
Abstract
A study in the Enshi Region between Sept-Nov 2023 assessed medical staff’s knowledge, attitude, and practice regarding multiple myeloma. The disease significantly impacts physical health, quality of life, and mental well-being. Medical professionals play crucial roles in its prevention and treatment. Analysis used Pearson’s correlation, logistic regression, and structural equation model (SEM). A total of 229 valid questionnaires were collected, with 68.6% of female participants, and 42.4% aged 31–40 years. The knowledge, attitude, and practice scores were 36.27 ± 4.97 (range: 25–53), 42.40 ± 5.78 (range: 30–56), and 29.71 ± 6.41 (range: 7–35), respectively. Pearson’s correlation analysis revealed significantly positive correlation between knowledge and attitude. Moreover, in both univariate and multivariate analysis, knowledge showed positive association with attitude. Several demographic factors independently associated with KAP scores were identified, including education level, age, occupation type, and frequency of academic conferences or medical education activities per year. SEM further indicated direct association between attitude and practice (β = 0.320, 95%CI: 0.189–0.452, P < 0.001). In the Enshi Region, medical staff displayed moderate knowledge, neutral attitudes, and proactive practices towards multiple myeloma. Moreover, significant positive association was found between knowledge and attitude. These discoveries provided valuable perspectives to the development of healthcare interventions and educational initiatives for improving medical staff’s knowledge, attitudes, and practices.
Similar content being viewed by others

Introduction
Multiple myeloma refers to the neoplastic proliferation of monoclonal plasma cells in the bone marrow, featured by excessive production and destructive growth of abnormal cells1. This disease has considerable health impacts on individuals, manifesting as compromised immune function, bone lesions, anemia, and impaired renal function2,3. Reportedly, its global incidence reached an increment of 126% between 1990 and 2016, with age-standardized rate of 1.78% in 20204,5. Elevated incidence and mortality were observed in developed countries, especially in Australia, New Zealand and norther America4. In China, the estimated age-standardized incidence and mortality rates reached 0.93 and 0.67 per 100,000 in 2019, respectively6. Given the escalating prevalence and healthcare burden associated with multiple myeloma, there is a pressing need for effective prevention and treatment strategies to address this public health challenge.
The impacts of multiple myeloma on patients extend beyond physical health to life quality and mental well-being. To be specific, multiple myeloma often causes pain, fatigue, and impaired physical function, which significantly reduce patients’ overall quality of life7. Moreover, dealing with chronic and potentially life-threatening illness can lead to mental health challenges8. Therefore, early diagnosis, timely intervention, and comprehensive management are crucial to improving the prognosis and enhancing the well-being of multiple myeloma patients. Medical staff, as frontline healthcare providers, play a critical role in preventing, treating, and managing multiple myeloma. By offering accurate information, timely interventions, and personalized care, medical staff can empower patients to make informed decisions and actively participate in their treatment. Additionally, medical staff’s mental support and empathy can significantly impact patients’ mental health, fostering positive outlook and effective coping mechanisms.
The knowledge, attitude, and practice (KAP) framework provides a comprehensive approach for examining medical staff’s understanding, attitudes, and behaviors concerning multiple myeloma. By assessing their knowledge, attitudes towards prevention and treatment, and actual implementation of recommended practices, this framework yields valuable insights that can guide targeted interventions and educational initiatives, and ultimately promote the overall well-being of patients. For example, in a mixed methods study conducted in European countries, 34% of hematologists and 69% of nurses had suboptimal knowledge regarding the mechanisms of action of new agents for multiple myeloma9. In addition, a study from Australia indicated that hematologists recognized the importance of physical activity for multiple myeloma, but lack confidence in recommending specific exercises and determining the appropriateness for managing specific disease complications10. Despite the potential clinical benefits from KAP studies, no research was available to explore the KAP scores among medical staff in China, which hampered the long-term development of multiple myeloma management in healthcare units.
Based on a cross-sectional study in Enshi Region, we aimed to investigate the KAP of medical staff regarding multiple myeloma and the influential factors of KAP. The findings of this study could identify areas for improvement and guide the development of targeted interventions to enhance the role of medical staff in the prevention and treatment of multiple myeloma.
