
Abstract
Pneumonia is a significant global public health problem, and climatic factors play a crucial role in disease epidemic dynamics. However, there are limited studies on this relationship in tropical monsoon coastal climate regions. This study aimed to analyze the impact of climatic factors on pneumonia pattern in Satun Province, a southern coastal province of Thailand, using Bayesian Structural Time Series (BSTS) modeling. This ecological study utilized monthly time series data spanning 10 years (January 2015 – December 2024). Pneumonia case data (ICD-10: J12-J18) were collected from the National Disease Surveillance System, and monthly climatic data were obtained from Satun Province meteorological stations. The BSTS model was employed to decompose long-term trend components, seasonal patterns, and the simultaneous effects of multiple climatic variables, using spike-and-slab priors technique for Bayesian variable selection. The median number of pneumonia cases was 63.0 cases per month (IQR: 34.0-102.0). BSTS model analysis revealed that relative humidity was the most influential climatic predictor of pneumonia cases, demonstrating a 2-month lag effect (Posterior Inclusion Probability [PIP] = 0.284). A one standard deviation increase in relative humidity was associated with approximately 6.4% increase in cases. Other climatic variables such as temperature, precipitation, and wind speed were not identified as robust predictors in the final model. Additionally, distinct seasonal epidemic patterns were observed, with case peaking during October-November. Relative humidity is a factor associated with pneumonia epidemics in Satun Province, challenging traditional concepts that typically emphasize temperature as the primary factor in temperate regions. The discovery of this 2-month lag relationship is significant for developing public health early warning systems, enabling effective preparation of resources and proactive preventive measure planning.
Similar content being viewed by others
Introduction
Pneumonia is a leading cause of death in children under 5 years of age, accounting for more than 700,000 deaths annually worldwide1,2. In Thailand, the burden of pneumonia has been a long-standing public health concern, with past research identifying high incidence rates in various regions, including the northeast and north between 2002 and 20143,4. Current national overview from just prior to the COVID-19 pandemic in 2019 reported a nationwide incidence rate of 388 cases per 100,000 population5. While these national figures are informative, they often mask significant regional disparities. The southern coastal provinces, for instance, have been identified as an area with a historical lack of granular climate-health data. Critically, local epidemiological surveillance reports from Satun Province confirm that pneumonia is not only a persistent but also an escalating public health crisis. The annual incidence rate surged from 93.02 cases per 100,000 population in 2021 to 414.08 in 2023, a more than fourfold increase6. This 2023 figure firmly establishes pneumonia as the highest-burden infectious disease in the province. This underscores that Satun is not only a climatically unique region but also a high-burden area, making it an ideal and crucial setting for this investigation.
Climate change is a significant driving factor affecting infectious disease epidemic patterns globally7. Climatic variables, including temperature, humidity, and precipitation, influence pathogen survival, airborne transmission, and human behavior7,8. In Thailand, studies on the relationship between pneumonia and climatic factors remain limited. Research in Lampang Province found seasonal epidemic patterns associated with humidity and temperature9, while Chiang Mai Province demonstrated similar patterns4. However, these studies employed traditional statistical methods with limitations in handling uncertainty in variable selection and parameter estimation. Furthermore, there is a lack of studies in coastal areas with specific local climatic characteristics, which may have different epidemic mechanisms compared to inland areas. As the direct interface for the Southwest Monsoon, the Andaman Sea coast experiences a unique climatic regime characterized by prolonged periods of high, stable humidity and distinct rainfall patterns10. This environment provides a critical natural laboratory to investigate the role of humidity-driven disease transmission, potentially isolating its effects from the large temperature fluctuations that dominate in temperate regions11.
Analyzing these complex climate-health relationships poses a methodological challenge. Traditional time series models, such as ARIMA, often face several key limitations: they have a limited capacity to incorporate external predictors, are not inherently robust to sudden structural changes in the data, and do not formally quantify uncertainty in parameter selection and forecasts12.To address these specific limitations, this study employs the Bayesian Structural Time Series (BSTS) model. This methodology has been successfully applied in various public health contexts, such as forecasting influenza outbreaks13 and evaluating policy impacts14, where it has often demonstrated superior performance over traditional models in terms of forecast accuracy and uncertainty quantification13,15. The BSTS framework is explicitly designed to overcome these challenges by seamlessly integrating multiple external variables, modeling dynamic shifts in trends through its flexible state-space components, and providing a complete probabilistic assessment of all sources of uncertainty13,14,15.
