
Abstract
The enzyme vanin-1 produces pantothenic acid (PA) and cysteamine, but the role of the vanin-1 /PA axis in metabolic and cardiovascular diseases remains less explored than the vanin-1 /cysteamine pathway. This study investigated the relationship between vanin-1 and PA with obesity, type-2 diabetes (T2D), and related cardiovascular complications (CVD). We found that patients with T2D, with or without CVD, had significantly lower plasma PA levels, which negatively correlated with glycemic markers and positively with HDL cholesterol. Individuals in the lowest PA tertile exhibited a markedly higher prevalence of T2D (76.6%). While vanin-1 levels did not significantly differ between groups, a trend towards higher levels in T2D was observed, and higher vanin-1 correlated with higher HbA1c, with the highest vanin-1 tertile showing a greater proportion of T2D (62.5%). Importantly, low PA levels were significantly associated with increased odds of T2D in patients with obesity (OR = 7.61) and increased odds of diabetes with CVD in both patients with and without obesity (OR = 12.03, OR = 7.24, respectively). In contrast, high vanin-1 was not associated with increased odds. Our findings suggest that low PA levels may serve as a potential biomarker for T2D and T2D with CVD. Future research should investigate the impact of vanin-1 modulation on PA levels and the therapeutic potential of PA supplementation in managing these conditions.
Similar content being viewed by others

Introduction
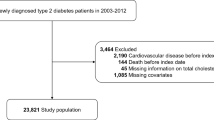
Diabetes mellitus (DM) is a chronic metabolic disorder characterized by persistent hyperglycemia, which arises from impaired insulin secretion, diminished insulin action, or a combination of both mechanisms1. The prevalence of DM is rapidly increasing worldwide, paralleling the alarming rise in obesity rates. Both conditions have reached epidemic proportions, significantly impacting public health and clinical outcomes2,3.Notably, at least half of individuals with diabetes and obesity face a heightened risk of developing cardiovascular diseases (CVD). This condition contributes to a significant portion of their mortality, estimated to be between one-third to one-half4,5. These concerning statistics underscore the urgent need for effective management strategies to prevent diabetes-related cardiovascular complications, beyond merely achieving glycemic control to delay the onset of these outcomes6.
Vascular non-inflammatory molecule-1 (vanin-1) is a membrane-bound enzyme with pantetheinase activity, catalyzing the hydrolysis of pantetheine to produce pantothenic acid (vitamin B5, PA) and cysteamine7. Elevated levels of vanin-1 have been associated with increased risks of diabetes, obesity, and coronary artery disease8,9,10. Recent investigations have illuminated vanin-1’s role in oxidative stress regulation, particularly its influence on glutathione (GSH) levels, positioning it as a critical player in redox homeostasis11. Notably, high concentrations of cysteamine can inhibit γ-glutamylcysteine synthetase (γ-GCS), leading to depleted intracellular GSH stores and exacerbating oxidative stress-related conditions12,13. Conversely, PA is believed to exert antioxidant effects by promoting GSH synthesis and enhancing coenzyme A (CoA) availability, thereby mitigating oxidative stress14,15,16. The differing effects of vanin-1’s downstream products have created ambiguity regarding its involvement in various diseases, particularly as research has predominantly focused on the vanin-1/cysteamine pathway while neglecting the vanin-1/PA axis (Fig. 1, Schematic overview of vanin-1’s role in disease).

Schematic overview of vanin-1’s role in disease. CoA, coenzyme A; γ-GCS, γ- glutamylcysteine synthetase; GSH, glutathione.
Numerous studies have demonstrated diverse associations between PA levels and diabetes17,18,19,20. Experimental evidence supports that PA and its precursor, dexpanthenol, exhibit protective properties across various tissues due to their anti-inflammatory, antioxidant, and anti-apoptotic effects21,22,23. Crucially, these compounds have shown promise in safeguarding cardiac function against the adverse effects of diabetes and preserving pancreatic β-cell integrity in the face of oxidative stress24,25. While direct clinical data is scant, emerging data suggest a link between low PA levels and cardiovascular diseases; for instance, lower plasma PA levels have been reported in patients with coronary heart disease26. Furthermore, pantethine treatment (a PA derivative) showed efficacy in lowering cardiovascular disease risk markers such as total cholesterol and low-density lipoprotein cholesterol (LDL-C) in patients with low to moderate CVD risk27. The relationship between PA and obesity is complex; while some studies indicate that higher PA intake may reduce obesity risk, others suggest an association with increased obesity likelihood28,29.
In this study, we aim to evaluate the biomarker potential of vanin-1 and PA together in the context of obesity, type-2 diabetes, and diabetes-related cardiovascular complications. By investigating both markers simultaneously, we seek to elucidate their combined roles in metabolic health and to identify potential therapeutic targets for managing these interconnected conditions, addressing a significant gap in the literature where prior research has typically focused on one of these factors in isolation.
