
Abstract
The neural mechanisms underlying time perception remain elusive. Although the cerebellum (CE) and basal ganglia (BG) are considered fundamental, evidence primarily stems from studies on neurodegenerative diseases, where progressive and widespread damage complicates linking deficits to specific brain structures. In contrast, brain stroke affects focal areas suddenly, allowing for the assessment of immediate functional consequences. Here, we compared patients with acute stroke in the CE and BG to age-matched healthy controls (HC) on both explicit (time bisection, free and 1-second finger tapping) and implicit (rhythmic, temporal orienting) timing tasks. Concerning explicit timing, both CE and BG patients were faster than HC in their free finger tapping, while BG lesions showed greater variability than HC in the 1-second tapping. Similarly, performance on the bisection task suggested deficits more related to cognitive complaints in stroke than specific temporal dysfunction. In implicit timing tasks, BG patients, like HC, effectively used information provided by the rhythm and the temporal orienting cues to anticipate the target onset, whereas CE patients failed and showed longer reaction times. Therefore, before compensatory mechanisms can take effect, acute CE damage might hinder implicit timing, whereas BG lesions could disrupt explicit temporal representation when processed alongside other cognitive functions.
Similar content being viewed by others

Introduction
Time perception is a crucial skill in everyday life and is even more relevant in activities that require fine motor planning and coordination, such as art and agonistic sports1. Based on extensive behavioural research, current evidence suggests that time intervals between seconds and minutes are essential in decision-making, while milliseconds are crucial for speech, motor control, and art2. Reasonably, the temporal processing of intervals longer than approximately one second requires cognitive involvement, whereas shorter intervals are highly perceptual, fast, parallel, and not accessible to cognitive control3,4. In order to better understand the mechanisms by which the brain represents the passage of time, an important distinction between explicit and implicit timing tasks has been identified5. The former refers to tasks in which the participant must explicitly provide an evaluation of temporal duration, e.g. by judging whether one stimulus is longer or shorter than another (“perceptual timing”) or by producing motor acts that have a duration, latency, or periodicity corresponding to those of a given time interval (“motor timing”). Implicit timing tasks, on the other hand, have non-temporal task goals but still require adherence to a precise temporal framework both in terms of inputs (i.e. temporal predictability of the next stimulus) and motor outputs (as a by-product of motor control dynamics) in an unintentional (“exogenous”) or deliberate (“endogenous”) way6.
However, the neurobiological mechanisms and neurophysiological underpinnings of time perception remain unclear1,7. Numerous theories and computational models have been formulated to identify the mechanisms accounting for the passage of time in the central nervous system (CNS), with some proposing time as an emergent property linked to the shared operational computations of all neuronal circuits8. However, these models often do not consider the possibility of combining temporal perceptions mediated by different sensory modalities9. Indeed, many studies highlighted that, although many different areas of the CNS are activated during temporal tasks (depending on, for example, the type of stimulus, cognitive load, and time interval), it is very unlikely that there is absolute decentralization and that each modality-specific circuit contains independent time measurements10.
Therefore, currently, the prevailing models are population ones, wherein time perception arises as an outcome of the collective activity of extensive populations of dynamically interacting neurons11, and several possible frameworks for the mechanism of temporal perception have been hypothesised: the specialised timing model, according to which particular brain regions show the unique ability to represent specific features of temporal data, and the distributed network timing model, which predicts an interaction between vast networks of neuronal groups to mediate temporal perception12. Although it is difficult to isolate the contribution of individual structures, considering the extensive connections between brain regions and the involvement of cortical areas in some temporal tasks - especially with a higher cognitive load7,13 – a great deal of evidence identifies the basal ganglia and the cerebellum as fundamental regions in time perception1,14,15.
Specifically, the basal ganglia seem to be involved in time intervals spanning both milliseconds and seconds range, and the dopaminergic circuit, encompassing the substantia nigra pars compacta, striatum, and frontal regions, might be an ideal candidate to perform this activity1,7. Indeed, the basal ganglia are involved in most explicit timing tasks, both perceptual16,17 and motor18,19 ones, as long as they last at least a few hundred milliseconds5. However, it is worth noting that alternative interpretations suggest an important role even in time intervals greater than one second, particularly when time is processed consciously, highlighting that their functional specialization remains largely unknown, at least in the context of temporal information processing7. Importantly, the administration of dopaminergic drugs or lesions affecting this network can significantly alter time perception20. Moreover, Parkinson’s disease (PD) patients, characterised by diminished dopamine levels resulting from substantia nigra degeneration, provide a direct means to assess the effects of this alteration and the differences observed following dopaminergic drug administration from a temporal perspective21,22. Importantly, PD patients show particularly marked alterations in explicit timing tasks in comparison to implicit timing ones, supporting the involvement of basal ganglia in this specific set of tasks23. However, the evidence is still often conflicting, reasonably due to different PD phenotypes (e.g. drug therapy, disease stage)24 and the potential impact of the dopaminergic system on other neural systems beyond the basal ganglia, which could affect performance in specific temporal perception tasks25,26. Therefore, it is possible that the widespread dopamine deficit that characterises PD is not ideal for assessing the implications on temporal perception.
Conversely, the cerebellum plays a key role especially when participants have to quickly estimate the passage of short time intervals and when time is processed in relation to specific salient events27,28. Indeed, it is fundamental in movement coordination, which implies a substantial temporal component, and its alterations can lead to a loss of temporal organisation of motor sequences29. Importantly, patients affected by cerebellar lesions perform continuous movements smoothly, whereas movements requiring precise timing of particular salient events (such as rhythmically tapping fingers) are impaired30,31. Moreover, cerebellar damage results in increased variability, particularly evident in tasks involving temporal production and the execution of precisely timed isolated movements31, along with compromised ability in discriminating durations30,32. Thus, it is hypothesised that the cerebellum explicitly encodes the timing of discrete successive events, especially in the millisecond range7, and it is particularly active in the explicit timing of motor, rather than perceptual, tasks33. Interestingly, however, the cerebellum seems also involved in implicit timing, both in exogenous34 and endogenous35 temporal expectations.
Crucially, a recent study on patients affected by PD or cerebellar degeneration demonstrated a double dissociation in temporal tasks, showing that basal ganglia and cerebellum contribute to functionally distinct mechanisms of rhythm- and interval-based temporal prediction for attentional orienting, respectively36. Furthermore, another work by the same group showed that cerebellar degeneration leads to deficits in temporal interval tasks but not in rhythmic ones, emphasising that the functional specificity of the cerebellum for interval-based tasks involves several domains (including the attentional one), especially in the sub-second range37.
However, study models using slow-evolving pathologies (such as PD or cerebellar neurodegeneration) often do not allow changes related to the dysfunction of a system to be assessed on its own, as chronic progression enables the CNS to recruit other regions to mediate the impaired functions, making it difficult to discriminate the roles played by the different involved areas38,39,40. Moreover, neurodegenerative diseases, although mainly affecting certain systems, often also damage other CNS districts directly or indirectly, making the interpretation of results much more complex41,42.
Conversely, stroke is characterised by the sudden onset of an often focal neurological deficit that may affect specific brain areas depending on the vascular territory affected by the ischaemic or haemorrhagic damage43. Therefore, excluding cases with massive extensions, it allows the functional consequences of focal damage to be investigated, and it has been used as a study model in numerous conditions44,45. Indeed, since brain reorganisation processes that restore impaired functions and/or replace them using other areas take several weeks to complete, it is possible to assess the immediate functional consequences of an injury in a specific brain area46. Moreover, brain stroke is the second most common cause of death and long-term disability worldwide43 and, among the common deficits that follow cerebrovascular damage, altered time perception is often described47,48,49.
These considerations are particularly relevant given that some studies examined patients with focal lesions in the basal ganglia and cerebellum, providing more precise insights into the roles of these structures in timing tasks. For instance, cerebellar lesions disrupt the precise timing of discrete movements but have less impact on continuous motor tasks, highlighting the cerebellum’s critical role in discrete interval-based timing31. Notably, a functional specialization within the cerebellum itself has been suggested, with lateral regions playing a key role in the precise timing of discrete movements, while medial areas are more involved in the execution of coordinated movement sequences50. Conversely, patients with unilateral striatal lesions exhibit only minor impairments in force control and, compared to controls, no significant temporal performance alterations, even when using the hand contralateral to the brain damage51. This is crucial, as suggested by the authors, in underscoring the need for caution when relying on neurodegenerative disease models to understand the functioning of neural networks. However, it is important to note that such studies remain scarce in the literature, typically feature small sample sizes, frequently mix different pathological conditions (e.g., tumors, stroke, atrophy), and, most importantly, primarily focus on the chronic phase of the disease. By this stage, network reorganization may have already occurred, making it considerably more challenging to draw definitive conclusions.