Given the identified research gaps, both geographical, concerning the understudied coastal climate of southern Thailand, and methodological, regarding the limitations of models used in prior inland studies, this study aims to analyze the dynamic association between key climatic drivers and pneumonia patterns in Satun Province. As a representative Andaman Sea coastal region, this study employs the robust Bayesian Structural Time Series (BSTS) model to fill these gaps. We hypothesize that (1) relative humidity and precipitation, as key indicators of the coastal monsoon climate, are significant drivers of pneumonia patterns, and (2) the BSTS framework can effectively identify and quantify complex temporal dynamics, including lagged effects, between these climatic variables and pneumonia incidence. The insights generated will hold significant policy relevance for the development of early warning systems and targeted public health interventions in similar climate-vulnerable regions.
Methodology
Study area and population
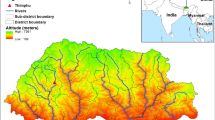
This study is an ecological study with the target area being Satun Province, located in southern Thailand on the Andaman Sea coast (latitude 6°39’ N, longitude 100°05’ E) (Fig. 1). Satun Province has a tropical monsoon climate influenced by the southwest monsoon, resulting in frequent rainfall and high relative humidity almost year-round, with an average annual temperature of approximately 27.7 °C and average annual precipitation of 2,348.3 millimeters.
The selection of Satun Province as the study area was based on the particularly concerning pneumonia situation, as it is one of the provinces with the highest morbidity rates in lower southern Thailand, with a pneumonia mortality rate of 28.55 per 100,000 population in 2023, which is high and continuously increasing, contrary to trends in other provinces in the region. Additionally, the morbidity rate has increased more than 4-fold over the past 3 years.
The study population consists of the aggregated dataset of all pneumonia patients in Satun Province during the specified time period. As no individual-level data were collected, this study employs an ecological time-series design. It is important to acknowledge the inherent limitations of this approach: the findings represent associations at a population level and cannot be used to infer risk for individuals (a limitation known as the ecological fallacy), and the results indicate statistical associations rather than direct causal relationships.

Study area: Satun Province, Thailand. This map was generated by the authors using QGIS software (Version 3.44, https://www.qgis.org).
Health data
The health data consisted of aggregated monthly pneumonia case counts collected retrospectively over a 10-year period from January 1, 2015, to December 31, 2024. This monthly aggregation was chosen to match the temporal resolution of the climate variables (as described in the “Climate Data” section) and to align with the study’s objective of analyzing seasonal patterns. The data were sourced from the National Disease Surveillance System (R506) via the Satun Provincial Public Health Office. This surveillance system consolidates reports from all public sector health facilities, ranging from community-level health centers to the provincial hospital; reports from private hospitals and clinics were not included in this dataset.
The case definition included all patients diagnosed with pneumonia according to the International Classification of Diseases, 10th Revision (ICD-10) codes J12-J18. As a data quality control measure to ensure the accuracy of the monthly totals, duplicate reports for the same patient within a 14-day period were excluded to prevent double counting. There were no major changes to this surveillance system or the case definition during the study period that would significantly affect data trends.
Climate data
Climate data consisted of monthly secondary data corresponding to the health data timeframe (2015–2024), collected from the Satun Province meteorological station of the Thai Meteorological Department. Variables used in the analysis included: mean temperature (°C), mean maximum temperature (°C), mean minimum temperature (°C), mean relative humidity (%), total monthly rainfall (mm), number of rainy days, mean wind speed (knots), and maximum wind speed (knots).
Data analysis
Descriptive statistics: basic statistics and Spearman correlations between climatic variables and pneumonia incidence were calculated, including cross-temporal correlation analysis to examine lag effects at 0–3 months.
BSTS model construction
patient count data were transformed using natural logarithm. Specifically, to handle months with zero cases (as the logarithm of zero is undefined), a continuity correction was applied by adding 0.5 to all case counts before the transformation. To handle months with zero cases, a continuity correction of + 0.5 was applied prior to the natural logarithm transformation. The + 0.5 correction is often recommended for count data as it provides better variance stabilization and can reduce bias upon back-transformation16.
