
Abstract
The characteristics of spontaneous movements in infants are essential for the early detection of neurological pathologies, with the Prechtl method being a widely recognized approach. While the Prechtl method is effective in predicting motor risks, its reliance on the evaluator’s expertise limits its scalability, particularly in low-income areas. In such contexts, the use of inertial sensors combined with automated analysis presents a promising accessible alternative; however, more research is necessary to get results comparable to those of the Precht method. This research aims to determine the more important metrics of trunk and limbs to assess spontaneous movement in healthy infants during the first semester of life as the basis of a sensor-based alternative. It was a cross-sectional study with 116 separate subjects divided into 3 groups: 0 M Group (N = 43), 3 M Group (N = 44), and 6 M (N = 29). Participants’ movements were recorded using 6 wireless inertial sensors (4 limbs, thorax, and pelvis). Parameters from the acceleration signal were estimated in relation to velocity, cross-correlation, kurtosis, skewness, area, and periodicity. The different stages (0 M,3 M, and 6 M) have different profiles of accelerometric parameters. Trunk and limb parameters can differentiate between 0 of 3 months (13/25 trunk and 17/36 limb parameters) and between 0 and 6 months (10/25 trunk and 20/36 limb). Mainly, trunk parameters can differentiate between 3 and 6 months (9/25 trunk vs. 3/36 limb). Additionally, only 2 trunk parameters (kurtosis and periodicity) can differentiate the 3 stages. Wearable devices can effectively detect significant differences in spontaneous movements during the first six months of life, particularly trunk-related data. The extremities could be insufficient to distinguish movements between 3 and 6 months. On the other hand, two key parameters—kurtosis of thorax velocity and periodicity of trunk velocity—successfully differentiate between the three age groups analyzed.
Similar content being viewed by others


Introduction
Currently, there is great interest in the early detection of predictive signs of developmental disorders in infants at risk since this allows an early intervention when the nervous system (NS) has greater plasticity1. The young infant has a specific development of the NS in each stage, which opens an opportunity to characterize spontaneous or induced behavior with sensitive and specific evaluations for clinical decision-making2. The spontaneous movements are all movements without any induction by an external agent (reflex, tasks, etc.), and the general movements(GMs) are a subset of these spontaneous behaviors3.
Babies show specific and well-defined characteristics in the development of their spontaneous movements during the first six months of life. These movements (GMs) are notable for their complexity, variability, and repetitiveness during this early stage4. Spontaneous motor activity and general movements follow a predictable timeline5,6. In normal development between 0 and 2 months, they present general movements known as “writhing” characterized by moderate amplitude and speed, high complexity and variability, and their motor skills are initially of great amplitude and lack of medialization, while at 2 to 5 months, these evolve into “fidgety” movements, which present circular shapes, mild amplitude, low speed, and high variability in acceleration, also characterized by reaching midline alignment at 3 months7, and between 4 and 6 months, they begin to reach for objects8, differentiating limb movements9. This progression gradually changes toward greater motor control as general movements fade. There are clear distinctions between gross movements and spontaneous movements throughout development1.
Assessment of spontaneous movements can be performed using tools such as ultrasound (fetal movement), neurological examinations, and the Prechtl method for assessing general movements. GMs are an integral part of the spontaneous movement repertoire of the entire body. When the nervous system (NS) is injured, GM loses its characteristic complexity and variability, becoming monotonous, restricted, and patternless5. The Prechtl method is currently the most cost-effective method for GM assessment, with a sensitivity of > 91% and a specificity of > 81%6,10.
However, this type of evaluation has been questioned due to its subjectivity, as it requires an experienced evaluator10 and a second opinion from an expert11. Moreover, it has limitations for its implementation, generalization, and global utility10,12,13,14, limiting its use in clinical practice15,16. For this reason, experiences with accelerometers and other accessible and low-cost technologies have been implemented to find an objective and feasible model based on the GMs’ description3,13,17. Recording the spontaneous movement of limbs at different age ranges mainly up to 3 months, researchers have demonstrated3,18 these technologies’ feasibility of use, substantial changes over time, and differences with the pathological development3,14.
Today, technology allows the use of small, light, and wireless inertial sensors so as not to interfere with the infant’s movements19,20; however, these accelerometric parameters, based mainly on the energy (acceleration, area, skewness), frequency (periodicity), variability (kurtosis) and coordination(cross-correlation), have not reported a sensitivity and specificity comparable to GMs. Additionally, there are two important knowledge deficits using this sensor information in typical development; (1) lack of trunk information, despite the importance of the trunk in motor development21, the literature mainly reports limbs’ movements3,18,22 ; and (2) it is not clear if the accelerometer parameters can differentiate infants before and after the disappearance of GMs after 5 months (most of the comparison are before 3 months)3,11,14.
