
Abstract
Antenatal depression is a commonly overlooked mental health condition that affects many women during pregnancy, often more severely than after childbirth. It presents with emotional distress and cognitive difficulties such as poor memory and concentration. Addressing this issue is vital, as it impacts not only the mother’s well-being but also the healthy development of her child. This study aims to assess the prevalence of antenatal depression and the factors contributing to it. A cross-sectional study was conducted on 363 pregnant women using the Beck Depression Inventory. Data were collected from February 1 to March 21, 2020, using a systematic random sampling method. Statistical analysis was performed using SPSS version 25, applying binary logistic regression to identify factors significantly associated with antenatal depression at a 95% confidence level. The prevalence of antenatal depression was found to be 22%, and factors such as marital status, education level, and lack of social support were associated with it. This result revealed that the prevalence of antenatal depression was 22%. This highlights the need for routine depression screening during ANC and strengthening psychosocial support services, particularly for women with unplanned pregnancies and limited social support.
Similar content being viewed by others


Introduction
Depression is a common mental health disorder characterized by persistent sadness, loss of interest, feelings of guilt, and low self-esteem. It ranks among the top three causes of global disease burden and is particularly disabling for women across their life course1,2. One specific form, antenatal depression (AD), occurs during pregnancy and is marked by emotional disturbances such as poor concentration, fatigue, and mood changes lasting more than two weeks. This condition is often underrecognized, despite its significant implications for maternal and child health3.
Pregnancy is often viewed as a time of joy and anticipation. However, many women, especially in resource-limited settings, experience substantial physiological, psychological, and social changes during this period, which may increase their vulnerability to emotional distress4. Global studies report that 15% to 65% of pregnant women may experience symptoms of depression5,6. If left untreated, antenatal depression can affect a woman’s ability to function, strain relationships, disrupt fetal development, reduce antenatal care attendance, and even increase the risk of postnatal depression and infant mortality7,8,9,10,11.
In Ethiopia, maternal mental health remains a neglected area within reproductive health services. Although national and regional efforts have improved maternal care, mental health, particularly during pregnancy, has not been adequately prioritized. Studies conducted across various parts of the country report the prevalence of antenatal depression ranging between 15.2% and 35.4%11,12,13,14,15. However, much of this evidence is concentrated in urban or central settings, leaving many rural areas under-researched.
The Beck Depression Inventory (BDI) captures a broader range of cognitive and somatic symptoms of depression, whereas the Edinburgh Postnatal Depression Scale (EPDS) is designed specifically to emphasize perinatal emotional symptoms. These differences in focus contribute to variations in prevalence estimates reported across studies.
To understand AD in its local context, it is helpful to consider social stress theory and biopsychosocial models, which emphasize the role of socio-demographic, psychological, and environmental stressors in shaping mental health outcomes during pregnancy. These frameworks guide this study in identifying both individual- and community-level risk factors16.
Although several studies in Ethiopia have reported antenatal depression, most are concentrated in urban or central areas. Little is known about rural settings such as East Gojjam Zone, where socio-cultural and economic contexts may uniquely influence maternal mental health.
Methods
Study design, setting, and period
A facility-based cross-sectional study was conducted from February 1 to March 21, 2020, at Shegaw Motta General Hospital, located in Motta town, East Gojjam Zone, Amhara Region, Ethiopia. Motta is situated approximately 371 km northwest of Addis Ababa, the capital city of Ethiopia, and about 120 km southeast of Bahir Dar, the regional capital. The town has one government health center, one general hospital, and five private clinics. According to local estimates, Motta has a total population of 37,504, comprising 18,606 males and 18,898 females. Among the female population, 14,278 are of reproductive age. Shegaw Motta General Hospital provides health services to over 25,000 people and delivers antenatal care (ANC) to more than 400 pregnant women each month.
Population
The source population comprised all pregnant women attending ANC services at Shegaw Motta General Hospital. Women with a self-reported history of depression were included because the study aimed to assess both current and recurrent depressive symptoms. However, pregnant women who were critically ill at the time of data collection were excluded from the study.