The climatic variables underwent standardization. The BSTS model comprised: (1) local linear trend for changeable trends, (2) seasonal component for 12-month annual seasonal patterns, and (3) regression component using spike-and-slab priors for climatic variable selection. The flexibility of the local linear trend component is particularly crucial, as it allows the model to adapt to unforeseen structural breaks in the time series, such as the one observed during the COVID-19 pandemic. Regarding the spike-and-slab prior for variable selection, instead of using the default settings, we specified a key hyperparameter by setting the expected model size to 2. This reflects a prior belief that a small number of predictors would be most influential. For this analysis, we adopted a threshold of Posterior Inclusion Probability (PIP) ≥ 0.20 as a screening criterion to identify variables with influence on pneumonia occurrence. The PIP, which ranges from 0 to 1, represents the probability that a variable has a genuine effect and should be included in the model. This approach allows for the consideration of all variables with non-trivial evidence of an association, a common practice in exploratory and predictive modeling to avoid the premature exclusion of potentially relevant factors17.
To quantitatively assess the model’s predictive performance, we conducted a hold-out validation. The dataset was split into a training set (January 2015 – December 2022) and a test set (January 2023 – December 2024). The BSTS model was fitted using only the training data, and a 24-month forecast was subsequently generated. The forecast accuracy was then evaluated on the test set by comparing the predicted values against the observed values, using three standard metrics: mean absolute error (MAE), root mean squared error (RMSE), and mean absolute percentage error (MAPE).
To address potential multicollinearity among the climate predictors (e.g., between mean, minimum, and maximum temperature, or between rainfall volume and rainy days), we first examined a correlation matrix of all candidate variables. Based on this analysis, a final subset of four representative predictors with lower inter-correlation was selected for inclusion in the final BSTS model. This variable selection step ensures a more stable and interpretable model.
Parameter Estimation and model assessment
Markov Chain Monte Carlo (MCMC) with 15,000 iterations was used, with a burn-in period of the first 1,500 rounds (10% of total iterations according to bsts package default). Model performance was assessed via diagnostic checks. MCMC convergence was confirmed by visually inspecting parameter trace plots. Residuals were then checked for serial correlation and normality using the autocorrelation function (ACF) plot and a histogram, respectively. Long-term 12-month forecasts were generated with 95% credible intervals and decomposition analysis to separate the effects of trend, seasonal, and climatic variables.
Data analysis tools
All analyses were conducted using R software (version 4.3.0) with main packages: bsts for Bayesian Structural Time Series, ggplot2 for graphing, and dplyr for data management.
Results
Table 1 shows the basic characteristics of data used in the study over a 10-year period, covering 120 months from January 2015 to December 2024 in Satun Province. Health outcomes: The number of pneumonia patients had a median of 63.0 cases per month (IQR: 34.0–102.0.0.0), with a range from 0 to 417 cases per month. The incidence per 100,000 population had a median of 19.5 cases (IQR: 12.6–31.6). Climatic variables: Characteristics of tropical humid climate in the southern region showed mean temperature of 28.7 ± 0.8 °C, with minimum and maximum temperatures in the ranges of 24.3 ± 0.6 °C and 33.1 ± 1.4 °C, respectively. Relative humidity was high with an average of 80.2 ± 5.8%. Rainfall showed the highest variability (203.7 ± 145.2 mm) with a wide range (0–674 mm). The average number of rainy days was 14.7 ± 7.1 days per month. Mean wind speed was relatively low (1.0 ± 0.7 knots), but maximum wind speed was 10.6 ± 1.2 knots.
Table 2 shows the results of Spearman correlation analysis between climatic variables and the number of pneumonia patients, comparing simple correlation (without lag) and lagged correlation at the optimal time period (best lag) for each variable. Simple correlation analysis revealed that maximum temperature and maximum wind speed showed statistically significant correlations (p < 0.01). Maximum temperature demonstrated a moderate negative correlation (ρ = −0.261), while maximum wind speed showed a moderate positive correlation (ρ = 0.236). Other variables were not statistically significant.
Lagged correlation analysis found the correlation in maximum temperature at 1-month lag (ρ = 0.323, p < 0.001), which changed from a negative correlation in the simple analysis to a positive correlation. This reversal likely occurs because the multivariate model adjusts for the confounding effects of other variables (like humidity) and the underlying temporal structure (trend and seasonality), thus revealing a more complex underlying relationship. Variables related to humidity showed significant positive correlations, including relative humidity (2-month lag, ρ = 0.267), rainy days (2-month lag, ρ = 0.260), and rainfall (3-month lag, ρ = 0.227). Conversely, mean wind speed demonstrated a negative correlation (2-month lag, ρ = −0.339, p < 0.001). Optimal lag periods varied according to variable characteristics. Variables related to temperature and maximum wind speed showed immediate effects or 1-month lag, while variables related to humidity and precipitation showed lag effects of 2–3 months.