Taken together, these findings suggest that stroke, especially in the early stages, represents a valuable model for assessing the functional consequences of damage to crucial areas in the physiological perception of time, i.e. the cerebellum and basal ganglia, and to shed light on the still controversial aspects of time perception. Indeed, although each study model entails specific strengths and limitations, an acute and focal injury of regions most critically involved in the perception of time, without the confounding linked to the involvement of other areas (which occurs at a later time), should allow us to understand the role physiologically played in this context by the cerebellum and basal ganglia and to assess their different contribution in the various temporal tasks (i.e. implicit vs. explicit, sub-second vs. supra-second).
Here, we investigated differences in time perception between acute phase stroke patients with basal ganglia (BG) or cerebellar (CE) lesions and healthy controls (HC), using four well-established paradigms in the framework of time perception research: a time bisection task and a finger tapping task, in order to evaluate the explicit timing; and, a rhythmic task and a temporal orienting task, in order to assess the implicit time processing. This allowed us not only to assess the differences between healthy individuals and acute stroke patients but also to evaluate the functional implications of basal ganglia and cerebellum lesions on different aspects of temporal perception.
Results
Neuropsychological assessment
Separate one-way ANOVAs were conducted on performances at neuropsychological tasks in HC, CE, and BG participants. A significant difference was observed in the Rey Auditory Verbal Learning Test (RAVLT; delayed condition) between HC and CE (p = 0.020), indicating that HC were more accurate than CE; moreover, a significant difference was observed in the Rey-Osterrieth complex figure (ROCF; delayed condition) between BG and CE (p = 0.028) indicating that BG were more accurate than CE (Table 1).
Explicit timing
Finger tapping task
Free finger tapping: As shown in Table 2; Fig. 1, the results indicated a main effect of Group when data were analysed in terms of mean Inter Tapping Interval (ITI) [F(2, 39.4) = 7.79, p = 0.001], highlighting that older adults were slower than CE (p = 0.036) and BG patients (p = 0.012). Moreover, main effect of Group was observed on Coefficient of Variability (CV) [F(2, 23.4) = 3.61, p = 0.043], however we found no significant differences at post-hoc comparisons.
1-sec finger tapping: The results presented in Table 2; Fig. 1, indicated no effect of Group on ITI (p = 0.210). Main effect of Group was observed on Coefficient of Variability (CV) [F(2, 19.4) = 3.58, p = 0.047]; post-hoc analyses indicated that BG patients were more variable than healthy older adults (p = 0.001); we found no significant differences between healthy older adults and CE patients (p = 0.659), nor between CE and BG patients (p = 0.112) (Table 2).

Free finger tapping task: (A) Mean Inter Tapping Interval (ITI) and (B) Coefficient of Variability as a function of Group. 1-sec finger tapping task: (A) Mean Inter Tapping Interval (ITI) and (B) Coefficient of Variability as a function of Group. Each dot represents a participant.
Time bisection task
Compared to HC, we found no significant differences in terms of accuracy for both the BG (risk ratio = 1.14, p = 0.445) and CE (risk ratio = 0.89, p = 0.513) groups. However, they significantly differed in terms of precision (BG: risk ratio = 0.67, p = 0.016; CE: risk ratio = 0.60, p = 0 0.005). As shown in Fig. 2, both the BG and CE groups exhibited flatter psychometric curves compared to the HC group. To assess differences between BG and CE, we refitted the probit regression with BG as the reference level for the Group factor. Based on these results, we found no significant differences between the two groups in terms of accuracy (risk ratio = 0.78, p = 0.244) or precision (risk ratio = 0.90, p = 0.599).

Psychometric curves for time bisection tasks. The figure shows the psychometric curves for the healthy control (HC; blue line), basal ganglia (BG; orange dashed line) and cerebellar (CE; green dotted line) groups. Flatter curves in basal ganglia (BG) and cerebellar (CE) groups indicate reduced precision compared to healthy controls (HC). For illustrative purposes, temporal intervals are reported on x-axes. Shaded error bars indicate 95% confidence intervals.
The probit mixed-effects regression offers information about the intercepts and slopes of psychometric curves. Past studies often focused on two key measures: the bisection point (BP) and just noticeable difference (JND), which reflect temporal discrimination accuracy and precision, respectively. To facilitate comparisons with earlier studies, as in Visalli and colleagues (2024)52, we fitted a probit mixed-effects regression without Group as a predictor and used the participants’ random intercepts and slopes from the model to calculate BPs and JNDs. Table 3 presents the means and standard deviations of BPs and JNDs for each group, and Fig. 3 provides a graphical representation of participants’ performance. Oneway ANOVA was conducted on BP and JND. No significant differences were found on BP between groups [F(2, 64) = 0.25; p = 0.443]; whereas significant differences were found on JND between groups [F(2, 64) = 0.25; p = 0.443] (BG vs. HC p = 0.221; CE vs. HC p = 0.053; BG vs. CE p = 0.753).

(A) Bisection Point (BP) and (B) Just Noticeable Differences (JNDs) by Group for the Time bisection task. Each dot represents a participant.
Implicit timing
Rhythm task
Concerning our effects of interest, we did not find any simple effect for BG (risk ratio = 0.07; p = 0.671) and CE (risk ratio = 0.11; p = 0.564). Moreover, we found a significant Rhythm effect, indicating an advantage in regular compared to irregular rhythmic sequences for the HC. Finally, concerning the interactions between Group and Rhythm, it was not significant for BG (risk ratio = 0.01; p = 0.775), but it was significant for the CE group (risk ratio = 0.14; p = 0.008). As shown in Fig. 4, while both the HC and BG groups showed shorter inverse-transformed Reaction Times (iRTs) after regular compared to irregular sequences, differences between regular and irregular sequences were negligible in the CE group.

Interaction plot of the effects of Rhythm and Group in the rhythm task. The figure shows the estimated marginal means for the healthy control (HC; left), basal ganglia (BG; middle), and cerebellar (CE; right) groups in irregular (blue) and regular (orange) rhythm conditions. Error bars indicate 95% confidence intervals. The asterisks indicate significant differences between Irregular and Regular rhythms within each group, as determined by pairwise comparisons using estimated marginal means with p < 0.001. For illustrative purposes, inverse-transformed reaction times have been rescaled to show response times in milliseconds on the y-axis.
Temporal orienting task
The results of the linear mixed-effects regression are presented in Table 4. Concerning our effects of interest, we found a significant interaction between Cue and Stimulus Onset Asynchrony (SOA), indicating the presence of a temporal orienting effect in the HC group. When examining between-group differences, we found no simple or interaction effects for BG (all p > 0.406). However, for the CE group, we observed a significant three-way interaction (p < 0.001). As shown in Fig. 5, while both the HC and BG groups exhibited shorter iRTs for validly-cued short SOAs compared to invalid ones, the CE group displayed longer iRTs for short SOAs, regardless of the cue.

Interaction plot of the effects of Cue, SOA and Group in the temporal orienting task. The figure shows the estimated marginal means for the healthy control (HC; left panel), basal ganglia (BG; middle panel), and cerebellar (CE; right panel) groups in early and late cue conditions for 350 ms (top row) and 1350 ms (bottom row) SOAs. Blue points and lines represent valid trials, while red points and lines represent invalid trials. Large points and error bars indicate group means and 95% confidence intervals, respectively. Small points connected by grey lines represent individual estimates. For illustrative purposes, inverse-transformed reaction times have been rescaled to show response times in milliseconds on the y-axis. The asterisks above panels indicate the significance level of the difference between valid and invalid trials for each group and SOA condition (*p ≤ 0.05, **p ≤ 0.01, ***p ≤ 0.001), based on pairwise comparisons with Tukey’s correction for multiple comparisons.
Discussion and conclusions
Time perception is a fundamental skill in everyday life, but its neurophysiological underpinnings are still largely unknown. Most studies have focused on disorders with widespread, slowly progressing alterations, which allow unaffected regions to compensate for the affected ones38,39,40. Consequently, while previous research identified the typical alterations in temporal task performance in pathological contexts such as PD or cerebellar degeneration, it might not be optimal to unambiguously attribute deficits to lesions affecting particular brain areas. Thus, here, we enrolled patients affected by early-stage cerebellar or basal ganglia stroke to assess the immediate consequences on temporal functions. Thereby, we aimed to evaluate their role in timing function and detail their specific contributions to this complex activity.
