
Abstract
The role and impact of viral infections remain a subject of interest, yet comparative data on influenza A/B, RSV, and SARS-CoV-2 in both hospitalized and non-hospitalized patients are limited. In this observational study, we analyzed data from adult patients with respiratory infections who underwent rapid testing for Influenza A/B, RSV, SARS-CoV-2, and Adenovirus between October 2023 and March 2024. Symptoms at emergency department presentation, laboratory results, risk factors, clinical course, and outcomes were assessed. Among 1,402 patients with respiratory infections, Influenza A was the most prevalent virus and the leading cause of hospitalizations, with the longest stay (mean: 9.86 days). SARS-CoV-2 was the second most common, primarily affecting older patients (mean age: 79 years), associated with the highest in-hospital mortality. RSV ranked third in prevalence, had the highest hospitalization rate among those infected, and was characterized by bronchospasm, with 25% of hospitalized patients requiring high-flow nasal cannula (HFNC). Influenza B primarily affected younger individuals and had a negligible hospitalization rate. SARS-CoV-2 patients sought care the fastest, while RSV patients had the most prolonged symptom duration before seeking medical attention. Despite differences in care-seeking timing, most Flu-A, Flu-B, and SARS-CoV-2 patients recovered within 2–5 days, with no significant difference observed. Vaccine effectiveness against Influenza A was 49.5%. This estimate should be interpreted with caution due to potential confounding by age and comorbidities. These findings offer comparative insights into the clinical burden of respiratory viruses during the 2023–2024 season, reflecting patterns in the post-pandemic era.
Similar content being viewed by others


Introduction
Influenza is a seasonal respiratory infection caused by type A (Flu-A) and B (Flu-B) viruses. Circulating mainly from late fall through early spring, it affects up to 20% of individuals each year1,2. These RNA viruses from the Orthomyxoviridae family mutate constantly, with type A capable of causing pandemics through major genetic shifts, while type B is generally milder and less common2. Since 2009, seasonal flu has included A(H3N2), A(H1N1)pdm09, and two B lineages. Most infections resolve within one to two weeks, but severe illness can lead to hospitalization, ICU admission, or even death—especially in older adults, pregnant individuals, and young children3. During a typical season, influenza causes 3–5 million severe cases and up to 650,000 respiratory deaths globally4. In the U.S., median influenza incidence over the past decade was 6.8% in adults 18–49 and 11.6% in those 50–645. Our team previously reported that in the 2023–2024 season, influenza A peaked in weeks 51–52 of 2023, slightly later than the previous season, while ERVISS data showed the epidemic began in week 50 and declined by week 4 of 2024, with influenza B peaking in week 106,7. Beyond health impacts, influenza imposes economic burdens through work absences and healthcare strain. Annual vaccination, recommended by CDC and ACIP for all individuals six months and older, reduces illness, hospitalizations, and deaths, yet uptake remains low, especially among adults 18–648,45.
A significant portion of influenza-like illness (ILI) is caused by viruses and bacteria other than influenza, with respiratory syncytial virus (RSV) being a major respiratory pathogen that primarily affects vulnerable populations such as young children, older adults, and individuals with underlying health conditions. In the U.S., RSV affects 3–7% of healthy older adults (≥ 65 years) and 4–10% of those at higher risk for severe infection9. While most cases are mild, RSV can lead to severe complications like pneumonia and exacerbation of chronic conditions such as Chronic Obstructive Pulmonary Disease (COPD), asthma, and heart failure, especially in older adults and immuno-compromised individuals10. A recent study found that over half of adults aged ≥ 60 hospitalized with RSV were aged ≥ 75, with common comorbidities including obesity, COPD, heart failure, and diabetes11. RSV is associated with more severe outcomes than influenza, including longer hospital stays, higher ICU admissions, increased pneumonia rates, and higher mortality12. In the U.S., RSV causes approximately 177,000 hospitalizations and 14,000 deaths annually in adults aged 65 and older13. Despite its impact, nearly half of primary care physicians rarely evaluate adults for RSV, often due to the lack of antiviral treatments and misconceptions about antibiotics14. CDC now recommends a single dose of any of the three FDA-licensed RSV vaccines for adults aged 75 and older, and those aged 60–74 at increased risk13. Despite this, vaccination coverage remains low, with only 24.4% of adults over 60 vaccinated as of May 2024, and an additional 10.7% planning to get the vaccine15.
Coronaviruses are common pathogens in humans and animals, with four endemic types causing mild respiratory illnesses and three zoonotic strains—SARS-CoV, MERS-CoV, and SARS-CoV-2—emerging in recent decades with severe outcomes16,17. SARS-CoV-2, the virus responsible for COVID-19, was declared a global pandemic by the WHO on March 11, 2020, and is no longer a public health emergency as of May 2023, though it continues to evolve and pose health risks18. As of March 2025, there have been approximately 778 million reported COVID-19 cases worldwide19. Risk factors for severe COVID-19 include advanced age, obesity, male sex, and comorbidities such as hypertension, diabetes, and chronic lung disease20. COVID-19 continues to pose challenges due to reduced immunity over time, the emergence of new variants, and variation in public health strategies. Despite reduced severity, new variants continue to appear, prompting the CDC to recommend the updated 2024–2025 COVID-19 vaccine for all individuals aged 6 months and older, with a focus on those aged 65 and older and at high risk for severe disease21. The WHO also stresses staying current with vaccinations, especially for those with underlying health conditions or immunocompromised states, to prevent severe outcomes and alleviate pressure on healthcare systems22.
Human adenoviruses (HAdVs) are a group of over 100 types that cause respiratory infections, including the common cold, pneumonia, and in severe cases, ARDS, especially in individuals with weakened immune systems. Transmission occurs through respiratory droplets, contaminated surfaces, and occasionally, water. While symptoms typically include fever, sore throat, cough, and runny nose, severe cases are linked to species B, C, and E23. A vaccine for types 4 and 7 is available for U.S. military personnel. New strains continue to emerge, with outbreaks of severe disease from HAdV-B7 reported in multiple regions, highlighting the need for ongoing monitoring24.
In the aftermath of the COVID-19 pandemic, the epidemiology and seasonality of respiratory viruses have shifted significantly, complicating diagnosis and public health planning. During the 2024/2025 winter season, the European Centre for Disease Prevention and Control (ECDC) reported sharp increases in influenza and respiratory syncytial virus (RSV) across the EU/EEA, with influenza test positivity exceeding 10% by week 49 and RSV-linked hospitalizations peaking in children under five and adults over 6525. SARS-CoV-2 circulation remained at low-to-moderate levels, but continued to drive hospitalizations, accounting for 84% of COVID-19-related admissions in older adults25. A systematic review by Golpour et al. found that influenza co-infection in COVID-19 patients reached 14% globally, with regional peaks of 17% for influenza A in Europe26. While our study does not assess co-infections, these findings highlight the clinical complexity introduced by overlapping viral activity. Contes and Liu report increasing synchronization of SARS-CoV-2, influenza, and RSV activity, creating diagnostic challenges and elevating the role of multiplex molecular testing27. Mathematical modeling by Rodríguez and Eguíluz further shows that virus-virus interactions—whether cooperative or competitive—can synchronize epidemic peaks, exacerbating healthcare system strain28. Eales et al. underscore the need for integrated surveillance systems to monitor concurrent respiratory epidemics and guide response strategies29. However, recent literature lacks studies that have simultaneously compared the clinical profiles of influenza A/B, RSV, and SARS-CoV-2 in adult populations within a single epidemic wave in the post–COVID-19 pandemic period. In this context, our study aimed to compare the clinical characteristics and hospitalization risks associated with the major respiratory viruses circulating during the 2023–2024 winter season in Greece—namely Influenza A/B, RSV, and SARSCoV-2—testing the hypothesis that each virus exhibits distinct clinical patterns relevant for differential diagnosis and public health preparedness in an era of viral co-circulation.
