
Abstract
This cross-sectional study aimed to investigate the association between the TyG index and both obesity indicators and hypertension among American adults. Data were drawn from 4,813 adults in the 2013–2018 National Health and Nutrition Examination Survey (NHANES). Multivariate logistic regression models indicated significant associations between TyG and obesity-related indices with hypertension. Using Cox regression analysis, we examined the relationship between TyG and obesity-related indices in relation to hypertensive prognosis, employing threshold effect analysis and fitted smoothed curves for consistency. Subgroup analyses and interaction tests were conducted. Results showed strong correlations between TyG, TyG-BMI, TyG-WHtR, TyG-WC and hypertension, with odds ratios (ORs) of hypertension rising across TyG quartiles (Q1–Q4). Cardiovascular mortality analysis revealed that TyG (HR = 1.89, 95% CI (1.03,3.51), P < 0.05) and the Q2 group (HR = 4.93, 95% CI (1.29,18.80), P < 0.05) were significantly associated with increased risk. A positive correlation between TyG and hypertension was noted below a threshold of 8.1, with inverse associations beyond this point. The TyG-BMI, TyG-WHtR, and TyG-WC exhibited positive correlations with hypertension, although weakened after reaching a certain threshold. These findings suggested that TyG and related indices are associated with hypertension and may aid in understanding risk stratification in this context.
Similar content being viewed by others
Introduction
Hypertension is one of the most common cardiovascular risk factors globally, characterized by persistently elevated blood pressure, which can lead to severe complications such as heart disease, stroke, and kidney disease1,2,3. A global report indicated that hypertension and its related complications impact over one billion people worldwide4. Even in developed countries, the prevalence of hypertension remained high. For instance, in the United States, approximately 45% of adults are affected by hypertension, resulting in significant healthcare costs and an increased strain on healthcare systems5. However, it has been reported that only about 54% of adult hypertensive patients worldwide have received a diagnosis4, highlighting that the global burden of hypertension may be far greater than current estimates suggest. This underscores the critical need to improve hypertension awareness, as well as early identification and management strategies.
The triglyceride-glucose (TyG) index was calculated as ln [fasting triglycerides (mg/dL) x fasting glucose (mg/dL)/2]. TyG index serves as a surrogate marker for insulin resistance (IR), which has been recognized risk factor for cardiovascular disease6. Glucose metabolism disorders are common in hypertensive patients7, possibly because the TyG index is associated with atherosclerosis8,9. A nine-year longitudinal study showed that higher TyG is associated with an increased risk of subsequent hypertension10. In addition, higher TyG index is significantly associated with increased risk of developing new-onset hypertension in adults11. Consequently, the TyG index offers predictive value for hypertensive disease.
Obesity poses a substantial burden on global healthcare systems12, with hypertension ranking among its common comorbidities. Relevant studies also indicate that obesity is independently associated with a significantly higher prevalence of both systolic and diastolic hypertension in adults13,14. While waist circumference (WC) and body mass index (BMI) have long been used to evaluate metabolic syndrome and central obesity, their ability to predict the risk of cardiometabolic illnesses is very restricted15. Current studies have found that the combination of obesity measures and TyG, such as the TyG-BMI, TyG-WC, and TyG-WHtR, can be used to predict hypertensive cardiovascular disease with relatively high accuracy16,17,18. However, these studies were limited to Asian and European populations, and most of them included only one indicator to explore the association with hypertension19,20,21. There is still no research on the connection between TyG and the combination of obesity indices and hypertension in the US population.
In light of the aforementioned background, this study aims to assess the cross-sectional association between the TyG index and various obesity indicators in relation to hypertension among U.S. adults. By examining these relationships, we hope to fill a significant gap in the current literature.