Importantly, stroke patients performed similarly to HC in neuropsychological evaluations. This allowed us to rule out the possibility that the differences in temporal task performance arose from age-related factors or baseline cognitive conditions. Exceptions were observed in the RAVLT and ROCF (both in the delayed phase) for CE patients, where HC performed better. However, memory performance alterations are a common finding after stroke irrespective of the damaged area, especially in episodic memory, and are at least partly due to the stress and significant emotional impact related to the clinical condition53,54. Furthermore, the cerebellum’s role in different cognitive functions, especially in complex tasks, even considering its significant connections with the frontal-parietal cortical network, which is pivotal in these activities, might provide a further explanation for these differences29. Therefore, to minimise potential confounding factors, only patients able to fully understand and attentively participate were included, with ample practice opportunities and breaks provided as needed.
About the finger tapping task, which assesses the participant’s ability to produce motor responses at an arbitrarily chosen or fixed rhythm of 1 s, significant differences were observed in both cases. Specifically, in the free finger tapping, HC tapped significantly slower than stroke patients, while we found no significant differences between CE and BG groups. Importantly, this suggests that the stroke itself, rather than the specific lesion site, leads to the choice of an arbitrarily faster rhythm compared to the preferred one of healthy age-matched participants. This finding may suggest a link between the emotional state of patients and the speed of the internal clock, possibly mediated by the cortical insular region and influenced by anxiety and concern about one’s health condition55. Such a link, consistent with known paradigms of sensorimotor integration, may have accelerated the patients’ internal clock, resulting in a preference for a faster motor pattern, although further research is needed to confirm this hypothesis56. However, stroke may also lead to a less efficient representation and functioning of internal models linking motor actions to sensory consequences, depending on the specific lesion site. Indeed, both cerebellar and basal ganglia lesions, key regions for generating and optimizing sensorimotor models, may result in a less effective representation of the sensorimotor relationship29. This inefficiency could lead to a faster rhythm to increase the granularity of afferent information and provide more frequent updates to the internal models. This is particularly relevant considering recent evidence suggesting that both monosynaptic and disynaptic connections between the cerebellum and basal ganglia may be crucial for internal model updating29,57. Thus, damage in either structure could correlate with alterations in these functions.
While in the free finger tapping task, each participant chose the rhythm freely, in the 1-sec finger tapping, it was imposed by the experimental conditions. This method ensures greater consistency in the results, as participants were explicitly instructed about the specific rhythm to adopt. In other words, each participant was asked to identify the duration that ideally corresponded to one second and reproduce it during the task. Thus, participants likely held the absolute interval matching the required duration in their working memory58. Although none of the participants reported difficulties in performing the tapping itself, while we found no significant differences for CE patients compared to healthy controls, BG patients exhibited greater variability than controls. As mentioned above, although the existing literature is highly heterogeneous, these findings appear consistent with those reported in PD patients, who experience difficulty in rhythm extraction and comparing rhythmic sequences59. Furthermore, our results align with those previously reported by Schwartze et al., demonstrating that patients with focal lesions in the basal ganglia exhibit more heterogeneous individual rhythms and more significant tapping variability, even when synchronizing to an external rhythm rather than generating one internally56. These findings support the role of the basal ganglia, as part of the cortico-striato-thalamo-cortical circuit, in temporal processing dependent on attention and interval-based timing2. Although this function is typically supported by an extensive cortico-subcortical network, the lack of differences between patients and controls in neuropsychological tests assessing executive functions suggests that the alterations observed are primarily attributable to the basal ganglia rather than attentional or working memory differences associated with cortical areas, especially the prefrontal regions60. While previous studies have shown that cerebellar lesions can be associated with increased variability in rhythmic pattern execution, depending on the lesion’s location and extent, the stabilizing influence of task repetition may have reduced variability measures, as demonstrated by our results and suggested by other authors30,56,61.
Regarding the second explicit timing task, namely the time bisection task, our results highlight that patients perform worse than HC without specific differences related to the brain lesion site. In particular, the demonstration of a flattened psychometric curve in both patient groups suggests that this outcome may depend more on purely cognitive aspects rather than alterations of the internal clock functioning. Indeed, if the latter were true, one would expect differences between the two patient groups due to the functional specialization in temporal information processing of these brain regions, namely the cerebellum and basal ganglia1. Conversely, the first hypothesis, consistent with our results, seems attributable to a ‘noisier’ memory representation of the standard interval durations. Indeed, as previously pointed out, patients differed from HC only in memory performance, as is often the case after a stroke53. This is particularly true for CE patients, but even those with BG lesions reported lower scores than HC, although not significantly, on the RAVLT, which critically depends on the integrity of memory functions62. Importantly, various pieces of evidence correlated memory abilities with temporal bisection tasks63,64. Coherently, not only do these functions share anatomical underpinnings, but pacemaker-based models of time perception assign a crucial role to memory in temporal bisection performance65,66,67. This could explain the flattened curve resulting from a poor representation of the duration ‘anchors’ in memory. Notably, these findings are supported by a recent study demonstrating that explicit timing tasks, such as duration discrimination, are critically dependent on broader cognitive resources across the adult lifespan52. Indeed, the authors showed that declines or reduced cognitive efficiency can lead to increased variability in explicit timing tasks, even in the absence of fundamental deficits in time processing. Consistently, the flattened psychometric curve observed in our patient groups could be interpreted as a consequence of such general cognitive challenges rather than a specific impairment in temporal information processing. Importantly, while these factors significantly affect explicit timing tasks, implicit ones appear to be less affected by such impairments52. This distinction highlights the role of cognitive load in explicit timing, particularly in conditions where neurological dysfunction may exacerbate cognitive inefficiency. Taken together, the results from the explicit timing tasks suggest an apparently limited (or at least not as dominant as expected) role for the basal ganglia, restricted to certain cognitively demanding tasks, and, especially, the cerebellum in this context, although some of the differences discussed earlier suggest that additional factors warrant further investigation. In contrast, the role of these subcortical regions - and the cerebellum in particular - was much more consistent in implicit timing tasks.
Specifically, in the rhythmic task, healthy controls, as expected, effectively used the information provided by the rhythm to prepare the subsequent motor response68. However, notably, while BG patients exhibited a faster motor response when the target was preceded by a regular rhythm compared to an irregular one (i.e., they were able to use the preparatory effect provided by the rhythm), CE patients were unable to use this information to prepare the motor response. This finding is, in some respects, unexpected, as previous studies have shown a double dissociation in temporal tasks, specifically showing that basal ganglia regulate the mechanisms of rhythm-based temporal prediction, while the cerebellum those of interval-based prediction36. However, it is important to note that their sample consisted of patients affected by neurodegenerative diseases, leading to the already discussed limitations, i.e., slow progression and widespread damage. Additionally, they employed a different paradigm to assess the performance of the patients in the rhythmic timing. Specifically, while their timing target was entirely predictable - given that they selected intervals between all stimuli identical to the target interval in each trial, ensuring it occurred on-beat within the induced rhythm - our experiment was designed to evaluate both the presentation of a regular and an irregular rhythm within the same session, to assess performance differences based on the type of rhythmic information. Furthermore, notably, this paradigm allowed us to assess participants using a truly exogenous rhythmic task, whereas other approaches might also introduce an endogenous component due to the instructions provided to participants or the way rhythmic information was manipulated69. These methodological aspects might explain the differences from previous evidence, given that the study populations and task stimuli were different. Moreover, a recent study demonstrated that, even in the domain of speech, patients with cerebellar degeneration were largely insensitive to the speaker’s rate and rhythm, whereas those with PD showed a stronger propensity to adapt than the controls70. Consistently, our data suggest that the cerebellum may be critical in regulating the rhythmic aspect of motor behavior when it is based on repeated temporally salient events, which allow for the updating of the sensorimotor representation through each repetition30,71. In contrast, the basal ganglia might be fundamental in shaping the most efficient motor pattern for performing the task through fine regulation of the effectors to be used (via the direct pathway) and inhibition of antagonistic or non-useful ones (via the indirect pathway)72. Accordingly, these complementary roles may explain the observed deficits. Indeed, in the case of cerebellar lesions, the inability to process rhythmic information prevents these patients from benefiting from the regular rhythm to facilitate the subsequent motor response. Conversely, in basal ganglia lesions, the rhythm is still processed at the cerebellar level and provides preparation for the subsequent motor act, though likely with reduced efficiency due to impaired motor pattern optimization73. However, as intriguingly suggested, the cerebellum could be dynamically involved in both types of predictions, one based on rhythmic information and the other on remembered temporal associations, depending on the time interval between the events74.