Results
Out of 1,402 patients finally included in the study, the mean age (± SD) was 51.64 (± 21.433). The study population consisted of 678 male (48.4%) and 724 (51.6%) female participants. Of those, 228 tested positive for Influenza A (16.2%), 196 for SARS-CoV-2 (14%), 64 for Influenza B (4.6%), 61 for RSV (4.4%), and 11 for adenovirus (0.8%). Due to the small number of adenovirus-positive patients, they were not analyzed further.
Hospitalized VS Non-hospitalized overall
Among 248 patients, approximately 20% required hospitalization for respiratory infections, while the remaining patients were discharged with home care instructions. Males (N = 140) were significantly more likely to be hospitalized than females (N = 108), with an odds ratio of 1.48 (95% CI: [1.13, 1.96], p = 0.005). The mean age of hospitalized patients was 70.60 years (± 16.87, 95% CI: [68.5, 72.7]), significantly higher than non-hospitalized patients (47.56 ± 20.08, 95% CI: [46.4, 48.8], p < 0.001). The mean BMI of hospitalized patients was 29.23 (± 16.15, 95% CI: [27.22, 31.26]), which was significantly higher than that of non-hospitalized patients (27.8 ± 13.36, 95% CI: [27.04, 28.59], p = 0.003). The average duration of symptoms before hospital admission was 4.79 ± 3 days for hospitalized patients, compared to 4.29 ± 4.58 days for non-hospitalized patients, with no statistically significant difference. Among hospitalized patients, 38 (15.3%) tested positive for Influenza A, 20 (8.1%) for SARS-CoV-2, 26 (10.5%) for RSV, 1 (0.4%) for Influenza B, and 1 (0.1%) for adenovirus. The remaining hospitalized patients tested negative for these specific viruses but were admitted due to the severity of their symptoms.
Hospitalization rates

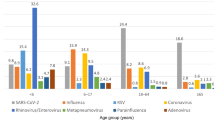
Distribution of Hospitalized and Non-Hospitalized Cases by Virus and Gender. Proportions of hospitalized and non-hospitalized individuals for Influenza A (Flu-A), Influenza B (Flu-B), SARS-CoV-2, and Respiratory Syncytial Virus (RSV), stratified by gender. The chart differentiates between hospitalized and non-hospitalized cases for males and females, highlighting variations across virus types.
Hospitalization rates varied significantly across viruses, with the highest involving RSV (42.6%), followed by Flu-A (16.6%), SARS-CoV-2 (10.2%), and Flu-B (rare, with one case). Gender differences emerged: women had higher hospitalization rates for RSV and SARS-CoV-2, while men were slightly more affected by Flu-A. Flu-B hospitalizations were rare in both sexes. Specifically, 13.55% of hospitalized women had Flu-A, 0% had Flu-B, 13.68% had SARS-CoV-2, and 44.4% had RSV. Among men, 20% had Flu-A, 3.22% had Flu-B, 6.90% had SARS-CoV-2, and 40% had RSV (Fig. 1).
Symptoms/Signs

Symptom Distribution by Virus and Hospitalization Status. Bar chart illustrating the frequency of symptoms/signs (fever, cough, sputum, dyspnea, and wheezing) among hospitalized and non-hospitalized individuals for Influenza A (Flu-A), Influenza B (Flu-B), Respiratory Syncytial Virus (RSV), and SARS-CoV-2. The figure highlights variations in symptom prevalence across virus types and hospitalization states.
Symptoms analysis based on virus type
Among Flu-A patients, hospitalized individuals had significantly higher rates of sputum production (95% CI: [1.08, 4.42], p = 0.042) and dyspnea (95% CI: [4.77, 23.65], p < 0.001), indicating greater respiratory compromise. Upper respiratory tract infection (URTI) symptoms were associated with a lower likelihood of hospitalization (p < 0.001). In Flu-B cases, only one out of 64 patients required inpatient care, suggesting a milder disease course. For SARS-CoV-2, dyspnea was again significantly more prevalent in hospitalized patients (p < 0.001), further highlighting its role as a key marker of disease severity in COVID-19 cases. RSV patients requiring hospitalization were more likely to present with fever (p = 0.008), suggesting that higher fever may be linked to the need for inpatient care in RSV infections. As in Flu-A, URTI symptoms were linked to outpatient management (p < 0.001) (Fig. 2).
Symptoms/Signs analysis between hospitalized patient groups
When grouped into systemic symptoms (including fever, myalgias/arthralgias, headache, and fatigue) or URTI symptoms (congestion and sore throat), no statistically significant differences were observed between the hospitalized patient groups.
However, symptom-specific differences did emerge. Cough prevalence differed significantly between groups (p = 0.014), with post-hoc analysis showing higher cough frequency in RSV compared to SARS-CoV-2 (p = 0.008). Sputum production also varied by group (p = 0.028), being significantly more common in RSV than in SARS-CoV-2 (p = 0.018), and in Flu-A compared to SARS-CoV-2 (p = 0.025). Wheezing was most frequently observed in RSV cases (~ 60%) and occurred significantly more often than in Flu-A (p = 0.038) and SARS-CoV-2 (p < 0.001), although there was no significant difference between Flu-A and SARS-CoV-2. These respiratory symptoms were reflected in treatment patterns: corticosteroids were used more often in RSV (50%; p = 0.005), and magnesium sulfate, a marker of severe bronchospasm, was administered only in RSV cases (p = 0.009).
Comparative analysis of symptoms/signs between Non-Hospitalized patient groups

Pairwise Comparisons of Symptoms/Signs Among Non-Hospitalized Patients Across Viral Infections. Heatmap of p-values for symptom/sign differences among non-hospitalized patients with Influenza A (Flu-A), Influenza B (Flu-B), Respiratory Syncytial Virus (RSV), and SARS-CoV-2. Systematic symptoms include fever, myalgias/arthralgias, headache, and fatigue; URTI symptoms include nasal congestion and sore throat. Darker colors denote stronger statistical significance. URTI: upper respiratory tract infection.
Analysis of non-hospitalized patients infected with Flu-A, Flu-B, RSV, or SARS-CoV-2 showed that systemic and upper respiratory tract (URTI) symptoms were common across all groups, with modest variation in frequency (Fig. 3). Systemic symptoms were reported in > 90% of Flu-A, Flu-B, and SARS-CoV-2 cases and somewhat less often in RSV (~ 80%). URTI symptoms were also frequent overall; Flu-B showed the highest proportion (85.7%), followed by SARS-CoV-2 (73.9%), RSV (62.9%), and Flu-A (61.6%).
Among individual symptoms, several pairwise differences reached statistical significance (Fig. 3). Fever was most common in influenza cases (Flu-A 83.2%, Flu-B 77.8%), and less common in SARS-CoV-2 (63.6%), and RSV cases (42.9%). Similarly, dyspnea occurred more often in RSV patients (31.4%) compared to all other viruses, where the prevalence remained below 15%. In contrast, cough was prevalent across all viruses, exceeding 84% in Flu-A, Flu-B, and RSV, with somewhat lower rates in SARS-CoV-2 (64.2%). Sputum production tended to be higher in RSV and Flu-B (45.7% and 47.6% respectively) than in SARS-CoV-2 (25%), while Flu-A patients showed intermediate rates (33.7%). Notably, no statistically significant differences were observed between Flu-A and Flu-B across the examined symptoms, underscoring their overlapping clinical presentations in outpatient settings.
Influenza A
Among Influenza A-positive patients, one in six required hospitalization, with the majority being male. Hospitalized patients were significantly older (75.68 ± 13.29 years, 95% CI: [71.3, 80.1) compared to non-hospitalized patients (45.1 ± 18.4 years, 95% CI: [42.5, 47.8]), with a large effect size (r = − 0.52, 95% CI: [–0.65, − 0.39], p < 0.001). Hospitalized patients had a higher BMI (28.28 ± 5.72) compared to non-hospitalized patients, though this difference was not statistically significant. Nearly all hospitalized patients had at least one comorbidity (95% CI: [4.54, 39.09], p < 0.001), with chronic pulmonary disease, chronic heart disease, diabetes mellitus, and immunocompromised status being strongly associated with hospitalization. Hospitalized patients had slightly longer symptom duration before seeking care (3.79 ± 2.26 days, 95% CI: [3.04, 4.53]) than non-hospitalized patients (95% CI: [2.81, 3.44]), with a small but significant effect (p = 0.049, r = − 0.13, 95% CI: [–0.26, − 0.001]). Radiological evidence of pneumonia was strongly associated with hospitalization (p < 0.001); patients with unilateral infiltrates had 46.5 times higher odds (95% CI: [8.04, 269.34]) and those with bilateral infiltrates had 140.4 times higher odds (95% CI: [8.00, 2461.53]) of admission.
