PMDD, it offers a unique lens into how people actively make sense of the condition, seek support, and manage symptoms across formal and informal care contexts.
Methods
Data sources and study design
We analyzed user activity from r/PMDD, a dedicated Reddit community for individuals discussing experiences, symptoms, and treatments related to premenstrual dysphoric disorder (PMDD). Publicly available posts were collected via the Pushshift.io Reddit API33, spanning March 2012 to January 2024. The dataset comprised 41,177 posts authored by 17,332 unique users. To safeguard privacy, all users were assigned pseudonymous identifiers. Posts by deleted or suspended accounts were excluded.
To situate PMDD-related discussions within the broader mental health landscape, we additionally curated 112 disorder-specific, support-oriented subreddits, collectively referred to as the Mental Health Subreddit Network (MHSN). These subreddits were manually selected from the 20,000 most popular communities, retaining only those dedicated to specific mental health conditions. Each was mapped to DSM-5-TR diagnostic categories, the text revision of the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders11 (e.g., r/bipolar2 categorized under Bipolar and Related Disorders). General, non-disorder-specific communities (e.g., r/MentalHealth) were not considered in the study to maintain diagnostic specificity. A detailed list of included subreddits and their DSM categories is provided in Supplementary Table S1. In summary, in addition to r/PMDD, 47.23% of the users active in r/PMDD were also engaged within the rest of MHSN, contributing to additional 80,905 posts that complete our dataset.
To account for substantial variation in posting activity over time, particularly the pronounced upward trend observed in r/PMDD, we incorporated explicit temporal adjustments into our analysis. Posting volume in this subreddit rose from just a few dozen posts per month in the early 2010s to several hundred per month by the 2020s, a trajectory that closely mirrors overall engagement in the MHSN (\(\rho > 0.9\), \(p < 0.001\)). This likely reflects both Reddit’s platform-wide growth and, to a lesser extent, increased cross-participation within mental health communities and rising awareness of PMDD. To mitigate potential biases from such temporal trends, all primary results are reported as averages computed over six-month sliding windows. We further assess the robustness of this approach through sensitivity analyses on window size and stride for each affected result (see Fig. A2a, Fig. A2c, and Fig. A2e). Supplementary Fig. A1 visualizes the posting trajectory of r/PMDD in context with broader disorder-category trends from the MHSN.
We further note two important aspects of the study design. First, we focused on studying behaviour around posts rather than comments, as posts are more likely to capture individuals actively seeking help or sharing personal experiences with PMDD. Prior work shows that in mental health subreddits, posts are the primary venue for individuals to share personal experiences and struggles related to their condition, while comments tend to be more reactive, offering feedback, support, or advice23. Second, participation in a disorder-specific community such as r/PMDD does not necessarily indicate a clinically confirmed diagnosis. Rather, posting behavior reasonably reflects individuals who identify with or experience symptoms related to the condition, consistent with research showing that mental health subreddits function as spaces for self-expression and help-seeking around perceived illness challenges23,34. Accordingly, the behaviors and content analyzed here capture how individuals frame and discuss their experiences, rather than verified medical histories.
Stationarity testing
Stationarity refers to the property of a time series where its statistical attributes, such as mean or variance, remain constant over time. To test for stationarity, we applied the Dickey-Fuller (D-F) and Kwiatkowski-Phillips-Schmidt-Shin (KPSS) tests35,36 in two temporality scenarios: (1) co-posting activity in MHSN among users active in r/PMDD (Fig. 1b), and (2) mentions of medication types by users in r/PMDD (Fig. 4d). Both tests were conducted under the classical assumption of no deterministic trend, meaning the model included only a constant term, as no prior assumption about trend components was imposed.
The D-F test assumes a null hypothesis of non-stationarity, specifically that the time series has a unit root. The test estimates the following autoregressive model:
where \(y_t\) is the time series at time t, \(\Delta y_t = y_t - \gamma y_{t-1}\) is the first difference, \(\alpha\) represents a constant term and \(\gamma\) is the coefficient for the lagged level. The null hypothesis of a unit root (\(\gamma = 0\)) is tested to determine if the series is non-stationary.
In contrast, the KPSS test assumes stationarity under the null hypothesis and is designed to detect deterministic trends or structural changes. The KPSS statistic evaluates the residuals of a regression of the time series on a deterministic component (constant or trend):
where T is the number of observations (in our case number of sliding windows), \(\sigma\) is the standard deviation of residuals, and \(S_t\) is the cumulative sum of residuals. Large values of the KPSS statistic indicate a rejection of stationarity.
We use both tests to achieve complementary perspectives on stationarity. The D-F tests for non-stationarity by detecting a unit root, while the KPSS checks for stationarity by identifying potential structural or deterministic trends. In this work, we use the pair of methods to investigate whether co-posting and medication discussions significantly change over time.
Difference-in-differences analysis
To examine behavioral shifts as an effect of joining the r/PMDD community, we applied a difference-in-differences (DiD) analysis. This method aimed to isolate changes specific to r/PMDD participation while controlling for broader trends, e.g., the rising popularity of r/ADHD or the decline of r/depression. More specifically, we analyzed user activity before and after their first post, comparing changes against a null model derived from general engagement trends in mental health subreddits. The purpose of the null model is to capture typical fluctuations in subreddit activity, independent of individual user behaviors. Deviations from this baseline would indicate shifts in cross-community participation linked to r/PMDD, ensuring that observed effects were not merely artifacts of overall Reddit dynamics.