Finally, the temporal orientation task also revealed a prominent role for the cerebellum in temporal information processing. Indeed, not only HC but also BG patients were able to use the combination of cue and time interval to prepare their motor responses, highlighting that both these groups exhibited a temporal orienting effect. In contrast, CE patients showed longer reaction times, in particular for shorter intervals, regardless of cue validity. Thus, they demonstrated difficulty managing temporal information, especially at shorter durations. These results are consistent with recent findings showing preservation of facilitation of motor responses by temporal orienting in the context of basal ganglia lesions, such as in striatal damage or PD patients23,36,75,76. In addition, previous research highlighted that deficits in temporal orienting are critically associated with frontal lesions, particularly in the prefrontal areas69,75. These data suggest that the basal ganglia may not play a predominant role in temporal orienting effects, as observed in our study, while the cerebellum might be more relevant in this context. Indeed, given its fundamental connections with frontal cortical networks, the cerebellum might be involved in these activities and support the processing of such information within interconnected brain areas29. Furthermore, it is noteworthy that these findings are consistent with recent evidence demonstrating the engagement of the cerebellum in perceptual processing based on temporal expectations37. This might explain the dissociation between CE and BG patients observed in our study as far as the time orientation effect is concerned.
Our study has several limitations. Firstly, the sample size is rather small, imposing caution when generalizing the results. Indeed, including patients in the acute stroke timeframe is complex due to several factors, primarily the clinical management in this serious stage of the disease. Additionally, the presence of symptoms that could potentially affect the correct execution of tasks (e.g., nausea, vomiting, oculomotion disturbances), as well as anxiety and concern for one’s health, could limit the willingness to participate in clinical studies. Therefore, considering these relevant issues, although limited, our sample describes the immediate functional consequences of damage in these brain regions from a timing function perspective and, to our knowledge, few studies in the literature have explored these aspects within this study model. Moreover, it is important to note that, at present, the limited sample size precludes the possibility of investigating potential functional contributions specific to each hemisphere. For instance, future studies might explore a potential distinct computational allocation between explicit and implicit timing tasks, as suggested by some evidence in the literature5,77. Another significant limitation is that not all patients underwent high-resolution neuroimaging (i.e., brain magnetic resonance imaging, MRI), with some only receiving a Computerised Tomography (CT) scan, which has lower resolution and consequently less precision in locating the damage. However, in these latter cases, patients generally underwent more than one CT scan, allowing for accurate lesion site identification and the exclusion of potential confounding factors related to artifacts. Another aspect to mention is that, unfortunately, due to the aforementioned neuroimaging limitations and the fact that stroke, although focal, rarely respects precise anatomical boundaries, we treated the cerebellum and basal ganglia as unified structures without considering the functional specialization of individual regions within them (e.g., caudate, putamen, cerebellar lobules). However, the consistency of observed alterations within groups allows us to suggest that, while further studies are needed to delve into the specific functional contributions of each region, the overall role played by these subcortical structures appears well-defined and characterized. Another aspect we can only hypothesize is that BG patients, while able to benefit from the regular rhythm to prepare the motor response, may not choose the optimal effector pattern due to damage in the structures that maximize the efficiency of motor output. However, the lack of kinematic analysis prevents a definitive interpretation of their motor pattern efficiency, highlighting the need for further studies. Finally, despite the practice phase and the possibility for breaks and clarifications, many of the included patients, especially older ones, were unfamiliar with using computers, which could have heightened their anxiety and affected their performance. However, the presence of this limitation in both the HC and patient groups, along with the simplicity of the tasks, allows us to consider the potential impact of these difficulties as negligible.
Taken together, our findings in early stroke patients suggest that the cerebellum plays a crucial role in implicit timing, while the basal ganglia appear more relevant in processing explicit temporal information, particularly when time is processed alongside other cognitive functions. These results support previous interpretations in the literature, which propose that the cerebellum is primarily involved in processing temporally salient events, whereas the basal ganglia contribute when time is consciously processed in conjunction with other cognitive functions7,78. This distinction is critical, as it not only confirms prior research highlighting the involvement of these brain regions in temporal tasks but also demonstrates their functional specialization depending on the nature of the task and the associated cognitive demands. By assessing the immediate consequences of damage to these areas, our study demonstrated that the observed deficits were due to the lesions in these regions, excluding the potential compensatory mechanisms that may develop over longer periods. Consistently, prior research on patients with chronic unilateral striatal lesions failed to identify significant deficits in temporal information processing compared to HC, although such studies were often limited by small sample sizes51. It is reasonable that, months after the stroke, the basal ganglia in the unaffected hemisphere compensate for the deficit, masking any alterations caused by damage to specific regions. In contrast, our study model—focused on the early phase before compensatory mechanisms can intervene—significantly reduces this possibility. Indeed, we observed differences compared to HC both in explicit (BG patients) and implicit timing tasks (CE patients). Future longitudinal studies in stroke patients will be fundamental to further explore the distinct contributions of the cerebellum and basal ganglia based on the timing of the injury, a critical factor for a deeper understanding of their complex roles in temporal processing. Based on these findings, our data align with the current literature and confirm that both the cerebellum and basal ganglia are critically involved in processing temporal information.
Materials and methods
Participants
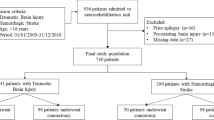
Stroke patients, with brain damages to cerebellum or basal ganglia, were recruited and tested at the Ferrara University Hospital, Ferrara (Italy). Sixteen CE patients (mean level of education = 11.53 years; SD = 4.32; mean age = 65.94 years; SD = 17.32) and twenty BG patients (mean level of education = 11.00 years; SD = 4.58; mean age = 64.17 years; SD = 9.73) were selected. After inspection of MRI and CT scans 4 CE and 2 BG patients were excluded due to the impossibility of reconstructing clear lesion mapping.
The final clinical sample included 12 CE patients (Fig. 6A) and 18 BG patients (Fig. 6B) were included in the study (Table 1). CE patients were tested 7.33 (SD = 3.98) days (range 2–15 days) after stroke, and BG patients were tested 6.22 (SD = 8.49) days (range 2–36) after stroke. Within the CE group 8 had ischemic stroke and 4 hemorrhagic; while within the BG group 10 had ischemic stroke, 5 hemorrhagic and 3 not specified. Individual brain lesions were manually reconstructed from the patients’ brain MRI Fluid Attenuated Inversion Recovery (FLAIR) images (N = 6) or CT scans (N = 24) using ITK-snap software79. A manual segmentation of each brain slice was performed by the authors (ZR, AA, and EMR). All images were reoriented and then normalized into MNI152 space using RegLSM software, running on Matlab80. Lesion overlays are depicted in Fig. 6A and B.
For BG patients, the maximal overlap (7 patients) occurred in the Putamen (MNI coordinates: X = 27, Y= -9, Z = 8). For the CE group, the maximal overlap (5 patients) occurred in Cerebellum 9 (MNI coordinates: X= -15, Y= -48, Z= -43). Brain regions labelling was based on the Automated Anatomical Labeling (AAL) atlas, present in MRIcron application. AAL template indicates the brain area corresponding to specific MNI coordinates.

Manual lesion reconstructions of patients with BG (A) and CE (B) lesions. Different color codes indicate the amount of overlapping lesions, from dark red (no overlap/minimal overlap) to white (maximum overlap). Colors represent the percentage of patients with a lesion at a specific voxel.
For all participants, exclusion criteria included: previous hospitalisations for cerebrovascular events, dementia or severe cognitive impairment evaluated with the Mini-Mental State Examination (MMSE)81, medications known to interfere with cognitive functioning, psychiatric disorders, upper limbs sensory-motor deficits that could affect the proper execution of tasks, or any condition (e.g., drowsiness, aphasia, apraxia) that would interfere with testing. Participants obtained at least a score equal to or greater than 26/30 at the MMSE81. All participants performed an extensive neuropsychological evaluation to investigate their cognitive abilities (Table 1).
All stroke patients included in the study were right-handed82 and were instructed to perform tasks not requiring the use of both hands (see subsequent sections) with their dominant one. The hand used for task completion was unaffected in 58% of patients in the CE group (including two patients with vermian lesions, which are distant from areas involved in distal motor control) and in 61% of those in the BG group. Healthy older adults were volunteers from the local community of Padova (Italy).