The objective of the study was to determine the variables of trunk and limbs that can differentiate stages of spontaneous movement in healthy term infants from 0 to 6 months of age. We hypothesize a clear differentiation with accelerometry between these different stages, particularly using trunk variables.
Methodology
Study design and participants
This was a cross-sectional study of three different developmental times within the first semester of life. We invited families with infants between 1 day to 6 months of age who were born at El Carmen Hospital in Santiago, Chile, between August 2018 and November 2019. Each participant attended with a caregiver once without a follow-up. A total of 116 subjects were classified into 3 different groups according to their post-term age. The first group, called “0 M” (0 months), comprised 43 infants between 1 day to 4 weeks. The second group, called “3 M” (3 months), comprised 44 infants from 9 weeks to 15 weeks. The third group, called “6 M” (6 months), comprised 29 infants between 23 weeks and 29 weeks (Fig. 1A). This categorization was based on the evolution of Prechtl’s movements.

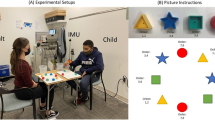
Experimental setup for data collection. (A) Room, elements used for data collection, and weeks of assessment per group. (B) Location of inertial sensors on the body. The green circles show the location of the inertial sensors used. GMs = General Movements, T = Thorax, P = Pelvis, RUE = Right Upper Extremity, LUE = Left Upper Extremity, RLE = Right Lower Extremity, LLE = Left Lower Extremity.
Participants were invited via a phone call using the hospital’s database and then assigned to one of the three groups described above. The inclusion criteria regarding pregnancy were no multiple pregnancies, pregnancy control from the third month, no drug use (alcohol, marijuana, etc.), no complications (placental abnormalities, hemorrhages, hypertensive pregnancy syndrome, gestational diabetes, among others); regarding delivery, the criteria were normal, induced or cesarean delivery, without rupture of the amniotic sac within 12 h of delivery, without infection; regarding the participants, criteria were birth between 37 and 42 weeks, weight greater than 2.5 kg, infants without an orthopedic disorder, hemorrhage or malformations of the central nervous system, hypoxic-ischemic encephalopathy, or alterations in other systems that could alter movement (cardiorespiratory or digestive disorders, among others). Parents or legal guardians signed informed consent from all subjects for both study participation and publication of identifying information/images. The Scientific Ethics Committee of the Central Metropolitan Health Service approved the informed consent. The work has been carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki).
Experimental setup
Data collection was carried out in a specially-conditioned room (see Fig. 1) at a temperature of 29 °C, with adequate lighting, without environmental noise, and without environmental stimuli that could cause non-spontaneous movements18. The subject was placed in a supine position on a tatami measuring 106 × 106 cm (2.5 cm thick, foam of density 95 kg/m3). The measurement conditions were the following: being awake, calm, wearing a diaper, and having been fed 1 to 2 h before the measurement16. If these conditions were not met, the process was repeated up to a maximum of 3 attempts. The recording was made for 5 min, always in the presence of the caregiver but outside the visual field of the infant. Movement of the distal limbs and trunk was recorded during the spontaneous behavior of the infants. Six small and light wireless inertial measurement unit (IMU) sensors (Wear Notch Pioneer kit) were attached by hypoallergenic tape in the ankles (distal anterior leg, above malleolus), wrists (distal dorsal forearm, like a watch), pelvis (anterior midline, between Anterior Superior Iliac Spines), and thorax (at the center of the sternum) of infants to get the 3D acceleration of Upper Extremities, Lower Extremities, and Trunk (see Fig. 1B). The sampling rate used was 100 fps. The sensors were calibrated according to the manufacturer’s suggestions in a calibration routine where the sensors were rotated in a figure-eight pattern.
Analysis
Accelerometry data were analyzed in Python (Python Software Foundation, Beaverton, United States) using our own codes. For the analysis, we used RUE, LUE, or BUE as acronyms for the Upper extremities sensors, meaning Right, Left, or Both Upper Extremities, respectively. Similar acronyms were used for the Lower extremities (RLE, LLE, and BLE). For the trunk, we used T for thoracic motions, P for pelvic motions, and Trunk when we analyzed P and T together.
First, the accelerometry signal (raw data is gravity removed) was filtered using a bidirectional filter without offset (4th order Butterworth, high pass of 0.1 Hz and a low pass of 20 Hz).
Additionally, we applied a noise threshold of 0.2 m/s2 (or -0.2 m/s2 for negative values) or deadband zone23, with the purpose of converting the basal noise into values equal to zero, to avoid the problem of cumulative error, particularly for the velocity estimation from the accelerometers.