Methods
Study design and participants
This cross-sectional study recruited medical staff at hospitals in Enshi Region between Sept 2023 and Nov 2023. Ethical approval was obtained from The Committee on Biomedical Research Ethics of the Central Hospital of Enshi Tujia and Miao Autonomous Prefecture, and informed consent was obtained from participants.
Inclusion criteria encompassed medical staff employed in medical, nursing, and medical technology professions at hospitals in Enshi Region. Exclusion criteria were as follows: (1) questionnaires with response times below 114 s (with a minimum of 2 s for single-choice questions and 3 s for multiple-choice questions) or exceeding 1800 s; (2) incomplete responses; (3) and participants who were unable to provide informed consent.
Sample size determination
The sample size was determined based on the total population of healthcare professionals in the Enshi region engaged in disciplines directly or indirectly related to multiple myeloma. This region comprises eight counties and cities with 19 hospitals classified as secondary level or higher, including two tertiary hospitals and one private hospital. The number of hematology specialists is fewer than 100. However, when accounting for professionals in nephrology, orthopedics, traumatology, and other related fields, the estimated population of medical staff involved in myeloma-related care is approximately 300.
Questionnaire and quality control
The questionnaire employed in this study was developed following relevant literature4,11,12 and The guidelines for the diagnosis and management of multiple myeloma in China (2022 revision)13. Refinements were made based on feedback from 3 senior hematologists. A pilot study involving 50 participants was conducted, and the Cronbach’s α coefficient of 0.757 demonstrated acceptable internal consistency14. The Kaiser-Meyer-Olkin (KMO) measure was 0.828, indicating strong validity for factor analysis.
The final Chinese version of the questionnaire consisted of four dimensions: demographic characteristics, knowledge, attitude, and practice. The demographic dimension included 10 items, covering gender, age, marital status, education level, profession type, occupation, professional title, type of medical institution, work experience duration, and frequency of academic conferences or medical education activities per year.
The knowledge dimension comprised a total of 13 questions. It consisted of two single-choice questions (K1 and K7), each scoring 1 point for a correct answer and 0 points for an unclear or incorrect answer. Additionally, there were eleven multiple-choice questions (K2-K6, K8-K13), with a perfect score of 5 points for all correct choices, 3 points for partially correct choices, and 0 points for any incorrect choices. The total score ranged from 0 to 57. The attitude dimension consisted of 12 questions, all measured using a five-point Likert scale, ranging from strongly agree (5 points) to strongly disagree (1 point). The 12th question was an open-ended question and was not scored. The total score ranged from 11 to 55. The practice dimension included 7 questions, also measured using a five-point Likert scale, with all items having positive scores ranging from strongly agree (5 points) to strongly disagree (1 point). The total score ranged from 7 to 35.
To assess the difficulty level of questionnaire items, the degree of difficulty was calculated as the percentage of participants who answer the item correctly. The degree of difficulty index ranges from 0 to 1, where higher values indicate easier questions15. Items with a difficulty level from 0 to 0.3 are classified as difficult; those from 0.3 to 0.8 are considered desirable; and items exceeding 0.8 are classified as easy15. The indicator provides valuable insights into the appropriateness of item difficulty levels within a questionnaire.
To evaluate the levels of knowledge, attitude, and practice (KAP), cut-off values of 60% and 80% of the total score were employed16. Participants were categorized into three levels based on their scores in each KAP dimension: good knowledge, positive attitude, and proactive practice (80–100%); moderate knowledge, neutral attitude, and moderate practice (60–79%); and inadequate knowledge, negative attitude, and inappropriate practice (below 60%).
Data collection and quality control
The online questionnaire was developed using Questionnaire Star (http://www.wjx.cn), a professional online survey software platform. Participants accessed the questionnaire via WeChat by scanning a QR code. To ensure data quality, each IP address was restricted to one submission, and all items of questionnaire were mandatory. After data collection, an Excel spreadsheet was exported from the Questionnaire Star platform. The research team carefully reviewed all questionnaires for integrity, internal coherence, and reasonableness.
Statistical analyses
Data analysis was conducted using the SPSS version 26.0 (IBM, Armonk, NY, USA) and Stata version 18.0 for structural equation modeling (SEM). For the descriptive analysis of participants’ demographic information and KAP scores, continuous variables were expressed as means ± standard deviations (SDs), while categorical variables were presented as frequencies and percentages. Student’s t-test was used for comparisons of KAP scores between two groups with normally distributed data, while the Wilcoxon-Mann-Whitney test was applied for non-normally distributed data between two groups. ANOVA was employed for continuous variables involving three or more groups with normal distribution and equal variances. Kruskal-Wallis analysis was used for categorical variables that did not follow a normal distribution for three or more groups.