Methods
Study population
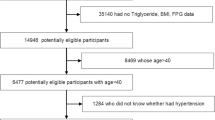
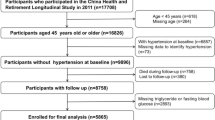
4,813 adults from the 2013–2018 NHANES were included in this cross-sectional investigation. The average response rate of the entire study was 63.76%, with relatively few missing and dropout populations. We excluded the following groups: (1) under the age of eighteen; (2) no TyG index or correlation with obesity indices; (3) no confounders or duplicate data. Finally, we also excluded subjects without data on covariates. The final population included in this study was 4,813. Figure 1 displays the screening process of participants. This study was conducted strictly in accordance with the Declaration of Helsinki.
Definitions of TyG, TyG‑WC, TyG‑WHtR, and TyG-BMI
When the participants provided a blood sample, the team would be in the initial stage of measuring their fasting plasma glucose (FSG) and triglyceride levels. Participants should wear standard examination, including a one-time shirt, pants, and slippers, to use electronic scale unit weight in kilograms. Stand height was to use a rangefinder measurement. Waist circumference was measured by palpation of the hip region to find the right iliac crest of the pelvis. Use cosmetic brush in the right iliac crest above the upper margin draw a horizontal line. In axillary mid-line through the marker, the line extend from the armpit to the side of the torso. The tape measure was placed around the waist and measured on the horizontal plane of the measurement mark. Prior to analysis, we performed quality checks to identify and exclude any outlier values or cases of missing data. This step is crucial to maintain the integrity of our calculations. Each participant’s TyG index was computed by applying the logarithmic transformation to the product of their fasting triglyceride and glucose levels, as described in the formula. The use of the natural logarithm helps normalize the distribution of the TyG index, which is important for subsequent statistical analyses. Participants were categorized into four groups (Q1, Q2, Q3, and Q4) according to the quartiles of the TyG index, TyG-WC, TyG-WHtR and TyG-BMI, with the Q1 group serving as the control group. The calculation formulas for these indices are listed below:
Definition of hypertension
Hypertension was defined as self-reported hypertension, either a systolic blood pressure ≥ 140 mmHg, a diastolic blood pressure ≥ 90 mmHg, or the use of antihypertensive medication.
Covariates
To assess the effects of potential confounders, several important covariates were selected, including individual sex, age, race, education level, alcohol consumption status, smoking status, glycated hemoglobin level, total cholesterol (TC) level, high-density lipoprotein cholesterol (HDL) level, and BMI. There are also many diseases closely related to hypertension, mainly coronary heart disease, heart failure, stroke and diabetes.
Data on mortality
The clinical outcome of all-cause mortality was defined as death for any reason. The cause of cardiovascular death was determined according to the 10th version of the International Classification of Disease (ICD-10). Cardiovascular death was defined as heart disease (ICD codes I 00-I 09, I11, I13, I20-I25, and I26-I51). The mortality rate data was extracted from NHANES public related mortality documents from 2013 to 2018. The mortality data of NHANES is correlated with the death certificate data of NCHS National Death Index.
Statistical analysis
The participants were split into two groups according to whether they had hypertension. Differences in baseline variables were analyzed by t-tests and chi-square tests. Multiple logistic regression was used to explore the relationship between the TyG index and its combination with obesity indices and hypertension. The covariates included in this study were closely related to TyG, obesity, and hypertension, which were partially included in previous a NHANES study22. Model 1 was adjusted for age and sex. Model 2 included race, sex, smoking status, heart failure status, stroke status, coronary heart disease status, diabetes status, alcohol consumption status, TC level, HDL cholesterol, and BMI. To assess the robustness of the association, we further analyzed the TyG index and its combination with obesity indices after dividing them into quartiles. These variables were also included in Cox regression analysis to explore the relationship between tyg and its obesity related index with the prognosis of hypertensive patients. We then performed subgroup analyses of the associations between the TyG index and obesity-related indices and hypertension to assess the stability of the associations. Smoothed curve fitting was used to examine the effect of TyG and its obesity-related index to determine whether there was any nonlinear relationship or threshold effect. This study also utilized a Generalized Additive Model (GAM) to examine the nonlinear relationships. The analysis employed the Smooth Curve Fitting (SCF) method to illustrate how TyG and its obesity-related index affects hypertension. If the resulting effect graph revealed a nonlinear trend, such as curvature or fluctuations, it would support the hypothesis of a nonlinear relationship. By detecting this nonlinearity, a recursive algorithm was used to identify significant inflection points between hypertension TyG and its obesity-related index, facilitating threshold analysis. The statistical packages R (The R Foundation; http://www.r-project.org; Version 4.1.3) and EmPowerStats (www.emPowerstats.com; X&Y Solutions Inc.) were used. The statistical significance was set to α = 0.05.