Methods
Study design and setting
This cross-sectional case-control study was performed between November 2022 and March 2023 at the Department of Internal Medicine of Zagazig University Hospitals. The study protocol was approved by the faculty of medicine of Zagazig University institutional review board (approval number 9350-23-2-2022) before subjects enrollment. The study was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki. Each participant gave informed consent before their inclusion in the study. Our study consists of four groups (35 subjects each): healthy controls, patients with obesity without diabetes, patients with diabetes, and patients with diabetes with cardiovascular disease (CVD).
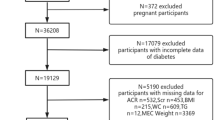
Patients with diabetes, and patients with diabetes with CVD were recruited from diabetes and endocrine inpatient unit and the cardiology unit, respectively, while healthy controls and patients with obesity without diabetes were recruited voluntarily from the general population through local advertisements and word of mouth. Our study exclusion criteria were age less than 18 years old or more than 65 years old, pregnancy, type 1 diabetes, malignant tumors, severe renal dysfunction (defined as estimated glomerular filtration rate < 15 mL/min/1.73 m2), and history of chronic liver disease.
Diabetes was defined as a fasting plasma glucose level of ≥ 126 mg/dL or HbA1c of ≥ 48 mmol/mol according to American Diabetes Association criteria30 or on current treatment with insulin and/or oral hypoglycemic agents. Myocardial ischemia was defined as presenting with acute coronary syndrome (ACS) or a history of stable or unstable angina, which was confirmed by a cardiac enzyme test, ECG, and echocardiography. Heart failure was defined as a history of chronic heart failure confirmed by Natriuretic Peptide Tests (BNP), ECG, and Echocardiography. Cardiomyopathy was defined as a history of early stage left ventricular remodeling and diastolic dysfunction preceding overt heart failure, confirmed by Natriuretic Peptide Tests (BNP), ECG, and Echocardiography. Obesity was defined as BMI > 30 kg/m2.
Data collection
We used case record forms completed by trained medical professionals to collect detailed information on each subject’s medical history, smoking habits, and medications intake. Medical histories were documented based on thorough clinical evaluations, diagnostic findings from patient records, and structured interviews. Weight and height were recorded, and body mass index (BMI, kg/m²) was calculated. Demographic data and laboratory values were retrieved from the hospital medical records; We used the data within 1 week of the sample collection. Fasting blood glucose was measured after an overnight fast of at least 8 h, and postprandial blood glucose was measured 2 h after a standardized meal using venous blood samples analyzed in the hospital’s central laboratory.
Blood sample collection and biomarkers analysis
Blood samples of all participants were collected in a heparin-coated tube after fasting for 8 h. Samples were centrifuged at 6000 rpm for 15 min at room temperature, plasma was divided into four Eppendorf tubes and kept at -80 until analysis. Vanin-1 plasma levels were measured using commercially available enzyme-linked immunosorbent assay Kits (ELISA) ((FineTest®, China) which has a reported sensitivity of 0.094 ng/mL and demonstrate high specificity, with no significant cross-reactivity or interference with related analogues. The intra- and inter-assay coefficients of variation (CVs) were < 8% and < 10%, respectively. PA level was measured using commercially available ELISA kits ((BT Lab bioassay, China) with a sensitivity of 10.96 ng/mL, with intra- and inter-assay CVs also reported to be < 8% and < 10%, respectively. Reduced Glutathione (GSH) was measured using a commercial colorimetric kit (Elabscience, USA). Malondialdehyde (MDA) level was measured using the thiobarbituric acid test method with a commercial colorimetric kit (Biodiagnostic, Egypt). All assays were performed following the manufacturers’ instructions.
Statistical analysis
All statistical analyses were performed using SPSS for Windows software (ver. 25). Continuous variables were expressed as a mean \(\:\pm\:\) standard deviation or median (Interquartile range), while categorical variables were expressed as the number and percentage (%). The normal distribution of the continuous variables was tested using the Shapiro–Wilk test before deciding the appropriate statistical test. For parametric variables, one-way ANOVA with the Fisher’s Least Significant Difference (LSD) post hoc test was used to evaluate the difference between the groups. For nonparametric variables (vanin-1, PA, GSH, MDA, and Triglycerides levels), the Kruskal Wallis test followed by pairwise comparison was used to evaluate the difference between the groups. The chi-square test (X2) and Montecarlo exact test were used for categorical variables. The correlations between variables were examined using Spearman’s correlation test. We performed multinomial logistic regression analysis adjusted for age, sex, and BMI to calculate Odds ratios (ORs) and their corresponding 95% CIs to investigate the association of plasma vanin-1 and PA levels with the development of diabetes, diabetes cardiovascular complications, and obesity. The tertiles of vanin-1 levels and PA of the subjects included in the study were used to classify these subjects into three groups. We considered subjects in the vanin-1 third tertile (vanin-1 level > 1.574 ng/mL) to have a high vanin-1 level, and subjects in the PA first tertile (PA level < 850.27 ng/ml) to have a low PA level. Differences with p < 0.05 were considered statistically significant.