Difference-in-Differences Framework In the proposed framework, the activity difference for each r/PMDD user (\(\Delta ^{\textit{obs}}_i\)) was calculated as:
where \(A_{i,\textit{post}}\) and \(A_{i,\textit{pre}}\) represent activity levels after and before their first post in r/PMDD, respectively. The corresponding expected activity difference under the null model (\(\Delta ^{null}_i\)) was computed using subreddit engagement patterns derived from general trends. Specifically, for each user in r/PMDD, we generate a corresponding synthetic user based on the null model, sampling their activity according to the overall probability distribution of community engagement. The average difference-in-differences (\(\Delta \Delta\)) is then computed as:
where \(N\) is the number of r/PMDD users analyzed, and also the number of synthetic users generated from the null model.
To account for variations in the number of active users over time, we computed differences between observed values and the null model within six-month sliding windows. The null model was derived from overall activity trends during each respective window. This approach generated a distribution of difference-in-differences values (\(\Delta \Delta _T\)), which we tested against zero using a one-sample \(t\)-test:
A mean of zero indicates no significant deviation from expected engagement trends, while a positive or negative mean suggests distinct behavioral shifts following participation in r/PMDD.
Symptom and medication extraction
We studied the prevalence and trends of symptoms and medications in r/PMDD posts using a mixed-method approach. We first used the Bio-Epidemiology-NER37 model, a Transformer-based38 named entity recognition (NER) system39 designed for detecting biomedical and epidemiological terms in textual data. This model, built on DistilBERT40, is optimized for both efficiency and performance, achieving predictive F1 scores of 0.9 across multiple benchmark datasets. Trained on domain-specific corpora, it classifies 42 distinct entity types, such as disease names, symptoms, medications, and demographic attributes.
To ensure a precise and medically relevant set of entities, we followed with filtering and manually curating symptom and medication references. First, we selected entities detected by the model and classified as either Symptoms and Signs or Medication with confidence scores exceeding 0.8. These high-confidence entities were then manually reviewed and categorized according to predefined clinical frameworks: symptoms were mapped to diagnostic criteria according to the Diagnostic and Statistical DSM-5-TR diagnostic criteria11, while medications were grouped into the following relevant PMDD medication categories: contraceptives, SSRI antidepressants, non-SSRI antidepressants, benzodiazepines, antipsychotics, antiepileptics, stimulants, beta blockers, azapirones, vitamins/minerals, other hormonal therapy, and finally other medications which do not belong to any of the earlier categories. A list of the 100 most frequent entities and their labels for both Symptoms and Signs and Medication is provided in the Supplementary Materials (Table S2 and Table S3).
After the manual stage, the curated labels were systematically applied to all entities detected to be Symptoms and Signs or Medications, with the aim to achieve a comprehensive dataset coverage while preserving the precision established during the manual stage. Sensitivity analyses confirming the stability of our results across varying model confidence thresholds are presented in Fig. A2).
Results
Cross-community activity of r/PMDD users
To investigate the relationship between PMDD and other mental health disorders in the context of both differential diagnosis and comorbidity, we analyzed the cross-community posting activity of r/PMDD users across the MHSN. We calculated the percentage of r/PMDD users who also posted in each of the 112 MHSN subreddits, aggregating co-posting values by DSM category and averaging them over six-month sliding windows to account for potential statistical trending effects (see Fig. 1, with robustness analysis in Fig. A2a). The two DSM categories with the highest co-posting rates were Depressive Disorders at \(11.61\% (\pm 0.20)\) and Anxiety Disorders at \(11.60\% (\pm 0.15)\), suggesting substantial diagnostic overlap with PMDD and highlighting the challenges of differential diagnosis in practice41. These were followed by Attention-Deficit/Hyperactivity Disorders at \(10.16\% (\pm 0.08)\), which—along with Anxiety Disorders—has previously been shown to be exacerbated by premenstrual conditions, including PMDD42,43,44.

Cross-community activity patterns of r/PMDD users across subreddits related to other mental health disorders. The left panel shows the average percentage of r/PMDD users co-posting in subreddits associated with the top 10 most co-posted disorder categories. The right panel depicts the temporal dynamics of co-posting from 2015 to 2024, highlighting notable declines in co-posting related to depressive and anxiety disorders, alongside a marked increase in co-posting for Attention-Deficit/Hyperactivity Disorders (ADHD) and autism.
The cross-community activity patterns have remained relatively consistent for most disorder categories over time since the inception of the r/PMDD subreddit. However, significant shifts in co-posting behavior were observed precisely in respect to the three disorder categories with the largest communities. As illustrated in Fig. 1, co-posting after 2018 on Depressive and Anxiety Disorders has declined threefold and twofold respectively. Conversely, co-posting on Attention-Deficit/Hyperactivity Disorders has shown a sharp increase of \(40\%\) between 2020 and 2021, a result that coincides with the general increase of posts on Reddit in this category (see Fig. A1). A non-stationarity statistical test confirmed the significance of the observed trends for all three disorder categories (\(p < 0.001\), test statistic range: \(2.45< \text {KPSS} < 8.66\)).
Shifts in cross-community activity
To explore how joining r/PMDD relates to broader support-seeking behavior, we analyzed user participation patterns across the MHSN. Specifically, we examined changes in posting activity before and after a user’s first contribution to r/PMDD, assessing whether involvement in this specialized community coincides with shifts in participation in others, such as those focused on depression and anxiety. If PMDD is a significant concern for users, we expect their participation in r/PMDD to alter their engagement with other mental health communities—either by reducing their need for external support, shifting their focus to co-occurring symptoms, or refining their self-perception.
We measured co-posting activity for each user over two 90-day periods—one preceding and one following their first post in r/PMDD. To account for the growth of r/PMDD and other subreddits in MHSN over time, we used six-month sliding window averages. Each window included all individuals who made their first post in r/PMDD within that period, capturing their co-posting activity in the corresponding pre- and post-periods. We then applied a difference-in-differences (DiD) analysis, comparing the observed changes in the r/PMDD cohort against a population-based null model sampled from general subreddit activity trends during the same time windows. This approach allowed us to isolate changes specific to r/PMDD users by controlling for broader platform-wide trends, ensuring that observed shifts were not mere artifacts of general platform dynamics.