Results
Baseline characteristics
This study included 4,813 participants, consisting of 2,363 men and 2,450 women. Of these, 1,971 participants (40.95%) were diagnosed with hypertension. Compared to the non-hypertensive population, hypertensive individuals were older, had higher education and income levels, higher glycated hemoglobin, and higher BMI. Additionally, they exhibited higher levels of TyG, TyG-BMI, TyG-WHtR, and TyG-WC, lower HDL, and had a higher prevalence of coronary heart disease, heart failure, stroke, diabetes, smoking, and alcohol consumption. For detailed information, please refer to Table 1.

Flow chart for screening participants included in this study.
To explore the connection between the TyG index and hypertension in more detail, we grouped participants based on the quartiles of the TyG index. The TyG index was divided into four intervals based on quartiles: Q1 ≤ 8.31, Q2 = 8.32–8.88, Q3 = 8.89–9.19, and Q4 ≥ 9.20. Participants in the fourth quartile were proned to be senior, had higher levels of education and household income, higher levels of glycated hemoglobin, have higher TC, have a higher BMI, have lower HDL, have a higher BMI, have a greater tendency to smoke, and have a greater risk of coronary heart disease and hypertension. In each of the four subdistricts, participants in the second quarter were more likely to have a stroke, and participants in the third quarter were more likely to have heart failure, diabetes, or alcohol consumption. For detailed information, please refer to Table 2.
Association between the TyG index and obesity indicators combined with hypertension
Multivariate logistic regression analysis revealed that the odds of hypertension increased with higher values of TyG, TyG-BMI, TyG-WHtR, and TyG-WC. The association was statistically significant in model 1 (P < 0.001). In Model 2, the OR of hypertension increased with increasing TyG-WHtR and TyG-WC indices. According to the TyG-BMI, individuals in the Q3 range had a greater risk of hypertension than did those in the Q4 range (ORQ3 = 2.64, 95% CI (2.06, 3.39) vs. ORQ4 = 2.62, 95% CI (1.82, 3.76)). Please refer to Tables 3, 4, 5 and 6 for specific details.
Stratified analysis
Stratified analyses were conducted based on gender, heart failure, coronary heart disease, stroke, diabetes, alcohol consumption, and smoking status to assess the consistency of associations between TyG and hypertension. The analysis showed that women, and individuals with heart failure, coronary heart disease, or stroke, were more likely to have hypertension. Subgroup analysis of TyG-BMI indicated that females and those with heart failure or coronary heart disease had a higher likelihood of developing hypertension. Moreover, individuals with heart failure were at increased risk in the TyG-WHtR subgroup, while females had a greater risk in the TyG-WC subgroup. Please refer to Supplementary materials Tables 1–4 for specific details.

Smooth curve fitting between the TyG and its combination with obesity indicators and hypertension incidence. The association between the TyG index (a), TyG-WC (b), TyG-WHtR (c), and TyG-BMI (d) with hypertension incidence was examined using smooth curve fitting. The results were adjusted for sex, age, race, marital status, PIR, smoking status, heart failure status, coronary heart disease status, stroke status, diabetes status, alcohol consumption status, TC, HDL, BMI and education.