Results
Patient characteristics and anthropometric data
The clinical and anthropometric characteristics of the study are summarized in Table 1. No significant differences were observed among the groups with respect to demographic data. However, a statistically significant difference in BMI was noted, with the control group exhibiting the lowest BMI. The diabetes groups demonstrated significantly elevated levels of HbA1c, fasting blood glucose, postprandial blood glucose, and triglycerides, alongside notably lower levels of HDL cholesterol. No significant differences were found between the groups regarding total cholesterol, LDL cholesterol, or MDA levels. Among the patients with cardiovascular diseases, 62.5% had ischemic heart disease, including acute coronary syndrome and stable angina (n = 20), 28.2% had chronic heart failure (n = 9), and 9.3% had cardiomyopathy (n = 3).
Low pantothenic acid levels represent a biomarker in diabetes
Plasma PA levels were significantly lower in patients with diabetes with CVD compared to both healthy controls and individuals with obesity. Additionally, PA levels in the diabetes group were lower than those in the control group (p = 0.05), as illustrated in Fig. 2a. To further elucidate the relationship between PA and other clinical parameters, we conducted a correlation analysis (Supplementary Table S1). A statistically significant negative correlation was observed between PA and HbA1c (r = -0.318, p = 0.0003) (Fig. 2b), fasting blood glucose (r = -0.304, p = 0.0005) (Fig. 2d), and postprandial blood glucose (r = -0.284, p = 0.0012) (Fig. 2e). Conversely, a significant positive correlation was found between PA and HDL cholesterol (r = 0.194, p = 0.03) (Fig. 2c). Notably, 76.6% (n = 23) of the subjects in the lowest tertile of pantothenic acid (n = 30) were diagnosed with diabetes (Fig. 2f). These findings suggest that higher PA levels are associated with favorable metabolic markers, while lower PA levels correlate with adverse diabetes-related indicators.

Pantothenic acid levels are reduced in diabetes. a, Comparison between the studied groups regarding serum pantothenic acid, data are expressed as the mean and standard deviation. b, Correlation between plasma pantothenic acid and glycated hemoglobin. c, Correlation between plasma pantothenic acid and fasting blood glucose. d, Correlation between plasma pantothenic acid and postprandial blood glucose. e, Correlation between plasma pantothenic acid and HDL-cholesterol, r Spearman rank correlation coefficient. f, Study participants distribution within pantothenic acid Q1 tertile (< 850.27 ng/ml).
Vanin-1 levels show a trend toward elevation in diabetes
While vanin-1 levels did not vary significantly across the groups, there was a noticeable trend toward higher levels in the diabetes cohorts (Fig. 3a). To further investigate the role of vanin-1 in diabetes, we conducted a correlation analysis with the studied parameters (Supplementary Table S2). This analysis revealed a significant positive correlation between plasma vanin-1 and HbA1c (r = 0.2, p = 0.023) (Fig. 3b). Notably, the prevalence of diabetes in the highest tertile of vanin-1 (n = 32) was 62.5% (n = 20) (Fig. 3e).

High Vanin-1 levels are dominant in diabetes. a, Comparison between the studied groups regarding plasma vanin-1, data are expressed as the mean and standard deviation. b, Correlation between plasma vanin-1 and glycated hemoglobin, r Spearman rank correlation coefficient. c, Comparison between the studied groups regarding serum Vanin-1 in vanin-1 Q3 tertile, data are expressed as the mean and standard deviation. d, Correlation between plasma vanin-1 and glycated hemoglobin in vanin-1 Q3 tertile, r Spearman rank correlation coefficient. e, study participants distribution within vanin-1 Q3 tertile (> 1.574 ng/ml).
When comparing plasma vanin-1 levels among different study groups within the third tertile (> 1.574 ng/mL), patients with diabetes exhibited a trend toward elevated vanin-1 levels (Fig. 3c). In this tertile, vanin-1 demonstrated a stronger positive correlation with HbA1c (r = 0.451, p = 0.01) (Fig. 3d).
Oxidative stress markers show no significant differences across groups
Plasma levels of glutathione (GSH) and malondialdehyde (MDA) showed no statistically significant differences across the study groups (Table 1). Additionally, GSH showed no significant correlations with PA (Supplementary Table S1) or vanin-1 (Supplementary Table S2), except for a positive correlation with MDA (r = 0.223, p = 0.011) (Supplementary Table S3). Similarly, MDA showed no significant correlations with either PA (Supplementary Table S1) or vanin-1 (Supplementary Table S2).