Multivariate binary logistic regression revealed that age (aOR = 0.896, p = 0.001), diabetes (aOR = 5.12, p = 0.034), unilateral pneumonia (aOR = 529.01, p < 0.001), and dyspnea (aOR = 4.82, p = 0.039) were strong predictors of hospitalization. The overall model was statistically significant (χ²(15) = 148.60, p < 0.001), explained 80.6% of the variance (Nagelkerke R² = 0.806), and correctly classified 95.2% of cases. However, vaccination did not significantly impact hospitalization outcomes (aOR = 1.178, p = 0.805), suggesting that comorbidities and disease severity were the primary drivers.
Influenza B
Out of 64 Influenza B-positive patients, only one required hospitalization. This patient was a 72-year-old male, obese, with multiple comorbidities, including COPD, coronary artery disease, and diabetes mellitus. He delayed seeking medical attention for approximately one week before presenting to the emergency department, subsequently developing unilateral pneumonia, likely due to a secondary bacterial infection. Despite prior influenza vaccination, hospitalization was required. In contrast, the majority of Influenza B-positive patients (30 males and 33 females, mean age 34.49 ± 16.17 years) sought medical care after an average of 3.43 ± 1.87 days and did not require hospitalization.
Seasonal influenza vaccination
The following analysis explores the relationship between influenza vaccination and outcomes in Flu-A positive patients during the 2023–2024 season. As this is an observational study, associations are reported without implying causation, and confounding factors—particularly age and comorbidity—are considered in both unadjusted and adjusted analyses.
Out of the total study population of 1,402 individuals, 1 out of 4 (N = 352) were vaccinated against Influenza. Among the 292 Flu-positive patients, only 39 (13.4%) had received the vaccine, with 33 cases attributed to the Flu-A strain and six to the Flu-B strain.
Given that only one Flu-B case resulted in hospitalization, the hospitalization analysis focused solely on Flu-A cases. Among Flu-A positive patients, 38 required hospitalization, of whom 11 had been vaccinated, representing 28.9% of hospitalized cases. In contrast, among the 190 non-hospitalized Flu-A patients, 22 were vaccinated (11.6%). When analyzing hospitalization rates based on vaccination status, 33.3% (11 out of 33) of vaccinated Flu-A patients were hospitalized, compared to 13.8% (27 out of 195) of non-vaccinated Flu-A patients. This difference was statistically significant, with a p-value of 0.01, indicating, at first glance, that vaccinated individuals had a higher observed higher hospitalization rate than their non-vaccinated counterparts.
Also, the calculated odds ratio of hospitalization,

indicate that, in unadjusted analysis, the vaccinated participants had approximately three times the odds of being hospitalized compared to unvaccinated individuals. However, this association must be interpreted with caution as significant confounding factors, such as age, comorbidities, timing of vaccination, and flu strain mismatch, could be influencing the results.
The data indicate a notable age difference between the two groups, with vaccinated Flu-A patients having a mean age of 70.55 years, while unvaccinated Flu-A patients had a mean age of 46.79 years. This difference is statistically significant (p < 0.001) and is critical to consider since older individuals are inherently more vulnerable to severe disease and hospitalization, regardless of their vaccination status.
Moreover, the prevalence of comorbidities was considerably higher in the vaccinated group. Among vaccinated individuals, 87.9% had at least one comorbidity, compared to only 40.5% in the unvaccinated group (p < 0.001). Specifically, chronic heart disease was present in 69.7% of vaccinated patients versus 28.2% of unvaccinated patients (p < 0.001), while diabetes mellitus affected 27.3% of vaccinated patients compared to just 8.2% of unvaccinated patients (p = 0.004). Given that these conditions independently increase the risk of severe outcomes, their uneven distribution between the two groups could be contributing to the observed difference in hospitalization rates.
The initial unadjusted analysis indicated that the vaccinated participants had 3.11 times higher odds of hospitalization compared to the unvaccinated counterparts. After adjusting for the aforementioned confounding factors using multivariate logistic regression, vaccination status was no longer significantly associated with hospitalization (aOR = 1.178, p = 0.805), indicating that vaccination was not an independent predictor of hospitalization risk. This finding suggests that the initially observed higher hospitalization rate among vaccinated individuals was likely driven by baseline differences in age and health status rather than the effect of vaccination itself. Instead, age, diabetes, pneumonia, and dyspnea emerged as the strongest predictors of hospitalization among FluA-positive patients.
We further calculated the vaccine effectiveness (VE) for Flu-A using the standard formula:

The attack rate in unvaccinated individuals was 0.1857 (18.57%), while the attack rate in vaccinated individuals was 0.0938 (9.38%).

Thus, the unadjusted estimated vaccine effectiveness was 49.5%, suggesting that vaccination was associated with a nearly 50% lower risk of Flu-A infection compared to unvaccinated individuals, indicating a moderate level of protection in our study population. However, this estimate should be interpreted with caution given the observational nature of the data and the potential for residual confounding.
SARS-COV-2
Among SARS-CoV-2 positive patients, 10% (20/196) required hospitalization, with the majority being female. Hospitalized patients were significantly older (79.35 ± 10.51 years, [95% CI: 72.0–85.0]) compared to non-hospitalized patients (60.17 ± 20.31 years, [95% CI: 60.0–69.0], p < 0.001), and almost all (19/20) had at least one comorbidity. Individuals with comorbidities had over 10 times higher odds of hospitalization (OR = 10.17, [95% CI: 1.33–77.78], p = 0.005). Among SARS-CoV-2–positive patients, hospitalization was significantly associated with chronic pulmonary disease (OR = 3.23, [95% CI: 1.17–8.89], p = 0.026), particularly COPD (OR = 6.00, [95% CI: 1.58–22.71]), as well as chronic heart disease (OR = 3.78, [95% CI: 1.21–11.75]; p = 0.017). Hospitalized patients also had a longer symptom duration (5.35 ± 3.35 days, [95% CI: 3.0–8.0]) before seeking medical care compared to non-hospitalized patients (3.04 ± 2.27 days, [95% CI: 2.0–3.0], p = 0.002). Radiological findings, including unilateral consolidative infiltrates, were strongly linked to hospitalization (OR = 87.5, [95% CI: 4.43–1729.99], p < 0.001). Notably, 40% of hospitalized patients had a history of prior SARS-CoV-2 disease, compared to 53.4% of non-hospitalized patients (p = 0.004).
Multivariate binary logistic regression identified age (p = 0.017), longer symptom duration before seeking care (p = 0.020), and dyspnea (p = 0.049) as significant predictors of hospitalization. The overall model was statistically significant (χ²(10) = 51.56, p < 0.001), explained 48.1% of the variance (Nagelkerke R² = 0.481), and showed good fit (Hosmer–Lemeshow p = 0.393).
SARS-COV-2 vaccination
In the study, 76.5% of the total population (1072/1402) were vaccinated against SARS-CoV-2, with most receiving three doses (52.1%), followed by two doses (26.2%) and four or more doses (15.1%). Only 6.5% received one dose. Among SARS-CoV-2 positive patients, 83.2% (163/196) were vaccinated. Of the 20 hospitalized SARS-CoV-2 patients, 18 were vaccinated and 2 unvaccinated, with no significant association between vaccination status and hospital admission (p = 0.537). Vaccination distribution among positive patients included 3.1% with one dose, 12.9% with two doses, 55.8% with three doses, and 28.2% with four or more doses.