Cox regression analysis
Using Cox regression analysis to evaluate the predictive value of TyG and its obesity related index for long-term prognosis of hypertension. In multivariate Cox regression analysis, TyG and its obesity related index were not associated with all-cause mortality in the included population. In terms of cardiovascular mortality, after fully adjusting for variables, TyG (HR = 1.89, 95% CI (1.03,3.51), P < 0.05) and the second quartile (HR = 4.93, 95% CI (1.29,18.80), P < 0.05) were significantly associated with cardiovascular mortality. In addition, we found correlation between TyG-BMI and increased cardiovascular mortality (HR = 1.03, 95% CI (1.00, 1.05), P < 0.05). Specific information is shown in Table 7.
Smooth curve fitting and threshold effect analysis
Smooth curve fitting revealed non-linear relationships between TyG, TyG-BMI, TyG-WHtR, TyG-WC and hypertension (Fig. 2). After adjusting for age, sex, race, marital status, PIR, smoking, heart failure, coronary heart disease, stroke, diabetes, alcohol consumption, TC, HDL, BMI, and education, threshold effect analysis identified turning points at TyG = 8.1, TyG-BMI = 247.94, TyG-WHtR = 5.32, and TyG-WC = 806.48. For instance, when TyG was less than 8.1, a positive correlation with hypertension was observed (OR = 2.9, 95% CI (1.8, 4.5), P < 0.001). However, once TyG exceeded 8.1, the correlation reversed (OR = 0.5, 95% CI (0.3, 0.8), P = 0.010). The association between TyG BMI, TyG WHtR, and TyG WC and hypertension weakens after reaching the threshold. Please refer to Table 8 for detailed information.
The results were adjusted for sex, age, race, marital status, PIR, smoking status, heart failure status, coronary heart disease status, stroke status, diabetes status, alcohol consumption status, TC, HDL, BMI and education.
Discussion
This study investigated the association of the TyG index and its combination with obesity indices with the incidence of hypertension in American adult citizens. This study aimed to discuss the blood pressure situation in adults, so the age limit was set at 18 years and above. Due to factors such as the growth and development of minors, their blood pressure is unstable and has significant differences. The covariates selected in this study were also closely related to IR and hypertension, so research results targeting the specific population of adults will be more accurate. In this study, we found strong associations between hypertension and TyG, TyG-BMI, TyG-WHtR and TyG-WC. This association remained significant after adjusting for relevant covariates. Cox regression analysis showed that TyG and TyG-BMI have certain reference value for predicting cardiovascular mortality in hypertensive patients. In addition, further analysis revealed that when the TyG index was less than 8.1, there was a positive correlation between the TyG index and hypertension, but when the TyG index was greater than 8.1, the relationship between them became inverse. TyG-BMI, TyG-WHtR and TyG-WC were positively correlated with hypertension, but this correlation weakened after a certain threshold was reached.
Our study found that TyG index may have a peak effect on the incidence rate of hypertension, and related studies have similar results. A cohort study involving 5,754 participants showed a nonlinear correlation between TyG index and all-cause mortality and cardiovascular mortality in patients with cardiac metabolic syndrome23. In addition, even in the general population, there is a non-linear correlation between TyG and all-cause mortality and cardiovascular mortality24. However, several studies indicated a linear relationship between the TyG index and the risk of developing hypertension. For instance, a meta-analysis of Chinese studies found a linear trend where each unit increase in the TyG index raised the risk of hypertension by 1.5 times25. Additional research from a large Japanese cohort supported this linear association, showing increased odds of prehypertension and hypertension with higher TyG index quartiles26. The discrepancy between the results of the above studies and ours can be mainly attributed to several aspects. Firstly, differences in sample selection play a significant role in shaping the results. The NAHENS study, for example, likely includes a more diverse and heterogeneous population, encompassing individuals of different age groups, ethnicities, and health statuses, which may result in a non-linear relationship between TyG and hypertension. Secondly, sample size and population heterogeneity can lead to varying outcomes. Larger sample sizes tend to capture a broader range of variability, thus revealing more complex relationships. Statistical methodology is another critical factor. Traditional linear regression models assume a simple linear relationship between variables, whereas non-linear models, such as Generalized Additive Models, can capture more intricate associations, which may explain the non-linear relationship observed in studies like NAHENS. Furthermore, differences in blood pressure measurement standards and classification criteria may influence the findings. For instance, some studies might rely on single blood pressure measurements, while NAHENS employs more rigorous standardized methods. Lifestyle factors (such as diet, physical activity and smoking) and potential confounders (such as diabetes and obesity) may also contribute to a non-linear relationship between TyG and hypertension, depending on the population studied. Lastly, TyG may exhibit a linear relationship within certain ranges, but beyond a specific threshold, the association could shift to a non-linear pattern. This threshold effect is more pronounced in non-linear models. In summary, the relationship between TYG and hypertension is influenced by multiple factors, including sample heterogeneity, statistical modeling choices, lifestyle factors, and genetic backgrounds, all of which collectively determine whether a linear or non-linear relationship is observed in different studies.