Low PA levels are associated with increased odds of obesity and diabetes
To assess the relationship between vanin-1, PA, and the odds of diabetes and related cardiovascular diseases, we conducted a multinomial logistic regression analysis (Table 2). Our findings revealed that low PA levels (< 850.27 ng/mL) were significantly associated with an increased odds of diabetes in patients with obesity (OR = 7.610, 95% CI = 1.37–42.05, p = 0.02). Additionally, low PA levels correlated with a higher odds of diabetes with cardiovascular disease (CVD) in both patients with/without obesity (OR = 7.237, 95% CI = 1.11–47.19, p = 0.038 for non-obese; OR = 12.028, 95% CI = 2.23–64.76, p = 0.004 for obese). In contrast, high vanin-1 levels did not demonstrate an association with increased odds for any of the conditions studied.
Diabetes medications do not impact plasma vanin-1/PA levels
To evaluate the impact of various diabetes medications on vanin-1 and PA levels, we performed a binary logistic regression analysis (Supplementary Table S4). The results indicated that neither insulin therapy nor oral hypoglycemic agents were associated with decreased vanin-1 levels or increased PA levels. However, these findings should be interpreted with caution due to the small sample size and the possibility of polypharmacotherapy for most of the subjects; further large-scale studies are needed to draw more definitive conclusions.
Discussion
To the best of our knowledge, there are few clinical studies that have investigated the association between vanin-1, PA, and diabetes along with its cardiovascular complications. Our findings indicate that patients with diabetes with cardiovascular comorbidities exhibit the lowest plasma levels of PA, and similarly low levels are observed in patients with diabetes overall. Furthermore, we identified a significant negative correlation between PA levels and various glycemic markers, with glycated hemoglobin demonstrating the strongest association. This suggests a potential link between reduced PA levels and glucose intolerance.
Notably, low PA levels were associated with a seven-fold increased likelihood of diabetes in patients with obesity, and an increased probability of diabetes with cardiovascular disease in both patients with (12-fold) and without obesity (7-fold). The striking prevalence of diabetes (76.6%) among subjects with low plasma PA levels further reinforces the association between reduced PA and diabetes, regardless of cardiovascular complications. It is worth noting that we further stratified diabetes based on obesity status since obesity is a common and metabolically significant comorbidity in diabetes, and its presence may influence both PA levels and their associations with different disease status. By analyzing patients with diabetes with and without obesity as separate subgroups, we aimed to explore potential differences in PA-related metabolic patterns, which may reflect distinct pathophysiological mechanisms. This approach provides a more refined understanding of PA’s relevance across varying metabolic profiles and may support future stratified therapeutic strategies.
The oxidative stress markers, GSH and MDA did not show significant differences across study groups or consistent correlations with vanin-1 or PA. These findings suggest that, within the context of our study population and measured parameters, systemic levels of GSH and MDA may not be the primary mediators of the observed associations between PA and diabetes with/ without CVD.
Our findings show lower PA levels in patients with diabetes with CVD compared to individuals with obesity, however, we did not observe a statistically significant difference in PA levels between the patients with obesity and patients with diabetes without CVD. The common metabolic and inflammatory state in obesity and diabetes might similarly suppress PA levels, obscuring group-level differences. Notably, the lower PA levels observed in diabetes with CVD group suggest a potential independent effect of CVD because of the additive influence of systemic chronic inflammation, endothelial dysfunction, or pharmacological treatments of CVD that alter PA levels.
In line with our findings, Gulle et al.25 demonstrated that dexpanthenol, a precursor to PA, alleviated diabetes-induced pancreatic damage and inflammation in rats, highlighting its antioxidant and potential antihyperglycemic properties. Also, a metabolomics study in China subsequently identified significantly lower levels of PA in patients with diabetes with nephropathy compared to patients with diabetes without complications18. Additionally, vanin-1-deficient animals displayed increased susceptibility to diabetes, suggesting impaired vanin-1 function may compromise tissue stress tolerance through reduced PA regeneration31,32,33. However, contrasting results emerged from Gogna et al., who found higher PA levels in patients with obesity with type 2 diabetes17. This discrepancy may be attributed to ethnic variations, as their study focused solely on South Indian Asian patients with diabetes.
