
Abstract
Direct resin restoration has been widely used to restore the tooth defect for its convenience and minimal invasion. However, the accuracy of the final contour of class II restoration is often unpredictable and quite technique-sensitive due to the limitation of traditional matrix band system. In this study, the authors developed a novel matrix band system using shape memory polymer (SMP), which possessed two reversible shapes including digitized permanent shape to reproduce anatomical proximal contour and programmable temporary shape for clinical practice and reservation. The permanent shape could be designed and customized in software or retrieved from imaging database collected from large general population. Only warm saline or water was needed to trigger the shape transformation without any auxiliary tools. The results of in vitro class II restoration showed the shape memory matrix bands brought the best proximal profile and contact point, compared to traditional metal matrix and sectional matrix. The novel shape memory matrix system represents the comfortable, precise, and minimally invasive trend of dentistry and has a broad industrialization prospect as a dental instrument.
Similar content being viewed by others

Introduction
Untreated caries in permanent teeth ranked the most common health condition globally (34.1%)1. In contemporary dentistry, direct resin restoration has been widely used to restore the tooth defect caused by caries, which is convenient, esthetic, and meets the principle of tooth structure preservation. However, while involving proximal caries, direct resin restoration is often limited by the proficiency and precision of the manual operation of the clinician. Digitized technology is gradually applied in dentistry, like inlay fabricated by CAD/CAM technology, improves the accuracy of tooth restoration2. However, additional tooth preparation is needed for inlay placement, and the relatively high cost and long waiting time also limit its application. Therefore, in this study, we explored to combine digital technology with direct resin restoration, achieving precise, efficient and minimally invasive restoration.
One of the greatest challenges associated with resin restoration is obtaining anatomically correct proximal contours3. Various commercial matrix systems have been adopted. However, improper proximal contact and overhangs may still exist4. Besides, auxiliary tools, such as separation ring and interdental wooden wedge, may cause uncomfortableness or be accidentally swallowed5,6. Shape memory polymers (SMP) are kind of stimuli-responsive materials, for which programmed shape(s) can be temporarily fixed and later recovered in response to an external stimulus on demand7,8,9. In our recent work, engineered bone membrane made of this stimuli-responsive 3-Dimesion (3D) material not only reconstructed the kinds of anatomical shapes of bone, but also achieved well retention by self-warping at the site of bone defect without auxiliary tools10.
In this study, we developed a novel matrix band system using SMP. The Scheme 1 displays the design, preparation and practice of digitized shape memory matrix band. This study combined smart biomaterials with digitzed technology, representing the comfortable, precise, and minimally invasive trend of dentistry.

The illustration of shape memory matrix band. (A) The obtaining of universal digitized tooth shape. The digitized tooth shape is retrieved from imaging database collected from large general population. With data analyzing and fitting, the digitized tooth replica is printed to prepare the shape memory matrix band. (B) The programming of shape memory matrix band. SMP film is chemical programmed to obtain the permanent shape with digitized proximal contour, and then physically programmed to obtain the temporary flat shape, which is convenient for sterilization and clinical operation. (C) The shape memory matrix band is inserted into the interdental space, and then recovered to its permanent shape of standardized proximal contour after gently washed by warm saline. Direct resin composite restoration is then performed.
Materials
Poly(ε-caprolactone) (PCL, Mn = 2000, and Mn = 10,000) (Sigma-Aldrich) were purchased commercially and used as received. PCL-diacrylate (PCLDA) was synthesized by the reaction between acryloyl chloride (Sigma-Aldrich) and PCL at a mass ratio of 1:1 according to previous study11. The precursor solution of SMP film was composed of PCLDA10000, PCLDA2000, DBTDL dibenzoyl peroxide (1 wt%) (Sigma-Aldrich), and N, N-dimethylformamide (10 wt%) (Sigma-Aldrich). The films were obtained by thermal polymerization at 80 °C and a vacuum oven was used to remove excess solvent. The film was fixed by the external force, then the permanent shape of the film was changed by transesterification inside the polymer network at a 140 °C.