The TyG index is regarded as a simple proxy for IR. Several studies have shown a relationship between hypertension and IR27,28. In addition, a recent cross-sectional study showed that the TyG index was strongly associated with the development of hypertension, and a longitudinal study of Chinese population showed that the TyG index could predict the development of hypertension10. Obesity is closely related to IR, and obesity may accelerate the development process of hypertension. Therefore, derived indicators, such as the TyG-BMI, TyG-WHtR, and TyG-WC, can help us further explore the correlation between obesity-related IR indicators and hypertension. A cross-sectional study of 15,464 participants with normal blood glucose showed that for every 10-unit increase in TyG-BMI (continuous variable), the incidence of hypertension increased by 31%. Moreover, this association remained stable across subgroup analyses20. These results align with our present study’s findings. In addition, a study showed that TyG-WHtR and TyG-WC also had high accuracy in diagnosing hypertension29. Therefore, the use of the TyG index and obesity-related indicators to explore the incidence and trend of hypertension has certain clinical significance.
Our study showed that TyG, TyG-WC, TyG-WHtR, and TyG-BMI were less strongly associated with hypertension in men than in women. This finding is in accord with current reports of sex differences in the incidence of hypertension. According to a previous study, women with diabetes and impaired glucose tolerance were more likely to suffer hypertension related to the same glucose metabolism issue than males. This suggested that in the case of other basic conditions, women may were more likely than men to suffer from hypertension30. In addition, regarding the associations between IR and obesity-related indicators and the incidence of hypertension, we found that people with coronary heart disease, heart failure and stroke were more likely to have hypertension. Research conducted in primary care settings has revealed that between 60% and 76% of patients who are overweight or obese also have hypertension, indicating a strong correlation between the two variables31. There is considerable evidence that overweight, obesity and IR increase cardiovascular disease and overall morbidity and mortality32,33. In this regard, an analysis from the Framingham Heart Study showed a positive association between excess weight and the relative risk of hypertension and CVD. People who suffered from stroke and heart failure have more cardiovascular risk factors, which can promote systemic and vascular inflammation and IR, leading to vascular stiffness and ultimately hypertension34,35.
Advantages and limitations
This study examined the correlation between TyG and obesity-related indicators and the incidence of hypertension. First, the strength of this study is that it was adjusted for covariates, including glycated hemoglobin, total cholesterol, and high-density lipoprotein (HDL), which would allow the results to be scientific and objective. Second, our study’s large sample size allowed us to perform group analyses. Additionally, to eliminate bias caused by oversampling and produce precise statistical validity, we employed weighted estimates and corrected for confounding variables. Finally, we explored the nonlinear relationship between IR and obesity-related indicators and hypertension and the potential tipping point of this relationship. The curve fitting results were consistent with the threshold, which showed that the results were stable and reliable. However, this study has certain limitations. This study utilized a cross-sectional design, which inherently limited our ability to infer causality in the observed association between the TyG index and hypertension. While this design enabled the examination of relationships at a single time point, it did not allow for determination of whether an elevated TyG index increases the risk of hypertension or whether pre-existing hypertension may influence metabolic parameters. Furthermore, despite NHANES data being nationally representative, potential biases should be considered. First, resource and sampling constraints may result in underrepresentation of specific subpopulations—such as ethnic minorities and low-income groups—potentially impacting the generalizability of the findings. Second, NHANES data incorporate both self-reported and objective measures; self-reported data may be subject to recall and social desirability biases, while objective measures, although more reliable, are still vulnerable to measurement error and protocol variability. Finally, despite adjusting for multiple confounders, residual confounding from unmeasured factors, such as genetic predispositions and environmental influences, may still affect the observed association between the TyG index and hypertension. These limitations highlight the need for cautious interpretation of the results. Future longitudinal studies or those incorporating alternative measures and sampling methods are warranted to validate these findings and provide a more comprehensive understanding of the role of the TyG index in hypertension and metabolic health.