Respiratory syncytial virus
Four out of ten RSV patients required hospitalization, with in-patients significantly older (71.3 ± 14.1 years, 95% CI: [66.0–82.0]) than non-hospitalized ones (45.5 ± 20.0 years, 95% CI: [32.0–55.97], p < 0.001). Patients aged 60–74 had 7.5 times higher odds (95% CI: 1.8–30.7, p = 0.005) and those over 75 had 24 times higher odds (95% CI: 4.6-124.9, p < 0.001) of hospitalization. Almost all hospitalized patients had at least one comorbidity, compared to 60% of non-hospitalized patients, with those affected having over four times higher odds of admission (OR = 4.13, 95% CI: [1.17–14.53], p = 0.022). Chronic heart disease, in particular, was strongly associated with hospitalization (OR = 5.40, 95% CI: [1.77–16.47], p < 0.001). None of the patients were vaccinated against RSV.
Multivariate logistic regression identified age (OR = 0.909, p = 0.002,) and fever (OR = 9.959, p = 0.011,) as significant predictors of hospitalization, with febrile patients having nearly 10 times higher odds of hospitalization. The model demonstrated excellent model fit (Omnibus test χ² = 77.703, p < 0.001; Nagelkerke R² = 0.967; Hosmer-Lemeshow test p = 1.000).
Comparative analysis of hospitalized patients with Influenza A, RSV, and SARS-CoV-2
Among hospitalized patients with Influenza A, RSV, and SARS-CoV-2, the average age was over 70, with SARS-CoV-2 patients being slightly older. Most had at least one comorbidity, commonly chronic heart disease. Symptom duration before admission was longest in SARS-CoV-2 cases, though not significantly. Unilateral pneumonia occurred in about 25%, while bilateral pneumonia was more frequent in Influenza A. Respiratory failure affected around half the patients, with conventional oxygen therapy most used. Hospital stays were longest for Influenza A, but differences were not significant. Mortality was low overall, highest in SARS-CoV-2 patients (Table 1.)
The analysis of laboratory findings among hospitalized patients with Influenza A, RSV, and SARS-CoV-2 revealed significant differences in white blood cell (WBC) count and lymphocyte (LYM) count, while C-reactive protein (CRP) levels did not differ significantly, despite higher CRP levels in RSV patients. WBC count was significantly higher in RSV patients compared to Influenza A (p = 0.016). Lymphocyte count varied significantly, with RSV patients having higher counts than Influenza A patients (p = 0.036), while SARS-CoV-2 patients had significantly lower lymphocyte levels than both Influenza A (p = 0.006) and RSV patients (p < 0.001). While lymphocyte counts in Influenza A and RSV remained normal, SARS-CoV-2 patients exhibited significant lymphopenia (Table 1.)
Comparative analysis of Non-Hospitalized patients with Influenza A/B, RSV, and SARS-CoV-2
Non-hospitalized Flu-A patients were significantly older than Flu-B patients (p < 0.001) but had a similar age distribution to RSV patients. SARS-CoV-2 patients were significantly older than Flu-A, Flu-B, and RSV patients (p < 0.001). RSV patients were also significantly older than Flu-B patients (p = 0.006).
SARS-CoV-2 patients had the highest comorbidity burden, with nearly 65% having at least one comorbidity, followed by RSV (60%) and Flu-A (38.9%), while Flu-B had the lowest (28.6%). Chronic heart disease was most common in SARS-CoV-2 patients (51.1%), and RSV patients had the highest rate of chronic lung disease (28.6%). Diabetes was more prevalent in SARS-CoV-2 and Flu-A patients but lower in Flu-B and RSV. RSV patients had the longest symptom duration before seeking medical attention, averaging 4.4 days, significantly longer than Flu-A (p < 0.001), Flu-B (p = 0.045), and SARS- CoV-2 (p < 0.001). Flu-A and Flu-B showed no significant difference, while SARS-CoV-2 symptoms lasted slightly shorter than Flu-B (p = 0.019).
Among the remaining patients, the majority of Flu-A, Flu-B, and SARS-CoV-2 patients experienced symptom relief within 2–5 days. However, RSV cases had a more even distribution between those recovering within 2–5 days and those needing more than 5 days. The overall distribution of symptom resolution time did not differ significantly among virus groups (p = 0.171) (Table 2.)
Discussion
The present study aimed to identify the seasonal patterns of common respiratory viruses in a Greek hospital and highlight their clinical differences and impact on hospitalized and non- hospitalized patients. On the basis of these aims, patients with compatible respiratory symptoms underwent rapid test for Flu-A, Flu-B, RSV, and SARS-CoV-2. 61% (854/1402) of respiratory viral tests in this study were negative, slightly lower than the 67.6% reported by Zimmerman et al.30 but consistent with other studies using PCR tests31,32 supporting the high accuracy of the rapid antigen tests used. The hospitalization rate among patients presenting to the emergency department (ED) with respiratory tract infections (RTIs) was 18%, similar to earlier findings of around 17%33 but higher than the 7.4% reported by Satia et al. (2020)34 possibly due to their separate assessment of COPD and asthma admissions, or the fact that our hospital, as a tertiary referral center, treats more critically ill patients. Hospitalizations were also more frequent among males, consistent with previous studies showing sex-based differences in RTI admissions34.
Additionally, RSV-associated hospitalizations were less frequent than those for influenza, mainly because RSV was rarer (4.4% positivity), in accordance with prior reports, (2.9%−9.1%) by Ambrosch et al31. and 5.91% by Yu et al.32 but higher than the 1.4% reported by Matsumura et al.35. In contrast, the influenza positivity rate was 21%, aligning with findings from Korsun et al.36 for the same season in Bulgaria. However, RSV patients were significantly more likely to be hospitalized than those with Influenza A (43% vs. 17%), likely due to the lack of specific treatments, absence of widespread vaccination, limited immunity, or delayed care-seeking, prompting greater caution for high-risk groups like the elderly. This observation aligns with a study by Falsey et al.37 which showed that RSV positivity was more strongly associated with hospitalization than other viral respiratory infections, and with the investigation of Lemarie et al.38 which found that patients with parainfluenza and RSV, were hospitalized more frequently than those with influenza. The highest hospital mortality was recorded in SARS-CoV-2 patients, possibly due to the older age. Although other studies suggest that the clinical course of respiratory disease is worse in SARS-CoV-2 patients31 the small sample size in this study limits the strength of this conclusion. Notably, while not statistically significant, Influenza A patients in our cohort had a longer mean hospital stay compared to those with RSV or SARS-CoV-2. This trend may in part reflect the occurrence of secondary bacterial pneumonia—a well- documented complication of influenza infection associated with greater morbidity and prolonged recovery39,40. While our dataset does not include information on in-hospital complications beyond mortality, this possibility highlights the potentially more complex clinical course of Influenza A in hospitalized patients.
In our study, the mean age of RSV hospitalized patients was 71 years, younger than those hospitalized with influenza A (76 years) and SARS-CoV-2 (79 years). Surie et al.41 reported a median age of 72 years for RSV patients, while Ackerson et al.42 found RSV patients to be slightly older than those with influenza (78.5 vs. 77.4 years). Ambrosch et al.31 noted that RSV patients were significantly older than those with SARS-CoV-2 (75.1 vs. 70.8 years), while Yu et al. (2024)32 found similar ages for RSV (75.4 years) and influenza (75.7 years). The age distribution of hospitalized patients with RSV, influenza, and SARS-CoV-2 varies across studies, primarily because most studies focus on patients aged 60 and over. The fact that SARS-CoV-2 patients are generally older, with older patients being disproportionately affected in our study as well, raises the question of whether biological aging plays the biggest role in this phenomenon or whether immune aging (immunosenescence) contributes the most. Immunosenescence, characterized by reduced T-cell production, functional exhaustion, and chronic low-grade inflammation (“inflammaging”), delays viral clearance and increases susceptibility to severe SARS-CoV-2 infections in older adults43. Understanding these mechanisms, including changes to the immune cell repertoire, epigenetic factors, NAD + levels, and inflammasome activity, is crucial for developing targeted interventions aimed at mitigating severe lymphopenia and immune dysfunction in high-risk populations44.