Methods
Explicit timing
Finger tapping tasks
Participants were required to tap the spacebar as regularly as possible at the pace they preferred (spontaneous tempo) or at a 1-sec pace (1-sec tempo)83. Both conditions consisted of two experimental blocks separated by a voluntary pause period. The beginning of each block was marked by a white cross on a black background presented at the center of the computer screen. The participants began to tap when they first saw the cross, and they continued until it disappeared, which was after 45 inter-tap intervals in each block for a total of 90 trials in each finger tapping task.
Time bisection task
The experimental session started with the learning phase in which each participant memorised two standard durations: 480 ms (short standard) and 1920 ms (long standard)63. The stimulus used was a dark grey circle on a white background. Both standard durations were presented 10 times in a fixed presentation order. After the learning phase, participants were required to judge the duration of new intervals and determine if they appeared more similar in duration to the short standard or long standard. Participants used their right and left index fingers to respond, and response keys were marked on the keyboard (S = Short and L = Long) after each response, there was a 1000-ms inter-trial interval. Seven comparison durations were used: 480, 720, 960, 1200, 1440, 1680, and 1920 ms. Participants performed two blocks, each duration was presented 6 times in a random order within each block (total of 84 trials). A practice phase was included to familiarise with the task.
Implicit timing
Rhythm task
The rhythm task was a visual adaptation of the auditory rhythm task developed by Cutanda et al. (2015)84. In this version, participants responded to a green target circle (displayed for 100 ms), which was preceded by a sequence of six red circles (each displayed for 100 ms) presented in either regular (fixed inter-stimulus interval (ISI): 550 ms) or irregular rhythms (random ISIs: 150, 350, 550, 750, and 950 ms). In both conditions, the ISI between the final circle in the sequence and the target was 1100 ms (i.e., twice the ISI used in the regular sequence)85,86. Participants were instructed to press the spacebar upon target onset within a maximum response window of 1100 ms. The experiment included 72 randomized trials (regular and irregular), preceded by two practice trials, one for each condition.
Temporal orienting task
We used a shortened version of the go/no-go temporal orienting task as in Correa et al. (2010)87. Participants were instructed to press the “B” key in response to go targets (the letters “O” or “X”, displayed for 100 ms) and to withhold responses for no-go targets (the digit “8”). The onset of the targets was predicted by two temporal cues: either a short red bar (indicating a short foreperiod of 350 ms - early target onset) or a long red bar (indicating a long foreperiod of 1350 ms - late target onset), both displayed for 50 ms. Participants were explicitly encouraged to use these cues to anticipate the target onset. A maximum of 2000 ms was given to respond.
The experiment began with a practice block of 16 trials (8 “early” trials with short-bar cues followed by 8 “late” trials with long-bar cues), with 100% cue validity88. The experimental phase comprised two “early” blocks and two “late” blocks, with 75% cue validity. These blocks were presented alternately and counterbalanced across participants. Each experimental block consisted of 32 trials, 25% of which were no-go trials. Therefore, the composition of the trials within each block was as follows: 18 valid go trials (9 for each foreperiod), 6 valid no-go trials (3 for each foreperiod), 6 invalid go trials (3 for each foreperiod), and 2 invalid no-go trials (1 for each foreperiod).
Neuropsychological Assessment
General cognitive abilities
The MMSE (Italian adaptation81,89 for stroke patients, depending on the age of the patients) is commonly used to evaluate the global cognitive functioning of elderly participants. The items are designed to assess orientation in time and space, attention, calculation, memory, language, and constructional apraxia. The maximum score is 30.
The Frontal Assessment Battery (FAB, Italian adaptation90,91 for stroke patients) is a short cognitive and behavioural six-subtest battery for the bedside screening of global executive dysfunction. It explores specific cognitive or behavioural domains such as conceptualisation, mental flexibility, motor programming, sensitivity to interference, inhibitory control, and environmental autonomy. FAB’s total score ranges from 0 to 18.
Verbal comprehension
The Token test was included to examine auditory comprehension92. The Token test contains 20 plastic token stimuli of two sizes (large and small), two shapes (square/rectangular and round), and five colors. The test has a variable number of sections that increase in sentence length and linguistic complexity (e.g., from “Point to a square” to “Put the small red square on the large blue circle”). Token test total score ranges from 0 to 36.
Memory abilities
The Rey Auditory Verbal Learning Test (RAVLT) consists of five consecutive immediate free-recall trials of 15 words pronounced by the examiner (immediate recall condition) and a recall trial after an interference period of 15 min (delayed recall condition)93,94. Performance is evaluated in terms of accuracy. Specifically, the number of words correctly recalled is calculated. The maximum score for the immediate part is 75 and for the delayed 15.
The Babcock Story Recall Test (BSRT) is a verbal memory measure in which participants are asked to provide immediate and delayed (after 20 min) recall of a brief story read by the examiner92. Performance is evaluated in terms of quantity and accuracy of the reported information. Maximum total score is 16 (8 at the immediate + 8 at the delayed part).
Attention
The Trail-Making Test (TMT, Italian normative data in95) consists of two parts (TMT-A and TMT-B). In Part A, participants are asked to connect 25 numbers in numerical order, whereas in Part B they have to connect 25 encircled numbers and letters in numerical and alphabetical order, alternating between numbers and letters. Part A is generally intended to test visual search and motor speed skills, whereas Part B is supposed to involve higher-level cognitive skills as well, such as mental flexibility. Performance is evaluated in terms of time (seconds) to complete the test accurately. In the present study, we considered the time to complete Part A and Part B.
Executive functions
Phonemic Verbal Fluency Test: The FAS Test (Italian normative data in93) measures phonemic verbal fluency. Participants are asked to orally produce as many words as possible that begin with a given alphabetic letter (letters “F”, “A” and “S”) within a prescribed time interval (60 s per letter), excluding proper names, numbers and words that begin with the same suffix. This task requires executive control over cognitive processes such as selective attention, mental set shifting, internal response generation, and self-monitoring. The performance score is the total number (sum of the words starting with all the requested letters) of correct words pronounced, repetitions excluded.
Visuo-constructional ability and visual memory
The ROCF was included to evaluate visuospatial constructional ability and visual memory96. It consists of two test conditions: Immediate Recall and Delayed Recall. In the first step, subjects are asked to draw the same figure. Subsequently, they are instructed to draw what they remembered.
Procedure
Psychopy97 and E-prime software98 were used to program and run the experiments for both the controls and the stroke patients; we used the paper-pen version of the neuropsychological tests for all participants. During the experimental session, controls were seated at a distance of approximately 60 cm in front of a 15-inch PC monitor screen.
Stroke patients were tested during two experimental sessions that lasted approximately 60 min. We decided to test patients in two separate sessions, one dedicated to computerised timing tasks and one dedicated to neuropsychological evaluation. The patients performed the computer tests in their hospital rooms, appropriately positioned at the bedside with laptop support or at the table (depending on the clinical condition) so that they could perform the tasks comfortably. The assessments were carried out at times that did not interfere with clinical activities to not compromise the performance of the tasks. They were seated at a distance of approximately 60 cm in front of a 15.6-inch PC monitor screen (HP 255 G9 Laptop). The neuropsychological assessments were carried out in rooms on the in-patient ward or in the neuropsychology section to ensure that the patient was alone with the examiner (i.e. experienced neuropsychologists), comfortably seated with a dedicated bed support or at the table in appropriate conditions for the tests to be carried out correctly and without possible sources of disturbances. Healthy older adults were individually tested in person in their own homes in a quiet and normally illuminated room, and all of them received the same instructions. They were seated approximately 60 cm from the computer screen. Healthy participants were tested in one experimental session, timing tasks were performed first, followed by the neuropsychological evaluation. Participants took breaks if necessary. All participants in both the HC and stroke groups underwent computer testing in the same order, specifically free and 1-second finger tapping task, time bisection, rhythmic task, and temporal orienting. Written informed consent was collected from all participants and the study was conducted in accordance with the Helsinki Declaration99. The study was approved by the ethics committee of the Department of General Psychology (n° 4258) and by the Area Vasta Emilia-Romagna Centro Ethics Committee (AVEC, protocol number CEAVEC 1020/2020/Oss/AOUFe).
Statistical analyses
Finger tapping task
Trials with missing or anticipated responses (RT ≤ 100 ms) were excluded from analyses (mean percentage of excluded trials). Trials excluded: Free finger tapping = 2.69% and 1-sec finger tapping = 0.72% of the total number of trials (6210 trials). Post-hoc analyses were performed with a Tukey correction.