Pearson correlation analysis was conducted to explore the inter-correlations between KAP scores. KAP scores were dichotomized as dependent variables based on the mean score of each dimension. Univariate and multivariate logistic regression analysis were performed to analyze associations between demographic factors and KAP scores. In the multivariate regression analysis, only variables with P value < 0.05 in the univariate analysis were included. SEM was employed to test the following hypotheses: (1) knowledge directly influences attitude, (2) attitude directly influences practice, and (3) knowledge directly influences practice. Model fit indices were assessed based on the following criteria: root mean square error of approximation (RMSEA) < 0.08, standardized root mean residual (SRMR) < 0.08, comparative fit index (CFI) > 0.80, and Tucker Lewis index (TLI) > 0.8017. P values was recorded with three decimals, and two-tailed P value less than 0.05 was considered statistically significant.
Results
Demographic characteristics
A total of 252 questionnaires were collected, and after removing 23 (9.13%) questionnaires due to incomplete contents or repetitive choices, 229 (90.87%) questionnaires were considered valid for formal analysis. Among the participants, 42.4% were aged between 31 and 40 years. The majority were female (68.6%), held bachelor’s degrees (77.7%), were married (75.1%), and worked as doctors and nurses (98.7%). Additionally, 41.9% had intermediate professional titles, and 90.8% belonged to general hospitals, with 46.3% being in public level 3 hospitals. Moreover, nearly half of the participants had more than 10 years of work experience (46.7%) and attended academic conferences or medical education activities 2–5 times per year (45.0%) (Table 1).
Knowledge
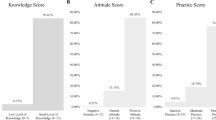
Participants obtained an average knowledge score of 36.27 ± 4.97 with range from 25.00 to 53.00, and 47.3% of participants scored above the mean knowledge score (Table 2). Higher knowledge scores were observed among participants who identified as male (P = 0.019), worked as technicians (P = 0.019), and attended academic conferences or medical education activities 6–10 times per year (P = 0.038) (Table 1). As shown in Table 3, 81.2% correctly identified the definition of multiple myeloma (K1), while only 29.7% were familiar with the different stages of multiple myeloma (K7). The degree of difficulty ranged from 0.297 to 0.883, with the median of 0.761.
Attitude
The participants exhibited an attitude score of 42.40 ± 5.78 with range from 30 to 56, and 54.1% of participants scored above the mean attitude score (Table 2). Male participants (P = 0.041), those with a master’s degree or higher (P < 0.001), doctors (P = 0.002), individuals with a senior professional title (P = 0.013), those affiliated with public level 1 hospitals (P = 0.004), and those attending academic conferences or medical education activities 10 times or more per year (P = 0.002) exhibited higher attitude scores (Table 1). In the attitude section, response rates of “Strongly agree” to “Agree” spanned from 26.2 to 85.1%. Notably, a significant proportion of participants (85.1%) expressed positive attitude towards the importance of support and cooperation from patients and their families during multiple myeloma treatment (A10). Conversely, only 26.2% of participants agreed that after completing multiple myeloma treatment, there was no need for follow-up examinations, and patients could monitor their condition on their own (A8). Similarly, merely 26.2% agreed that after completing multiple myeloma treatment, patients could choose not to follow the doctor’s follow-up plan (A11). The degree of difficulty varied from 0.574 to 0.889, with the median of 0.756 (Table 4).
Practice
The practice score of medical staff showed mean value of 29.71 ± 6.41 ranging from 7 to 35, and 38.0% scored above the mean practice score (Table 2). Higher practice scores were observed among participants who attended academic conferences or medical education activities 10 times or more per year (P = 0.031) (Table 1). Notably, participants demonstrated varying levels of adherence to recommended practices, with proportions ranging from 82.1 to 89.1%. The highest proportion of participants (89.1%) actively conducted regular follow-up examinations and visits during the treatment of multiple myeloma patients (P7). Additionally, the second highest proportion (88.2%) educated multiple myeloma patients about the importance of exercise and dietary management (P6). Moreover, 82.1% regularly observed and recorded the vital signs of multiple myeloma patients (P1). The degree of difficulty varied from 0.819 to 0.877, and the median value was 0.856 (Table 5).