Methods and results
The fabrication and characterization of SMP film
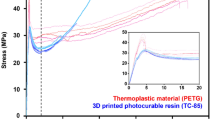
The remolding, programming, and recovery ability of the synthesized SMP was evaluated. As shown in Fig. 1A, the polymer network was synthesized by PCLDA of different molecular weight. The original flat rectangular film can be physically programmed into a reversible 3D spiral shape, or chemically programmed into an irreversible one by stress relaxation. Obtained polymer has the stimulus response temperature of 45 °C and excellent stability in cyclic thermomechanical testing using Differential scanning calorimetry (Q200, TA Instruments) (Fig. 1B,C), which is suitable for clinic reuse12. The solid-plasticity was verified in the stress relaxation curve by Dynamic mechanical analyses (DMA Q800, TA Instruments), confirming the establishment of the new permanent shape under external force (Fig. 1D). Cell viability testing showed the synthesized material had good biocompatibility (Fig. 1E). To demonstrate the shape memory process, we made a band replicating the shape of premolar crown, which could recover from a flatten shape with thermal stimulus (Fig. 1F,G, Appendix Movie 1).

The fabrication and characterization of SMP film. (A) Schematic diagram of programming and recovery of SMP film. (B) Differential scanning calorimetry curves. (C) Quantitative shape memory cycles tested by dynamic mechanical analyses. (D) Stress relaxation curve for the SMP. (E) Immunofluorescence of cell viability staining (green/alive, red/dead), scale bar is 500 μm. (F) Crown shape programming and (G) recovery images.
In vitro class II restoration in standard dental model
We fabricated the shape memory matrix band using SMP film and performed class II restoration in standard plastic dental crowns. Figure 2A showed the fabrication and application of shape memory matrix band. The temporary shape of this matrix was designed as a flattened thin piece with thickness of 50 um, which is convenient for sterilization and clinical operation. To test the restoration effect, an in vitro experiment was conducted in standard dental model (Appendix Movie 2), sectional matrix and traditional metal matrix were used as control group (Fig. 2B). A metal crown with lateral window was used to prepare standardized Class II cavity in plastic teeth (Appendix Fig. 1). The occlusal and lateral views showed that the use of SMP matrix band could reduce the overhang caused by poor adaptation of matrix band (Fig. 2B). The profiles of resin-restored teeth and original plastic teeth were fitted and quantitative analysis of the restoration area showed the proximal profile reconstructed by shape memory matrix had the smallest deviation with the original tooth (Fig. 2C). Moreover, the shape memory matrix had higher blue light transmittance compared with metal, thus reducing microleakage caused by incomplete curing during resin filling (Appendix Fig. 2).

In vitro class II restoration in standard dental model. (A) Fabrication and operation process of shape memory matrix on standard plastic teeth. The SMP film is tightly attached to the tooth model under chemical programing at 140 °C to obtain the permanent shape with standardized proximal contour. Then, the SMP film is compressed into a thin sheet under physical programing to obtain the temporary flat shape. Upon thermal stimulus, the flat matrix band would bend and recover to its permanent shape. (B) The occlusal and mesial surface of resin restoration restored with standard shape memory matrix, sectional matrix and traditional metal matrix. Standard class II cavity was outlined with red line and the resin restoration was outlined with green line. (C) The profiles of resin-restored teeth and original plastic teeth were fitted. Quantitative analysis of the accuracy of class II cavity restoration with three matrix systems.
Fabrication of customized and universal shape memory matrix band
The shape memory matrix band originated from standard plastic teeth could not be directly applied in clinical practice. How to obtain the natural profile of defected tooth was the following key point.
Ideally, the customized digitized proximal surface could be accurately obtained through digital technique as follows: after Class II preparation, the defected tooth is intraorally scanned and the restoration is designed by a technician in CAD software (Fig. 3A). The customized shape memory matrix band could be fabricated by replicating the contour of the designed 3D printed model. However, this protocol is time-consuming and costly, making it unsuitable for the chairside resin composite restoration.