For the finger tapping tasks, the mean inter-response interval (IRI) and the coefficient of variation (CV = SD/mean) were calculated for the free and 1-sec finger tapping tasks. The CV was chosen as a measure of variability. One-way ANOVAs were carried out on each task to examine the differences in mean IRI and CV between patients and controls.
Time bisection task
Data from practice trials and trials without a response were rejected from the analysis. The mean percentage of excluded trials was as follows: HC = 4.2% (SD = 5.3%), BG = 4.8% (SD = 4.3), CE = 7.3% (SD = 9.1). Response data were analysed by means of mixed-effects probit regression63 using the lme4 R library100. Specifically, the probability of “long” responses was modelled as a function of interval duration (centered and scaled to improve their interpretation and the fit of the model), Group (three-level factor with HC as reference level), and their interaction. The model also included by-participant correlated random intercepts and slopes for the duration. This model provides information about the between-group differences in the intercept and slope of the psychometric curves. In detail, the simple effects for the BG and CE groups indicate differences compared to the HC group in the probability of saying “Long” at the intermediate duration, which is an index of accuracy. Significant interactions between interval duration and each of the BG and CE groups indicate differences compared to the HC group in the shape (slope) of the psychometric curve, which is an index of precision.
Rhythm task
Data from practice trials, trials with premature responses (i.e., before target onset), and trials with anticipated responses (i.e., RT < 150 ms) were excluded from the analysis. The mean percentage of excluded trials was as follows: HC = 2.8% (SD = 4.1%), BG = 11.6% (SD = 13.5), CE = 14.9% (SD = 17.9). Analyses were performed using a mixed-effects linear regression100 on the inverse-transformed RTs (iRT), computed as -1000/RT101 to control for the impact of positive skewness in the distribution of RTs. The fixed-effects part of the model included the factors Group and Rhythm (irregular vs. regular), along with their interaction. Additionally, we included the centered and scaled trial number to account for potential time-on-task effects, such as learning/adaptation or fatigue102. Unlike our usual analytical approach for the control of autocorrelation in RT63,103, we could not include the response time from the preceding trial due to the need to exclude trials with missing responses at the previous trial, resulting in some patients having less than 30% of analysable trials. The random part of the model also included by-participant correlated random intercepts and slopes for rhythm. Visual inspection of the model residuals was performed to assess normality. Following Baayen and Milin104, trials with absolute standardized residuals higher than 2.5 SD were considered outliers and removed (2% of the trials). After the removal of outlier trials, the model was refitted achieving reasonable closeness to normality. For the model interpretation, the simple effects for BG and CE groups indicate differences compared to the HC group in iRTs in the irregular rhythm condition, which is taken as an index of general response speed. Significant interactions between rhythm and each of the BG and CE groups indicate differences compared to the HC group in the iRT difference between regular and irregular conditions, which is an index of advantage/cost for regular rhythms.
Temporal orienting task
For the temporal orienting task, the analysis focused only on data from go trials, given the limited number of no-go trials in the invalid condition. Data from practice trials, trials with premature responses (i.e., before target onset), trials with anticipated responses (i.e., RT below 150 ms), and trials without a response were rejected from the analysis. The mean percentage of excluded trials was as follows: HC = 4.2% (SD = 2.0%), BG = 8.8% (SD = 5.3%), CE = 15.2% (SD = 25.5%).
Analyses were performed using a mixed-effects linear regression on the iRT. As effects of interest, the fixed-effects part of the model included the factors Group, Cue (late vs. early), and SOA (350 and 1350 ms), along with their interactions. Since this task was divided into blocks, the centered and scaled trial number within a block, the centered and scaled block number, and their interaction were included to account for potential time-on-task effects. The random part of the model included by-participant correlated random intercepts and slopes for Cue, SOA, and their interaction. Since visual inspection of the model residuals showed that they were skewed, trials with absolute standardized residuals higher than 2.5 SD were considered outliers and removed (2% of the trials). After the removal of outlier trials, the model was refitted achieving reasonable closeness to normality. For the model interpretation, significant three-way interactions between Group, SOA, and Cue are an index of between-group differences in temporal orienting effects.
Data availability
The data supporting this study’s findings are available from the corresponding author, AA, and senior authors, GM and MP, upon reasonable request.
References
Tanaka, M., Kameda, M. & Okada, K. Springer International Publishing, Cham, Temporal Information Processing in the Cerebellum and Basal Ganglia. in Neurobiology of Interval Timing (eds. Merchant, H. & de Lafuente, V.) 95–116 (2024). https://doi.org/10.1007/978-3-031-60183-5_6
Buhusi, C. V. & Meck, W. H. What makes us tick? Functional and neural mechanisms of interval timing. Nat. Rev. Neurosci. 6, 755–765 (2005).
Lewis, P. A. & Miall, R. C. Distinct systems for automatic and cognitively controlled time measurement: evidence from neuroimaging. Curr. Opin. Neurobiol. 13, 250–255 (2003).
Mioni, G., Stablum, F. & Grondin, S. Interval discrimination across different duration ranges with a look at spatial compatibility and context effects. Front. Psychol. 5, 717 (2014).
Coull, J. & Nobre, A. Dissociating explicit timing from temporal expectation with fMRI. Curr. Opin. Neurobiol. 18, 137–144 (2008).
Herbst, S. K., Obleser, J. & van Wassenhove, V. Implicit Versus Explicit timing-separate or Shared mechanisms? J. Cogn. Neurosci. 34, 1447–1466 (2022).
Koch, G., Oliveri, M. & Caltagirone, C. Neural networks engaged in milliseconds and seconds time processing: evidence from transcranial magnetic stimulation and patients with cortical or subcortical dysfunction. Philosophical Trans. Royal Soc. B: Biol. Sci. https://doi.org/10.1098/rstb.2009.0018 (2009).
Hass, J. & Durstewitz, D. Neurocomputational models of time perception. Adv. Exp. Med. Biol. 829, 49–71 (2014).
Buonomano, D. V. & Karmarkar, U. R. How do we tell time? Neuroscientist 8, 42–51 (2002).
Mioni, G., Grondin, S., Bardi, L. & Stablum, F. Understanding time perception through non-invasive brain stimulation techniques: a review of studies. Behav. Brain. Res. 377, 112232 (2020).
Zhou, S. & Buonomano, D. V. Neural population clocks: encoding time in dynamic patterns of neural activity. Behav. Neurosci. 136, 374–382 (2022).
Ivry, R. B. & Spencer, R. M. C. The neural representation of time. Curr. Opin. Neurobiol. 14, 225–232 (2004).
Merchant, H., Harrington, D. L. & Meck, W. H. Neural basis of the perception and estimation of time. Annu. Rev. Neurosci. 36, 313–336 (2013).
Breska, A. & Ivry, R. B. Taxonomies of timing: where does the Cerebellum Fit in? Curr. Opin. Behav. Sci. 8, 282–288 (2016).
Spencer, R. M. C. & Ivry, R. B. Cerebellum and timing. in Handbook of the Cerebellum and Cerebellar Disorders (eds Manto, M. U., Gruol, D. L., Schmahmann, J. D., Koibuchi, N. & Sillitoe, R. V.) 1359–1377 (Springer International Publishing, Cham, doi:https://doi.org/10.1007/978-3-030-23810-0_52. (2022).
Livesey, A. C., Wall, M. B. & Smith, A. T. Time perception: manipulation of task difficulty dissociates clock functions from other cognitive demands. Neuropsychologia 45, 321–331 (2007).
Pouthas, V. et al. Neural network involved in time perception: an fMRI study comparing long and short interval estimation. Hum. Brain Mapp. 25, 433–441 (2005).
Bengtsson, S. L., Ehrsson, H. H., Forssberg, H. & Ullén, F. Dissociating brain regions controlling the temporal and ordinal structure of learned movement sequences. Eur. J. Neurosci. 19, 2591–2602 (2004).
Jantzen, K. J., Oullier, O., Marshall, M., Steinberg, F. L. & Kelso, J. a. S. A parametric fMRI investigation of context effects in sensorimotor timing and coordination. Neuropsychologia 45, 673–684 (2007).
Matell, M. S. & Meck, W. H. Cortico-striatal circuits and interval timing: coincidence detection of oscillatory processes. Brain Res. Cogn. Brain Res. 21, 139–170 (2004).
Magalhães, F. et al. Neurochemical changes in basal ganglia affect time perception in parkinsonians. J. Biomed. Sci. 25, 26 (2018).
Miyawaki, E. K. & Review Subjective time perception, dopamine signaling, and Parkinsonian Slowness. Front. Neurol. 13, 927160 (2022).