Sample size determination
The sample was determined using the first and second objectives.
The required sample size was determined using a single population proportion formula by taking a p-value of 23%17, 95% confidence level, 5% margin of error, and adding a 10% non-response rate.
The formula to determine the sample size was.
Then the sample became 370 after adding a 10% non-response rate.
For the second objective factor17, as shown in the table below, was calculated using Epi Info software version 7 by considering the following assumptions: confidence level of 95%, power of 80%, and exposure to the unexposed ratio of 1 (Table 1).
After adding a 10% non-response rate, the final sample size became 370, and being a housewife was the determining factor of the sample size from the second objective.
Sampling procedure
A systematic random sampling technique was employed to select the study participants. According to the most recent two-month report from the ANC registration book, a total of 830 pregnant women attended ANC services at the facility. The sampling frame included all eligible pregnant women attending ANC during the study period.
To begin, the first participant was selected using the lottery method from among the first three attendees on the initial day of data collection. Subsequently, participants were selected at a regular interval for every third attendee (k = N/n = 830/370 ≈ 2.24, rounded to 3), where N represents the total population and n denotes the required sample size. This process continued in sequence according to the order of arrival for ANC follow-up until the desired sample size was achieved.
Measurements and operational definition
The dependent variable in this study was AD. It was defined as a BDI score ≥ 17, indicating moderate to severe depressive symptoms. Independent variables included socio-demographic characteristics, obstetric factors, substance use, and psychosocial attributes. AD was assessed using the BDI, a widely used standardized screening tool for depressive symptoms. The BDI consists of 21 items, each rated on a 4-point Likert scale, with total scores ranging from 0 to 63. The tool has demonstrated strong internal consistency in various populations, with Cronbach’s alpha ranging from 0.85 to 0.9018. In the current study, the Amharic-translated version of the BDI was pretested, and the reliability yielded a Cronbach’s alpha of 0.87, indicating high internal consistency.
Data collection tools and procedures
Data were collected using a face-to-face interviewer-administered questionnaire that was pretested for clarity and reliability. The BDI was translated into Amharic using a forward and backward translation process to ensure linguistic and conceptual equivalence. The Amharic version was then pilot-tested in a similar population, demonstrating acceptable validity and reliability for this study. The questionnaire also included items on socio-demographic characteristics, obstetric history, substance use, and psychosocial factors. Two diploma-level midwives served as data collectors, supervised by two BSc-level midwives who ensured data quality.
Data quality control
Data quality assurance measures were implemented before, during, and after data collection. The questionnaire was initially developed in English, translated into Amharic, and subsequently back-translated into English to ensure semantic consistency. A pretest was conducted on 19 participants at Bichena Hospital, a facility not included in the main study, to evaluate the questionnaire’s clarity, appropriateness, and reliability. Based on the pretest findings, revisions and adjustments were made to enhance the tool’s validity. Additionally, a one-day training session was provided to data collectors and supervisors, emphasizing a clear understanding of the research objectives, sampling procedures, and the ethical responsibilities of the research team, as guided by the principal investigator.
Data processing and analysis
After coding and verifying for completeness, the data were entered into EpiData version 4.2 and subsequently exported to SPSS version 25 for statistical analysis. Descriptive statistics were used to summarize the independent variables. To examine the association between AD and the explanatory variables, binary logistic regression analysis was conducted. Variables with a p-value ≤ 0.25 in the bivariate analysis were considered for inclusion in the multivariable logistic regression model. We controlled for potential confounders such as socioeconomic status and obstetric history in the multivariable logistic regression model. While this threshold is more liberal than the conventional p < 0.05, it was chosen to reduce the risk of omitting potentially important variables at the exploratory stage, as recommended in certain epidemiological studies. Logistic regression assumptions were carefully checked before analysis. Model fit was evaluated using the Hosmer-Lemeshow goodness-of-fit test (p = 0.17), suggesting an acceptable fit. However, we acknowledge that this test only assesses overall calibration. Future studies may consider additional model evaluation tools such as the Receiver Operating Characteristic curve and Area Under the Curve to better assess model discrimination. Statistical significance in the final model was declared at p < 0.05, and adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were reported.