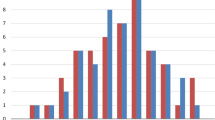
Design of the customized and universal proximal surface contour. (A) The design procedure of the customized proximal surface: The right maxillary first molar with a Class II cavity was laser scanned, and the restoration fitting the cavity was designed in a CAD software to achieve an ideal proximal surface. (B) The design procedure of universal proximal surface: CBCT images with intact right maxillary first molars were collected and the 3D crown model of the right maxillary first molar was segmented and constructed. A set of feature points (5 rows × 13 columns, totally 65 points) uniformly distributed over each proximal surface was designated. A unified 3D coordinate system OXYZ was established to provide spatial coordinate values of feature points. The origin of the coordinate system was the center of the tooth crown, and the X, Y, Z axes indicated the buccal, proximal, and occlusal orientations, respectively. The spatial locations of these feature points were recorded as Xi-j, Yi-j, Zi-j, where i indicated the row number and the j presented the column number. In total, N sets of feature points of proximal surfaces were extracted from N healthy right maxillary first molars. The coordinate values of the corresponding feature points with the same row and column numbers were averaged and recorded as \(\frac{1}{\text{N}}\) ƩXi−j, \(\frac{1}{\text{N}}\) ƩYi−j, \(\frac{1}{\text{N}}\) ƩZi−j. A universal proximal surface was formed by connecting the points with averaged coordinate values using spline curves. (C) The reconstructed crown model was integrated with a universal root to form a 3D tooth model. This 3D tooth model was printed for the following experiment.
Hence, we further designed a universal digitized proximal surface, which was obtained through image analysis and data fitting from imaging database. As shown in Fig. 3B, the CBCT images of 20 adult male patients (18–32 years) with intact right maxillary first molars were collected from the Affiliated Stomatology Hospital, Zhejiang University School of Medicine. The exclusion criteria were that the right maxillary first molar was affected by malformation, caries, or malocclusion. Based on the gray values of CBCT images, the proximal surface of the corresponding crown was extracted. Feature points uniformly distributed over the proximal surface were designated, and a unified 3D coordinate system was established to provide coordinate values of feature points. Thereafter, feature points form 20 proximal surfaces were collected and fitted in the unified 3D coordinate system, where the mean coordinate values of the corresponding feature points with same row and column numbers were computed (Table 1), and a universal proximal surface was formed by connecting the points with averaged coordinate values using spline curves. Tooth replica with universal proximal surface was printed and universal shape memory matrix band was fabricated. The reconstructed crown model with customized or universal proximal surface was integrated with a universal root to form a 3D tooth model (Fig. 3C). This 3D tooth model was printed for programming the shape memory matrix.
In vitro class II restoration in customized dental model
Furthermore, the both shape memory matrix bands mentioned above were fabricated and conducted an in vitro experiment. For standardization, the tooth replica composed of a individual crown, which was retrieved from CBCT images of a healthy right first molar and visually prepared with a Class II cavity in software, and a universal root, which was designed to fit the socket of the plastic alveolar base. This model was then 3D printed and placed into the socket of plastic dental model for in vitro experiment as shown in Fig. 4A. The tooth repaired with universal and customized shape memory matrix had good proximal emergence profile (Fig. 4B). Quantitative analysis showed that the universal and customized groups achieved better results than other two groups, and the proximal surface of the teeth repaired with metal matrix had the largest suspension area (Fig. 4C,D). With universal dynamometer (MTS, USA) detecting the adjacent position and tightness13, we obtained the Force-Distance curve (Fig. 4E), showing that the customized shape memory matrix group had the closest tightness to the original tooth, followed by the universal shape memory matrix (Fig. 4F). The customized and universal shape memory matrix obtained no significant different proximal contact point with the original tooth, better than the other two groups (Fig. 4G).