In addition to its potential link to diabetes, PA may also play a protective role against cardiovascular complications associated with the condition. Supporting this hypothesis, Gulle et al. demonstrated that dexpanthenol could help prevent cardiovascular issues in diabetes by protecting endothelial function and reducing oxidative stress in a streptozotocin model of diabetes25. Similarly, Kalkan et al. showed that dexpanthenol administration significantly mitigated cardiac damage, improved ECG abnormalities, and lowered oxidative stress in a myocardial infarction model34. Recent studies have further confirmed the cardioprotective properties of vitamin B5 across various cardiac injury models by reducing oxidative stress and inflammation35,36. Consistent with our findings, a study from China reported that higher plasma levels of PA were linked to a lower incidence of coronary heart disease10. However, a conflicting study found a correlation between higher PA intake and increased coronary calcification scores in diabetes patients with chronic kidney disease37. However, they did not measure serum PA levels.
Regarding vanin-1, our findings indicated no significant differences in plasma levels among the study groups, though a trend toward higher levels was observed in patients with diabetes. Notably, vanin-1 levels demonstrated a stronger positive correlation with HbA1c in the highest tertile compared to the correlation in the whole dataset, as indicated by a higher correlation coefficient, suggesting a potential link between elevated vanin-1 and impaired glucose tolerance. However, we did not find an association between high vanin-1 levels and increased odds of obesity, diabetes, or diabetes with CVD. Supporting our findings, Küçük et al. reported higher serum vanin-1 levels in diabetes patients compared to those without diabetes, with a positive correlation to the insulin resistance index (HOMA-IR)8. Similarly, Hosohata et al. observed that the individuals with higher urinary vanin-1 had significantly higher HbA1c and plasma glucose levels38. Mosaad et al. reported a significant correlation between vanin-1 gene expression and HbA1c level9; however, our study assessed vanin-1 protein levels. Other studies did not find a significant correlation between vanin-1 and fasting blood glucose10 or HbA1c levels8,10.
These observations align with preclinical data indicating that vanin-1 serum levels are elevated in diabetes animal models. Specifically, knocking down vanin-1 in the liver alleviated insulin resistance and impaired glucose tolerance39. Mechanistically, vanin-1 may contribute to these issues by activating gluconeogenesis through the Akt signaling pathway39,40. However, while some studies noted increased vanin-1 activity in diabetic models, the absence of vanin-1 resulted in only mild improvements in glucose tolerance and insulin sensitivity41. Pharmacological inhibition of vanin-1 using RR6 also did not significantly affect insulin sensitivity or fasting blood glucose levels42,43. Interestingly, in models of vanin-1 deficiency, mice exhibited worsened insulin resistance and glucose tolerance. Yet, restoring vanin-1 activity in white adipose tissue significantly mitigated these effects, and enhancing vanin-1 expression in brown adipose tissue produced similar benefits40,44. The variability in findings across studies may stem from differences in assessing vanin-1 activity, suggesting that its effects on diabetes may be tissue-specific.
We did not find any previous studies examining the role of vanin-1 in cardiovascular complications of diabetes. However, there are some reports on the role of vanin-1 in cardiovascular diseases and cardiovascular disease risk factors. A recent study reported that patients with coronary artery disease had elevated plasma vanin-1 concentrations, which were linked to both the presence and severity of coronary artery disease10. Furthermore, vanin-1 deficiency leads to substantially reduced neointima formation following carotid artery ligation in animals45. Wedel et al.46 further confirmed these findings, they found that vanin-1 inhibition diminished the formation of neointima after aortic allografts, primarily by decreasing oxidative stress. Altogether, vanin-1 has an atherosclerotic effect, increasing the risk of cardiovascular diseases. Also, vanin-1 showed a positive correlation with several cardiovascular risk factors including waist circumference, BMI, and carotid intima-media thickness8.
Our present understanding of the vanin-1/PA role in metabolic diseases is ambiguous. As evident from our present study, this unclear understanding may arise from the differential role of vanin-1 and PA in diabetes and its associated CVD. While PA seems to be protective against these conditions, vanin-1 might have an unfavorable effect in these conditions. Moreover, previous studies have focused on the vanin-1/cysteamine arm of the pathway, which is thought to create a state of disease induction through participating in oxidative stress7, this perspective overlooked the vanin-1/ PA arm of the pathway which might hold promise in optimizing diabetes and its associated CVD management.
An intriguing finding of our study is the tendency for increased vanin-1 concentration alongside lower PA levels in diabetes. Given that vanin-1 catabolizes pantetheine to both PA and cysteamine, this apparent discrepancy suggests a more complex regulation of the pathway in diabetes. One possible explanation is a shift in the relative production of vanin-1 downstream products, potentially favoring cysteamine over PA. Preclinical studies have shown that cysteamine levels and vanin-1 activity can be elevated in certain disease states associated with oxidative stress, which is often increased in diabetes9,12,13. Additionally, altered Pantetheine availability due to alteration in Coenzyme A (CoA) metabolism in diabetes47, of which pantetheine is an intermediate, might contribute to low PA levels, since even with slightly increased vanin-1 activity, the net production of PA might still be reduced. Although current clinical studies directly addressing these mechanisms are limited, our findings underscore the need for future studies to simultaneously measure PA, cysteamine, pantetheine, and vanin-1 to provide a more comprehensive understanding of this complex pathway in the context of diabetes and its cardiovascular complications.