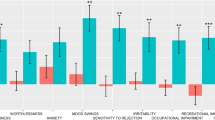
Changes in co-posting activity on subreddits related to other mental health conditions before and after a user’s first post in r/PMDD. The top panel illustrates the overall average number of posts per user before and after joining r/PMDD, highlighting a slight increase in posting activity. The main panel presents the changes in co-posting activity for the 10 most co-posted disorders, comparing r/PMDD users (colored bars) to a population-based null model (gray bars). Statistically significant differences between r/PMDD users and the null model, as determined by a difference-in-differences test, are annotated with p-values.
The results on cross-community activity shifts are shown in Fig. 2. First, we observed an overall increase in MHSN activity for individuals after their initial engagement with r/PMDD, with an average of 0.56 (\(\pm 0.03\)) posts per user prior to joining compared to 0.63 posts after joining (\(\pm 0.03\)). Despite this overall increase, there was a significant decrease in co-posting activity for two disorder categories: Depressive Disorders (\(-0.439\% \pm 0.060\)) and Anxiety Disorders (\(-0.156\% \pm 0.051\)). Conversely, we observed significantly higher increases than expected under the null model for Post-Traumatic Stress Disorders (\(+0.438\% \pm 0.019\)), Obsessive-Compulsive Disorders (\(+0.234\% \pm 0.023\)), and Social Anxiety Disorders (\(+0.162\% \pm 0.023\)). These shifts suggest that after engaging with r/PMDD, users may begin to recontextualize or expand their understanding of their mental health by moving away from broader, more generic diagnostic categories and increasingly associating their experiences with more specific or nuanced conditions that better reflect their symptom patterns.
The observed increase in co-posting activity for Post-Traumatic Stress Disorder may partly reflect the association between PMDD and early-life trauma, which is hypothesized as a significant risk factor for the disorder45,46. Similarly, hormonal fluctuations associated with the menstrual cycle are known to exacerbate obsessive-compulsive symptoms, potentially explaining the increase in co-posting activity related to Obsessive-Compulsive Disorders47,48. Although direct studies linking PMDD to Social Anxiety Disorders are lacking, the simultaneous reduction in co-posting for general Anxiety Disorders and increase for Social Anxiety Disorders may indicate a shift in users’ self-perception and symptom categorization. The re-evaluation of anxiety-related experiences could be influenced by engagement with the r/PMDD community and underscores the potential of further research to explore how community interaction shapes symptom identification and reporting.
Symptoms
We examined how PMDD symptoms are discussed in the r/PMDD community to find out how the experiences of users align with clinical diagnostic criteria. A clear understanding of PMDD symptoms is essential for accurate clinical diagnosis and for those affected to manage their condition in daily life. However, individual manifestations may be more complex and may not fully align with the diagnostic criteria outlined in the DSM and ICD. According to the diagnostic criteria of DSM-5-TR11, the defining characteristic of PMDD, named as criterion A, is the distinct temporal pattern: symptoms emerge in the final week before menses, improve within a few days after onset, and remain minimal or absent in the post-menses weeks. However, the specific cyclical symptoms outlined as diagnostic criteria are broad and significantly overlap with other conditions, as no individual symptom outside of criterion A is unique to PMDD. The diagnostic framework categorizes these symptoms into two groups: criteria B include emotional symptoms such as affective lability, irritability, depressed mood, and anxiety, while criteria C encompass physical symptoms such as fatigue, changes in appetite, and difficulty concentrating. For a PMDD diagnosis, at least one symptom from each group must follow the temporal patterning defined by criterion A. Given the generality and diagnostic overlap of criteria B and C with other mental health conditions, we examined user discourse to understand how individuals articulate their experiences in relation to the clinical definition of the condition.
Symptom references in r/PMDD posts were identified through a mixed automated and manual process, combining transformer-based biomedical entity detection with manual validation aligned to DSM-5-TR criteria (see Methods for details). A list of the 100 most frequent symptom entities is provided in Supplementary Table S2.
The symptom (Fig. 3) analysis showed that \(55.47\% \, (\pm 0.14)\) of users referred to at least one B symptom. Among these, the most commonly reported was depressed mood (B3), mentioned by \(33.75\% \, (\pm 0.16)\) of users, followed by affective lability (B1) at \(29.05\% \, (\pm 0.19)\) and anxiety (B4) at \(24.91\% \, (\pm 0.08)\). Irritability and/or anger (B2) was mentioned by the fewest users, at \(21.41\% \, (\pm 0.15)\). On the other hand, \(42.73\% \, (\pm 0.14)\) of users referred to at least one C symptom. Among these, physical symptoms (C7) were the most frequently reported, mentioned by \(34.40\% \, (\pm 0.13)\) of users, followed by fatigue (C3) at \(15.01\% \, (\pm 0.07)\) and changes in appetite (C4) at \(4.62\% \, (\pm 0.05)\). Finally, only \(3.79\% \, (\pm 0.05)\) of users referred to psychological symptoms not explicitly covered in the DSM-5-TR diagnostic criteria for PMDD49 (labeled as Other), with depersonalization, body dysmorphia, and forgetfulness being the most commonly mentioned. This indicates that the diagnostic criteria largely align with the symptoms discussed within the community. These results were computed using distributions over six-month sliding windows to mitigate potential statistical trending effects. Robustness of the findings with respect to window size and stride is examined in Fig. A2d.