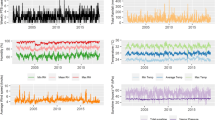
Figure 2 shows the following analytical results: Pneumonia cases over time (A) presents the trend in incidence rates over the study period, highlighting significant temporal changes. The blue line shows monthly data, while the red line shows the long-term trend (LOESS smoothing). The peak of disease occurrence appeared in late 2024 with over 400 cases per month, and clear seasonal variation was observed. Climatic variables (B) showed changes in four important climatic variables: maximum temperature (32–37 °C) displaying clear seasonal patterns with annual peaks and relatively high variation; monthly rainfall (0–600 millimeters) showing the highest variability with distinct seasonal patterns; relative humidity (70–90%) varying according to rainy and dry seasons; and wind speed (0–3 knots) with periodic seasonal peaks. Seasonal patterns of pneumonia (C) revealed the distribution of patient numbers in each month throughout the year. The period with the highest number of patients was October-November (average ~ 120 cases per month), which corresponds to the post-rainy season period, while the period with the lowest number of patients was April-May (average ~ 45–50 cases per month) during the hot season. The difference between the highest and lowest periods was nearly 3-fold. Error bars show the standard error of the mean.
Relationship between humidity and (D) displays the distribution of all monthly data using relative humidity as the X-axis and number of patients as the Y-axis. Each data point shows temperature through color gradation (dark color = low temperature, light color = high temperature). The red trend line shows a slight positive relationship between humidity and disease occurrence, but considerable data variability was observed.

Time Series Overview and Seasonal Patterns of Pneumonia Cases and Climate Variables in Satun Province, 2015–2024.
Bayesian structural time series analysis
Based on the correlation analysis in Table 2, climatic variables that showed significant lagged relationships were selected for Bayesian Structural Time Series (BSTS) model construction. To address multicollinearity issues, variables with high intercorrelations were reduced to representatives of each group, including: relative humidity (2-month lag), maximum temperature (1-month lag), wind speed (2-month lag), and rainfall (3-month lag).
The BSTS model was designed to comprise three main components: (1) Local linear trend component for capturing long-term trends, (2) 12-month seasonal component for seasonal patterns, and (3) Regression component using spike-and-slab priors for automatic climatic variable selection. This process enables identification of variables with statistical relationships to pneumonia occurrence through PIP values, where variables with PIP ≥ 0.20 are considered to have strong evidence for association. The analysis was conducted using MCMC sampling with 15,000 iterations following standardization of climatic variables to make coefficient comparisons meaningful. Results of component decomposition and model performance are shown in Fig. 3.

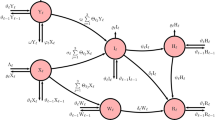
Decomposition and forecasting performance of BSTS model for pneumonia cases in Satun Province in southern Thailand.
Figure 3 shows the following analytical results: (A) Observed vs. model-fitted values compares actual data (black line) and model-estimated values (red line) throughout the study period. The BSTS model was able to closely track the patterns of actual data, including capturing seasonal variation and long-term trends, and notably, the sharp structural break (the rapid decline during 2021 and subsequent recovery) associated with the COVID-19. The high concordance between both lines demonstrates the model’s effectiveness in explaining data variance. The long-term trend component (B) presents changes in the main trend free from seasonal and climatic factor influences. The trend shows interesting changes in three main periods that align closely with the key phases of the COVID-19 pandemic: the first period (2015–2019; represents the stable pre-pandemic baseline) remained stable at levels of 3.5–4.5; the second period (2020–2021; coincides with the peak of the pandemic) experienced rapid and severe decline to the lowest point at approximately 0.5; and the third period (2022–2024; marks the post-intervention recovery phase) showed continuous recovery and increase to level 5.5, which is higher than the initial level. The dark blue curve (LOESS smoothing) clearly illustrates the overall direction of this trend. The seasonal component (C) reveals patterns that consistently repeat each year throughout the study period. The seasonal pattern varies between + 0.5 to −0.25, with a total difference of approximately 0.75 logarithmic units. Maximum and minimum points occur in the same months every year. The reference line at zero shows the baseline level of seasonal effects. The consistency of this pattern demonstrates the stability of seasonal factors in the study area. 12-month forecast with uncertainty intervals (D) demonstrates the model’s capability for future prediction, using the most recent 24 months of data (black line) as the basis for forecasting the next 12 months (red line). The vertical blue dashed line shows the division between actual data and forecasts. The red shaded area around the forecast line shows the 95% confidence interval, which expands as the forecast extends further. The forecast shows a trend that continues to remain at high levels consistent with current trends, along with seasonal patterns consistent with historical patterns. The out-of-sample forecast accuracy of the BSTS model was evaluated on the hold-out test period from January 2023 to December 2024. The model’s predictive performance resulted in a MAE of 108.58, a RMSE of 129.40, and a MAPE of 95.76%.