In vitro class II restoration in customized dental model. (A) Standard class II cavity restoration images of traditional metal matrix, sectional matrix, universal shape memory matrix and customized shape memory matrix. The proximal profile was marked with red lines. (B) Radiograph of the resin restoration in four groups. (C) The fitting of restored teeth and control tooth replica using scanning images. (D) Quantitative analysis of the accuracy of class II cavity restoration with four matrix systems. (E) The curves of the position and tightness of adjacent points tested by universal dynamometer. (F) Relevant statistics of force and (G) the distance of the proximal contact point. N ≥ 4.
Discussion
Direct resin restoration follows the principle of minimally invasive medicine, which preserves more healthy dental tissue. However, the accuracy of the final outcome of restoration is often exquisitely associated with the selection and placement of traditional matrix, which is quite technique-sensitive, sometimes time-consuming, especially for the beginners14. In clinical practice, improper proximal contact and overhangs may still exist due to the identical shape of traditional matrix band and improper operation, which could result in food impaction along with recurrent caries and periodontal problems4. Pre-contoured matrix band is more optimal for better supporting the marginal ridge than a straight matrix15. However, neither traditional sectional matrix nor circumferential matrix band system is able to obtain preferable proximal contour, especially when the proximal cavity overextend to the buccal or lingual side16. In this study, we demonstrated that the shape memory matrix band easily obtained anatomical proximal surface profile from our recruited clinical image data. Accuracy is ensured due to excellent shape memory performance of PCLDA, including intact shape reproduction and shape recovery ratios higher than 95%.
Also, during the placement, a significant proportion of patients may feel uncomfortable caused by the compression or even damage to gingiva, particularly for children5. And this discomfort can be exacerbated by the necessary use of auxiliary tools, such as separation ring and interdental wooden wedge, which are needed to keep retention and compensate for the thickness of matrices6. Shape memory matrix greatly reduced the difficulty to tightly wrap around the cavity. It can recover to the preprogrammed shape in response to thermal stimulation under suitable temperature for oral cavity within approximately 20 s. Because of its pre-contoured shape, auxiliary tools like wedge is not necessary.
Moreover, customized inlay, crown or matrix band usually means longer waiting time and higher expense, making it inconvenient for the chairside restoration. Therefore, we explored the universal digitized shape memory matrix band. In this study, the universal shape memory matrix bands had the same repair effects with the customized ones, indicating the introduction of patient data provides the opportunity of personalized treatment.
In terms of clinical practice, the shape memory matrix is reusable after ultraviolet disinfection, with stable recovery rate after multiple use. In all, our shape memory matrix successfully meets the demand of ideal matrix band system including requiring minimal auxiliary tools and possessing properties including customized anatomical configuration and self-retention17. Therefore, we believed the universal shape memory matrix has a broad industrialization prospect as a dental instrument.
However, certain limitations should be acknowledged in our current study. To obtain a more representative proximal surface profile, the sample size for the existing shape memory matrix is not large enough. The process of data extraction and integration is done manually, which is tedious and time-consuming. Therefore, it is more efficient and convenient to develop an algorithm for extracting the proximal anatomical shape automatically. Besides, as all the restoration treatments with different matrix systems were conducted on in vitro models, more validated randomized clinical trials are required in the future.
Data availability
All data generated or analysed during this study are included in this published article and its supplementary information files.
References
Peres, M. A. et al. Oral diseases: a global public health challenge. Lancet 394(10194), 249–260 (2019).
Angeletaki, F., Gkogkos, A., Papazoglou, E. & Kloukos, D. Direct versus indirect inlay/onlay composite restorations in posterior teeth. A systematic review and meta-analysis. J. Dent. 53, 12–21 (2016).
Brackett, M. G., Contreras, S., Contreras, R. & Brackett, W. W. Restoration of proximal contact in direct class II resin composites. Oper. Dent. 31(1), 155–156 (2006).
Chuang, S.-F., Su, K.-C., Wang, C.-H. & Chang, C.-H. Morphological analysis of proximal contacts in class II direct restorations with 3D image reconstruction. J. Dent. 39(6), 448–456 (2011).