From the filtered and cleaned signal, 36 parameters were calculated based on the 3D acceleration of each limb following the analyses developed by Meinecke et al.22, Heinze et al.18, and Bultmann et al.3. In these studies, 6 parameter categories (36 variables) are estimated because they have been related to some characteristics of the writhing and fidgety movements. These categories are the following:
-
a.
Acceleration and velocity. Filtered and noise rejected 3D acceleration and the integral of the acceleration time series. For each segment, we combined the x, y, and z axes using the Euclidean norm of acceleration or velocity. The values of acceleration and velocity depict the capacity to control forces in time adjusted to internal or external demands. Usually, the maximum and minimum values increase during the development, augmenting the range of possibility of this control.
-
b.
Cross-correlation. It is a measure of similarity between 2 signals. It reflects the degree of synchronization between 2 segments in time. In relation to cross-correlation, if we observe synchronized movements between segments, could characterize two different kinds of control. In newborns, the cross-correlation is high because they have a global pattern of motion without selective control. On another hand, at the end of the first semester, the cross-correlation is high because they have more interlimb or intersegmental coordination. Therefore, high values of cross-correlation should be interpreted together with other parameters.
-
c.
Skewness of acceleration and velocity. It is the measure of the degree of symmetry of the distribution with respect to the mean. If the value is close to 0, the distribution is symmetrical; if it is positive, it means that the data accumulates to the left, and if it is negative, it means that the data accumulates to the right.
If the infants do not prefer a specific velocity, the Skewness is symmetrical; however, if they choose lower values preferentially, the skewness is asymmetric and positive.
For example, in the extremities, as the baby grows, the movements become smoother, then the infants prefer lower values in their distribution (energy optimization).
-
d.
Kurtosis of acceleration and velocity. Measure of the data distribution’s tailedness in relation to the normal distribution. A positive Kurtosis indicates a greater concentration of similar values, while a negative Kurtosis indicates a distribution with wider and homogeneous values. As the infants grow, they become softer and more coordinated, then they prefer lower values of acceleration and velocity in their limbs.
-
e.
Periodicity of velocity. It is quantified by the number of intersections of the velocity signal with the average of this signal calculated in windows of 1000 frames (moving window). The purpose of the periodicity is to determine the regularity and frequency of the motions in time.
It refers to the fact that in each period of time, how many times a motor response appears. As the infant grows, the periodicity should increase compared to newborns in healthy development.
-
f.
Area outside the mean or standard deviation of velocity. It is a metric computed by subtracting the area of the velocity signal with the moving average or the moving standard deviation of the signal. We used a moving window of 100 frames. The purpose was to estimate the amplitude variability of motions. This variable increases after birth, meaning the older infants can control the motion energy or amplitude. This control differs between the trunk, arms, and legs, reflecting the unique developmental trajectories of each body part.
The details of all these parameters are found in Bultmann et al. 2019, Meinecke et al., 2006, and Tables 2 and 33,22.
Additionally, 25 similar variables were estimated in the trunk, using the thorax and pelvis sensors and applying the 6 categories explained above.
All these variables were analyzed in each participant, and then individual data were grouped by age stage for statistical analysis. There was no follow-up of each participant; therefore, there was a cross-sectional recording in each age group.
Statistical methods
Before the statistical analysis, we removed the outlier data of each parameter using a threshold of 1.5 times of IQR above the upper quartile (75th percentile) and below the lower quartile (25th percentile).
The processed variables were then also analyzed in Python with the Pingouin library, using the Shapiro-Wilk test to check the normality of the data distribution and then a 1-way ANOVA test comparing the 3 age groups. After that, a Dunn-Sidak post hoc analysis was performed. Partial eta squared was used as an effect size metric.
A principal component analysis (PCA) was performed to obtain the weight of the different variables in each principal component, calculated in Python with the TensorFlow library within each age group and between the age groups for the trunk and limbs variables of acceleration, velocity, cross-correlation, skewness, kurtosis, periodicity, and area outside the velocity’s mean and standard deviation. The first step was to center and scale each variable individually (centering the dataset to make the variables have a mean equal to zero and scaling the dataset to make the standard deviation equal to one), and then calculate the PCA24. We estimated the weight of each variable per age group. Then, we estimated the weight in relation to the age variations (0 M vs. 3 M, 0 M vs. 6 M, 3 M vs. 6 M). As the subjects were different across age groups, we performed a permutation analysis with 1892 repetitions to obtain values of variation between the ages of 0-3 M and 3-6 M before performing the PCA that considers all possible crosses of subjects.