Bayesian analysis of climate variables influencing pneumonia cases in Satun Province, southern Thailand. Forest plot showing the magnitude and direction of effects from selected variables with credible intervals and PIP value.
Figure 4 shows the following analytical results: Forest plot displays effect sizes and significance levels of climatic variables on pneumonia occurrence in Satun Province, using results from the BSTS model after decomposing trend and seasonal components. Relative humidity (2-month lag) is the only variable showing strong evidence with a PIP of 0.284. The large red dot indicates high significance level and positive effect, with a standardized coefficient of approximately 0.062, meaning that a one standard deviation increase in relative humidity results in a 0.062 unit increase in the logarithm of patient numbers, or approximately 6.4% increase in patient count. The 95% credible interval (0.000, 0.365); as the lower bound includes zero, this represents borderline evidence rather than a conclusively significant effect. Other climatic variables including monthly rainfall (3-month lag), wind speed (2-month lag), and maximum temperature (1-month lag) show moderate evidence with PIP values of 0.059, 0.050, and 0.050, respectively, which are below the significance threshold. The smaller orange dots indicate lower significance levels. The coefficients of these variables are very small and close to zero, with wind speed showing a slight negative effect (−0.0025), while maximum temperature and rainfall show very small positive effects (0.0024 and 0.0000, respectively).
Discussion
Our analysis identified relative humidity (with a 2-month lag) as the most influential climatic predictor of pneumonia occurrence among the variables assessed in this study. While its PIP of 0.284 indicates moderate evidence for inclusion and the credible interval for its effect was borderline, it was the only variable to emerge from the model’s stringent selection process. This positions relative humidity as a noteworthy contributing factor rather than a definitive main driver. This finding of a positive association in a tropical humid coastal area contrasts with many studies from temperate zones that found negative correlations between humidity and respiratory diseases, which commonly report that dry and cold air increases the risk of influenza and pneumonia infections18. While other climatic variables that commonly show relationships in previous research, such as maximum temperature, wind speed, and rainfall, all had PIP below 6%. The use of spike-and-slab priors in BSTS allows for more stringent variable selection compared to traditional correlation analysis, which found significant relationships in multiple variables simultaneously but may have been merely spurious correlations from multicollinearity.
This study’s results are consistent with studies in tropical zones that found positive correlations between humidity and pneumonia occurrence, in Tanzania which reported incidence rate ratios of 1.01–1.02 for humidity increases19. A comprehensive study on acute respiratory infections in children in Ho Chi Minh City, Vietnam, found that lower respiratory tract infections (which include pneumonia) peaked during the wet season and were significantly associated with rainfall and humidity20. The effect size found in this study (6.4% increase per SD) indicates the clinical importance of this relationship in a public health context. To put this into perspective, based on the median of 63 monthly cases, a one standard deviation increase in relative humidity could be associated with approximately 4 additional pneumonia cases per month. The discovery of a 2-month lag effect is important evidence supporting the biological mechanism of this relationship, differing from studies in temperate zones that commonly find immediate effects or lags of only a few weeks18. This lag period is consistent with the time required for pathogens to accumulate in the environment, from pathogen survival capability in high humidity conditions to changes in airborne droplets affecting transmission21, all of which require time to impact population infection rates.
The positive relationship between relative humidity and pneumonia occurrence with a 2-month lag indicates biological mechanisms different from temperate zones, requiring a review of humidity-transmission dynamics concepts in tropical humid regions. In temperate zones, dry and cold conditions cause respiratory droplets to evaporate quickly and persist in the air as aerosol nuclei for extended periods, while low humidity promotes the survival of many viruses, including influenza virus22,23. Conversely, tropical humid environments have more complex mechanisms, where high humidity promotes transmission through indirect pathways, including accumulation and survival of bacteria on environmental surfaces such as children’s toys, childcare equipment, and shared contact surfaces. Studies found that Streptococcus pneumoniae in biofilm form can survive on environmental surfaces for weeks, while planktonic bacteria die within hours, and can accumulate in the environment to levels sufficient for infection24.