Extended implications for comorbid psoriasis and cardiovascular risk
This study highlightd the association of the TyG index and its derived indicators (TyG-BMI, TyG-WC and TyG-WHtR) with hypertension risk. These indicators are particularly relevant for patients with high metabolic risk, such as those with psoriasis—a chronic inflammatory disease that is strongly associated with increased risks of metabolic syndrome and cardiovascular disease. The systemic inflammation characteristic of psoriasis, driven in part by the IL-23/IL-17 axis, may exacerbate insulin resistance and metabolic dysfunction, thereby compounding cardiovascular risks36. In this context, metabolic markers such as TyG-BMI may serve as valuable tools for identifying heightened metabolic and cardiovascular risks in psoriasis patients37. This combined assessment could enable clinicians to implement individualized interventions aimed at both inflammation and metabolic health, thereby potentially reducing the burden of comorbid hypertension in this high-risk group. Given the unique metabolic and cardiovascular risks in psoriasis patients, further longitudinal research is warranted to explore the impact of biologic therapies on the relationship between the TyG index and cardiovascular health. This approach would help elucidate the potential long-term metabolic benefits of biologics in psoriasis management and further clarify the role of the TyG index as a marker for cardiovascular risk in patients with chronic inflammatory diseases.
Practical implications for healthcare providers
The findings of this study suggest that the TyG index, as a readily accessible metabolic indicator, may could serve as an adjunct tool for healthcare providers in identifying individuals at higher risk of hypertension, especially in the early stages before significant pathophysiological changes occur. Given the strong association between obesity indicators and hypertension risk, combining TyG with obesity metrics may allow for a more comprehensive risk assessment. This combined assessment could inform individualized intervention strategies, including lifestyle modifications and metabolic health management, aimed at preventing or delaying the onset of hypertension. This approach may be particularly beneficial in primary care settings, where early identification and targeted management of at-risk patients could significantly impact public health outcomes.
Conclusion
These findings indicate that the TyG index and its related indicators are significantly associated with the presence of hypertension. This relationship provides valuable insights into the potential role of these markers in the early identification and stratification of individuals at risk for developing hypertension.Future research should focus on longitudinal studies to confirm the causal relationship between the TyG index, obesity indicators, and hypertension development. Such studies could provide more definitive evidence on whether the TyG index and obesity markers directly contribute to hypertension risk. Additionally, intervention studies assessing how lifestyle or pharmacological changes in the TyG index impact hypertension risk over time would be valuable. These approaches could further validate the TyG index as a predictive tool for hypertension and support its use in clinical risk stratification.
Data availability
The dataset used in this study can be found in online repositories. The database website are as follows: https://www.cdc.gov/nches/nhanes and https://www.cdc.gov/nchs/data-linkage/mortality.htm.
References
Burnier, M. & Damianaki, A. Hypertension as cardiovascular risk factor in chronic kidney disease. Circ. Res. 132, 1050–1063 (2023).
Feigin, V. L. & Owolabi, M. O. Pragmatic solutions to reduce the global burden of stroke: A World Stroke Organization-Lancet Neurology Commission. Lancet Neurol. 22, 1160–1206 (2023).