Ethical consideration
Ethical approval
for this study was obtained from the Institutional Review Board (IRB) of Bahir Dar University, College of Medicine and Health Sciences, per the Declaration of Helsinki. Before data collection, formal permission letters were secured from the relevant health authorities. All participants were thoroughly informed about the purpose, objectives, and potential benefits of the study. Written informed consent was obtained from each participant, and confidentiality of the information provided was strictly maintained throughout the study process.
Results
Socio-demographic characteristics of respondents
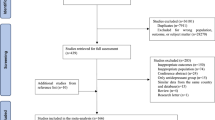
Out of the 370 eligible respondents, 363 participated, yielding a response rate of 98.1%. The mean age of the participants was 25 years (SD ± 6.25). The majority, 254 (70%), resided in urban areas, and 109 (30%) were housewives. Nearly all participants, 355 (97.8%), identified as Amhara by ethnicity. Regarding educational status, 77 (21.2%) had attained only primary education. In terms of economic status, 130 participants (35.8%) reported an average monthly income of less than 2,000 Ethiopian Birr (Table 2).
Obstetric characteristics of respondents
Among the respondents, 106 (29.2%) were primigravida. Nearly one-third, 32 (12.5%), reported a history of preterm birth. Additionally, 63 (17.4%) of the women experienced complications during their most recent pregnancy (Table 3).
Psychosocial and substance use characteristics of respondents
A total of 41 (11.3%) respondents reported a previous history of depression, while 31 (8.5%) indicated a family history of depression. Approximately half of the respondents, 188 (50.8%), reported having social support. Additionally, 69 (19%) of the participants had experienced stressful life events. Substance use was reported by only 12 (3.3%) of the respondents (Table 4).
Prevalence of antenatal depression
The overall prevalence of AD was 22% with 95% CI (17.75–26.32). Out of the total, tiredness 289(79.6%) and loss of energy 268(73.8%) were the most reported symptoms in the antenatal period (Table 5).
Factors associated with antenatal depression
In the multivariable analysis, marital status [AOR = 3.87, 95% CI: 1.87–7.99], educational status [AOR = 4.44, 95% CI: 1.79–11.00], history of medical problems [AOR = 3.35, 95% CI: 1.44–7.83], previous history of depression [AOR = 2.60, 95% CI: 1.11–6.10], lack of social support [AOR = 3.82, 95% CI: 1.96–7.45], and unplanned pregnancy [AOR = 3.79, 95% CI: 1.91–7.56] were significantly associated with antenatal depression (Table 6).
Discussion
The prevalence of depression in our study was 22%, compared to 24.5% in Northeast Ethiopia12 and 23% in Gondar17, Hawassa (21.5%)19, North India (21%)20, and Brazil (21.1%) [21. However, the observed prevalence was lower than that reported in Maichew (31.1%)21, Adama Hospital (31.2%)22, Saudi Arabia (31.9%)23, and Bangalore (35.7%)5. These discrepancies may be attributed to several contextual factors, including variations in cultural beliefs, socioeconomic status, and healthcare accessibility. For example, in settings like Saudi Arabia and Bangalore, different cultural expectations and limited mental health integration into antenatal services may contribute to higher AD rates. Methodological differences also play a role; unlike our study, which used the BDI, other studies employed tools such as the EPDS, which differ in sensitivity and symptom threshold. Such methodological variations can influence the detection rate and severity classification of depression symptoms.
Conversely, our prevalence was higher than findings from Debre Tabor (11.8%)10, Brazil (14.2%)24, and Washington (9.9%)25. These differences may be influenced by differences in the sociodemographic makeup of the population, awareness and stigma surrounding mental health, or sample size and timing of data collection during pregnancy.