Several studies have suggested that RSV-hospitalized patients have worse clinical outcomes than those with COVID-19 or influenza, requiring HFNC and ICU admission more frequently, while the economic burden of RSV is also higher41,42. However, other studies reported no statistically significant differences between RSV and influenza infections in terms of oxygen saturation, ICU admissions, and discharge outcomes32 which aligns with our findings. Notably, the majority of RSV patients (70%) required conventional oxygen therapy (COT), a proportion higher than that observed in COVID-19 (60%) and influenza (50%) patients. In contrast, the need for HFNC was most pronounced among influenza patients (28%), followed by RSV patients (23%), while COVID-19 patients had the lowest requirement at just 10%.
Differentiating RSV, influenza, and SARS-CoV-2 infections can be challenging due to significant symptom overlap. While influenza infections are more likely to present with fever, RSV infections are often non-febrile or present with only a low-grade fever32. In our study, a higher proportion of influenza patients experienced fever (80%) compared to those with RSV (55%) and SARS-CoV-2 (65%), though fever was generally common among hospitalized patients with any of these viral infections. Importantly, our finding that fever strongly predicted hospitalization in RSV-positive adults indicates that fever should be regarded as a clinical marker of greater severity, consistent with reports linking febrile presentations to lower respiratory involvement and increased risk of adverse outcomes45,46,47. Coughing was most prevalent in patients with RSV and least prevalent in those with SARS-CoV-2, in line with the findings of Ambrosch et al.31 and our own study (p < 0.001). Additionally, a characteristic pattern of symptoms in RSV-hospitalized patients was found concerning wheezing, with 57.7% presenting more severe bronchospasm requiring systemic corticosteroids and/or magnesium sulfate, a percentage higher than the 46% noted by Falsey et al.37. This aligns with previous studies reporting that RSV infections are more commonly associated with wheezing symptoms compared to influenza48,49.
Leukocyte levels were elevated in RSV-hospitalized patients compared to those with Influenza A or SARS-CoV-2, as reported by Ambrosch et al.31 and similarly observed in our study. Additionally, the typical laboratory pattern distinguishing these infections in our study was the SARS-CoV-2-related lymphopenia. This finding is more severe and prolonged compared to other viral infections50 as seen in our study, where hospitalized SARS-CoV-2 patients had significantly lower lymphocyte counts than those with influenza or RSV. Unlike common transient lymphopenia seen in most viral infections51 COVID-19-driven lymphopenia, affecting both CD4 + and CD8 + T cells, is linked to poor prognosis and worsened disease severity50,52. Mechanisms contributing to this depletion include the inflammatory cytokine storm, metabolic acidosis, stress hematopoiesis, and apoptosis. Despite low ACE2 expression on T cells, alternative viral entry pathways such as CD147 may facilitate direct infection, further exacerbating immune suppression52.
During the 2023–2024 season, influenza severity was moderate, with activity returning to pre-pandemic levels53. This season was also shorter than previous ones, with positivity above the 10% threshold for 15 weeks compared to 25 weeks in 2022–202354. Our findings align with post-pandemic trends, showing an overall influenza positivity rate of 20.8%, consistent with the reported 15–20% range despite increased testing54. This contrasts with pre-pandemic seasons, where positivity rates were higher (25–32%), suggesting possible shifts in virus circulation, testing practices, or immunity dynamics. Reflecting these seasonal patterns, Flu-A was more prevalent than Flu-B in our dataset, accounting for 78% of cases compared to 22% for Flu-B, consistent with previous studies reporting that Influenza A accounted for 74.9–95.1% of cases across multiple seasons, while Influenza B ranged from 4.9 to 25.1%55.
This higher prevalence of Flu-A is reflected in hospitalization patterns with 38 Flu-A cases requiring admission compared to just one Flu-B case, reinforcing findings that Flu-A leads to more hospitalizations, likely due in part to its higher prevalence55. Additionally, influenza A-related pneumonia (FluA-p) has been associated with increased ICU admissions and mortality56 a trend shown in our data, where 21 FluA-p cases were identified compared to only one FluB-p. These findings emphasize the importance of strain identification in managing severe cases. Data have also shown that most influenza and severe acute respiratory infections (SARI) hospitalizations were Flu-A related and affected those ≥ 60 years old54. Our results mirror this, with over 90% (36/39) of hospitalized influenza patients belonging to this age group. A notable demographic difference emerged, as Flu-A patients were significantly older than Flu-B patients (50.23 ± 20.99 vs. 35.08 ± 16.715, p < 0.001), consistent with prior research55. Meanwhile, symptoms between Flu-A and Flu-B cases were similar56 therefore, subtype surveillance is crucial for monitoring influenza infections, especially in the elderly.
Moreover, our initial unadjusted analysis indicated a higher rate of hospitalization among patients with Influenza A who had received the influenza vaccine. However, this observation warrants careful interpretation. In our cohort, vaccinated individuals were, on average, significantly older and more likely to have underlying comorbidities—both of which are well-recognized risk factors for severe outcomes57,58,59. After adjusting for these confounding variables in a multivariate logistic regression model, vaccination status was no longer independently associated with an increased risk of hospitalization. These findings underscore the importance of accounting for baseline differences when evaluating vaccine effects in observational studies. They should not be taken as evidence questioning the safety or effectiveness of influenza vaccination.
Finally, in line with the seasonal influenza vaccination recommendations in Greece, our study found that 1 in 4 participants were vaccinated, with a vaccine effectiveness (VE) of 49.5% in reducing the risk of Flu-A infection. Vaccine effectiveness can fluctuate from season to season, mainly due to the circulating virus subtype and the degree of antigenic match between the vaccine and the strains in circulation. Recent reports from the 2023–2024 season showed similar protection levels, with interim data from Europe indicating up to 51% protection in primary care settings and 38% in hospital settings54. CDC reported a VE of 42% for the same season, with higher protection in children (52%−61%) compared to adults (41%−44%)53. Studies from the UK have estimated moderate VE, with 40% effectiveness among older adults in England and 53% in Scotland for hospitalization due to laboratory-confirmed influenza60 while other studies reported VE of 39% against hospitalization and 47% against emergency department or urgent care encounters in adults61.
Limitations
As with any study, several limitations should be considered. First, this single-center ED study may introduce selection bias toward more severe cases, limiting generalizability. However, in Greece, primary healthcare (PHC) is often underutilized, and even patients with milder illness commonly seek care directly at hospital EDs. This pattern may partially reduce severity-related selection bias. Previous studies have documented low reliance on public PHC and high rates of ED use for conditions typically manageable in primary care settings62,63. Nonetheless, caution is advised when generalizing to the wider community. Second, although RT-PCR is considered the reference standard for viral detection, we used four CE-certified rapid diagnostic tests (RDTs) that comply with EN ISO 13485:2016. These tests have demonstrated high sensitivity and specificity in prior validation studies64 and are widely implemented in emergency settings, where timely diagnostic information is critical for clinical decision-making, infection control, and resource allocation. While the use of RDTs may carry some risk of misclassification, their strong diagnostic performance and practical advantages support their use in real-world, high-throughput frontline settings. Only symptomatic patients were included, though the focus was on disease severity, not prevalence. Data on influenza treatment and antibiotic use were not collected, though most influenza cases likely received Oseltamivir and hospitalized patients received antibiotics, underscoring the value of pathogen identification. Co-infections may have been missed, as testing was limited to rapid diagnostics. This exclusion, while methodologically justified, may underrepresent the full spectrum of respiratory illness severity. Statistical correction for multiple comparisons was not applied due to the study’s exploratory nature; however, findings were interpreted cautiously in light of this limitation. Finally, stratification of Influenza A cases by subtype (e.g., H1N1 vs. H3N2) was not feasible. While we acknowledge that subtype-specific analysis could have provided additional epidemiological insight, our primary aim was to explore broader clinical patterns, symptomatology, and vaccine effectiveness. Within this scope, we believe that analysis based on overall Influenza A data still offers meaningful and informative conclusions.