Correlation and logistic analysis
Pearson’s correlation analysis indicated significantly positive correlation between knowledge and attitude (Pearson’s rho = 0.184, P = 0.005) (Table S1). In the univariate analysis, participants with master’s degree or higher education level had significantly higher knowledge scores compared to those with junior college or below (OR = 3.636, 95% CI: 1.054–12.546, P = 0.041). Additionally, nurses exhibited lower knowledge scores compared to doctors (OR = 0.585, 95% CI: 0.346–0.991, P = 0.046). Moreover, participants attending academic conferences or medical education activities 6–10 times per year achieved higher knowledge scores, as evidenced in both univariate (OR = 3.200, 95% CI: 1.191–8.599, P = 0.021) and multivariate analysis (OR = 2.898, 95% CI: 1.022–8.217, P = 0.045) (Table S2).
In the attitude dimension, consistently positive associations between knowledge and attitude scores were observed in both univariate (OR = 1.102, 95% CI: 1.042–1.167, P = 0.001) and multivariate analysis (OR = 1.112, 95% CI: 1.043–1.186, P = 0.001). In the univariate analysis, male participants scored higher in the attitude dimension than female participants (OR = 1.769, 95% CI: 1.008–3.107, P = 0.047). Participants within the age range of 41–50 years (OR = 2.768, 95% CI: 1.284–5.970, P = 0.009) and above 50 years (OR = 3.273, 95% CI: 1.128–9.497, P = 0.029) achieved higher attitude scores. Moreover, participants with bachelor’s degree scored higher in attitude compared to those with junior college or below in the univariate analysis (OR = 2.524, 95% CI: 1.119–5.692, P = 0.026). Additionally, participants with master’s degree or above achieved higher attitude scores in both univariate (OR = 12.519, 95% CI: 2.888–54.255, P = 0.001) and multivariate analysis (OR = 10.199, 95% CI: 1.785–58.265, P = 0.009). In contrast, nurses had lower attitude scores than doctors in the univariate analysis (OR = 0.347, 95% CI: 0.202–0.596, P < 0.001). Furthermore, participants attending academic conferences or medical education activities 10 times or more per year achieved higher attitude scores compared to those with attendances < 2 times (OR = 3.086, 95% CI: 1.098–8.673, P = 0.033) (Table S3).
Regarding the practice dimension, participants attending academic conferences or medical education activities 10 times or more per year achieved higher practice scores (OR = 7.022, 95% CI: 1.525–32.326, P = 0.012) compared to those with attendances < 2 times (Table S4).
SEM
SEM demonstrated a good model fit (RMSEA = 0.064, SRMR = 0.091, TLI = 0.875, CFI = 0.887) (Table S5). Besides, positive association was observed between attitude and practice (β = 4.76, P < 0.001) (Table S6). SEM findings further indicated direct association between attitude and practice (β = 0.320, 95%CI: 0.189–0.452, P < 0.001) (Table 6; Fig. 1). However, no total and direct effects were observed between knowledge and attitude, and between knowledge and practice.

The structural equation model (SEM) showing the associations between KAP scores. Rectangles show observed variables, ellipses indicate potential variables, and circles represent residual terms.
Discussion
The study findings indicated that medical staff had moderate knowledge, neutral attitudes, and proactive practices towards multiple myeloma. Additionally, significantly positive association were observed between knowledge and attitude. Demographic factors, including education level, age, occupation type, and frequency of academic conferences or medical education activities per year, were found to be associated with KAP scores. These results provided valuable insights that can inform the development of healthcare interventions and educational programs targeted at improving KAP among medical staff.
KAP studies offer a scientific foundation for designing targeted interventions that address knowledge gaps, reshape attitudes, and improve practices18. Gaps in KAP were identified in the survey, informing educational programs and policy support to enhance healthcare delivery of multiple myeloma. The moderate knowledge among medical staff in Enshi reflected a common trend in less-resourced settings, where professional training in hematology is limited. Our findings were consistent with previous research from European countries, which revealed significant knowledge gaps among hematologists and nurses regarding multiple myeloma and its treatment agents9. Similarly, a study from the USA showed that clinicians lacked knowledge and confidence in providing patient-specific treatment for multiple myeloma, especially for high-risk cases19. Despite moderate knowledge, medical staff in Enshi exhibited proactive practices. This finding contrasted with the study from USA, where practice gaps persisted among clinicians despite high awareness of screening testing20. Besides, Belarusian physicians exhibited good understanding of the role of autologous stem-cell transplantation (ASCT) as first-line treatment for multiple myeloma, and the majority practiced first-line treatment for more than 4 months21. The KAP gaps herein can inform the essentiality of building local capacity in Enshi region, such as practical workshops tailored to regional needs.