In tropical humid zones, when humidity remains consistently high (> 70% RH), high humidity promotes biofilm formation on various surfaces, helping microorganisms survive and grow better in unfavorable environments25. Studies found that when relative humidity exceeds 60%, microorganisms can continuously multiply, while humidity below 60% stops microbial multiplication26,27. Climate changes in tropical humid regions, including changes in temperature, humidity, and rainfall patterns, can increase the severity and spread of diseases from various pathogens28.
A key finding of this study is the lack of a robust association between pneumonia cases and variables such as maximum temperature and wind speed, despite their reported influence in many prior studies. Several factors could explain this discrepancy. First, regional differences are critical; in a tropical coastal environment like Satun with relatively stable year-round temperatures, the influence of temperature may be less pronounced compared to temperate regions with distinct seasons. In this context, the more variable factor, relative humidity, may emerge as the more dominant climatic driver. Second, methodological factors play a role. Our use of a stringent Bayesian variable selection method is designed to isolate the most consistent predictors. It is therefore possible that the effects of temperature and wind are more subtle, confounded by other variables, or part of complex, non-linear interactions not captured by the current model, which warrants further investigation29.
This study’s results support a multi-pathway transmission model for pneumonia in the tropics, incorporating both direct droplet transmission and indirect environmental transmission. In the human context, transmission through contaminated surfaces and prolonged environmental persistence may play important roles in tropical humid conditions, especially in environments with human congregation (childcare facilities, schools) and limited ventilation. Studies found that S. pneumoniae can survive on environmental surfaces such as toys and bedding in childcare facilities for weeks24.
The discovery of a 2-month lag relationship between relative humidity and pneumonia occurrence opens opportunities for developing climate data-based early warning systems. Public health agencies can use monthly humidity data as indicators to prepare for increased pneumonia cases in the following 2 months. Close surveillance during high humidity periods will help appropriately allocate medical resources such as hospital beds, antibiotics, and medical personnel. The distinct seasonal pattern with peaks in October-November should be utilized for proactive prevention strategies. Hospitals and health facilities in Satun Province should prepare resources to handle patient increases accordingly.
Using BSTS models for real-time surveillance can improve public health decision-making systems, as the model can update forecasts with new data and provide reliable credible intervals for planning. For community-level prevention, educating the public about increased risks during high humidity periods and after the rainy season will help promote appropriate preventive behaviors, such as wearing masks in crowded places, avoiding close contact with patients, and seeking rapid treatment when symptoms appear. Risk communication should focus on vulnerable groups such as young children, elderly individuals, and those with chronic diseases. Integrating climate data into provincial disease surveillance systems will help improve epidemic response efficiency. Using automated alert systems connected to Thai Meteorological Department data can warn public health officials when humidity begins increasing to concerning levels. For example, an operational strategy could involve establishing a statistical threshold, such as when the 2-month lagged relative humidity exceeds one standard deviation above its seasonal mean. An alert triggered by this threshold would signal the need for heightened surveillance and resource preparation for the coming months. To make these forecasts more actionable, future early warning systems should integrate these climate-based alerts with real-time epidemiological indicators, such as trends in hospital admissions for respiratory symptoms or laboratory surveillance data. Such systems will provide additional preparation time and reduce impacts on health systems during peak epidemic periods. However, the implementation of such advanced systems requires careful consideration of their feasibility in resource-limited settings. A phased approach, starting with simpler alert thresholds and capacity building for local staff, could be a practical first step.
Limitation
The limitation of this study is being an ecological study that cannot infer causal relationships at the individual level. The relationship between relative humidity and pneumonia occurrence found may be influenced by ecological fallacy or aggregation bias. Using climate data from a single station may not reflect the environmental diversity within Satun Province, especially in areas with different topography. The exclusion of other important confounding variables such as air pollution, population density, and socioeconomic factors may affect estimation accuracy; the omission of these factors could lead to omitted-variable bias, and future studies incorporating them are needed to confirm the robustness of the humidity effect. A comparative sensitivity analysis would be a valuable next step in this line of research.
Bayesian epidemic model studies emphasise the importance of incorporating behavioural factors and population dynamics in models. However, adding these variables must consider overfitting problems and model complexity. The study area to a single province requires caution in applying results to other areas. Although Satun Province is a good representative of tropical humid coastal areas, differences in population demographics, healthcare accessibility, and local environmental factors may affect study application. As suggested, to validate these population-level findings and explore specific risk factors, we recommend that future research employ individual-level study designs.