Mioni, G. et al. Dissociating explicit and implicit timing in Parkinson’s Disease patients: evidence from bisection and Foreperiod tasks. Front. Hum. Neurosci. 12, 17 (2018).
Greenland, J. C., Williams-Gray, C. H. & Barker, R. A. The clinical heterogeneity of Parkinson’s disease and its therapeutic implications. Eur. J. Neurosci. 49, 328–338 (2019).
Mitchell, J. M., Weinstein, D., Vega, T. & Kayser, A. S. Dopamine, time perception, and future time perspective. Psychopharmacol. (Berl). 235, 2783–2793 (2018).
Speranza, L., di Porzio, U., Viggiano, D., de Donato, A. & Volpicelli, F. Dopamine: The Neuromodulator of Long-Term Synaptic Plasticity, Reward and Movement Control. Cells 10, 735 (2021).
Bareš, M. et al. Consensus paper: decoding the contributions of the Cerebellum as a Time Machine. From neurons to clinical applications. Cerebellum 18, 266–286 (2019).
Ohmae, S., Kunimatsu, J. & Tanaka, M. Cerebellar roles in self-timing for sub- and Supra-Second intervals. J. Neurosci. 37, 3511–3522 (2017).
Antonioni, A. et al. The cerebellum and the Mirror Neuron System: a matter of inhibition? From neurophysiological evidence to neuromodulatory implications. A narrative review. Neurosci. Biobehavioral Reviews. 105830 https://doi.org/10.1016/j.neubiorev.2024.105830 (2024).
Ivry, R. B., Spencer, R. M., Zelaznik, H. N. & Diedrichsen, J. The cerebellum and event timing. Ann. N Y Acad. Sci. 978, 302–317 (2002).
Spencer, R. M. C., Zelaznik, H. N., Diedrichsen, J. & Ivry, R. B. Disrupted timing of discontinuous but not continuous movements by cerebellar lesions. Science 300, 1437–1439 (2003).
Nichelli, P., Alway, D. & Grafman, J. Perceptual timing in cerebellar degeneration. Neuropsychologia 34, 863–871 (1996).
Jahanshahi, M., Jones, C. R. G., Dirnberger, G. & Frith, C. D. The substantia nigra pars compacta and temporal processing. J. Neurosci. 26, 12266–12273 (2006).
Pollok, B., Gross, J., Kamp, D. & Schnitzler, A. Evidence for anticipatory motor control within a cerebello-diencephalic-parietal network. J. Cogn. Neurosci. 20, 828–840 (2008).
Sakai, K., Ramnani, N. & Passingham, R. E. Learning of sequences of finger movements and timing: frontal lobe and action-oriented representation. J. Neurophysiol. 88, 2035–2046 (2002).
Breska, A. & Ivry, R. B. Double dissociation of single-interval and rhythmic temporal prediction in cerebellar degeneration and Parkinson’s disease. Proc. Natl. Acad. Sci. U S A. 115, 12283–12288 (2018).
Breska, A. & Ivry, R. B. The human cerebellum is essential for modulating perceptual sensitivity based on temporal expectations. Elife 10, e66743 (2021).
Draganova, R. et al. Neurostructural changes and declining sensorimotor function due to cerebellar cortical degeneration. J. Neurophysiol. 125, 1735–1745 (2021).
Navntoft, C. A. & Dreyer, J. K. How compensation breaks down in Parkinson’s disease: insights from modeling of denervated striatum. Mov. Disord. 31, 280–289 (2016).
Sun, J. et al. Neural compensation in manifest neurodegeneration: systems neuroscience evidence from social cognition in frontotemporal dementia. J. Neurol. 270, 538–547 (2023).
Barone, P. Neurotransmission in Parkinson’s disease: beyond dopamine. Eur. J. Neurol. 17, 364–376 (2010).
Selvadurai, L. P., Harding, I. H. & Corben, L. A. Georgiou-Karistianis, N. Cerebral abnormalities in Friedreich ataxia: a review. Neurosci. Biobehav Rev. 84, 394–406 (2018).
Saini, V., Guada, L. & Yavagal, D. R. Global Epidemiology of Stroke and Access to acute ischemic stroke interventions. Neurology 97, S6–S16 (2021).
Idesis, S. et al. Inferring the dynamical effects of stroke lesions through whole-brain modeling. Neuroimage Clin. 36, 103233 (2022).
Karnath, H. O., Sperber, C. & Rorden, C. Mapping human brain lesions and their functional consequences. Neuroimage 165, 180–189 (2018).
Vaidya, A. R., Pujara, M. S., Petrides, M., Murray, E. A. & Fellows, L. K. Lesion studies in contemporary neuroscience. Trends Cogn. Sci. 23, 653–671 (2019).
Coelho, P., Rodrigues, J. A., Alves, N., Fonseca, A. C. & P. & Time perception changes in stroke patients: a systematic literature review. Front. Neurol. 13, 938367 (2022).
Harrington, D. L., Lee, R. R., Boyd, L. A., Rapcsak, S. Z. & Knight, R. T. Does the representation of time depend on the cerebellum? Effect of cerebellar stroke. Brain 127, 561–574 (2004).
Mole, J., Winegardner, J., Malley, D. & Fish, J. Time perception impairment following thalamic stroke: a case study. Neuropsychol. Rehabil. 28, 208–222 (2018).
Ivry, R. B., Keele, S. W. & Diener, H. C. Dissociation of the lateral and medial cerebellum in movement timing and movement execution. Exp. Brain Res. 73, 167–180 (1988).
Aparicio, P., Diedrichsen, J. & Ivry, R. B. Effects of focal basal ganglia lesions on timing and force control. Brain Cogn. 58, 62–74 (2005).
Visalli, A., Capizzi, M. & Mioni, G. Explicit and implicit timing across the adult lifespan. Psychol. Aging. https://doi.org/10.1037/pag0000866 (2024).
Al-Qazzaz, N. K., Ali, S. H., Ahmad, S. A., Islam, S. & Mohamad, K. Cognitive impairment and memory dysfunction after a stroke diagnosis: a post-stroke memory assessment. Neuropsychiatr Dis. Treat. 10, 1677–1691 (2014).
Tang, E. Y. H., Price, C., Stephan, B. C. M., Robinson, L. & Exley, C. Impact of memory problems post-stroke on patients and their family carers: a qualitative study. Front. Med. 7, (2020).
Craig, A. D. B. Emotional moments across time: a possible neural basis for time perception in the anterior insula. Philos. Trans. R Soc. Lond. B Biol. Sci. 364, 1933–1942 (2009).
Schwartze, M., Keller, P. E., Patel, A. D. & Kotz, S. A. The impact of basal ganglia lesions on sensorimotor synchronization, spontaneous motor tempo, and the detection of tempo changes. Behav. Brain Res. 216, 685–691 (2011).
Bostan, A. C. & Strick, P. L. The basal ganglia and the cerebellum: nodes in an integrated network. Nat. Rev. Neurosci. 19, 338–350 (2018).
Dutke, S. Remembered duration: working memory and the reproduction of intervals. Percept. Psychophys. 67, 1404–1413 (2005).
Grahn, J. A. & Brett, M. Impairment of beat-based rhythm discrimination in Parkinson’s disease. Cortex 45, 54–61 (2009).
Funahashi, S. & Andreau, J. M. Prefrontal cortex and neural mechanisms of executive function. J. Physiol. Paris. 107, 471–482 (2013).
Schwartze, M., Keller, P. E. & Kotz, S. A. Spontaneous, synchronized, and corrective timing behavior in cerebellar lesion patients. Behav. Brain. Res. 312, 285–293 (2016).
Bowler, D. Rey Auditory Verbal Learning Test (Rey AVLT). in Encyclopedia of Autism Spectrum Disorders (ed Volkmar, F. R.) 3976–3980 (Springer International Publishing, Cham, doi:https://doi.org/10.1007/978-3-319-91280-6_539. (2021).
Capizzi, M., Visalli, A., Faralli, A. & Mioni, G. Explicit and implicit timing in older adults: dissociable associations with age and cognitive decline. PLoS One. 17, e0264999 (2022).
Kopec, C. D. & Brody, C. D. Human performance on the temporal bisection task. Brain Cogn. 74, 262–272 (2010).
Lustig, C., Matell, M. S. & Meck, W. H. Not ‘just’ a coincidence: frontal-striatal interactions in working memory and interval timing. Memory 13, 441–448 (2005).