The knowledge dimension revealed both positive and concerning aspects of medical staff’s knowledge of multiple myeloma. A significant proportion (81.2%) correctly identified the definition of multiple myeloma, indicating good level of awareness. This understanding was essential as it formed the basis for accurate diagnosis and appropriate management. However, only 29.7% exhibited familiarity with the stages of multiple myeloma. The slow development and uneven advancement of hematology in the Enshi region emerge as key contributing factors. Considering the critical importance of understanding disease stages for implementing precise treatment strategies, it is essential to organize targeted educational programs and training sessions for medical staff in this area22. These initiatives would play a significant role in fostering the continuous enhancement of their professional expertise.
The attitude section yielded valuable insights into medical staff’s perspectives and beliefs regarding multiple myeloma treatment. A significant proportion (85.1%) exhibited positive attitude towards the importance of patient and family support during treatment, highlighting their recognition of its crucial role in managing multiple myeloma. Since emotional and psychological support from loved ones could greatly impact the well-being and treatment outcomes of patients, understanding the significance of such support could enable medical staff to adopt holistic approach to patient care and address their overall well-being. However, a low agreement rate (26.2%) was observed regarding the necessity of follow-up examinations and patients’ ability to self-monitor their condition after completing treatment. Similarly, more than a quarter (26.2%) agreed that patients could choose not to follow the doctor’s follow-up plan after treatment, indicating negative attitude towards adhering to medical advice and treatment plans. Regular follow-up examinations are essential for assessing treatment efficacy, monitoring potential relapses, and managing treatment-related side effects23. Due to the significance of compliance in ensuring timely intervention24,25, grassroots myeloma training courses should be expanded to include post-treatment monitoring and patient education. To ensure sustainability and scalability, submitting proposals is recommended to the State Health Commission to prioritize hematology education, including organizing academic seminars and offering training opportunities for local medical staff.
The results of practice dimension shed light on medical staff’s adherence to recommended practices for treating multiple myeloma patients. One noteworthy discovery was that 89.1% consistently conducted follow-up examinations and visits during treatment. Another significant observation was that 88.2% proactively educated multiple myeloma patients about exercise and dietary management. By informing patients about exercise and dietary considerations, medical staff could empower them to play an active role in their treatment journey, potentially leading to improved lifestyle choices, treatment efficacy, and quality of life26,27. Furthermore, 82.1% regularly observed and recorded vital signs of multiple myeloma patients. This vigilant monitoring was crucial for promptly identifying changes in the patient’s health status and addressing potential complications28. Although overall adherence to recommended practices was relatively high, it was essential to acknowledge room for improvement. Some medical staff did not fully adhere to certain practices, highlighting the need for targeted interventions and educational programs to address these areas of concern.
No significant correlations of knowledge and attitude with practice were observed, indicating that possessing knowledge and positive attitude towards multiple myeloma might not necessarily lead to better adherence to recommended practices among medical staff. Several explanations could account for this lack of correlation. Firstly, unexamined factors like institutional policies, resource availability, time constraints, and workload might influence medical staff’s practices towards multiple myeloma patients29,30. Secondly, the complexity of the disease and patient diversity could also contribute to the absence of correlation31,32. Additionally, the research unveiled the positive association between knowledge and attitude towards multiple myeloma, which aligned with the theory of planned behavior that attitude was shaped by beliefs about behavioral outcomes33. The non-significant associations of knowledge with attitudes and practices were reported in SEM, suggesting the gaps in knowledge translation. Also, SEM analysis reveal a direct association between attitudes and practices. In resource-limited settings like Enshi, where medical staff may face additional challenges such as limited access to continuing education, fostering positive attitudes toward multiple myeloma care may be a more pragmatic approach than focusing solely on knowledge dissemination. Taken these results together, educational programs that enhance knowledge and foster attitudinal shifts towards multiple myeloma can be pivotal for better management. Further, since this study was regional, replicating this research in different settings could validate the universality of these findings and potentially lead to broader policy changes in cancer care.