Results
The demographic features of the groups, such as birth weight, head circumference, and sex distribution, are shown in Table 1. The detailed results of movement variables are shown in Table 2 for the trunk and in Table 3 for the extremities. Additionally, Tables 1 and 2 of Supplementary Material have the p values and effect size (partial eta square) of the group comparisons for trunk and extremities variables.
Comparison of trunk movement between groups
The parameters of the thorax and pelvis in the 3 study groups were compared (Fig. 2). Table 1-Suplementary Material shows the p-values. When comparing groups 0 M-3 M, 3 M-6 M, and 0 M-6 M, we can highlight that there are 2 parameters out of 25 that can clearly differentiate the 3 groups in their spontaneous movements: the Kurtosis of the velocity of the thorax and the Periodicity in the velocity of the trunk (thorax-pelvis). There are 17 parameters that can differentiate 0 M-3 M groups, 9 parameters 3 M-6 M groups, and 10 parameters 0 M-6 M groups.

Trunk parameters by group. (A) Radar plot showing the scaled values per variable by age. (B) Variables with significant differences between age groups. White squares depict non-significant differences. The colorbar represents p-values of significant differences.
The most representative parameters for each group are described below:
0 M Group. The variables with values significantly higher than the 3 M and 6 M groups are the Minimum acceleration of the thorax and the Skewness of the acceleration of the thorax. Also, the significantly smaller variables are Maximum acceleration of the pelvis and Maximum acceleration of the thorax, Maximum velocity of the pelvis, Median acceleration of the thorax, Kurtosis of the velocity of the thorax, and Periodicity in the velocity of the trunk.
3 M Group. The parameters with significantly higher values than the groups 0 M and 6 M are the Median acceleration of the pelvis and the Periodicity in the velocity of the trunk. Additionally, significantly lower parameters, such as Minimum acceleration of the pelvis, Kurtosis of the acceleration of the thorax, and Kurtosis of the velocity of the thorax stand out.
6 M Group. A significantly higher variable than the 0 M and 3 M groups is the Maximum velocity of the thorax. The parameters Kurtosis of the velocity of the thorax and Periodicity in the velocity of the trunk have intermediate and significantly different values compared to the other groups. The significantly lower value than the 0 M and 3 M is the Cross-correlation of acceleration between thorax and pelvis.
There are also several values that partially differentiate groups (e.g., 0 M vs. 3 M, but not 0 M vs. 6 M) that are not described in the text but can be seen in Fig. 2.
Comparison of extremities’ movement between groups
When comparing between groups, none of the 36 parameters used can differentiate the 3 groups for the spontaneous movement of infants (Fig. 3). Table 2-Supplementary material contains the p-values of the statistical comparisons.

Extremities parameters by group. (A) Radar plot showing the scaled values per variable by age. (B) Variables with significant differences between age groups. White squares depict non-significant differences. The colorbar represents p-values of significant differences.
There are 18 parameters that can differentiate the 0 M-3 M groups and 20 parameters that differentiate the 0 M-6 M groups. Only 3 variables can differentiate the 3 M-6 M groups.
For the extremities, the most representative parameters per group are summarized below:
Group 0M. There are significantly higher values than 3 M and 6 M, such as the Minimum acceleration of the extremities, the Minimum velocity of the extremities, and the Cross-correlation values of the acceleration between the extremities (parameters 9,15–18 Table 3). Also noteworthy are significantly lower values than 3 M and 6 M, such as Skewness of the acceleration of the lower extremities, Skewness of the velocity of the upper extremities, Kurtosis of the velocity of the upper extremities, and Periodicity in the velocity of the upper extremities.
Group 3M. No parameter can simultaneously differentiate this group from the other 2 groups (0 M and 6 M).
Group 6M. There are significantly higher values than 0 M and 3 M, such as the Skewness of the acceleration of the upper extremities and the Kurtosis of the acceleration of the upper extremities. The Cross-correlation of the velocity of LUE and RLE is significantly lower than in the other groups.
The parameters that partially differentiate the groups are not described in the text but can be seen in Fig. 3.
The contribution of the trunk and extremities (PCA)
For each age group, we analyzed the variables that provide more information by combining the trunk and extremities data. For this, the first 10 variables with the highest variance were tabulated, differentiating the variables of trunk and extremities, represented in Fig. 4. The figure highlights the importance of trunk variables in groups 0 M and 3 M (5/10, 7/10, and 3/10 for groups 0 M, 3 M, and 6 M, respectively).

Principal Component Analysis (PCA) of trunk and extremities parameters by age (First 10 variables).
It can be noted that within the first 4 most significant parameters in the 3 age groups, 8/12 correspond to the trunk, highlighting the parameters of skewness and cross-correlation.
