
Abstract
Nephrotic syndrome, the most common glomerular disease in pediatric population, is classified into two groups of steroid sensitive (SSNS) and resistant (SSRS). There is growing evidence on the role of T cells cytokines, including interleukin-13, in pathophysiology of nephrotic syndrome and steroid response. This study was a cross-sectional study conducted at Children’s Medical Center Hospital in order to explore the relationship between urinary IL-13 levels and responsiveness to corticosteroid treatment. All children (1 to 15 years) referred from January 2021 to January 2022 diagnosed with nephrotic syndrome were included. Urine samples were collected during the initial phase or relapse of nephrotic syndrome, before the initiation of steroid or alternative treatments. Interleukin-13 levels in the urine were measured using the ELISA method. In this study, 83 cases of nephrotic syndrome were enrolled, of whom 30 (36.1%) were girls and 53 (63.9%) were boys. Out of the 83 cases, 63 (75.9%) were identified as SSNS and 20 (24.1%) as SRNS. There was no significant difference between the urinary interleukin-13 levels between SSNS and SRNS groups (P-value: 0.84). Sex (P-value: 0.598) and age (P-value: 0.704) also had no association with interleukin-13 levels. Further studies in larger population are recommended to better assess the potential of this biomarker to predict response to treatment. .
Similar content being viewed by others

Introduction
Nephrotic syndrome, a chronic kidney disease and the most common glomerular disease in pediatric population, is characterized by edema, proteinuria and hypoalbuminaemia. In children under the age of 16, the incidence is 2 to 7 per 100,0001. The most common childhood type is idiopathic type, for treatment of which corticosteroids play a pivotal role. Based on the response to corticosteroid therapy resulting in remission of proteinuria, cases are divided into two groups of steroid-sensitive (SSNS) or resistant (SRSN) nephrotic syndrome. Therefore, the response to corticosteroids could be regarded as a prognostic factor. In SRNS, corticosteroids are insufficient, necessitating further immunosuppressive agents such as calcineurin inhibitors or cyclophosphamide to achieve disease control2,3.
There are no definite laboratory markers to differentiate these two types, and the classification is based on the steroid response. Biopsy is a method for distinguishing between these two clinical forms of the disease, which is an invasive method. However, children with nephrotic syndrome usually do not undergo biopsies unless they exhibit unusual features or are resistant to steroids. Recent research has focused on developing biomarkers for early diagnosis and differentiation of these types, and also prediction of prognosis and long-term outcomes4,5.
Interleukin-13 (IL-13) is a cytokine that has been implicated in various immune responses and has recently gained attention for its potential role in nephrotic syndrome pathogenesis. It has been shown that in those patients who respond well to steroids, the immune system switches to Th2 response, with IL-13 overexpression and production6,7,8. Elevated levels of IL-13 have also been associated with raised permeability of the glomerular filtration barrier, suggesting a possible link to proteinuria in nephrotic syndrome9.
However, the relationship between urinary IL-13 levels and responsiveness to corticosteroid treatment in children with nephrotic syndrome remains unclear. Given the potential of IL-13 as a non-invasive diagnostic approach, this study aims to evaluate the potential capability of urinary IL-13 in distinguishing between steroid-sensitive and steroid-resistant nephrotic syndrome in patients referring the Children’s Medical Center.
Method
This study was a cross-sectional study conducted from January 2021 to January 2022 at Children’s Medical Center Hospitals. Children aged 1 to 15 years diagnosed with nephrotic syndrome and referred to the nephrology department or clinic were included.
Participants grouping
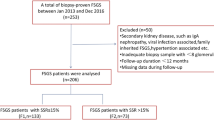
All cases referred in the defined duration of study were enrolled (census). The inclusion criteria were a confirmed diagnosis of nephrotic syndrome, without any evidence of inflammatory conditions or infections. Exclusion criteria included chronic diseases like cancer, interstitial tubular nephritis evident in initial biopsy, secondary nephrotic syndrome due to infection or drugs, and systemic vascular or metabolic disorders. Patients who were under any immunosuppressive therapy at the time of urine sample collection, such as steroids were also excluded, and those who were in the active phase of nephrotic syndrome. As urine IL13 level is impressed by the acute phase of any infectious or inflammatory disorder, these cases were also excluded.
The diagnosis of nephrotic syndrome and steroid resistance or sensitivity was confirmed based on clinical information, response to therapy, and biopsy results from the patients’ records.
Sample collection
Urine samples were collected during the initial phase or relapse of nephrotic syndrome, before the initiation of steroid or alternative treatments. These samples were stored at -80 °C in the laboratory of the Children’s Medical Center.
Interleukin-13 measurement
Interleukin-13 levels in the urine were measured using the ELISA method according to the manufacturer’s instructions. Interleukin-13 levels were measured using the Karmania Pars Gene kit, which has a sensitivity of 5 picograms per milliliter and an accuracy of Inter-assay < 9% and Intra-assay < 3%. The standard value for the kit is available in Table 1.