This study had some limitations. Firstly, it was carried out in solitary region with relatively limited sample size, potentially constraining the generalizability of the outcomes. Nevertheless, these findings could serve as fundamental reference for evaluating the impacts of forthcoming educational interventions on medical staff in terms of preventing and treating multiple myeloma. Besides, the cross-sectional design limited the ability of causal inference. Intervention-based designs are needed to better understand how educational initiatives or policy implementations may influence behavior and attitudes over time. Moreover, the KAP findings might have been swayed by social desirability bias, potentially resulting in inflation of scores, since participants might have given socially desirable answers rather than reflecting their actual behaviors34 .
Conclusions
In conclusion, medical staff exhibited moderate knowledge, neutral attitudes, and proactive practices towards multiple myeloma. Moreover, a significant positive correlation was observed between knowledge and attitude scores. Targeted educational interventions were recommended to enhance knowledge and attitudes, especially among specific groups, such as female individuals, those with bachelor’s degrees or lower education, nurses, and individuals with lower professional titles.
Data availability
All data generated or analysed during this study are included in this published article and its supplementary information files.
References
Fairfield, H., Falank, C., Avery, L. & Reagan, M. R. Multiple myeloma in the marrow: pathogenesis and treatments. Ann. N Y Acad. Sci. 1364, 32–51 (2016).
Bridoux, F. et al. Management of acute kidney injury in symptomatic multiple myeloma. Kidney Int. 99, 570–580 (2021).
Cowan, A. J. et al. Diagnosis and management of multiple myeloma: a review. Jama 327, 464–477 (2022).
Huang, J. et al. The epidemiological landscape of multiple myeloma: a global cancer registry estimate of disease burden, risk factors, and temporal trends. Lancet Haematol. 9, e670–e677 (2022).
Padala, S. A. et al. Epidemiology, staging, and management of multiple myeloma. Med. Sci. (Basel) 9, (2021).
Liu, J. et al. Burden of multiple myeloma in China: an analysis of the Global Burden of Disease, injuries, and risk factors study. Chin. Med. J. (2019).
Larsen, R. F. et al. Physical function in patients newly diagnosed with multiple myeloma; a Danish cohort study. BMC Cancer. 20, 169 (2020).
Niazi, S. et al. Impact of psychiatric comorbidities on health care utilization and cost of care in multiple myeloma. Blood Adv. 2, 1120–1128 (2018).
Murray, S. et al. Identifying educational needs and practice gaps of European hematologists and hematology nurses in the treatment and management of multiple myeloma. Hemasphere 2, e33 (2018).
Nicol, J. L., Hill, M. M., Burton, N. W. & Skinner, T. L. Promoting exercise for patients with multiple myeloma: attitudes and practices of clinical haematologists. J. Cancer Surviv. 16, 688–695 (2022).
Brody, H. Multiple myeloma. Nature 480, S33 (2011).
Urban, V. S., Cegledi, A. & Mikala, G. Multiple myeloma, a quintessential malignant disease of aging: a geroscience perspective on pathogenesis and treatment. Geroscience 45, 727–746 (2023).
[The guidelines for the. Diagnosis and management of multiple myeloma in China(2020 revision)]. Zhonghua Nei Ke Za Zhi. 59, 341–346 (2020).
Schrepp, M. On the usage of Cronbach’s alpha to measure reliability of UX scales. J. Usability Stud. 15, (2020).
Chae, Y. M., Park, S. G. & Park, I. The relationship between classical item characteristics and item response time on computer-based testing. Korean J. Med. Educ. 31, 1–9 (2019).
Alzahrani, M. M., Alghamdi, A. A., Alghamdi, S. A. & Alotaibi, R. K. Knowledge and attitude of dentists towards obstructive sleep apnea. Int. Dent. J. 72, 315–321 (2022).
Sathyanarayana, S. & Mohanasundaram, T. Fit indices in structural equation modeling and confirmatory factor analysis: reporting guidelines. Asian J. Econ. Bus. Acc. 24, 561–577 (2024).
Launiala, A. How much can a KAP survey tell us about people’s knowledge, attitudes and practices? Some observations from medical anthropology research on malaria in pregnancy in Malawi. Anthropol. Matters 11, (2009).