McEvoy, J. W. et al. 2024 ESC guidelines for the management of elevated blood pressure and hypertension. Eur. Heart J. 45, 3912–4018 (2024).
Kario, K., Okura, A., Hoshide, S. & Mogi, M. The WHO Global report 2023 on hypertension warning the emerging hypertension burden in globe and its treatment strategy. Hypertens. Res. 47, 1099–1102 (2024).
Muntner, P. et al. Potential US Population Impact of the 2017 ACC/AHA high blood pressure Guideline. Circulation 137, 109–118 (2018).
Hong, S., Han, K. & Park, C. Y. The triglyceride glucose index is a simple and low-cost marker associated with atherosclerotic cardiovascular disease: A population-based study. BMC Med. 18, 361 (2020).
Gu, S., Wang, A., Ning, G., Zhang, L. & Mu, Y. Insulin resistance is associated with urinary albumin-creatinine ratio in normal weight individuals with hypertension and diabetes: The REACTION study. J. Diabetes. 12, 406–416 (2020).
Yan, Y. et al. Triglyceride-glucose index trajectory and arterial stiffness: Results from Hanzhong adolescent hypertension cohort study. Cardiovasc. Diabetol. 21, 33 (2022).
Wu, Z. et al. Association of TyG index and TG/HDL-C ratio with arterial stiffness progression in a non-normotensive population. Cardiovasc. Diabetol. 20, 134 (2021).
Zheng, R. & Mao, Y. Triglyceride and glucose (TyG) index as a predictor of incident hypertension: A 9-year longitudinal population-based study. Lipids Health Dis. 16, 175 (2017).
Gao, Q. et al. Positive association of triglyceride-glucose index with new-onset hypertension among adults: A national cohort study in China. Cardiovasc. Diabetol. 22, 58 (2023).
Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 390, 2627–2642 (2017).
Movahed, M. R., Motieian, M. & Bates, S. Overweight (BMI of 25–30) is independently Associated with significantly higher prevalence of systolic and diastolic hypertension in adults. Crit. Pathw. Cardiol. 22, 146–148 (2023).
Yatsuya, H. Increasing role of Overweight/Obesity as the determinant of hypertension and the Consequent Cardiovascular diseases in Japan. J. Atheroscler Thromb. 30, 323–325 (2023).
Elagizi, A. et al. An overview and update on obesity and the obesity Paradox in Cardiovascular diseases. Prog Cardiovasc. Dis. 61, 142–150 (2018).
Chen, L. et al. High triglyceride glucose-body mass index correlates with prehypertension and hypertension in east Asian populations: A population-based retrospective study. Front. Cardiovasc. Med. 10, 1139842 (2023).
Li, Y. et al. Predicting hypertension by obesity- and lipid-related indices in mid-aged and elderly Chinese: A nationwide cohort study from the China Health and Retirement Longitudinal Study. BMC Cardiovasc. Disord. 23, 201 (2023).
Yuan, Y., Sun, W. & Kong, X. Comparison between distinct insulin resistance indices in measuring the development of hypertension: The China Health and Nutrition Survey. Front. Cardiovasc. Med. 9, 912197 (2022).
Gui, J. et al. Obesity-and lipid-related indices as a predictor of hypertension in Mid-aged and Elderly Chinese: A cross-sectional study. Res. Sq. 23, 201 (2023).
Huang, X. et al. TyG-BMI and hypertension in Normoglycemia subjects in Japan: A cross-sectional study. Diab Vasc. Dis. Res. 20, 14791641231173617 (2023).
Nikbakht, H. R. et al. Triglyceride glucose-body mass index and hypertension risk in Iranian adults: A population-based study. BMC Endocr. Disord.. 23, 156 (2023).
Zhang, F. & Hou, X. Association between the triglyceride glucose index and heart failure: NHANES 2007–2018. Front. Endocrinol. (Lausanne). 14, 1322445 (2023).
Liu, Q. et al. Association of the triglyceride-glucose index with all-cause and cardiovascular mortality in patients with cardiometabolic syndrome: A national cohort study. Cardiovasc. Diabetol. 23, 80 (2024).