The primary contribution of this study is the investigation of associations between marker levels and various disease states as allowed by the cross-sectional case-control design of the study, thereby generating hypotheses for future research. However, this study has several limitations. First, the sample size in each group is relatively small. Second, the cross-sectional nature of the study limits our ability to establish causality and exclude the potential reverse causation between biomarkers and diseases, highlighting the need for larger interventional studies. Third, our study lacks a comparison group of patients with CVD without diabetes; the inclusion of such a group wasn’t feasible within the scope of our study due to ethical approval considerations. There is a crucial direction for future research to include such a group, with the necessary ethical approvals, to further elucidate the interplay between diabetes, CVD, and the investigated biomarkers. Additionally, we recognize that the lack of cysteamine measurements limits our ability to definitively determine the relative contributions of PA and cysteamine to the observed associations and to fully support the hypothesis of a dichotomic role of vanin-1. However, our decision to focus solely on PA levels was primarily was influenced by several factors (i) existing literature has indeed focused on the vanin-1/cysteamine axis, particularly its role in oxidative stress., while the vanin-1/PA pathway is often-overlooked ; (ii) we measured glutathione (GSH) levels, a key marker influenced by cysteamine, and found no significant differences in its level across our study groups or significant correlations with vanin-1, suggesting that the vanin-1/cysteamine axis might not be the primary driver of the associations observed; and (ii) our primary research question centered on the biomarker potential of PA in these conditions.
Future studies should prioritize the simultaneous measurement of both PA and cysteamine, alongside relevant markers of oxidative stress like GSH, to gain a more comprehensive understanding of the vanin-1 pathway’s role in metabolic and cardiovascular diseases and to fully explore the potential for a dichotomic mechanism. Lastly, as the study exclusively included Egyptian patients, further investigation is required to determine whether these findings are generalizable to other populations.
Conclusions
In conclusion, this study highlights the significant association between low PA levels and the presence of diabetes, particularly in patients with cardiovascular complications. Our findings suggest that PA may serve as a potential biomarker for diabetes and its related conditions, with lower levels correlating with higher glycemic markers and a greater odds of diabetes in both individuals with and without obesity. While vanin-1 levels did not show significant differences between groups, a trend towards higher levels in patients with diabetes was observed, indicating a possible link to impaired glucose tolerance. These results underscore the need for further research to explore the mechanisms underlying the roles of PA and vanin-1 in diabetes and cardiovascular health, as well as to assess the generalizability of our findings across diverse populations. Future studies should aim to elucidate the clinical implications of PA supplementation and vanin-1 inhibition as potential therapeutic strategies in managing diabetes and its complications.
Data availability
All data generated or analyzed during this study are included in this published article and the supplementary material.
Abbreviations
- DM:
-
Diabetes mellitus
- CVD:
-
Cardiovascular diseases
- vanin-1:
-
Vascular non-inflammatory molecule-1
- GSH:
-
Reduced glutathione
- γ-GCS:
-
γ-glutamylcysteine synthetase
- CoA:
-
Coenzyme A
- BNP:
-
Natriuretic Peptide Tests
- BMI:
-
Body mass index
- ELISA:
-
Enzyme-linked immunosorbent assay Kits
- MDA:
-
Malondialdehyde
- PA:
-
Pantothenic acid
- ORs:
-
Odds ratios
- HDL:
-
High-density lipoprotein cholesterol
- LDL:
-
Low-density lipoprotein cholesterol
- HbA1c:
-
Glycated hemoglobin
- ECG:
-
Electrocardiogram
- HOMA-IR:
-
Insulin resistance index
References
Petersmann, A. et al. Definition, classification and diagnosis of diabetes mellitus. Exp. Clin. Endocrinol. Diabetes. 127, S1–S7 (2019).
International Diabetes Federation. IDF Diabetes Atlas 10th edn (International Diabetes Federation, 2021).
Tim, L., Rachel, J. L., Jaynaide, P., Hannah, B. & Maggie, G. World Obesity Atlas 2023 (World Obesity Federation, 2023).
Einarson, T. R., Acs, A., Ludwig, C. & Panton, U. H. Prevalence of cardiovascular disease in type 2 diabetes: a systematic literature review of scientific evidence from across the world in 2007–2017. Cardiovasc. Diabetol. 17, 83 (2018).
International Diabetes Federation. IDF Diabetes Atlas 9th edn (International Diabetes Federation, 2019).
Ma, C. X. et al. Cardiovascular disease in type 2 diabetes mellitus: progress toward personalized management. Cardiovasc. Diabetol. 21, 74 (2022).