Matthews, W. J. & Meck, W. H. Temporal cognition: connecting subjective time to perception, attention, and memory. Psychol. Bull. 142, 865–907 (2016).
Üstün, S., Kale, E. H. & Çiçek, M. Neural networks for Time Perception and Working Memory. Front. Hum. Neurosci. 11, (2017).
Sanabria, D., Capizzi, M. & Correa, Á. Rhythms that speed you up. J. Exp. Psychol. Hum. Percept. Perform. 37, 236–244 (2011).
Triviño, M., Arnedo, M., Lupiáñez, J., Chirivella, J. & Correa, A. Rhythms can overcome temporal orienting deficit after right frontal damage. Neuropsychologia 49, 3917–3930 (2011).
Späth, M. et al. The role of the basal ganglia and cerebellum in adaptation to others’ speech rate and rhythm: a study of patients with Parkinson’s disease and cerebellar degeneration. Cortex 157, 81–98 (2022).
Del Olmo, M. F., Cheeran, B., Koch, G. & Rothwell, J. C. Role of the Cerebellum in externally paced rhythmic finger movements. J. Neurophysiol. 98, 145–152 (2007).
Song, J., Lin, H. & Liu, S. Basal ganglia network dynamics and function: role of direct, indirect and hyper-direct pathways in action selection. Network: Comput. Neural Syst. 34, 84–121 (2023).
Dhawale, A. K., Wolff, S. B. E., Ko, R. & Ölveczky, B. P. The basal ganglia control the detailed kinematics of learned motor skills. Nat. Neurosci. 24, 1256–1269 (2021).
Terranova, S. et al. Cerebellar Direct Current Stimulation reveals the causal role of the cerebellum in temporal prediction. Cerebellum https://doi.org/10.1007/s12311-023-01649-8 (2023).
Triviño, M., Correa, A., Arnedo, M. & Lupiáñez, J. Temporal orienting deficit after prefrontal damage. Brain 133, 1173–1185 (2010).
Zokaei, N. et al. Temporal orienting in Parkinson’s disease. Eur. J. Neurosci. 53, 2713–2725 (2021).
Wiener, M., Turkeltaub, P. & Coslett, H. B. The image of time: a voxel-wise meta-analysis. NeuroImage 49, 1728–1740 (2010).
Grondin, S. The Perception of Time: Your Questions Answered (Routledge, 2019). https://doi.org/10.4324/9781003001638
Yushkevich, P. A. et al. User-guided segmentation of Multi-modality Medical Imaging datasets with ITK-SNAP. Neuroinformatics 17, 83–102 (2019).
Biesbroek, J. M. et al. Brain Infarct Segmentation and Registration on MRI or CT for lesion-symptom mapping. JoVE 59653 https://doi.org/10.3791/59653 (2019).
Magni, E., Binetti, G., Bianchetti, A., Rozzini, R. & Trabucchi, M. Mini-mental state examination: a normative study in Italian elderly population. Eur. J. Neurol. 3, 198–202 (1996).
Oldfield, R. C. The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia 9, 97–113 (1971).
Perbal, S., Couillet, J., Azouvi, P. & Pouthas, V. Relationships between time estimation, memory, attention, and processing speed in patients with severe traumatic brain injury. Neuropsychologia 41, 1599–1610 (2003).
Cutanda, D., Correa, Á. & Sanabria, D. Auditory temporal preparation induced by rhythmic cues during concurrent auditory working memory tasks. J. Exp. Psychol. Hum. Percept. Perform. 41, 790–797 (2015).
de la Rosa, M. D., Sanabria, D., Capizzi, M. & Correa, A. Temporal Preparation driven by rhythms is resistant to working memory interference. Front. Psychol. 3, 308 (2012).
Lange, K. Can a regular context induce temporal orienting to a target sound? Int. J. Psychophysiol. 78, 231–238 (2010).
Correa, Á., Triviño, M., Pérez-Dueñas, C., Acosta, A. & Lupiáñez, J. Temporal preparation, response inhibition and impulsivity. Brain Cogn. 73, 222–228 (2010).
Capizzi, M., Correa, A. & Sanabria, D. Temporal orienting of attention is interfered by concurrent working memory updating. Neuropsychologia 51, 326–339 (2013).
Measso, G. et al. The mini-mental state examination: normative study of an Italian random sample. Dev. Neuropsychol. 9, 77–85 (1993).
Appollonio, I. et al. The Frontal Assessment Battery (FAB): normative values in an Italian population sample. Neurol. Sci. 26, 108–116 (2005).
Dubois, B., Slachevsky, A., Litvan, I. & Pillon, B. The FAB: a Frontal Assessment Battery at bedside. Neurology 55, 1621–1626 (2000).
Spinnler, H. & Tognoni, G. Standardizzazione E Taratura Italiana di test Neuropsicologici: Gruppo Italiano per lo Studio Neuropsicologico dell’Invecchiamento (Masson Italia Periodici, 1987).
Carlesimo, G. A., Caltagirone, C. & Gainotti, G. The Mental Deterioration Battery: normative data, diagnostic reliability and qualitative analyses of cognitive impairment. The Group for the standardization of the Mental Deterioration Battery. Eur. Neurol. 36, 378–384 (1996).
Rey, A. L’examen psychologique dans les cas d’encéphalopathie traumatique. (Les problems.). [The psychological examination in cases of traumatic encepholopathy. Probl. ] Archives de Psychologie. 28, 215–285 (1941).
Giovagnoli, A. R. et al. Trail making test: normative values from 287 normal adult controls. Ital. J. Neurol. Sci. 17, 305–309 (1996).
Caffarra, P., Vezzadini, G., Dieci, F., Zonato, F. & Venneri, A. Rey-Osterrieth complex figure: normative values in an Italian population sample. Neurol. Sci. 22, 443–447 (2002).
Peirce, J. et al. PsychoPy2: experiments in behavior made easy. Behav. Res. Methods. 51, 195–203 (2019).
Taylor, P. J. & Marsh, J. E. E-Prime (Software). in The International Encyclopedia of Communication Research Methods 1–3 (Wiley, Ltd, doi:https://doi.org/10.1002/9781118901731.iecrm0085. (2017).
General Assembly of the World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. J. Am. Coll. Dent. 81, 14–18 (2014).
Bates, D., Mächler, M., Bolker, B. & Walker, S. Fitting Linear mixed-effects models using lme4. J. Stat. Soft 67, (2015).
Brysbaert, M. & Stevens, M. Power Analysis and effect size in mixed effects models: a Tutorial. J. Cognition. 1, 9 (2018).
Baayen, R. H. & Linke, M. An introduction to the generalized additive model. in Practical Handb. corpus Linguistics 563–591 (2020).
Visalli, A., Capizzi, M., Ambrosini, E., Kopp, B. & Vallesi, A. P3-like signatures of temporal predictions: a computational EEG study. Exp. Brain Res. 241, 1919–1930 (2023).
Baayen, R. H. & Milin, P. Analyzing reaction Times. Int. J. Psychol. Res. 3, 12–28 (2010).
Acknowledgements
We are deeply grateful to all participants. Moreover, we thank Caterina Garuti, Niccolò Cotta Ramusino, Anna Chiara Pelizzari, Francesca Panzacchi, Sara Stefanelli, Veronica Lissandron, and Anna Campion for their help in collecting data. M.C. is supported by a grant (PID2021-128696NA-I00) funded by MICIU/AEI/ 10.13039/501100011033 and ERDF/EU. She also acknowledges the support of a María Zambrano Fellowship at the University of Granada from the Spanish Ministry of Universities and the European Union NextGeneration.
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
AA conceptualized the study; AA, EMR, MC, and GM cured the Data; AA, EMR, MC, ZR, AV, and GM analyzed the Data; AA, EMR, AG, PA, EC, MC, and GM were responsible for the Investigation; MC, GM, and MP cured the methodology; MC, ZR, AV, and GM was responsible for the Resource and Software; MC, DG, GM, and MP supervised the work; AA, EMR, MC, and GM wrote the original manuscript; all the authors reviewed and edited the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Written informed consent was collected from all participants, and the study was conducted in accordance with the Helsinki Declaration. The study was approved by the ethics committee of the Department of General Psychology (n° 4258) and by the Area Vasta Emilia-Romagna Centro Ethics Committee (AVEC, protocol number CEAVEC 1020/2020/Oss/AOUFe).
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Antonioni, A., Raho, E.M., Capizzi, M. et al. Time perception in cerebellar and basal ganglia stroke patients. Sci Rep 15, 4948 (2025). https://doi.org/10.1038/s41598-025-89311-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-89311-7