Symptoms reported in the r/PMDD community. The top panel illustrates the percentage of r/PMDD users who referred to symptoms grouped according to the DSM-5-TR diagnostic criteria, with emotional symptoms (criteria B) and physical symptoms (criteria C) represented separately. The bottom panel provides a more detailed breakdown, showing the frequency of specific symptom groups within these criteria. Depressed mood (B3) and general symptoms from Criterion C were the most frequently mentioned.
We also analyzed associations between symptoms mentioned in PMDD-related discussions, as understanding how symptoms co-occur can help differentiate variations of PMDD and distinguish it from related conditions, such as severe premenstrual syndrome (PMS). We measured the association patterns of criteria B and criteria C by computing their co-appearance in a single post (shown in Fig. 5). Using a chi-squared test for independence (Bonferroni-adjusted \(p<0.001\)), we found the strongest association (\(OR=2.82\)) between subjective difficulty in concentration (C2) and lethargy (C3). This reflects the documented interplay between cognitive and physical fatigue symptoms, which often overlap in their symptomatology50,51. The second strongest association (\(OR=2.77\)) was between marked anxiety (B4) and a sense of being overwhelmed or out of control (C6), a pair of symptoms that conceptually overlap as they both reflect heightened emotional dysregulation and feelings of loss of control. Notably, four pairs of symptoms were significantly less likely to co-occur than expected by chance, all involving pairs of the general physical symptoms (C7) and the four emotional symptoms from criteria B. The lowest odds (\(OR=0.46\)) were observed between physical symptoms (C7) and depressed mood (B3). Such results are suggesting a subgroup of r/PMDD users who primarily focus on physical symptoms outlined in criteria C. This pattern may reflect cases in which users experience milder forms of PMDD or symptoms more closely aligned with severe premenstrual syndrome (PMS), a condition that, unlike PMDD, is not classified as a mental health disorder.
Medications
We analyzed patterns of medication-related discussions in the r/PMDD community to understand treatment preferences and trends over time. Various medications have been shown to effectively alleviate the physical and emotional symptoms of PMDD, including antidepressants, anxiolytics, hormonal contraceptives, and other hormonal treatments, with the majority of research focusing on Selective Serotonin Reuptake Inhibitors (SSRI antidepressants)52,53. However, these treatment options differ significantly in their mechanisms of action, usage patterns, and side effect profiles. Hormonal treatments require sustained use and directly influence the endocrine system, while SSRI antidepressants can be used intermittently. Given these distinctions, it is essential to examine the prevalence of posts about specific medication use, how discussions around different treatments have evolved over time, and whether distinct user subgroups emerge based on treatment preferences. To address this, we analyzed patterns of medication-related discussions in the r/PMDD community, assessing both the longitudinal trends in treatment mentions and the extent of overlap between different medication types.
We extracted information about medications using the same text-processing pipeline applied in the symptom analysis. Here, the detected medications were classified into 12 mutually exclusive types (listed in Fig. 4a). Once again, to account for potential statistical trending effects, prevalence was computed using distributions over six-month sliding windows. Robustness analyses related to model confidence are presented in Fig. A2d, and those concerning the choice of window size and stride are shown in Fig. A2e. A list of the 100 most frequent medication entities is provided in the Supplementary Materials (Table S3).
The results revealed that contraceptives are the most frequently discussed medication types, with \(20.63\% \, (\pm 0.16)\) of users mentioning such treatments in their posts. Within this medication type, oral estroprogestins are the most mentioned (\(\ge 2.69\%\)), followed by localized hormonal intrauterine devices (\(\ge 1.02\%\)) and leuprolide (\(\ge 0.55\%\)), a gonadotropin-releasing hormone typically prescribed for severe PMDD cases (see Fig. 4b). SSRI antidepressants are the second most discussed medication type, being referred by \(18.14\% \, (\pm 0.26)\) of users. Fluoxetine (\(\ge 5.21\%\)) is the most frequently mentioned in this group of medications, followed by sertraline (\(\ge 4.25\%\)) and escitalopram (\(\ge 1.51\%\)), all of which are studied for their effects via intermittent usage. Non-SSRI antidepressants were infrequently discussed, appearing in only \(5.03\% \, (\pm 0.11)\) of users’ posts. While anxiolytics can alleviate certain PMDD symptoms, benzodiazepines were referenced by just \(2.01\% \, (\pm 0.07)\) of users. Noteworthy, despite the strong association between r/PMDD users and Attention-Deficit/Hyperactivity Disorder (ADHD), stimulants (commonly prescribed for ADHD) were mentioned by only \(0.61\% \, (\pm 0.03)\) of users. This suggests that r/PMDD users ADHD and PMDD treatment distinct, reflecting a clear conceptual differentiation between the two disorders.

Presence and trends of discussed medications in the r/PMDD community. (a) Bar plot showing the percentage of r/PMDD users mentioning medications from 12 different types, highlighting contraceptives and SSRI antidepressants as the most frequent categories. (b) Bar plot detailing the percentage of users mentioning specific medications within the types. (c) Cross-community engagement patterns, comparing users who post about contraceptives in r/PMDD with those discussing SSRI antidepressants. (d) Temporal dynamics of medication mentions, depicting six-month averages for the percentage of users mentioning each medication type. While early years exhibit higher volatility due to lower activity, no significant qualitative shifts in medication trends are observed in later years.