Bhatia, H. P., Sood, S., Sharma, N., Singh, A. & Rajagopal, V. Comparative evaluation of clinical efficiency and patient acceptability toward the use of circumferential matrix and sectional matrix for restoration of class II cavities in primary molars: an in vivo study. Int. J. Clin. Pediatr. Dent. 14(6), 748–751 (2021).
Loomans, B. A. C., Opdam, N. J. M., Roeters, E. M., Bronkhorst, F. J. M. & Dörfer, C. E. A clinical study on interdental separation techniques. Oper. Dent. 32(3), 207–211 (2007).
Behl, M., Razzaq, M. Y. & Lendlein, A. Multifunctional shape-memory polymers. Adv. Mater. 22(31), 3388–3410 (2010).
Mather, P. T., Luo, X. & Rousseau, I. A. Shape memory polymer research. Annu. Rev. Mater. Res. 39(1), 445–471 (2009).
Xie, T. Recent advances in polymer shape memory. Polymer. 52(22), 4985–5000 (2011).
You, D. et al. 4D printing of multi-responsive membrane for accelerated in vivo bone healing via remote regulation of stem cell fate. Adv. Funct. Mater. 31(40), 2103920 (2021).
Song, H. et al. Synergetic chemical and physical programming for reversible shape memory effect in a dynamic covalent network with two crystalline phases. ACS Macro Lett. 8(6), 682–686 (2019).
Zhang, G. et al. Exploring dynamic equilibrium of Diels-Alder reaction for solid state plasticity in remoldable shape memory polymer network. ACS Macro Lett. 5(7), 805–808 (2016).
Kampouropoulos, D., Paximada, C., Loukidis, M. & Kakaboura, A. The influence of matrix type on the proximal contact in class II resin composite restorations. Oper. Dent. 35(4), 454–462 (2010).
Almushayti, M. & Arjumand, B. Operators’ ease and satisfaction in restoring class II cavities with sectional matrix versus circumferential matrix system at Qassim University Dental Clinics. Cureus 14(1), e20957 (2022).
Loomans, B. A. C., Roeters, F. J. M., Opdam, N. J. M. & Kuijs, R. H. The effect of proximal contour on marginal ridge fracture of Class II composite resin restorations. J. Dent. 36(10), 828–832 (2008).
Alonso, V., Caserio, M. & Darriba, I. Use of transparent tips for obtaining tight proximal contacts in direct class II composite resin restorations. Oper. Dent. 44(5), 446–451 (2019).
Peumans, M., Venuti, P., Politano, G. & Van Meerbeek, B. Effective protocol for daily high-quality direct posterior composite restorations. The interdental anatomy of the class-2 composite restoration. J. Adhes. Dent. 23(1), 21–34 (2021).
Acknowledgements
We thank Xiaoling Chen, Weikun Fang and Ziming Xu, Stomatology Hospital of Zhejiang University, for the support on primary material collection.
Funding
This work was financially supported by Natural Science Foundation of Zhejiang Province (LY22H140005), National Natural Science Foundation of China (82201122, 81900974, 82001046), Medical Health Science and Technology Project of Zhejiang Provincial Health Commission (2021KY191), the Key Research and Development Program of Zhejiang (No. 2023C03072).
Author information
Authors and Affiliations
Contributions
C. Liu, contributed to design, conception, data acquisition, analysis, interpretation, drafted and critically revised the manuscript; D. You, B. Feng, contributed to design, data acquisition, analysis, and interpretation, drafted the manuscript; G. Ye, Q. Huang, L. Lin, contributed to interpretation and drafted the manuscript; Y. Wang, T. Zhu, J. Wu contributed to data acquisition and drafted the manuscript; H. Yang, W. Zhang contributed to design, conception, analysis, interpretation and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Liu, C., Huang, Q., Feng, B. et al. Digitized thermo-responsive shape memory matrix band for tooth restorations. Sci Rep 15, 2523 (2025). https://doi.org/10.1038/s41598-025-85459-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-85459-4