This study identified several significant predictors of antenatal depression, each of which was explained as follows:
Marital status
Single women were more likely to experience antenatal depression than their married counterparts. This finding is consistent with studies from Northeast Ethiopia12, Arbaminch26, and Brazil27. The increased vulnerability may be attributed to stigma associated with premarital pregnancy, leading to social isolation, lack of partner and family support, and economic challenges. In the Ethiopian context, cultural expectations around marriage and motherhood can intensify emotional stress for unmarried pregnant women, further compounding mental health risks.
Chronic medical illness
Women with a history of chronic illness showed significantly higher odds of experiencing depression, showing findings from Nigeria28, Arbaminch26, and Washington25. Chronic illnesses may reduce a woman’s ability to carry out daily activities, lower her self-confidence, and foster a sense of hopelessness, factors that can aggravate depressive symptoms. In rural Ethiopian communities, limited access to ongoing treatment or specialist care may worsen this burden.
Unplanned pregnancy
Consistent with literature from Dubti1, Oman29, and Turkey2, distress, uncertainty, and financial insecurity often accompany unplanned pregnancies, especially in low-income settings where reproductive autonomy may be limited. In traditional Ethiopian society, cultural expectations around marriage, childbearing, and family roles can result in negative community attitudes toward unplanned pregnancies, increasing social pressure and stigma.
Lack of family support
Women reporting low social support were at increased risk of depression, as seen in studies from Hawassa19, Rwanda30, and Bangladesh31. In Ethiopian culture, family is often the primary support system during pregnancy. When this is absent due to migration, marital conflict, or stigma, the resulting emotional and material insecurity can predispose women to mental distress. Support systems provide not only emotional comfort but also practical help in navigating pregnancy-related challenges.
Previous history of depression
Women with a prior diagnosis of depression were more likely to report antenatal depression. Similar associations were found in Debre Tabor10, Tanzania9, and Brazil24. This suggests that biological vulnerability, along with unresolved psychological stressors, can recur during pregnancy. Given the cyclical nature of depression, pregnancy may act as a trigger for relapse.
Educational status
Lack of formal education was significantly associated with antenatal depression, supporting evidence from Nigeria28, Arbaminch32, and Bangladesh31. Lower educational attainment may limit women’s health literacy, economic independence, and coping strategies. In the Ethiopian setting, uneducated women may have reduced access to accurate health information, leading to delayed help-seeking and greater susceptibility to emotional stressors.
Implications and limitations
This study was done by using a cross-sectional design, which prevents the determination of cause-and-effect relationships. As this was a hospital-based study, the findings may not fully represent the prevalence of antenatal depression in the wider community. Moreover, relying on self-reported data may introduce reporting bias, as participants might underreport symptoms due to stigma or cultural perceptions of mental illness. Methodologically, the use of different screening tools like EPDS vs. BDI can impact prevalence estimates. Each tool has unique cutoff thresholds and symptom sensitivity, which may partially explain cross-study differences.
These findings suggest integrating depression screening into routine ANC visits, strengthening community-based psychosocial support networks, and prioritizing vulnerable groups such as women with unplanned pregnancies, single mothers, and those with chronic illness. Training health workers in early identification and referral of antenatal depression should be a key policy priority.
Conclusion
Antenatal depression affected 22% of pregnant women in this study. Factors such as being single, uneducated, having a chronic illness, lacking family support, and experiencing an unplanned pregnancy increased the risk. Integration of depression screening into ANC, coupled with targeted psychosocial interventions, is urgently needed to improve maternal and child health outcomes in Ethiopia.
Data availability
All relevant data are within the manuscript.
References
Belay, Y. A., Moges, N. A., Hiksa, F. F., Arado, K. K. & Liben, M. L. Prevalence of antenatal depression and associated factors among pregnant women attending antenatal care at Dubti Hospital: a case of pastoralist region in Northeast Ethiopia. Depression Research and Treatment 2018. (2018).
Yanikkerem, E., Ay, S., Mutlu, S. & Goker, A. Antenatal depression: prevalence and risk factors in a hospital-based Turkish sample. J. Pak Med. Assoc. 63 (4), 472–477 (2013).