Clinical and Public Health Implications
Our findings carry important clinical and public health implications. The high hospitalization rates among older adults with RSV infection emphasize the growing need for awareness and preventive strategies, particularly as newly approved RSV vaccines become available for this age group. The consistent association of lymphopenia with SARS-CoV-2 infection reinforces its value as a useful marker for both diagnosis and risk stratification in clinical settings. Likewise, the frequent occurrence of pneumonia in Influenza A cases highlights the ongoing importance of timely vaccination and prompt antiviral treatment, especially for those at increased risk of complications. Collectively, these observations point to the need for more targeted approaches to prevention, early detection, and management of respiratory viral infections—efforts that are essential to reducing the burden on individuals and healthcare systems alike.
Conclusion
In conclusion, to our knowledge, this is the first large-scale Greek real-world cohort study of adults focusing on the association between viral types, illness severity, and clinical outcomes, offering valuable insights into everyday healthcare settings. By including diverse patient populations with varying comorbidities and vaccination statuses, this study assessed disease burden and diagnostic effectiveness, which is essential for shaping healthcare strategies, improving diagnostic protocols, and enhancing patient care, particularly as we adapt to new vaccination approaches post-COVID-19. While the observational design limits causal inference, the findings highlight important clinical patterns, including the vulnerability of older adults with RSV and moderate vaccine effectiveness against Influenza A. The observed association between vaccination and hospitalization was likely driven by confounding and should not be interpreted as evidence of reduced vaccine benefit.
Methods
Study design and setting
This cross-sectional study was conducted at the Emergency Department (ED) and the Respiratory Medicine Department of the University Hospital of Larissa (UHL). The study period spanned from October 16, 2023, to March 31, 2024, covering all on-call days (i.e., every second day) during the winter season of 2023–2024.
Patient recruitment and data collection
Nasopharyngeal samples were systematically collected from all patients presenting respiratory infection symptoms upon arrival at the ED. These symptoms included fever, fatigue, myalgias/arthralgias, cough, sputum production, sore throat, runny nose, headache, and dyspnea within the preceding 10 days. A clinician’s assessment was required to confirm that the illness was attributable to an infectious process.
Samples underwent antigen testing for the detection of four pathogens: Influenza A/B, SARS-CoV-2, Respiratory Syncytial Virus (RSV), and Adenovirus. Validated antigen tests, benchmarked against the gold-standard reverse transcription polymerase chain reaction (RT-PCR)64 were utilized. To enhance efficiency, a streamlined specimen collection method was introduced, requiring a single swab instead of four separate samples for the detection of all targeted pathogens.
Demographic and clinical data were obtained through patient interviews and medical records, including in-hospital outcomes observed during hospitalization. Among 1,434 patients who presented with respiratory infection symptoms and underwent antigen testing, 1,402 were included in the study. Thirty-two patients (< 2.3%) were excluded due to test results indicating coinfection with RSV, SARS-CoV-2, or influenza, or due to missing in-hospital outcome data. These cases were excluded from the relevant analyses. (Fig. 4.)

Flowchart illustrating the patient enrollment process and follow-up. Excluded data include incomplete data/questionnaires and viral coinfections.
Patient monitoring and hospitalization criteria
Patients were monitored based on their clinical needs, with hospitalization decisions following international guidelines according to the severity of the clinical presentation. Although a single, standardized criterion was not universally applied, hospital admissions were generally based on a combination of clinical considerations. These included: (1) symptoms of respiratory distress (e.g., dyspnea, hypoxia), (2) abnormal vital signs (e.g., tachypnea, hypotension, oxygen desaturation), (3) presence of significant comorbidities (such as heart failure, chronic lung disease, or immunosuppression), (4) altered mental status, (5) persistent or worsening symptoms, and (6) the need for close monitoring or supportive care that could not be adequately provided in an outpatient setting. For hospitalized patients, additional data were collected, including laboratory findings, clinical signs (such as wheezing or respiratory failure), therapeutic interventions (including drug administration and oxygen therapy), length of hospital stay, and disease outcomes. Non-hospitalized patients received follow-up phone calls 10 days after their ED visit to assess symptom resolution.
Inclusion and ethical considerations
Inclusion criteria required the presence of respiratory infection symptoms within the preceding 10 days, adulthood, and the provision of written informed consent. The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of the University of Thessaly on October 16, 2023. Written informed consent was obtained from all participants prior to their inclusion in the study.
Principle of assay
The rapid diagnostic tests (RDTs) used in this study detect viral antigens through an immunochromatographic lateral flow assay. Antibodies specific to viral proteins are applied to the test line of a nitrocellulose membrane. During testing, viral antigens in the specimen interact with antibodies conjugated to gold nanoparticles. As the sample migrates upward through the membrane, it reacts with immobilized antibodies, producing a visible colored line in the test region, indicating a positive result. A control line appears to confirm test validity. Results are interpreted after 15min.
Rapid test technology has significantly improved since the COVID-19 pandemic, not only for SARS-CoV-2 but also for other respiratory viruses, increasing their reliability compared to previous years65,66. The four RDTs used were manufactured by PROGNOSIS BIOTECH S.A. (Larissa, Greece) and comply with EN ISO 13485:2016. These tests have demonstrated high sensitivity and specificity in previous studies: Flu-A/B test: sensitivity 91.15%, specificity 98.96%, Adenovirus test: sensitivity 92.45%, specificity 99.32%, RSV test: sensitivity 92.59%, specificity 99.47%, SARS-CoV-2 test: sensitivity 100.00%, specificity 99.74%. These results affirm the reliability of these tests for diagnosing infections, making them valuable for clinical decision-making.
Statistical analysis
Data analysis was performed using Microsoft Excel 2019 (Microsoft Corporation, Redmond, WA, USA) and IBM SPSS Statistics version 26 (IBM Corporation, Chicago, IL, USA). Prior to further analysis, the normality of continuous variables was assessed using the Kolmogorov-Smirnov test. Continuous variables were presented as means and standard deviations (SD) to maintain consistency in reporting. Depending on the distribution of the data, appropriate statistical tests were applied; nonparametric tests were used when normality assumptions were not met. For categorical variables, the chi-square (χ²) test or Fisher’s exact test was used, as appropriate. A P-value of < 0.05 was considered statistically significant.
In addition, logistic regression analysis was conducted to evaluate the association between key independent variables and the binary outcome variable of hospitalization. Variables with a P-value < 0.05 in univariate analysis were included in the multivariable logistic regression model. Adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were reported to determine the strength and direction of associations. To assess model adequacy, the Hosmer-Lemeshow goodness-of-fit test was used to evaluate the fit of the logistic regression models. Post hoc pairwise comparisons between virus groups were performed following ANOVA. Although no formal correction for multiple comparisons was applied, results were interpreted cautiously given the study’s exploratory nature. Effect sizes with 95% confidence intervals were consistently reported alongside p-values to improve transparency and interpretability.
Data availability
The data that support the findings of this study are available on request from the corresponding author.
References
Hu, T. et al. Economic burden and secondary complications of influenza-related hospitalization among adults in the US: a retrospective cohort study. J. Med. Econ. 27, 324–336 (2024).
Immunity following influenza disease and administration of influenza vaccines. European Centre for Disease Prevention and Control. (2024)., March 27 https://www.ecdc.europa.eu/en/seasonal-influenza/prevention-and-control/vaccines/immunity
World Health Organization: WHO & World Health Organization: WHO. Influenza (seasonal). (2025)., February 28 https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal).
Flu Burden. https://www.cdc.gov/flu-burden/php/about/index.html 5. About estimated flu burden et al. Understanding the Global Burden of Influenza in Adults Aged 18–64 years: A Systematic Literature Review from 2012 to 2022. Advances in Therapy vol. 40 4166–4188 Preprint at (2024)., November 13 https://doi.org/10.1007/s12325-023-02610-1 (2023).
Maleki, F. et al. Understanding the Global Burden of Influenza in Adults Aged 18–64 years: A Systematic Literature Review from 2012 to 2022. Advances in Therapy vol. 40 4166–4188 Preprint at (2023). https://doi.org/10.1007/s12325-023-02610-1
Rousogianni, E. et al. Proportions and seasonal patterns of respiratory viruses via rapid tests in adults at a Greek hospital. J Pers. Med 14,8 824. https://doi.org/10.3390/jpm14080824 (2024).