To examine the evolution of treatment strategies and user adaptation, we computed the percentage of users referencing each medication type over time using the six-month sliding window approach (Fig. 4d). A non-stationarity test indicated that all medication types, except non-SSRI antidepressants (\(p < 0.001\), test statistic range: \(0.46< \text {KPSS} < 2.66\)), exhibited non-stationary trends, yet no qualitative shifts in medication practices were observed after 2019. Despite a significant decline in the association between r/PMDD users and users posting to Depressive and Anxiety Disorders since 2019 (Fig. 1), antidepressant mentions remained stable. This discrepancy may stem from either (1) the slow evolution of medication practices, particularly in the absence of major advances in alternative treatments, or (2) a decoupling of antidepressant use from their traditional role in treating depression. This decoupling might be further emphasized in PMDD treatment, as SSRI antidepressants are also prescribed intermittently during the luteal phase to target PMDD-specific symptoms rather than chronic mood disorders.
Our analysis of medication co-occurrence patterns in posts revealed distinct treatment clusters within the r/PMDD community (Fig. 5). SSRI antidepressants and contraceptives co-occurred three times less often than would be expected by chance (\(OR=0.39\), Bonferroni-adjusted \(p<0.001\)). Similarly, contraceptives exhibited low co-occurrence with five other medication types, reinforcing a separation in treatment approaches. In contrast, vitamins and minerals frequently co-occurred with medications classified as Other, indicating a subgroup of users focused on complementary medicine. As a follow-up, we analyzed cross-posting behavior among those discussing contraceptives and SSRI antidepressants. Users in the SSRI group were more likely to engage in subreddits related to various other disorders (Fig. 4c). The most pronounced differences were observed for Post-Traumatic Stress Disorder, where the SSRI group had an \(81\% (\pm 4.86\%)\) higher co-posting rate, and Autism Spectrum Disorder, where the SSRI group exhibited a \(69\% (\pm 2.40\%)\) higher co-posting rate.
Finally, we measured co-appearances of symptoms and treatment types in a single post (Fig. 5). The strongest positive association was between anxiety (B4) and benzodiazepines (\(OR=2.33\), Bonferroni-adjusted \(p<0.001\)), aligning with their established use for acute anxiety relief. Only a weak association was observed between depressed mood (B3) and contraceptives (\(OR=1.17\)). Conversely, we identified seven significantly negative associations, with the strongest being between physical symptoms (C7) and SSRI antidepressants (\(OR=0.57\)), suggesting that users concerned with physical symptoms may be less inclined to discuss this medication type as a relevant treatment option. This aligns with the symptom analysis, which indicated a subgroup primarily experiencing physical symptoms more characteristic of PMS rather than PMDD.

Associations of symptoms and medications discussed in r/PMDD posts. The figure presents three heatmaps illustrating the odds ratios for the co-appearance of symptom-symptom pairs (top left), medication-medication pairs (top right), and symptom-medication pairs (bottom) in a single post. Only significant associations (Bonferroni-adjusted \(p<0.001\), based on a chi-squared test) are shown. The odds ratios are represented by color intensity, with red indicating positive associations (greater co-appearance than expected by chance) and blue indicating negative associations (less co-appearance than expected by chance).
Discussion
Our analysis of over twelve years (2012 2024) of posts from the online peer support community r/PMDD, alongside 112 related mental health subreddits, reveals large-scale patterns in comorbidity, symptom expression, and treatment preferences that are rarely captured in clinical research. Over time, co-posting with depression and anxiety subreddits declined, while engagement with ADHD-related subreddits increased markedly after 2019. While the growing prominence of ADHD discourse only reflects broader trends beyond the PMDD community, our findings suggest that individuals joining r/PMDD may reassess their relationship with depression and anxiety—evidenced by decreased engagement with those subreddits following their initial post. Rather than indicating a diagnostic shift, this change may reflect a reconfiguration of symptom interpretation and comorbid associations prompted by participation in a peer support space that better resonates with users’ lived experiences.
PMDD is clinically classified as an affective disorder, yet physical symptoms were reported by 34.4% of users, and psychological symptoms co-occurred with physical symptoms less frequently than expected (\(OR < 1\)). This pattern suggests that some individuals engaging in r/PMDD may present with symptom profiles more consistent with PMS than PMDD, highlighting heterogeneity among those seeking support for the condition.
Regarding treatment, contraceptives were the most frequently referenced medication type, followed by SSRI antidepressants. Despite the declining engagement with depression subreddits, discussions of SSRI antidepressants remained stable over time. Additionally, a strong negative association emerged between discussions of antidepressants, contraceptives, and complementary medicine (\(OR < 0.4\)), suggesting that users tend to focus on one treatment strategy at a time rather than considering multiple approaches concurrently. Expanding on this, users discussing SSRI antidepressants in r/PMDD exhibited greater cross-community activity across most mental health conditions compared to those discussing contraceptives. This underscores the interaction between comorbidities and treatment choices, showing that mental health conditions are best understood not in isolation, but as part of a complex, interconnected system in which diagnoses and interventions dynamically shape one another.
Relevance to research and clinical practice
The episodic nature of PMDD, its reliance on self-tracking, and the diagnostic ambiguity pose challenges for traditional clinical research. Conventional assessments, often limited to peak symptom severity, provide only a narrow snapshot of the condition. In contrast, online mental health communities offer a broader and more diverse sample, including individuals without formal diagnoses or access to healthcare. These platforms enable spontaneous, user-driven discussions that yield unfiltered insights into symptom conceptualization, peer support, and treatment exploration. As such, studies on online mental health support communities can help identify gaps in care, prevalent misconceptions, and diagnostic challenges, ultimately guiding more precise patient education and diagnostic criteria. Furthermore, integrative studies combining online and offline data can pave the way into studying not only potential comorbidities, but also detailed coping strategies and patient treatment dynamics, with unique perspectives on the progression of PMDD and help-seeking behaviors, ultimately allowing for more efficient and personalized treatment approaches.