Ritter, L. M., Fagerlie, S. R., Ghobrial, I. M., Vij, R. & Repetto P. Current practices in managing multiple myeloma (MM): elucidating Educational needs of Hematology/Oncology clinicians. Clin. Lymphoma Myeloma Leuk. 17, 329 (2017).
Derman, B. A., Jasielec, J. K. & Jakubowiak, A. J. Clinician attitudes and practices toward measurable residual disease in multiple myeloma. Br. J. Haematol. 190, 470–472 (2020).
Iskrou, I., Uss, A., Golubev, S. & Papok, V. Physicians’ behavior, diagnostics and treatment patterns in multiple myeloma management in belarus: nation-wide survey. Blood 132, 5853 (2018).
Dhanasekaran, R., Suzuki, H., Lemaitre, L., Kubota, N. & Hoshida, Y. Molecular and immune landscape of hepatocellular carcinoma to guide therapeutic decision making. Hepatology (2023).
Berenbaum, F. et al. Subcutaneous tanezumab for osteoarthritis of the hip or knee: efficacy and safety results from a 24-week randomised phase III study with a 24-week follow-up period. Ann. Rheum. Dis. 79, 800–810 (2020).
Breckenridge, A. et al. Poor medication adherence in clinical trials: consequences and solutions. Nat. Rev. Drug Discov. 16, 149–150 (2017).
Carls, G. S. et al. Understanding the gap between efficacy in randomized controlled trials and effectiveness in real-world use of GLP-1 RA and DPP-4 therapies in patients with type 2 diabetes. Diabetes Care. 40, 1469–1478 (2017).
Chang, Y. L. et al. The effectiveness of a nurse-led exercise and health education informatics program on exercise capacity and quality of life among cancer survivors after esophagectomy: a randomized controlled trial. Int. J. Nurs. Stud. 101, 103418 (2020).
Hamidi, S., Gholamnezhad, Z., Kasraie, N. & Sahebkar, A. The effects of self-efficacy and physical activity improving methods on the quality of life in patients with diabetes: a systematic review. J. Diabetes Res. 2022 (2022).
Muth, C. et al. Evidence Supporting the best Clinical Management of Patients with Multimorbidity and Polypharmacy: A Systematic Guideline Review and Expert Consensus 272–288 (Wiley Online Library, 2019).
Mosadeghrad, A. M. Factors affecting medical service quality. Iran. J. Public. Health. 43, 210–220 (2014).
Cranage, K. & Foster, K. Mental health nurses’ experience of challenging workplace situations: a qualitative descriptive study. Int. J. Ment Health Nurs. 31, 665–676 (2022).
Marinac, C. R., Ghobrial, I. M., Birmann, B. M., Soiffer, J. & Rebbeck T. R. dissecting racial disparities in multiple myeloma. Blood Cancer J. 10, 19 (2020).
Schavgoulidze, A., Cazaubiel, T., Perrot, A., Avet-Loiseau, H. & Corre, J. Multiple myeloma: heterogeneous in every way. Cancers (Basel) 13, (2021).
Bosnjak, M., Ajzen, I. & Schmidt, P. The theory of planned behavior: selected recent advances and applications. Europe’s J. Psychol. 16, 352 (2020).
Bergen, N. & Labonté, R. Everything is perfect, and we have no problems: detecting and limiting social desirability bias in qualitative research. Qual. Health Res. 30, 783–792 (2020).
Author information
Authors and Affiliations
Contributions
Luping Zou and Jinhua Li carried out the studies, participated in collecting data, and drafted the manuscript. Luping Zou, Jinhua Li and Hang Xiang performed the statistical analysis and participated in its design. Jun Tan and Yan Zeng participated in acquisition, analysis, or interpretation of data and draft the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This work has been carried out in accordance with the Declaration of Helsinki (2000) of the World Medical Association. The work was approved by the Ethics Committee of the Central Hospital of Enshi Tujia and Miao Autonomous Prefecture (2023-075-001). Informed consent was obtained from participants.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zou, L., Li, J., Xiang, H. et al. Knowledge, attitude and practice towards multiple myeloma among medical staff in Enshi Region. Sci Rep 15, 3406 (2025). https://doi.org/10.1038/s41598-025-88079-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-88079-0