The high MAPE value is likely influenced by months with low case counts in the test period, a known limitation of the metric. The MAE and RMSE, which are more stable in this context, indicate the absolute magnitude of the forecast error. These results suggest that while the model is effective in explaining historical patterns, long-term forecasting remains a challenge, highlighting an important area for future work.
Conclusion
This study analysed the impact of climate variables on pneumonia patterns in coastal areas of southern Thailand using BSTS modelling. Relative humidity emerged as the most influential climatic predictor, with a two-month lag effect, where each one standard deviation increase was associated with approximately a 6.4% rise in cases. In addition, a distinct seasonal peak in pneumonia incidence was observed from October to November. These findings underscore the value of incorporating climatic indicators, particularly humidity, into public health early warning systems to support timely resource allocation and preventive strategies.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Unicef Pneumonia: A child dies of pneumonia every 43 seconds, (2024). https://data.unicef.org/topic/child-health/pneumonia/
World Health Organization. Pneumonia in children, (2022). https://www.who.int/news-room/fact-sheets/detail/pneumonia
Jordan, H. T. et al. A comparison of population-based pneumonia surveillance and health-seeking behavior in two provinces in rural Thailand. Int. J. Infect. Dis. 13, 355–361. https://doi.org/10.1016/j.ijid.2008.07.014 (2009).
Ruchiraset, A. & Tantrakarnapa, K. Time series modeling of pneumonia admissions and its association with air pollution and climate variables in Chiang Mai Province, Thailand. Environ. Sci. Pollut. Res. 25, 33277–33285. https://doi.org/10.1007/s11356-018-3284-4 (2018).
Poovieng, J., Sakboonyarat, B. & Nasomsong, W. Bacterial etiology and mortality rate in community-acquired pneumonia, healthcare-associated pneumonia and hospital-acquired pneumonia in Thai university hospital. Sci. Rep. 12, 9004. https://doi.org/10.1038/s41598-022-12904-z (2022).
Satun Provincial Health Office. Inspection and Supervision. Report, Fiscal Year Round 1 (Ekkasan Prakop Kan Truat Ratchakan Lae Nithet Ngan Korani Pokkati, Rop Thi 1, Pi Ngoppraman 2567) [in Thai], Ministry of Public Health Inspection Portal https:// (2024). inspection.moph.go.th/e-inspection/file_provinec/2024-02-16-10-28-40.pdf (2024).
Mirsaeidi, M. et al. Climate change and respiratory infections. Ann. Am. Thorac. Soc. 13, 1223–1230. https://doi.org/10.1513/AnnalsATS.201511-729PS (2016).
Feng, Y. et al. Impact of hot and cold nights on pneumonia hospitalisations in children under five years: evidence from low-, middle-, and high-income countries. Environ. Int. 192, 109041. https://doi.org/10.1016/j.envint.2024.109041 (2024).
Olsen, S. J., Laosiritaworn, Y., Siasiriwattana, S., Chunsuttiwat, S. & Dowell, S. F. The incidence of pneumonia in rural Thailand. Int. J. Infect. Dis. 10, 439–445. https://doi.org/10.1016/j.ijid.2006.06.004 (2006).
Limsakul, A. & Singhruck, P. Long-term trends and variability of total and extreme precipitation in Thailand. Atmos. Res. 169, 301–317. https://doi.org/10.1016/j.atmosres.2015.10.015 (2016). https://doi.org/https://doi.org/
Paynter, S. Humidity and respiratory virus transmission in tropical and temperate settings. Epidemiol. Infect. 143, 1110–1118. https://doi.org/10.1017/s0950268814002702 (2015).
Petrică, A. C., Stancu, S. & Tindeche, A. Limitation of ARIMA models in financial and monetary economics. Theor. Appl. Econ. 23, 19–42 (2016).
Scott, S. L. & Varian, H. R. Predicting the present with bayesian structural time series. Int. J. Math. Modelling Numer. Optimisation. 5, 4–23. https://doi.org/10.1504/ijmmno.2014.059942 (2014).
Brodersen, K. H., Gallusser, F., Koehler, J., Remy, N. & Scott, S. L. Inferring causal impact using Bayesian structural time-series models. (2015).
Liu, J. et al. Bayesian structural time series for biomedical sensor data: A flexible modeling framework for evaluating interventions. PLoS Comput. Biol. 17, e1009303. https://doi.org/10.1371/journal.pcbi.1009303 (2021).
Yamamura, K. Transformation using (x + 0.5) to stabilize the variance of populations. Researches Popul. Ecol. 41, 229–234. https://doi.org/10.1007/s101440050026 (1999).