Finally, we performed a similar analysis, but comparing between groups (0 M-3 M, 3 M-6 M and 0 M-6 M). The results are shown in Fig. 5. Again, the importance of the trunk variables stands out (5/10, 5/10 and 4/10 for the contrasts 0 M-3 M, 3 M-6 M and 0 M-6 M, respectively).

Principal Component Analysis (PCA) of trunk and extremities parameters by group contrasts (First 10 variables).
We can also highlight that, within the 4 most significant parameters in each of the contrasts, 9/12 corresponds to trunk data, again highlighting skewness and cross-correlation parameters.
Therefore, the information provided by the mobility of the trunk (thorax and pelvis) is equally or more relevant than the one provided by the extremities to analyze spontaneous sensorimotor behavior in the first semester of life.
Discussion
Our results demonstrate a clear differentiation of healthy term infants at 0, 3, and 6 months of age, using accelerometry to characterize spontaneous movement. Only trunk variables could differentiate the 3 developmental infant stages. Also, when we weigh the trunk and extremities’ parameters in a PCA model, the mobility of the trunk is equally or more relevant than that of the extremities.
The present study demonstrates that several of the parameters of spontaneous limb movement proposed by previous research3,18,22 can differentiate the chosen age groups, although any of the limb parameters can differentiate the 3 age groups. The inclusion of trunk data improves the differentiation between the 3 groups. The trunk variables that can differentiate the 3 age groups are the Kurtosis of the velocity of the thorax and the Periodicity in the velocity of the trunk.
The PCA applied to the limbs and trunk parameters highlights how the main differentiators of spontaneous movement correspond to trunk parameters in the first trimester. We did not find previous studies using these trunk variables. However, there are other studies that use videos to obtain trunk information25,26.
Other studies on infant development using voluntary and involuntary movements also highlight the importance of the trunk to describe the different stages of the first semester4,8,27. Babies in the first trimester experience significant changes in trunk movement in the sagittal plane and then between 3 and 6 months in the frontal plane for purposeful sensorimotor activities such as reaching28,29,30.
The kurtosis of the velocity of the thorax decreases at 3 months and then slightly increases at 6 months, being able to differentiate the 3 ages. At 0 months, it is positive (leptokurtic), reflecting low variability of the velocity. At 3 and 6 months, it becomes less positive than at 0 months, indicating more variability in the speed control, which is probably related to the selection of a more flexible control strategy than at 0 months, All these changes can reflect a better neuromotor organization or motor control that is consistent with the maturation of postural control4,25, changes in general movements, medialization7,31, and evolution of functional tasks such as reaching and grasping4.
The Periodicity in the velocity of the trunk increases at 3 months and then decreases at 6 months, also differentiating the 3 groups. This reflects that at 3 months, the number of trunk movements increases compared to 0 months, followed by an efficient refinement of the number of movements at 6 months. This pattern indicates that between 0 and 3 months, trunk motor responses evolve to allow more motor exploration. By 6 months, the decrease in periodicity suggests enhanced postural stability, greater movement efficiency, and increased motor precision, particularly in the upper limbs and upper trunk32.
Several parameters do not show a linear increment or decrement in the 3 age stages; some of these parameters increase at 3 months and then decrease at 6 months or vice versa. This can be interpreted as a controlled exploration stage at 3 M and the selection of a preferential and flexible strategy at 6M4,27. This could be the result of the change to fidgety movements and better postural control, allowing greater motor smoothness8,27,30.
Unlike the trunk parameters, no extremity parameter can differentiate the 3 age stages evaluated. The extremity parameters allow us to differentiate mainly 0 M vs. 3 M and 0 M vs. 6 M, but the 3 M-6 M contrast partially. Other studies do not measure at 6 months using IMUs, so there is no literature for the 3 to 6 months’ period to compare it3, despite this period’s importance since Fidgety-type movements disappear at 18 weeks.
The velocity and the acceleration in the upper and lower extremities increase between months 0 and 3, and some of these parameters decrease (e.g. feet’s median acceleration) or increase (e.g. maximum acceleration of all extremities) in the 3 M-6 M period. Consistent accelerometry findings with our 0 M to 3 M data have been found by Bultmann et al.3. They studied premature babies without risk factors with measurements between months 0 and 4 through wired accelerometers located in the upper limbs and lower limbs, and they found that acceleration and velocity increased between both periods.