While exploratory, this study illustrates the potential of online mental health data to complement traditional research, particularly for underdiagnosed and understudied conditions. As mental health increasingly intersects with digital platforms, recognizing these communities as valuable sources of patient perspectives can enhance our understanding of how individuals navigate complex disorders like PMDD. Integrating findings from these discussions into clinical practice could help bridge gaps between patient experiences and medical guidelines, leading to more patient-centered care.
Limitations
We acknowledge several limitations in this research. First, Reddit data, while offering a rich and organic source of user-generated content, is subject to demographic skew. The platform predominantly attracts a younger, Western, and U.S.-based audience, which may limit the generalizability of our findings to older or non-Western demographics54,55. Additionally, as participation is voluntary, self-selection bias is possible, with individuals experiencing more severe symptoms or distress potentially being overrepresented21. However, this characteristic of online peer support communities can also serve as a strength, offering access to candid, real-world narratives that may be underrepresented in clinical settings.
Second, Reddit data does not inherently provide clinical validation and user-generated content does not necessarily align with standardized diagnostic criteria used in medical and epidemiological research21. This introduces uncertainty regarding the clinical diagnoses of users and variability in how individuals describe their symptoms, making it challenging to verify self-reported experiences56. While shifts in engagement in r/PMDD provide important clues about symptom trajectories, it remains unclear whether changes in posting behavior reflect actual shifts in symptom severity, evolving self-perception, or exposure to new diagnostic narratives. The observational nature of this study also limits our ability to determine whether engagement in r/PMDD actively influences users’ understanding of their symptoms or simply reflects pre-existing beliefs. Despite these limitations, given the large volume of data analyzed and the stability of results, individual inconsistencies are unlikely to overshadow the broader patterns that emerge, as strong trends in discussions, symptom and medication descriptions, and co-posting behaviors persist despite the inherent noise.
Future research aiming to address these limitations could benefit from integrating online peer support data with self-reported information collected through online surveys. Combining these sources would not only validate findings but also contextualize engagement patterns, distinguishing between passive participation, active symptom discussion, and exploratory engagement with different diagnostic categories. More specifically, extending this type of research with survey-based methods would capture critical factors not typically present in peer support discussions, such as menstrual cycle tracking, formal diagnoses, and medical history, offering a more comprehensive view of the symptomatology across different healthcare access levels.
Privacy and ethical considerations
The subreddits analyzed in this study are publicly accessible, require no login credentials, and host large, active user bases. As such, individuals posting in these spaces are knowingly sharing content in a context where it is reasonable to expect observation by strangers. Reddit’s pseudonymous account system further reduces the likelihood of linking posts to real-world identities. To enhance privacy protection, usernames were additionally pseudoanonymized prior to analysis.
Given the sensitive and personal nature of the disclosures that may appear in these spaces, we prioritized strict adherence to ethical and privacy standards throughout the research process. The study was purely observational and involved no direct interaction or intervention with users. We made no attempt to contact individuals, and all findings were reported in aggregate, with no focus on individual cases.
Our approach aligns with widely recognized ethical frameworks for internet-mediated research57,58,59,60,61. In particular, under the U.S. Department of Health and Human Services (45 CFR 46), research is considered to involve human subjects only when it includes direct interaction or the use of identifiable private information—neither of which applied here. Furthermore, our methodology follows the British Psychological Society’s Ethics Guidelines for Internet-Mediated Research (2021), which emphasize proportional safeguards based on the level of risk and acknowledge that informed consent may not be required when analyzing data from platforms where there is no reasonable expectation of privacy and where individuals could expect to be observed.
This study received ethical approval from the MVLS College Ethics Committee at the University of Glasgow (Reference number: 200240023).
Data availability
Subreddit metadata and aggregated data supporting the findings of this study are provided in the supplementary materials. This data will also be made publicly available upon publication via the Figshare repository: https://doi.org/10.6084/m9.figshare.28695257. Due to platform terms of service, raw Reddit post content cannot be publicly shared. Additional aggregated data may be made available upon reasonable request by contacting the corresponding author.
Code availability
The code used to produce all figures in the paper is available at https://github.com/boevkoski/rPMDD.
References
Sharp, G. C. & Giorgio, L. Menarche, menstruation, menopause and mental health (4m): A consortium facilitating interdisciplinary research at the intersection of menstrual and mental health. Front. Glob. Women’s Health 4, 1258973 (2023).
Menstruation Matters. Nature, accessed January 22, 2025. https://www.nature.com/collections/dfecidfcac (2024).
Hantsoo, L. & Epperson, C. N. Premenstrual dysphoric disorder: Epidemiology and treatment. Curr. Psychiatry Rep. 17(11), 87 (2015).
Eisenlohr-Moul, T. Premenstrual disorders: A primer and research agenda for psychologists. Clin. Psychol. 72(1), 5 (2019).
Green, L., O’Brien, P., Panay, N., Craig, M. & Obstetricians, R. C. Gynaecologists: Management of premenstrual syndrome. Bjog 124(3), 73–105 (2017).
Obstetricians, T.A.C., Gynecologists: Premenstrual Syndrome (PMS) - ACOG. accessed November 27, 2021. https://www.acog.org/Patients/FAQs/Premenstrual-Syndrome-PMS (2015).
Tolossa, F. W. & Bekele, M. L. Prevalence, impacts and medical managements of premenstrual syndrome among female students: Cross-sectional study in college of health sciences, Mekelle University, Mekelle, northern Ethiopia. BMC Womens Health 14, 1–9 (2014).
Thakrar, P., Bhukar, K. & Oswal, R. Premenstrual dysphoric disorder: Prevalence, quality of life and disability due to illness among medical and paramedical students. J. Affect. Disorders Rep. 4, 100112 (2021).
Brown, D., Smith, D. M., Osborn, E. & Wittkowski, A. The experiences and psychological impact of living with premenstrual disorders: A systematic review and thematic synthesis. Front. Psych. 15, 1440690 (2024).