Interleukin-13 levels will be reported in 10 ranges, each with a size of 0.01 g, and categorized into 10 groups as presented in Table 2.
Data collection and analysis
Data collection was done using a checklist that included laboratory results and basic demographic information such as age and gender. The age of disease onset was also recorded. Quantitative levels of Interleukin-13 in urine samples were measured and recorded in both groups (SSNS and SRNS).
The data were then entered into statistical software for analysis. The collected data were analyzed using SPSS Statistics version 27. Cross-tabulation and Fisher’s Exact Test were used to examine the relationship between qualitative variables, including gender and age and steroid response groups, to determine the P-value. McNemar’s test was used to evaluate the differences in IL-13 levels between SSNS and SRNS groups. A P-value of 0.05 was considered statistically significant.
Ethical consideration
Informed consent
was obtained from all participants. Ethical approval for this study was obtained from the Ethics Committee of Tehran University of Medical Sciences, allowing access to and extraction of patient data from hospital files and records (Batch Number: IR.TUMS.CHMC.REC.1401.188). All methods were carried out in accordance with relevant guidelines and regulations. All methods of project were carried out in accordance with and the manuscript has been written aligned with STROBE checklist for observational studies.
Result
In total, 83 cases of nephrotic syndrome met the inclusion criteria and were enrolled. The number of girls and boys was 30 (36.1%) and 53 (63.9%), respectively. The age of the patients ranged from 3 to 8 years, with a mean age of 4.46 years (SD = 1.307). Out of the 83 cases, 63 (75.9%) were classified as SSNS and 20 (24.1%) as SRNS.
The frequency of cases in 10 group classification of IL-13 is available in Table 3. There was no significant difference between the urinary Interleukin-13 levels between SSNS and SRNS groups (P-value: 0.84).
Similarly, no significant difference in urinary Interleukin-13 levels was found in male and female (P-value: 0.598). This lack of significant difference was also observed in comparison of the levels in age > 5 and ≤ 5 years (P-value: 0.704).
Discussion
This cross-sectional study was conducted at a children’s medical center to assess urine IL-13 level in nephrotic patients and evaluate its association with steroid response. We found that IL-13 levels were not associated with steroid response. Moreover, there was no significant difference in the levels of this cytokine between different sexes and age groups. The measurements were taken while ensuring that patients were not under any immunosuppressive therapy, such as steroids, and were not in the active phase of nephrotic syndrome, as these treatments inhibit cytokine production. As urine IL-13 level is impressed by the acute phase of any infectious or inflammatory disorder, these cases were also excluded.
It has been argued that in nephrotic patients, an imbalance in Th1, Th2, and Treg cells leads to steroid resistance. IL-13 is a Th2 cytokine, and its levels are notably elevated in SSNS patients who respond well to glucocorticoid therapy. Th1-dominant cytokine profiles are often associated with glucocorticoid resistance, and even in relapse, higher levels of Th-1 cytokines have been reported in SSNS patients. So based on literature, a Th2-dominant profile, characterized by higher IL-13 levels, tends to predict a better therapeutic outcome that our study could not confirm through urine measurements10,11.
T cells, via the production of cytokines, lead to increased glomerular permeability. However, the exact mechanisms by which this phenomenon is occurred is poorly understood. One such hypothesized theory is by cytokines release like IL-13. Minimal change disease, the most common type of nephrotic syndrome, is widely known as being sensitive and rapidly responsive to steroid therapy. A study conducted by Zeybek et al. on six patients with minimal change disease found that urine IL-13 levels in active phase of disease was significantly higher than in remission stage12. Lai and colleagues’ study further supported the link between IL-13 and minimal change disease, demonstrating that IL-13 transgenic mice showed significant albuminuria, hypoalbuminemia, and hypercholesterolemia compared to control mice13. A study by Mishra et al. investigated 40 idiopathic nephrotic syndrome cases and 16 controls. They observed that serum IL-13 levels were significantly higher in the case group compared to the controls, suggesting a potential role of IL-13 in the disease pathogenesis6.
This result suggests that while elevated IL-13 levels have been associated with a Th2 response in other studies on SSNS patients, urinary IL-13 may not reflect the underlying immune mechanisms linked to steroid response, or that other factors may play a more critical role. Also, we can argue that the cytokine dynamics in urine might differ from serum. Other biomarkers, or a panel of biomarkers, might provide more accuracy in predicting steroid response.