In our study, cross-correlation as a metric of synchronization decreased in the extremities during the first semester, with main decrements in the first 3 months. According to the maturational process, infants begin to have a slight selectivity and purpose after 3 months1,8,27,30,33. Bultmann et al.(2019) also found a decrease in the cross-correlation of the limbs between months 0 and 4 in healthy preterm infants, which they interpret as a sign of a global decrease in synchrony, which is in turn related to an increase in the variability of motor behavior. Our values present ranges similar to this study and others3,34. Disselhorst-Klug et al.(2012) report an increase in the cross-correlation of acceleration between the left and right lower limb between months 1 and 3 and then a decrease from months 3 to 5, which differs from Bultmann et al.(2019) and our results3,17. A possible explanation for this difference is the location of the sensors, as we placed them before the distal segment (distal forehand and shank), but they placed them in the distal segment (hand and foot)3,17. Also, we used wireless sensors, and they utilized wired sensors.
Regarding limb speed skewness, our results show that it increases as infants develop. The successive disappearance of writhing and fidgety movements1,5,6 may be related to this increase and to the appearance of movements with greater postural adjustment and selectivity27,30,35. On the other upper limb, Disselhorst-Klug et al.(2012) found that the skewness of the feet increased continuously between months 0 and 5, with a greater variation between months 3 and 5. For Bultmann et al.(2019), the skewness of acceleration and speed of the upper limbs and feet decreased significantly between months 0 and 4. Therefore, our results are similar to Disselhorts-Klugs’ and opposite to Bultmann et al.’s. We interpret this decrease as the optimization of energy due to the low-speed motion preference3,17.
Our results also show a progressive increase in kurtosis among age groups, depicting a greater preference for smaller values of speed or acceleration. We observed in our data distributions a mix of right skewness and higher kurtosis, then the older infants prefer smooth movement.
However, Bultmann et al.(2019) reported a significant decrease in kurtosis of acceleration of limbs between months 0 and 43.
In our results, the periodicity of the velocity of the upper and lower limbs’ velocity increased significantly from months 0 to 3, with no change from months 3 to 6. In Disselhorst-Klug et al. no variation in periodicity was found when comparing between months 0, 3, and 5. However, Bultmann et al., who evaluated from 0 to 4 months, found that the periodicity in the velocity of the upper limbs and feet increased significantly, similar to our results17. These can be the result of an increment in limb frequency of motions in the first trimester.
Regarding the area parameters, we observed no important variation for the limbs, which is similar to Bultmann et al.3. This metric is probably more sensible to abnormal motions.
Overall, the infants are refining and optimizing the control of extremities during the first semester, and they exhibit the main changes in the first 3 months, seen in the increase of Skewness and Kurtosis parameters and the decrease of Cross-correlation.
A large number of studies have made efforts to determine the differentiation of ideal spontaneous movement and risk, comparing records in healthy and pathological populations and establishing differentiated motor behavior algorithms. However, we consider it essential to demonstrate that the parameters that describe the general movements change within the typical development, mainly when these spontaneous movements disappear (after 5 or 6 months). One of the aims of this study was to verify this.
In the present study, two trunk sensors were incorporated since the development of postural control is what allows purposeful changes and greater extremities’ control4,27,29. In order to analyze the transition through the writhing, fidgety, and purposeful stages, we performed a PCA analysis of the variation of all the variables between different contrasts of the registered months (0-3-6 M). The parameters that clearly determine the 3 groups mostly correspond to parameters of the trunk, mainly skewness and cross-correlation variables.
Heinze et al.’s(2010) study with accelerometers on healthy and premature babies of 0, 3, and 5 months of term at risk establishes a genetic algorithm to determine the best combination of the movement parameters described by Meinecke et al.18,22. Heinze et al. propose that the best combination of parameters for the limbs includes cross-correlation of acceleration and skewness of the acceleration; they also propose area and acceleration variables, with the third best combinatorial including the maximum acceleration of all limbs and the minimum velocity of all limbs18. These results are partially similar to our PCA results.
The typical infant movement is highly variable and complex, but voluntary movements are not adapted to the demands of the environment during the first trimester4,27. From 3 to 6 months, a transition period is described where there are better postural adjustments, as well as selectivity and recruitment of limbs for voluntary movements8,27,30,33. This could explain the differences between 0 and 3 and 3–6 months of age in the parameters analyzed, which is supported by maturational evolution of the NS that changes general movements36. This is consistent with the achievements for 3 months such as gaze stabilization and antigravity activity, which explain the transition from spontaneous movements to voluntary movements37.
Among the limitations of our study, a follow-up of each infant was not carried out, but it was done on cohorts of each age stage. On the other hand, the sample only includes typical children, so there is no contrast with risky or pathological motor behavior. The analysis was based on the parameters used by Heinze et al.(2010) and Bultmann et al.(2019), with some methodological variations (such as the sensor locations, and trunk parameters)3,18.