Yu, H. et al. Vanin1 (VNN1) in chronic diseases: future directions for targeted therapy. Eur. J. Pharmacol. 962, 176220 (2024).
Küçük, Ş. D., Gezer, E., Çalan, M. & Yüksel, A. Relationship between serum Vanin 1 level and metabolic parameters in patients with type 2 diabetes mellitus. Int. J. Diabetes Dev. Ctries. 43, 801–806 (2023).
Mosaad, Y. O. et al. Vanin 1 gene role in modulation of iNOS/MCP-1/TGF-β1 signaling pathway in obese diabetic patients. J. Inflamm. Res. 15, 6745–6759 (2022).
Kishimoto, Y., Saita, E., Ohmori, R., Kondo, K. & Momiyama, Y. High plasma concentrations of vanin-1 in patients with coronary artery disease. Heart Vessels. 39, 10–17 (2024).
Bartucci, R., Salvati, A., Olinga, P. & Boersma, Y. L. Vanin 1: its physiological function and role in diseases. Int. J. Mol. Sci. 20, 3891 (2019).
Kavian, N. et al. Imbalance of the Vanin-1 pathway in systemic sclerosis. J. Immunol. 197, 3326–3335 (2016).
Kang, M. et al. VNN1, a potential biomarker for pancreatic cancer-associated new-onset diabetes, aggravates paraneoplastic islet dysfunction by increasing oxidative stress. Cancer Lett. 373, 241–250 (2016).
Jung, S., Kim, M. K. & Choi, B. Y. The long-term relationship between dietary pantothenic acid (vitamin B(5)) intake and C-reactive protein concentration in adults aged 40 years and older. Nutr. Metab. Cardiovasc. Dis. 27, 806–816 (2017).
Wojtczak, L. & Slyshenkov, V. S. Protection by pantothenic acid against apoptosis and cell damage by oxygen free radicals—the role of glutathione. Biofactors 17, 61–73 (2003).
Slyshenkov, V. S., Dymkowska, D. & Wojtczak, L. Pantothenic acid and Pantothenol increase biosynthesis of glutathione by boosting cell energetics. FEBS Lett. 569, 169–172 (2004).
Gogna, N., Krishna, M., Oommen, A. M. & Dorai, K. Investigating correlations in the altered metabolic profiles of obese and diabetic subjects in a South Indian Asian population using an NMR-based metabolomic approach. Mol. Biosyst. 11, 595–606 (2015).
Ma, T. et al. UPLC-MS-based urine nontargeted metabolic profiling identifies dysregulation of pantothenate and coa biosynthesis pathway in diabetic kidney disease. Life Sci. 258, 118160 (2020).
Tian, M. et al. Serum metabolites as an indicator of developing gestational diabetes mellitus later in the pregnancy: a prospective cohort of a Chinese population. J. Diabetes Res. 2021, 8885954 (2021).
Ma, L. et al. Relationship between Circulating metabolites and diabetic retinopathy: a two-sample Mendelian randomization analysis. Sci. Rep. 14, 4964 (2024).
Üremiş, M. M., Gürel, E., Aslan, M. & Taşlıdere, E. Dexpanthenol protects against nicotine-induced kidney injury by reducing oxidative stress and apoptosis through activation of the AKT/Nrf2/HO-1 pathway. Naunyn Schmiedebergs Arch. Pharmacol. 397, 1105–1114 (2024).
Zhao, X., Zhang, S. & Shao, H. Dexpanthenol attenuates inflammatory damage and apoptosis in kidney and liver tissues of septic mice. Bioengineered 13, 11625–11635 (2022).
Shin, J. Y. et al. Dexpanthenol promotes cell growth by preventing cell senescence and apoptosis in cultured human hair follicle cells. Curr. Issues Mol. Biol. 43, 1361–1373 (2021).
Demirci, B., Demir, O., Dost, T. & Birincioglu, M. Protective effect of vitamin B5 (dexpanthenol) on cardiovascular damage induced by Streptozocin in rats. Bratisl Lek Listy. 115, 190–196 (2014).
Gulle, K., Ceri, N. G., Akpolat, M., Arasli, M. & Demirci, B. The effects of dexpanthenol in streptozotocin-induced diabetic rats: histological, histochemical and immunological evidences. Histol. Histopathol. 29, 1305–1313 (2014).
Sun, P. et al. Association between plasma vitamin B5 and coronary heart disease: results from a case-control study. Front. Cardiovasc. Med. 9, 906232 (2022).
Evans, M. et al. Pantethine, a derivative of vitamin B5, favorably alters total, LDL and non-HDL cholesterol in low to moderate cardiovascular risk subjects eligible for Statin therapy: a triple-blinded placebo and diet-controlled investigation. Vasc Health Risk Manag. 10, 89–100 (2014).