Reilly, T. J. et al. The prevalence of premenstrual dysphoric disorder: Systematic review and meta-analysis. J. Affect. Disord. 349, 534–540 (2024).
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) (American Psychiatric Association Publishing, 2022). https://doi.org/10.1176/appi.books.9780890425787.
Matsumoto, T., Egawa, M., Kimura, T. & Hayashi, T. Comparison between retrospective premenstrual symptoms and prospective late-luteal symptoms among college students. Gynecol. Reprod. Endocrinol. Metab. 1(2021), 31–41 (2021).
Craner, J. R., Sigmon, S. T. & McGillicuddy, M. L. Does a disconnect occur between research and practice for premenstrual dysphoric disorder (PMDD) diagnostic procedures?. Women Health 54(3), 232–244 (2014).
Frank, R. T. The hormonal causes of premenstrual tension. Arch. Neurol. Psychiatry 26(5), 1053–1057 (1931).
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) (American Psychiatric Association Publishing, 2013). https://doi.org/10.1176/appi.books.9780890425596.
Reed, G. M. et al. Innovations and changes in the ICD-11 classification of mental, behavioural and neurodevelopmental disorders. World Psychiatry 18(1), 3–19 (2019).
Matthews, L. & Riddell, J. Premenstrual dysphoric disorder (PMDD): The UK research agenda. University of the West of Scotland. www.uws.ac.uk/pmdd (2023).
EUniWell. The iHera Project: Initiative for Health Education, Research, and Awareness for PMS and PMDD (iHera), accessed 17 Mach, 2025. https://www.euniwell.eu/what-we-offer/seed-funding-programme/projects-of-the-seventh-seed-funding-call-2024/ihera-initiative-for-health-education-research-and-awareness-for-pms-and-pmdd (2023).
Osborn, E., Wittkowski, A., Brooks, J., Briggs, P. E. & O’Brien, P. S. Women’s experiences of receiving a diagnosis of premenstrual dysphoric disorder: A qualitative investigation. BMC Womens Health 20, 1–15 (2020).
McCoy, R.T., Bongar, B.: Premenstrual dysphoric disorder (PMDD). In Encyclopedia of Sexual Psychology and Behavior 1–5 (Springer, 2024).
Funnell, E. L., Martin-Key, N. A., Spadaro, B. & Bahn, S. Help-seeking behaviours and experiences for mental health symptoms related to the menstrual cycle: A UK-wide exploratory survey. npj Women’s Health 2(1), 2 (2024).
Naslund, J. A., Aschbrenner, K. A., Marsch, L. A. & Bartels, S. J. The future of mental health care: Peer-to-peer support and social media. Epidemiol. Psychiatric Sci. 25(2), 113–122 (2016).
De Choudhury, M., De, S.: Mental health discourse on reddit: Self-disclosure, social support, and anonymity. In Proceedings of the International AAAI Conference on Web and Social Media vol. 8 71–80 (2014).
Aschbrenner, K. A. et al. A survey of online and mobile technology use at peer support agencies. Psychiatr. Q. 89, 539–548 (2018).
Bauer, B. et al. Using large language models to understand suicidality in a social media-based taxonomy of mental health disorders: Linguistic analysis of reddit posts. JMIR Mental Health 11, 57234 (2024).
Feldhege, J., Moessner, M. & Bauer, S. Who says what? Content and participation characteristics in an online depression community. J. Affect. Disord. 263, 521–527 (2020).
Sowles, S. J. et al. A content analysis of an online pro-eating disorder community on Reddit. Body Image 24, 137–144 (2018).
Guntuku, S. C., Yaden, D. B., Kern, M. L., Ungar, L. H. & Eichstaedt, J. C. Detecting depression and mental illness on social media: An integrative review. Curr. Opin. Behav. Sci. 18, 43–49 (2017).
Reece, A. G. et al. Forecasting the onset and course of mental illness with Twitter data. Sci. Rep. 7 (1), 13006 (2017).
Low, D. M. et al. Natural language processing reveals vulnerable mental health support groups and heightened health anxiety on reddit during covid-19: Observational study. J. Med. Internet Res. 22(10), 22635 (2020).
Lehtimaki, S. et al. Evidence on digital mental health interventions for adolescents and young people: Systematic overview. JMIR Mental Health 8(4), 25847 (2021).
Berrouiguet, S. et al. From eHealth to iHealth: Transition to participatory and personalized medicine in mental health. J. Med. Internet Res. 20(1), 2 (2018).
Baumgartner, J., Zannettou, S., Keegan, B., Squire, M., & Blackburn, J. The pushshift reddit dataset. In Proceedings of the International AAAI Conference on Web and Social Media vol. 14 830–839 (2020)
Morini, V., Sansoni, M., Rossetti, G., Pedreschi, D. & Castillo, C. Participant behavior and community response in online mental health communities: Insights from Reddit. Comput. Hum. Behav. 165, 108544 (2025).
Kwiatkowski, D., Phillips, P. C., Schmidt, P. & Shin, Y. Testing the null hypothesis of stationarity against the alternative of a unit root: How sure are we that economic time series have a unit root?. J. Economet. 54(1–3), 159–178 (1992).
Dickey, D. A. & Fuller, W. A. Distribution of the estimators for autoregressive time series with a unit root. J. Am. Stat. Assoc. 74(366a), 427–431 (1979).
Raza, S., Reji, D. J., Shajan, F. & Bashir, S. R. Large-scale application of named entity recognition to biomedicine and epidemiology. PLOS Digital Health 1(12), 0000152 (2022).
Lin, T., Wang, Y., Liu, X. & Qiu, X. A survey of transformers. AI Open 3, 111–132 (2022).