Dibaba, Y., Fantahun, M. & Hindin, M. J. The association of unwanted pregnancy and social support with depressive symptoms in pregnancy: evidence from rural Southwestern Ethiopia. BMC Pregnancy Childbirth. 13 (1), 1–8 (2013).
Alipour, Z., Kheirabadi, G. R., Eslami, A. A. & Kazemi, A. Psychological profiles of risk for antenatal depression and anxiety in the Iranian sociocultural context. J. Educ. Health Promotion 7 (2018).
Sheeba, B. et al. Prenatal depression and its associated risk factors among pregnant women in bangalore: a hospital-based prevalence study. Front. Public. Health. 7, 108 (2019).
Dadi, A. F., Miller, E. R., Bisetegn, T. A. & Mwanri, L. Global burden of antenatal depression and its association with adverse birth outcomes: an umbrella review. BMC Public. Health. 20, 1–16 (2020).
Hanlon, C. Maternal depression in low-and middle-income countries. Int. Health. 5 (1), 4–5 (2013).
Manikkam, L. & Burns, J. K. Antenatal depression and its risk factors: an urban prevalence study in KwaZulu-Natal. South. Afr. Med. J. 102 (12), 940–944 (2012).
Rwakarema, M., Premji, S. S., Nyanza, E. C., Riziki, P. & Palacios-Derflingher, L. Antenatal depression is associated with pregnancy-related anxiety, partner relations, and wealth in women in Northern tanzania: a cross-sectional study. BMC Women’s Health. 15 (1), 1–10 (2015).
Bisetegn, T. A., Mihretie, G. & Muche, T. Prevalence and predictors of depression among pregnant women in Debretabor town, Northwest Ethiopia. PloS One. 11 (9), e0161108 (2016).
Biratu, A. & Haile, D. Prevalence of antenatal depression and associated factors among pregnant women in addis Ababa, ethiopia: a cross-sectional study. Reproductive Health. 12 (1), 1–8 (2015).
Beyene, G. M., Azale, T., Gelaye, K. A. & Ayele, T. A. Depression remains a neglected public health problem among pregnant women in Northwest Ethiopia. Archives public. Health. 79 (1), 1–12 (2021).
Bitew, T., Hanlon, C., Kebede, E., Medhin, G. & Fekadu, A. Antenatal depressive symptoms and maternal health care utilisation: a population-based study of pregnant women in Ethiopia. BMC Pregnancy Childbirth. 16 (1), 1–11 (2016).
Beketie, E. D., Kahsay, H. B., Nigussie, F. G. & Tafese, W. T. Magnitude and associated factors of antenatal depression among mothers attending antenatal care in Arba minch town, Ethiopia, 2018. PloS One. 16 (12), e0260691 (2021).
Habtamu Belete, A., Alemayehu Assega, M., Alemu Abajobir, A., Abebe Belay, Y. & Kassahun Tariku, M. Prevalence of antenatal depression and associated factors among pregnant women in aneded woreda, North West ethiopia: a community based cross-sectional study. BMC Res. Notes. 12, 1–6 (2019).
Bah, A. J. & A COLLABORATIVE CARE MODEL FOR PERINATAL MENTAL HEALTH CARE IN SIERRA LEONE. Queen Margaret University, Edinburgh; (2023).
Ayele, T. A. et al. Prevalence and associated factors of antenatal depression among women attending antenatal care service at Gondar university Hospital, Northwest Ethiopia. PloS One. 11 (5), e0155125 (2016).
Beck, A. T., Steer, R. A., Ball, R. & Ranieri, W. F. Comparison of Beck depression Inventories-IA and-II in psychiatric outpatients. J. Pers. Assess. 67 (3), 588–597 (1996).
Duko, B., Ayano, G. & Bedaso, A. Depression among pregnant women and associated factors in Hawassa city, ethiopia: an institution-based cross-sectional study. Reproductive Health. 16 (1), 1–6 (2019).
Dahiya, N., Aggarwal, K. & Kumar, R. Prevalence and correlates of antenatal depression among women registered at antenatal clinic in North India. Tzu-Chi Med. J. 32 (3), 267 (2020).