In conclusion, wireless accelerometry can detect significant differences in the changes of spontaneous movements (without associated stimuli) during the sensorimotor maturation process of infants in their first semester of life. Only two trunk parameters can differentiate between 0 M vs. 3 M, 3 M vs. 6 M, and 0 M vs. 6 M. The limb variables mainly explain the variation between 0 M vs. 3 M and 0 M vs. 6 M. When we compared the weight of trunk and limb parameters, we concluded that the trunk parameters were equal or more important than the limb ones.
Due to its characteristics, wireless accelerometry could be a viable system for screening infants, making them less dependent on trained professionals18. For this system to be implemented, we should determine behavior algorithms that allow us to discriminate between normal, risk, and atypical movement in a future study in which these data can be contrasted with infants with developmental disorders.
Data availability
The data reported here could be available at reasonable request and within relevant legal constraints. Please contact Pablo Burgos (burgosp@uchile.cl) for requests.
References
Hadders-Algra, M. General movements: a window for early identification of children at high risk for developmental disorders. J. Pediatr. 145, S12–18 (2004).
Cioni, G., D’Acunto, G. & Guzzetta, A. Perinatal brain damage in children: neuroplasticity, early intervention, and molecular mechanisms of recovery. Prog Brain Res. 189, 139–154 (2011).
Bultmann, C. S. et al. Spontaneous movements in the first four months of life: an accelerometric study in moderate and late preterm infants. Early Hum. Dev. 130, 1–9 (2019).
Dusing, S. C. Postural variability and sensorimotor development in infancy. Dev. Med. Child. Neurol. 58, 17–21 (2016).
Einspieler, C. & Prechtl, H. F. R. Prechtl’s assessment of general movements: a diagnostic tool for the functional assessment of the young nervous system. Ment Retard. Dev. Disabil. Res. Rev. 11, 61–67 (2005).
Burger, M. & Louw, Q. A. The predictive validity of general movements – A systematic review. Eur. J. Paediatr. Neurol. 13, 408–420 (2009).
Lucaccioni, L. et al. The ontogeny of limbs movements towards midline in healthy infants born at term. Early Hum. Dev. 155, 105324 (2021).
Hadders-Algra, M. Typical and atypical development of reaching and postural control in infancy. Dev. Med. Child. Neurol. 55(Suppl 4), 5–8 (2013).
Ohmura, Y., Gima, H., Watanabe, H., Taga, G. & Kuniyoshi, Y. Developmental changes in intralimb coordination during spontaneous movements of human infants from 2 to 3 months of age. Exp. Brain Res. 234, 2179–2188 (2016).
Adde, L., Rygg, M., Lossius, K., Oberg, G. K. & Støen, R. General movement assessment: predicting cerebral palsy in clinical practise. Early Hum. Dev. 83, 13–18 (2007).
Adde, L., Helbostad, J. L., Jensenius, A. R., Taraldsen, G. & Støen, R. Using computer-based video analysis in the study of fidgety movements. Early Hum. Dev. 85, 541–547 (2009).
Einspieler, C. et al. Early markers for cerebral palsy: insights from the assessment of general movements. Future Neurol. 7, 709–717 (2012).
Dusing, S. C., Izzo, T. A., Thacker, L. R. & Galloway, J. C. Postural complexity differs between infant born full term and preterm during the development of early behaviors. Early Hum. Dev. 90, 149–156 (2014).
Marcroft, C., Khan, A., Embleton, N. D., Trenell, M. & Plötz, T. Movement recognition technology as a method of assessing spontaneous general movements in high risk infants. Front. Neurol. 5, (2015).
Garcia, J. M., Gherpelli, J. L. D. & Leone, C. R. The role of spontaneous general movement assessment in the neurological outcome of cerebral lesions in preterm infants. J. Pediatr. (Rio J). 80, 296–304 (2004).
Prechtl, H. F. et al. An early marker for neurological deficits after perinatal brain lesions. Lancet Lond. Engl. 349, 1361–1363 (1997).
Disselhorst-Klug, C., Heinze, F., Breitbach-Faller, N., Schmitz-Rode, T. & Rau, G. Introduction of a method for quantitative evaluation of spontaneous motor activity development with age in infants. Exp. Brain Res. 218, 305–313 (2012).
Heinze, F., Hesels, K., Breitbach-Faller, N., Schmitz-Rode, T. & Disselhorst-Klug, C. Movement analysis by accelerometry of newborns and infants for the early detection of movement disorders due to infantile cerebral palsy. Med. Biol. Eng. Comput. 48, 765–772 (2010).
Airaksinen, M. et al. Automatic posture and movement tracking of infants with wearable movement sensors. Sci. Rep. 10, 169 (2020).