Yu, Y. et al. Sex differences in the nonlinear association of triglyceride glucose index with all-cause and cardiovascular mortality in the general population. Diabetol. Metab. Syndr. 15, 136 (2023).
Xu, A. R., Jin, Q., Shen, Z., Zhang, J. & Fu, Q. Association between the risk of hypertension and triglyceride glucose index in Chinese regions: A systematic review and dose-response meta-analysis of a regional update. Front. Cardiovasc. Med. 10, 1242035 (2023).
Xu, J., Xu, W., Chen, G., Hu, Q. & Jiang, J. Association of TyG index with prehypertension or hypertension: A retrospective study in Japanese normoglycemia subjects. Front. Endocrinol. (Lausanne). 14, 1288693 (2023).
Jian, S., Su-Mei, N., Xue, C., Jie, Z. & Xue-Sen, W. Association and interaction between triglyceride-glucose index and obesity on risk of hypertension in middle-aged and elderly adults. Clin. Exp. Hypertens. 39, 732–739 (2017).
Akande, T. O., Adeleye, J. O. & Kadiri, S. Insulin resistance in nigerians with essential hypertension. Afr. Health Sci. 13, 655–660 (2013).
Miao, H., Zhou, Z., Yang, S. & Zhang, Y. The association of triglyceride-glucose index and related parameters with hypertension and cardiovascular risk: A cross-sectional study. Hypertens. Res. 47, 877–886 (2024).
Connelly, P. J., Currie, G. & Delles, C. Sex differences in the prevalence, outcomes and Management of Hypertension. Curr. Hypertens. Rep. 24, 185–192 (2022).
Hall, J. E., do Carmo, J. M., da Silva, A. A., Wang, Z. & Hall, M. E. Obesity, kidney dysfunction and hypertension: Mechanistic links. Nat. Rev. Nephrol. 15, 367–385 (2019).
Koenen, M., Hill, M. A., Cohen, P. & Sowers, J. R. Obesity adipose tissue and vascular dysfunction. Circ. Res. 128, 951–968 (2021).
Louie, J. Z., Shiffman, D., McPhaul, M. J. & Melander, O. Insulin resistance probability score and incident cardiovascular disease. J. Intern. Med. 294, 531–535 (2023).
Chen, L. et al. Regulation of glucose and lipid metabolism in health and disease. Sci. China Life Sci. 62, 1420–1458 (2019).
Zhang, Z., Zhao, L., Zhou, X., Meng, X. & Zhou, X. Role of inflammation, immunity, and oxidative stress in hypertension: New insights and potential therapeutic targets. Front. Immunol. 13, 1098725 (2022).
Ten Bergen, L. L., Petrovic, A., Krogh Aarebrot, A. & Appel, S. The TNF/IL-23/IL-17 axis-head-to-head trials comparing different biologics in psoriasis treatment. Scand. J. Immunol. 92, e12946 (2020).
Huang, D. et al. Positive association between different triglyceride glucose index-related indicators and psoriasis: Evidence from NHANES. Front. Immunol. 14, 1325557 (2023).
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by the National Natural Science Foundation of China (82374280).
Author information
Authors and Affiliations
Contributions
P.H.,H.Z.,G.R.,Y.W., S.F.,Y.L. and Z.Z. wrote the main manuscript text, P.H. prepared figures and tables. L.G. and X.M. Supervised the manuscript. All authors reviewed the manuscript. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics statement
The NHANES study was approved by the Institutional Review Board (IRB) of the National Center for Health Statistics (NCHS) at the Centers for Disease Control and Prevention (CDC). The study has obtained informed consent from all participants and/or their legal guardians.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Huang, P., Zhang, H., Ren, G. et al. Association of the triglyceride glucose index with obesity indicators and hypertension in American adults based on NHANES 2013 to 2018. Sci Rep 15, 2443 (2025). https://doi.org/10.1038/s41598-025-86430-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-86430-z