Overview of Respiratory Virus Epidemiology in the EU/EEA, Week 12, 2025. (2025).
Morbidity and Mortality Weekly Report (MMWR) Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices-United States, 2024-25 Influenza Season. https://www.fda.gov/advisory-committees/advisory-committee-calendar/vaccines-and-related-biological-products-
Falsey, A. R., Hennessey, P. A., Formica, M. A., Cox, C. & Walsh, E. E. Respiratory Syncytial Virus Infection in Elderly and High-Risk Adults. www.nejm.org (2005).
Alfano, F., Bigoni, T., Caggiano, F. P. & Papi, A. Respiratory Syncytial Virus Infection in Older Adults: An Update. Drugs and Aging vol. 41 487–505 Preprint at (2024). https://doi.org/10.1007/s40266-024-01118-9
Havers, F. P. et al. Morbidity and Mortality Weekly Report (MMWR) Characteristics and Outcomes Among Adults Aged ≥ 60 Years Hospitalized with Laboratory-Confirmed Respiratory Syncytial Virus-RSV-NET. https://stacks.cdc.gov/view/cdc/133296
Vega-Piris, L. et al. Severity of respiratory syncytial virus compared with SARS-CoV-2 and influenza among hospitalised adults ≥ 65 years. Journal Infection, 89,5 , 106292. https://doi.org/10.1016/j.jinf.2024.106292 (2024).
RSV in older adults. (2024, August 30). Respiratory Syncytial Virus Infection (RSV). https://www.cdc.gov/rsv/older-adults/index.html
La, E. M. et al. Respiratory syncytial virus knowledge, attitudes, and perceptions among adults in the united States. Hum Vaccin Immunother 20,1 , 2303796. https://doi.org/10.1080/21645515.2024.2303796 (2024).
The Lancet Respiratory Medicine. Respiratory syncytial virus vaccines: the future is bright. The Lancet Respiratory Medicine vol. 12 499 Preprint at (2024). https://doi.org/10.1016/S2213-2600(24)00184-X
Rousogianni, E., Perlepe, G., Boutlas, S., Papagiannis, D. & Gourgoulianis, K. I. Letter to the Editor Regarding the Article by Karami et al. on the Surveillance of Endemic Coronaviruses During the COVID-19 Pandemic in Iran, 2021–2022. Influenza and other Respiratory Viruses vol. 18 Preprint at (2024). https://doi.org/10.1111/irv.70001
Corman, V. M., Muth, D., Niemeyer, D. & Drosten, C. Hosts and Sources of Endemic Human Coronaviruses. in Advances in Virus Research vol. 100 163–188Academic Press Inc., (2018).
Sarker, R., Roknuzzaman, A. S. M., Hossain, M. J., Bhuiyan, M. A. & Islam, M. R. The WHO declares COVID-19 is no longer a public health emergency of international concern: benefits, challenges, and necessary precautions to come back to normal life. Int. J. Surg. 109, 2851–2852 (2023).
COVID-19 cases | WHO COVID-19 dashboard. (n.d.). Datadot. https://data.who.int/dashboards/covid19/cases.
Lamers, M. M. & Haagmans, B. L. SARS-CoV-2 pathogenesis. Nature Reviews Microbiology vol. 20 270–284 Preprint at (2022). https://doi.org/10.1038/s41579-022-00713-0
Staying Up to Date with COVID-19 Vaccines. ( January 7). COVID-19. (2025). https://www.cdc.gov/covid/vaccines/stay-up-to-date.html. 22. World Health Organization Europe.
World Health Organization, W. H. O. October 23). Vaccines for the vulnerable: new WHO/Europe study shows the impact of COVID-19 vaccines in safeguarding health and saving lives. World Health Organization: WHO. (2024). https://www.who.int/europe/news/item/23-10-2024-vaccines-for-the-vulnerable--new-who-europe-study-shows-the-impact-of-covid-19-vaccines-in-safeguarding-health-and-saving-lives.
Radke, J. R. & Cook, J. L. Human adenovirus infections: Update and consideration of mechanisms of viral persistence. Current Opinion in Infectious Diseases vol. 31 251–256 Preprint at (2018). https://doi.org/10.1097/QCO.0000000000000451
Shen, K., Wang, Y., Li, P. & Su, X. Clinical features, treatment and outcomes of an outbreak of type 7 adenovirus pneumonia in centralized residence young adults. Journal Clin. Virology, 154 105244. https://doi.org/10.1016/j.jcv.2022.105244 (2022).
European Centre for Disease Prevention and Control Acute Respiratory Infections in the EU/EEA (2024): Epidemiological Update and Current Public Health Recommendations. Available at: https://erviss.org/. (Accessed: 15 July 2025).
Golpour, M. et al. Co-infection of SARS-CoV‐2 and influenza A/B among patients with COVID-19: a systematic review and meta-analysis. BMC Infectious Diseases vol. 25 Preprint at (2025). https://doi.org/10.1186/s12879-025-10521-5
Contes, K. M., Liu, B. M. & Epidemiology Clinical Significance, and Diagnosis of Respiratory Viruses and Their Co-Infections in the Post-COVID Era. Pathogens vol. 14 Preprint at (2025). https://doi.org/10.3390/pathogens14030262
Rodríguez, J. P. & Eguíluz, V. M. Coupling between infectious diseases leads to synchronization of their dynamics. Chaos, 33, 2 , 021103. https://doi.org/10.1063/5.0137380 (2023).
Eales, O. et al. Key challenges for respiratory virus surveillance while transitioning out of acute phase of COVID-19, Emerging infectious diseases 30,2 e230768. https://doi.org/10.3201/eid3002.230768 (2024).
Zimmerman, R. K. et al. Population-based hospitalization burden estimates for respiratory viruses, 2015–2019. Influenza Other Respir Viruses. 16, 1133–1140 (2022).
Andreas, A., Doris, L., Frank, K. & Michael, K. Focusing on severe infections with the respiratory syncytial virus (RSV) in adults: risk factors, symptomatology and clinical course compared to influenza A / B and the original SARS-CoV-2 strain. Journal Clin. Virology, 161 105399. https://doi.org/10.1016/j.jcv.2023.105399 (2023).
Yu, J. et al. Comparative study on the epidemiological characteristics and hazards of respiratory syncytial virus and influenza virus infections among elderly people. BMC Infect. Dis. 24, 1129 (2024).
Hossain, F. B., Muscatello, D., Jayasinghe, S. & Liu, B. Trends in hospitalisations for vaccine preventable respiratory infections following emergency department presentations in new South wales, australia, 2012–2022. Influenza Other Respir Viruses, 18, 10, e70015. https://doi.org/10.1111/irv.70015 (2024).
Satia, I. et al. Influence of age, sex and respiratory viruses on the rates of emergency department visits and hospitalisations with respiratory tract infections, asthma and COPD. https://doi.org/10.1183/23120541.00053
Matsumura, Y. et al. Epidemiology of respiratory viruses according to age group, 2023–24 winter season, kyoto, Japan. Sci Rep, 15,1 924. https://doi.org/10.1038/s41598-024-85068-7 (2025).
Korsun, N. et al. Etiological Spectrum of Acute Respiratory Infections in Bulgaria During the 2023–2024 Season and Genetic Diversity of Circulating Influenza Viruses. Viruses 17, (2025).
Falsey, A. R. et al. Respiratory syncytial virus and other respiratory viral infections in older adults with moderate to severe influenza-like illness. J. Infect. Dis. 209, 1873–1881 (2014).
Lemarie, B. et al. Predictors of hospitalization and superinfection in viral respiratory tract infections between influenza and paramyxoviruses: the SUPERFLUOUS study. J. Infect. Dis. 226, 1027–1035 (2022).