Li, J., Sun, A., Han, J. & Li, C. A survey on deep learning for named entity recognition. IEEE Trans. Knowl. Data Eng. 34(1), 50–70 (2020).
Sanh, V.: Distilbert, a distilled version of BERT: Smaller, faster, cheaper and lighter. Preprint at arXiv:1910.01108 (2019).
Landén, M. & Eriksson, E. How does premenstrual dysphoric disorder relate to depression and anxiety disorders?. Depress. Anxiety 17(3), 122–129 (2003).
Yonkers, K. A. Anxiety symptoms and anxiety disorders: How are they related to premenstrual disorders?. J. Clin. Psychiatry 58(3), 62–69 (1997).
Yen, J.-Y. et al. Association between generalized anxiety disorder and premenstrual dysphoric disorder in a diagnostic interviewing study. Int. J. Environ. Res. Public Health 17(3), 988 (2020).
Dorani, F., Bijlenga, D., Beekman, A. T., Someren, E. J. & Kooij, J. S. Prevalence of hormone-related mood disorder symptoms in women with ADHD. J. Psychiatr. Res. 133, 10–15 (2021).
Pilver, C. E., Levy, B. R., Libby, D. J. & Desai, R. A. Posttraumatic stress disorder and trauma characteristics are correlates of premenstrual dysphoric disorder. Arch. Womens Ment. Health 14, 383–393 (2011).
Kulkarni, J., Leyden, O., Gavrilidis, E., Thew, C. & Thomas, E. H. The prevalence of early life trauma in premenstrual dysphoric disorder (PMDD). Psychiatry Res. 308, 114381 (2022).
Labad, J. et al. Female reproductive cycle and obsessive-compulsive disorder. J. Clin. Psychiatry 66(4), 428–435 (2005).
Vulink, N. C., Denys, D., Bus, L. & Westenberg, H. G. Female hormones affect symptom severity in obsessive-compulsive disorder. Int. Clin. Psychopharmacol. 21(3), 171–175 (2006).
American Psychiatric Association. Premenstrual dysphoric disorder. In Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) 197–201 (American Psychiatric Association Publishing, 2022). https://doi.org/10.1176/appi.books.9780890425787.
Boksem, M. A., Meijman, T. F. & Lorist, M. M. Effects of mental fatigue on attention: An ERP study. Cogn. Brain Res. 25(1), 107–116 (2005).
Faber, L. G., Maurits, N. M. & Lorist, M. M. Mental fatigue affects visual selective attention. PLoS ONE 7(10), 48073 (2012).
Kleinstäuber, M., Witthöft, M. & Hiller, W. Cognitive-behavioral and pharmacological interventions for premenstrual syndrome or premenstrual dysphoric disorder: a meta-analysis. J. Clin. Psychol. Med. Settings 19, 308–319 (2012).
Sepede, G., Sarchione, F., Matarazzo, I., Giannantonio, M. & Salerno, R. M. Premenstrual dysphoric disorder without comorbid psychiatric conditions: A systematic review of therapeutic options. Clin. Neuropharmacol. 39(5), 241–261 (2016).
Review, W. P. Reddit Users by Country 2025. Retrieved March 21, 2025. https://worldpopulationreview.com/country-rankings/reddit-users-by-country (2025).
Finlay, S. C. Age and gender in Reddit commenting and success. J. Inf. Sci. Theory Pract. 2 (3), 18–28 (2014).
Park, A., Conway, M. Tracking health related discussions on Reddit for public health applications. In AMIA Annual Symposium Proceedings vol. 2017, 1362 (2018)
King, S. A. Researching internet communities: Proposed ethical guidelines for the reporting of results. Inf. Soc. 12(2), 119–128 (1996).
Eysenbach, G. & Till, J. E. Ethical issues in qualitative research on internet communities. BMJ 323(7321), 1103–1105 (2001).
Moreno, M. A., Goniu, N., Moreno, P. S. & Diekema, D. Ethics of social media research: Common concerns and practical considerations. Cyberpsychol. Behav. Soc. Netw. 16(9), 708–713 (2013).
Chancellor, S., Birnbaum, M. L., Caine, E. D., Silenzio, V. M., De Choudhury, M. A taxonomy of ethical tensions in inferring mental health states from social media. In Proceedings of the Conference on Fairness, Accountability, and Transparency 79–88 (2019)
Balsamo, D., Bajardi, P., Salomone, A. & Schifanella, R. Patterns of routes of administration and drug tampering for nonmedical opioid consumption: Data mining and content analysis of Reddit discussions. J. Med. Internet Res. 23(1), 21212 (2021).
Funding
SL and JR are funded by MRC/CSO Social and Public Health Sciences Unit (Core funding, MC_UU_00022/3; SPHSU18). PKN acknowledges partial funding by the research programme Knowledge Technologies (P2-0103). This publication is the result of research conducted at Central European University, Private University, with open-access provided through the CEU Open Access Fund.
Author information
Authors and Affiliations
Contributions
B.E., S.L., and J.R. contributed to the study s conception and design. B.E. conducted data collection, developed the methodology, and performed the statistical analysis. B.E., S.L., and J.R. collaborated on the annotation of symptoms and medications. S.L. and P.K.N. provided critical revisions and supervised the project. B.E., S.L., P.K.N. and J.R. drafted the initial manuscript, and all authors reviewed and provided feedback on previous versions. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study received ethical approval from the MVLS College Ethics Committee at the University of Glasgow (Reference number: 200240023). Informed consent to participate was not required for this study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Evkoski, B., Letina, S., Kralj Novak, P. et al. Premenstrual dysphoric disorder in online peer support communities: a Reddit case study. Sci Rep 15, 34300 (2025). https://doi.org/10.1038/s41598-025-19220-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-19220-2