Hara, R. B. O. & Sillanpää, M. J. A review of bayesian variable selection methods: what, how and which. Bayesian Anal. 4, 85–117. https://doi.org/10.1214/09-BA403 (2009).
Makrufardi, F. et al. Extreme temperatures increase the risk of pediatric pneumonia: a systematic review and meta-analysis. Front. Pediatr. 12, 1329918. https://doi.org/10.3389/fped.2024.1329918 (2024).
Miyayo, S. F., Owili, P. O., Muga, M. A. & Lin, T. H. Analysis of Pneumonia Occurrence in Relation to Climate Change in Tanga, Tanzania. Int. J. Environ. Res. Public. Health https://doi.org/10.3390/ijerph18094731 (2021).
Ho, N. T. et al. Retrospective analysis assessing the Spatial and Temporal distribution of paediatric acute respiratory tract infections in Ho Chi Minh City, Vietnam. BMJ Open. 8, e016349. https://doi.org/10.1136/bmjopen-2017-016349 (2018).
Marr, L. C., Tang, J. W., Van Mullekom, J. & Lakdawala, S. S. Mechanistic insights into the effect of humidity on airborne influenza virus survival, transmission and incidence. J. R Soc. Interface. 16, 20180298. https://doi.org/10.1098/rsif.2018.0298 (2019).
Lowen, A. C., Mubareka, S., Steel, J. & Palese, P. Influenza virus transmission is dependent on relative humidity and temperature. PLoS Pathog. 3, e151. https://doi.org/10.1371/journal.ppat.0030151 (2007).
Shaman, J. & Kohn, M. Absolute humidity modulates influenza survival, transmission, and seasonality. Proc. Natl. Acad. Sci. 106, 3243–3248. https://doi.org/10.1073/pnas.0806852106 (2009).
Marks, L. R., Reddinger, R. M. & Hakansson, A. P. Biofilm formation enhances fomite survival of Streptococcus pneumoniae and Streptococcus pyogenes. Infect. Immun. 82, 1141–1146. https://doi.org/10.1128/iai.01310-13 (2014).
Qiu, Y. et al. The Effects of Ventilation, Humidity, and Temperature on Bacterial Growth and Bacterial Genera Distribution. Int. J. Environ. Res. Public. Health https://doi.org/10.3390/ijerph192215345 (2022).
Beuchat, L. R. et al. Low–Water activity foods: increased concern as vehicles of foodborne pathogens. J. Food. Prot. 76, 150–172. https://doi.org/10.4315/0362-028X.JFP-12-211 (2013). https://doi.org/
Tremblay, Y. D., Hathroubi, S. & Jacques, M. [Bacterial biofilms: their importance in animal health and public health]. Can. J. Vet. Res. 78, 110–116 (2014).
Lahlali, R. et al. Effects of climate change on plant pathogens and host-pathogen interactions. Crop Environ. 3, 159–170. https://doi.org/10.1016/j.crope.2024.05.003 (2024). https://doi.org/https://doi.org/
Sohn, S. et al. Pneumonia weather’: Short-term effects of meteorological factors on emergency room visits due to pneumonia in Seoul, Korea. J. Prev. Med. Public. Health. 52, 82–91. https://doi.org/10.3961/jpmph.18.232 (2019).
Acknowledgements
The authors would like to thank the Satun Provincial Health Office was supporting health data and the Thai Meteorological Department was support climate data.
Funding
No funding.
Author information
Authors and Affiliations
Contributions
Kuafhum Koolong: Conceptualization; methodology; investigation; data curation; formal analysis; writing – original draft.Aroon La-up: Conceptualization; methodology; investigation; formal analysis; visualization; writing – original draft; writing – review & editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study was approved by Mahidol University Central Institutional Review Board (MU-CIRB). The approval number was MU-CIRB 2024/440.0111. This study was conducted in full accordance with the Declaration of Helsinki and relevant national guidelines. The requirement for informed consent was formally waived by the MU-CIRB as the research was based on a retrospective analysis of anonymized and aggregated secondary data with no personal identifiers.
Declaration of AI and AI-assisted technologies in the writing process
During the preparation of this work, the author(s) used AI in order to improve clarity and language in the manuscript, as well as for debugging and refining R code used for data analysis and visualization. After using these tools/services, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Koolong, K., La-up, A. Association of climate variables with pneumonia patterns in a tropical coastal province of thailand: a bayesian structural time series analysis. Sci Rep 15, 45266 (2025). https://doi.org/10.1038/s41598-025-30086-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-30086-2