Morris, D. E., Cleary, D. W. & Clarke, S. C. Secondary bacterial infections associated with influenza pandemics. Frontiers in Microbiology vol. 8 Preprint at (2017). https://doi.org/10.3389/fmicb.2017.01041
MacIntyre, C. R. et al. The role of pneumonia and secondary bacterial infection in fatal and serious outcomes of pandemic influenza a(H1N1)pdm09. BMC Infect. Dis, 18,1 637. https://doi.org/10.1186/s12879-018-3548-0 (2018).
Surie, D. et al. Disease Severity of Respiratory Syncytial Virus Compared with COVID-19 and Influenza Among Hospitalized Adults Aged ≥ 60 Years — IVY Network, 20 U.S. States, February 2022–May 2023. vol. 6 (2023). https://www.cdc.gov/flu/vaccines-work/ivy.htm
Ackerson, B. et al. Severe morbidity and mortality associated with respiratory syncytial virus versus influenza infection in hospitalized older adults. Clin. Infect. Dis. 69, 197–203 (2019).
Zhang, S. et al. Are older people really more susceptible to SARSCoV-2? Aging Dis. 13, 1336–1347 (2022).
Mueller, A. L. & McNamara, M. S., Sinclair DA. Why does COVID-19 disproportionately affect older people? Aging (Albany NY). doi: 10.18632/aging.103344. Epub 2020 May 29. PMID: 32470948; PMCID: PMC7288963 (2020).
Fistera, D. et al. Adult patients with severe respiratory syncytial virus infections in the emergency department. Med. (United States). 103, e39265 (2024).
Clausen, C. L. et al. Clinical manifestations and outcomes in adults hospitalized with respiratory syncytial virus and influenza a/b: A multicenter observational cohort study. Open Forum Infect. Dis, 11,10, ofae513.https://doi.org/10.1093/ofid/ofae513 (2024).
Rozenbaum, M. H. et al. Incidence of Respiratory Syncytial Virus Infection in Older Adults: Limitations of Current Data. Infectious Diseases and Therapy vol. 12 1487–1504 Preprint at (2023). https://doi.org/10.1007/s40121-023-00802-4
Rello, J. & Sabater-Riera, J. Challenges in Respiratory Syncytial Virus in Adults With Severe Community-acquired Pneumonia. Chest vol. 161 1434–1435 Preprint at (2022). https://doi.org/10.1016/j.chest.2022.01.050
Wildenbeest, J. G., Lowe, D. M., Standing, J. F. & Butler, C. C. Respiratory syncytial virus infections in adults: a narrative review. Lancet Respir Med. https://doi.org/10.1016/s2213-2600(24)00255-8 (2024).
Zhang, S., Asquith, B., Szydlo, R., Tregoning, J. S. & Pollock, K. M. Peripheral T cell lymphopenia in COVID-19: potential mechanisms and impact. Immunotherapy Advances vol. 1 Preprint at (2021). https://doi.org/10.1093/immadv/ltab015
Guo, Z., Zhang, Z., Prajapati, M. & Li, Y. Lymphopenia caused by virus infections and the mechanisms beyond. Viruses vol. 13 Preprint at (2021). https://doi.org/10.3390/v13091876
Shouman, S. et al. SARS-CoV-2-associated lymphopenia: possible mechanisms and the role of CD147. Cell Communication and Signaling vol. 22 Preprint at (2024). https://doi.org/10.1186/s12964-024-01718-3
2023–2024 Influenza season Summary: Influenza severity Assessment, burden and burden Prevented. (2024, November 22). Influenza (Flu). https://www.cdc.gov/flu/whats-new/flu-summary-addendum-2023-2024.html
Seasonal influenza - Annual Epidemiological Report for 2023/2024. European Centre for Disease Prevention and Control. (2024)., November 21 https://www.ecdc.europa.eu/en/publications-data/seasonal-influenza-annual-epidemiological-report-20232024
Sharma, Y., Horwood, C., Hakendorf, P. & Thompson, C. Clinical characteristics and outcomes of influenza A and B virus infection in adult Australian hospitalised patients. BMC Infect. Dis, 20,1 913. https://doi.org/10.1186/s12879-020-05670-8 (2020).
Chen, L., Han, X., Di, Li, Y. L., Zhang, C. X. & Xing, X. Q. Severity and outcomes of influenza-related pneumonia in type A and B strains in China, 2013–2019. Infectious Diseases of Poverty vol. 9 Preprint at (2020). https://doi.org/10.1186/s40249-020-00655-w
People at increased risk for flu complications (2024) Centers for Disease Control and Prevention. Available at: (2025). https://www.cdc.gov/flu/highrisk/index.htm(Accessed: 15 July).
Cui, C., Timbrook, T. T., Polacek, C., Heins, Z. & Rosenthal, N. A. Disease burden and high-risk populations for complications in patients with acute respiratory infections: a scoping review. Frontiers in Medicine vol. 11 Preprint at (2024). https://doi.org/10.3389/fmed.2024.1325236
Branche, A., Ramesh, M. & Francis, B. A. Narrative Review of Key Risk Factors for Severe Illness Following SARS-CoV-2, Influenza Virus, and Respiratory Syncytial Virus Infection. Infectious Diseases and Therapy vol. 14 39–61 Preprint at (2025). https://doi.org/10.1007/s40121-024-01081-3
Whitaker, H. et al. Interim 2023/2024 season influenza vaccine effectiveness in primary and secondary care in the united Kingdom. Influenza Other Respir Viruses, 18,5 e13284. https://doi.org/10.1111/irv.13284 (2024).
Tenforde, M. W. et al. Influenza vaccine effectiveness against hospitalizations and emergency department or urgent care encounters for children, adolescents, and adults during the 2023–2024 season, united States. Clin. Infect. Dis. https://doi.org/10.1093/cid/ciae597 (2024).
Oikonomou, N. & Tountas, Y. Insufficient Primary Care Services to the Rural Population of Greece. (2011). http://www.rrh.org.au
Re-Profiling Emergency Medical Services in Greece Assesment Report (2017) World Health Organization. Available at: http://www.euro.who.int/pubrequest(Accessed: 15 July 2025).
Papagiannis, D. et al. Proportion of Respiratory Syncytial Virus, SARS-CoV-2, Influenza A/B, and Adenovirus Cases via Rapid Tests in the Community during Winter 2023—A Cross Sectional Study. Diseases 11, (2023).
Rosenblatt, K. P., Romeu, H., Romeu, C. & Granger, E. Performance evaluation of a SARS-CoV-2 and influenza A/B combo rapid antigen test. Front Mol. Biosci, 111308202. https://doi.org/10.3389/fmolb.2024.1308202 (2024).
Bernstein, D. I., Mejias, A., Rath, B., Woods, C. W. & Deeter, J. P. Diagnostic accuracy of commercially available tests for respiratory syncytial virus: A scoping literature review in the COVID-19 era. Preprint at (2022). https://doi.org/10.1101/2022.02.14.22270927
Acknowledgements
The authors express their gratitude to the patients who participated in the study. The authors also extend their appreciation to the Emergency Department of the University Hospital of Larissa, with special thanks to Georgia Papadamou and Irene Poulakida, for their exceptional support. Additionally, the authors acknowledge PROGNOSIS BIOTECH S.A. for providing rapid tests.
Author information
Authors and Affiliations
Contributions
Conception and Design: D.P. and K.I.G.; Data collection, E.R., S.B., G.R., E.G., E.M., G.M.; Data analysis, Er.R, E.R., D.P.; Materials and Resources, K.I.G.; Manuscript Writing, E.R., G.P.; Critical Revision, G.P., Er.R, D.P., A.E., K.I.G.; Visualization, E.R., Er.R.; Project Administration: D.P., K.I.G.All authors reviewed and approved the final version of the manuscript. All authors agree to be accountable for all aspects of the work, ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of the University of Thessaly (registration number 48757, approved on 16 October 2023). Written informed consent was obtained from patients.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Rousogianni, E., Perlepe, G., Boutlas, S. et al. Clinical features and outcomes of viral respiratory infections in adults during the 2023–2024 winter season. Sci Rep 15, 35800 (2025). https://doi.org/10.1038/s41598-025-19236-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-19236-8