The main limitation of this study was the retrospective collection of nephrotic syndrome diagnostic information from patient records, which resulted in some incomplete data and the exclusion of certain patients. Another limitation was the lack of precise information on the definitive diagnosis of all cases, both sensitive and resistant, which would allow for better understanding and comparison of individual diagnoses using this test. SRNS has more diverse and complex pathogenic mechanisms, often involving genetic mutations in podocyte-related genes, independent of immune system dysregulation. In such cases, IL-13 may not play a significant role and this could have impacted the results of this study. Future studies, with genetic assessment confirmation, are recommended in larger populations considering the mentioned limitations. Moreover, distinguishing nephrotic syndrome types based on biopsy samples could offer a more detailed analysis and better diagnostic differentiation.
Conclusion
In our study, urinary IL-13 was chosen as a diagnostic marker to distinguish steroid-sensitive from steroid-resistant nephrotic syndrome. However, we found no significant difference in IL-13 levels between the two groups. Therefore, IL-13 measurement alone might not differentiate between steroid-sensitive and steroid-resistant nephrotic syndrome. Future research should consider combining IL-13 measurements with other biomarkers or investigating IL-13 levels in different biological samples, such as serum, to improve the accuracy of predicting steroid responsiveness in nephrotic syndrome.
Data availability
Data could be available from the corresponding author upon reasonable request.
References
Rodriguez-Ballestas, E. & Reid-Adam, J. Nephrotic syndrome. Pediatr. Rev. 43(2), 87–99 (2022).
Vivarelli, M., Gibson, K., Sinha, A. & Boyer, O. Childhood nephrotic syndrome. Lancet 402(10404), 809–824 (2023).
Zotta, F., Vivarelli, M. & Emma, F. Update on the treatment of steroid-sensitive nephrotic syndrome. Pediatr. Nephrol. 37(2), 303–314 (2022).
Hodson, E. M., Hahn, D., Alexander, S. I., Graf, N. & McCarthy, H. Steroid Sensitive Nephrotic Syndrome, 405–442 (Springer, 2023).
Cara-Fuentes, G. & Smoyer, W. E. Biomarkers in pediatric glomerulonephritis and nephrotic syndrome. Pediatr. Nephrol. 36(9), 2659–2673 (2021).
Mishra, O. P., Teli, A. S., Singh, U., Abhinay, A. & Prasad, R. Serum immunoglobulin E and interleukin-13 levels in children with idiopathic nephrotic syndrome. J. Trop. Pediatr. 60(6), 467–471 (2014).
Al Rushood, M., Al-Eisa, A. A. & Haider, M. Z. Interleukin-4 and interleukin-13 gene polymorphisms in children with idiopathic nephrotic syndrome. Front. Pead. 8, 591349 (2020).
Nickavar, A., Valavi, E., Safaeian, B., Amoori, P. & Moosavian, M. Predictive value of serum interleukins in children with idiopathic nephrotic syndrome. Iran. J. Allergy Asthma Immunol. 19(6), 632–639 (2020).
Mamizadeh, N., Otukesh, H., Hoseini, R. & Moshfegh, F. Serum interleukin 13 level in steroid sensitive nephrotic syndrome. J. Compr. Pediatr., 8(3). (2017).
Ahmadian, E. et al. The role of cytokines in nephrotic syndrome. Mediat. Inflamm. 2022(1), 6499668 (2022).
Hackl, A. et al. The role of the immune system in idiopathic nephrotic syndrome. Mol. Cell. Pediatr. 8, 1–11 (2021).
Zeybek, C. H. D. et al. The roles of urine interleukin-13, CD80, CD28, matrix metalloproteinase-2 and granzyme B in the pathogenesis of childhood minimal change nephrotic syndrome. J. Clin. Exp. Invest. 5(3), 354–361 (2014).
Lai, K. W. et al. Overexpression of interleukin-13 induces minimal-change-like nephropathy in rats. J. Am. Soc. Nephrol. 18(5), 1476–1485 (2007).
Acknowledgements
We would like to thank the personnel of Children’s Medical Center for their invaluable support and assistance.
Funding
None.
Author information
Authors and Affiliations
Contributions
BE, DF and MM conceptualized the study. AV, NP, and MHA did the ELISA test. NS drafted the manuscript. MM, DF, BB, and AA supervised the study. All have critically revised the manuscript. All authors have read and approved the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
Informed consent was obtained from all participants. Ethical approval for this study was obtained from the Ethics Committee of Tehran University of Medical Sciences, allowing access to and extraction of patient data from hospital files and records (Batch Number: IR.TUMS.CHMC.REC.1401.188). All methods of project were carried out in accordance with and the manuscript has been written aligned with STROBE checklist for observational studies.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ermian, B., Samieefar, N., Vahidi, A. et al. Urinary interleukin 13 level in steroid sensitive and resistant nephrotic syndrome: a cross-sectional single center study. Sci Rep 15, 4323 (2025). https://doi.org/10.1038/s41598-025-86488-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-86488-9
Keywords
This article is cited by
-
Immune dysregulation in pediatric cancer–associated nephrotic syndrome: current insights
Pediatric Nephrology (2025)