Mossie, T. B., Sibhatu, A. K., Dargie, A. & Ayele, A. D. Prevalence of antenatal depressive symptoms and associated factors among pregnant women in Maichew, North ethiopia: an institution based study. Ethiop. J. Health Sci. 27 (1), 59–66 (2017).
Martha, A. S., Mesfin, T. S., Tadese, A. & Dessalegn, B. Prevalence and predictors of antenatal depressive symptoms among women attending Adama hospital antenatal Clinic, Adama, Ethiopia. Int. J. Nurs. Midwifery. 9 (5), 58–64 (2017).
Al-Hejji, Z., Al-Khudhair, M., Al-Musaileem, M. & Al-Eithan, M. Prevalence and associated risk factors of antenatal depression among women attending antenatal clinics in primary health care centers in the ministry of health in Al-Ahsa City, Saudi Arabia. J. Family Med. Prim. Care. 8 (12), 3900 (2019).
Pereira, P. K., Lovisi, G. M., Pilowsky, D. L., Lima, L. A. & Legay, L. F. Depression during pregnancy: prevalence and risk factors among women attending a public health clinic in Rio de Janeiro, Brazil. Cadernos de Saúde Pública 25, 2725–2736 (2009).
Melville, J. L., Gavin, A., Guo, Y., Fan, M-Y. & Katon, W. J. Depressive disorders during pregnancy: prevalence and risk factors in a large urban sample. Obstet. Gynecol. 116 (5), 1064 (2010).
Woldetsadik, A. M., Ayele, A. N., Roba, A. E., Haile, G. F. & Mubashir, K. Prevalence of common mental disorder and associated factors among pregnant women in South-East Ethiopia, 2017: a community based cross-sectional study. Reproductive Health. 16 (1), 1–8 (2019).
Silva RAd, Jansen, K., Souza, L. D. M., Moraes, I. G. S., Tomasi, E. & Silva GDGd Dias MdS, Pinheiro RT: depression during pregnancy in the Brazilian public health care system. Brazilian J. Psychiatry. 32, 139–144 (2010).
Thompson, O. & Ajayi, I. Prevalence of antenatal depression and associated risk factors among pregnant women attending antenatal clinics in Abeokuta North Local Government Area, Nigeria. Depression research and treatment 2016. (2016).
Al-Azri, M. et al. Prevalence and risk factors of antenatal depression among Omani women in a primary care setting: cross-sectional study. Sultan Qaboos Univ. Med. J. 16 (1), e35 (2016).
Millar, K. R. Prevalence and Associated Factors of Antenatal Depression in post-conflict Rwanda: Implications for Nurse Midwifery Policy and Practice (University of California, 2018).
Nasreen, H. E., Kabir, Z. N., Forsell, Y. & Edhborg, M. Prevalence and associated factors of depressive and anxiety symptoms during pregnancy: a population based study in rural Bangladesh. BMC Women’s Health. 11 (1), 1–9 (2011).
Gebremichael, G., Yihune, M., Ajema, D., Haftu, D. & Gedamu, G. Perinatal depression and associated factors among mothers in Southern Ethiopia: evidence from Arba Minch Zuria health and demographic surveillance site. Psychiatry journal 2018. (2018).
Acknowledgements
The authors would like to acknowledge the participants, data collectors, supervisors, and Shegaw Motta General Hospital Administrative.
Funding
This research received no specific grant from any funding agency.
Author information
Authors and Affiliations
Contributions
TYA conceived and designed the study. TYA, AA, SA, AAF, and BYA wrote the paper and conducted data analysis. BYA prepared the first draft of the manuscript. All the authors finalized the manuscript for publication.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ashenef, T.Y., Asres, A., Animen, S. et al. Prevalence and associated factors of antenatal depression among pregnant women attending Shegaw Motta general Hospital, East Gojjam Zone, Ethiopia. Sci Rep 15, 45451 (2025). https://doi.org/10.1038/s41598-025-29496-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-29496-z