Gholamalizadeh, M. et al. Index of nutritional quality (INQ) and the risk of obesity in male adolescents: a case-control study. Biol. Trace Elem. Res. 199, 1701–1706 (2021).
Taleban, R. et al. Is dietary vitamin B intake associated with weight disorders in children and adolescents? The weight disorders survey of the CASPIAN-IV study. Health Promot Perspect. 9, 299–306 (2019).
Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 20, 1183–1197 (1997).
Roisin-Bouffay, C. et al. Mouse vanin-1 is cytoprotective for islet beta cells and regulates the development of type 1 diabetes. Diabetologia 51, 1192–1201 (2008).
Naquet, P., Pitari, G., Duprè, S. & Galland, F. Role of the Vnn1 Pantetheinase in tissue tolerance to stress. Biochem. Soc. Trans. 42, 1094–1100 (2014).
Miallot, R., Millet, V., Galland, F. & Naquet, P. The vitamin B5/coenzyme A axis: a target for immunomodulation? Eur. J. Immunol. 53, e2350435 (2023).
Kalkan, F. et al. Protective and therapeutic effects of dexpanthenol on isoproterenol-induced cardiac damage in rats. J. Cell. Biochem. 119, 7479–7489 (2018).
Yildiz, A. et al. Protective effects of dexpanthenol in carbon tetrachloride-induced myocardial toxicity in rats. Tissue Cell. 77, 101824 (2022).
Ozcan, M. S. et al. Dexpanthenol ameliorates lipopolysaccharide-induced cardiovascular toxicity by regulating the IL-6/HIF1alpha/VEGF pathway. Heliyon 10, e24007 (2024).
Machado, A. D. et al. Association between dietary intake and coronary artery calcification in non-dialysis chronic kidney disease: the PROGREDIR study. Nutrients 10, 372 (2018).
Hosohata, K. et al. Urinary vanin-1 associated with chronic kidney disease in hypertensive patients: a pilot study. J. Clin. Hypertens. (Greenwich). 22, 1458–1465 (2020).
Chen, S. et al. Vanin-1 is a key activator for hepatic gluconeogenesis. Diabetes 63, 2073–2085 (2014).
Chen, S. et al. Systemic nanoparticle-mediated delivery of Pantetheinase vanin-1 regulates lipolysis and adiposity in abdominal white adipose tissue. Adv. Sci. (Weinh). 7, 2000542 (2020).
van Diepen, J. A. et al. Genetic and Pharmacological Inhibition of vanin-1 activity in animal models of type 2 diabetes. Sci. Rep. 6, 21906 (2016).
Jansen, P. A. et al. Discovery of small molecule Vanin inhibitors: new tools to study metabolism and disease. ACS Chem. Biol. 8, 530–534 (2013).
van Diepen, J. A. et al. PPAR-alpha dependent regulation of vanin-1 mediates hepatic lipid metabolism. J. Hepatol. 61, 366–372 (2014).
Sun, C. et al. Brown adipose Vanin-1 is required for the maintenance of mitochondrial homeostasis and prevents diet-induced metabolic dysfunction. Mol. Metab. 80, 101884 (2024).
Dammanahalli, K. J., Stevens, S. & Terkeltaub, R. Vanin-1 Pantetheinase drives smooth muscle cell activation in post-arterial injury neointimal hyperplasia. PLoS One. 7, e39106 (2012).
Wedel, J. et al. Pharmacological Inhibition of Vanin activity attenuates transplant vasculopathy in rat aortic allografts. Transplantation 100, 1656–1666 (2016).
Jackowski, S. & Leonardi, R. Deregulated coenzyme A, loss of metabolic flexibility and diabetes. Biochem. Soc. Trans. 42, 1118–1122 (2014).
Funding
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB). This paper is based upon work supported by Science, Technology & Innovation Funding Authority (STDF) under grant number 46040.
Author information
Authors and Affiliations
Contributions
Hany M. El-Bassossy, Mayada M. Mousa, and Mahmoud H. Elbatreek designed the study. Nada K. Shoura and Mahmoud H. Elbatreek carried out the measurements. Nada K. Shoura , Hany M. El-Bassossy, Mayada M. Mousa, Mahmoud H. Elbatreek, and Omar Y. El-Azzazy analyzed and interpreted the data. Nada K. Shoura drafted the original manuscript. All the authors have revised and approved the final manuscript before submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study protocol received approval from the institutional review board of the faculty of medicine of Zagazig University (approval number 9350-23-2-2022) and was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki. Each participant gave informed consent before their inclusion in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shoura, N.K., Elbatreek, M.H., Mousa, M.M. et al. Biomarker potential of vanin-1-derived pantothenic acid in diabetes and its associated cardiovascular complications. Sci Rep 15, 32549 (2025). https://doi.org/10.1038/s41598-025-19271-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-19271-5