Airaksinen, M., Vaaras, E., Haataja, L., Räsänen, O. & Vanhatalo, S. Automatic assessment of infant carrying and holding using at-home wearable recordings. Sci. Rep. 14, 4852 (2024).
Bertenthal, B. & Von Hofsten, C. Eye, head and trunk control: the foundation for manual development. Neurosci. Biobehav Rev. 22, 515–520 (1998).
Meinecke, L. et al. Movement analysis in the early detection of newborns at risk for developing spasticity due to infantile cerebral palsy. Hum. Mov. Sci. 25, 125–144 (2006).
Brønd, J. C., Møller, N. C. & Grøntved, A. The Intrinsic Properties of ActiGraph Counts and Alternatives. https://doi.org/10.1123/jmpb.2023-0049 (2024).
James, G., Hastie, T., Tibshirani, R., Taylor, J. & Witten, D. Linear Regression. In an Introduction to Statistical Learning: with Applications in Python (Springer, 2023).
Blok, J. et al. Quantification of the development of trunk control in healthy infants using inertial measurement units. In International Conference on Rehabilitation Robotics (ICORR) 1–6 https://doi.org/10.1109/ICORR55369.2022.9896546 (IEEE, 2022).
Chambers, C. et al. Computer vision to automatically assess infant neuromotor risk. IEEE Trans. Neural Syst. Rehabil Eng. 28, 2431–2442 (2020).
Hadders-Algra, M. Development of postural control during the first 18 months of life. Neural Plast. 12, 99–108 (2005). discussion 263–272.
Bly, L. & Ariz, T. N. Motor skills acquisition in the first year, an illustrated guide to normal development. (1995).
Rachwani, J., Santamaria, V., Saavedra, S. L. & Woollacott, M. H. The development of trunk control and its relation to reaching in infancy: a longitudinal study. Front. Hum. Neurosci. 9, (2015).
Hadders-Algra, M. Variability in infant motor behavior: a hallmark of the healthy nervous system. Infant Behav. Dev. 25, 433–451 (2002).
Sermpon, N. & Gima, H. Relationship between fidgety movement and frequency of movement toward midline: an observational study. Early Hum. Dev. 177–178, 105718 (2023).
Kanemaru, N., Watanabe, H. & Taga, G. Increasing selectivity of interlimb coordination during spontaneous movements in 2- to 4-month-old infants. Exp. Brain Res. 218, 49–61 (2012).
de Graaf-Peters, V. B. et al. Development of postural control in typically developing children and children with cerebral palsy: possibilities for intervention? Neurosci. Biobehav Rev. 31, 1191–1200 (2007).
Gravem, D. et al. Assessment of infant movement with a compact wireless accelerometer system. J. Med. Devices. 6, 021013 (2012).
Boxum, A. G. et al. Postural adjustments in infants at very high risk for cerebral palsy before and after developing the ability to sit independently. Early Hum. Dev. 90, 435–441 (2014).
Hadders-Algra, M. Early human motor development: from variation to the ability to vary and adapt. Neurosci. Biobehav Rev. 90, 411–427 (2018).
Einspieler, C., Peharz, R. & Marschik, P. B. Fidgety movements - tiny in appearance, but huge in impact. J. Pediatr. 92, S64–70 (2016).
Acknowledgements
We thank Rocio Cerda P.T. and Maria Navarrete P.T. for coordinating and collaborating with data collection in “El Carmen” Hospital. We extend our sincere thanks to all families and infants who participated in the study. We are especially grateful to the first volunteer, Agustín Burgos and family. We sincerely appreciate the cooperation and assistance provided by the nursery unit of El Carmen Hospital, Maipú, Santiago, Chile.
Funding
The study was partially supported by Contec #78959 Corfo and Fondecyt Grant #11181337 from the National Agency for Research and Development (ANID), Government of Chile.
Author information
Authors and Affiliations
Contributions
M.M-P: conceptualization, methodology, data interpretation, visualization, writing—original draft. I.R-S.: Annotations, data collection, writing—review and editing. J.B-C: Conceptualization, data interpretation, methodology, writing—review and editing. J.C-P: data analysis, data interpretation, resources, writing—review and editing. R.Z-I: data interpretation, resources, writing—review and editing. P.I.B.: Conceptualization, methodology, supervision, data analysis, data interpretation, resources, writing—original draft.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Marín-Palma, M., Rojas-Sepulveda, I., Becerra-Caroca, J. et al. The importance of trunk motion in wearable based infant spontaneous movement analysis. Sci Rep 15, 1419 (2025). https://doi.org/10.1038/s41598-025-85621-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-85621-y
