
Abstract
Bottled water consumption has increased in recent decade due to many reasons, especially significant decline in water quality and quantity. The concentration of fluoride and nitrate in bottled waters may vary based on brands and locations. This study was carried out to determine the levels of fluoride and nitrate in bottled waters consumed in Kermanshah city and assess the related non -carcinogenic risks. Totally, 22 brands of bottled water were collected from markets. Fluoride and nitrate measurement was conducted via a UV-visible spectrophotometer (DR-5000). From the results, Fluoride and nitrate levels in the studied bottled waters were 0.32 ± 0.18 mg/L and 2.3 ± 1.41 mg/L, respectively. The risk of non-carcinogenic in term of HQ for fluoride exposure, for only 2 brands of bottled water were > 1 for infants group. HQ was less than 1 for nitrate in all the brands for all the age groups revealed non-carcinogen risks. Hazard index (HI) calculation showed that only in 2 brands of bottled water HI was > 1 for infants group. The HI were as infants (0.64) > children (0.36) > teenagers (0.27) > adults (0.24). From Monte Carlo simulation, 95th Percentile for nitrate and fluoride was less than 1 for all the groups. This result indicated non-carcinogenic risks of nitrate and fluoride for 95% of the studied groups. Moreover, sensitivity analysis showered that concentration for both nitrate and fluoride had the highest effect on HQ for all the groups. From this work, although fluoride and nitrate content in the bottled waters were at standard range, but infants were proportionally at higher risk.
Similar content being viewed by others


Introduction
Safe water is defined as water free of any pollutants (chemical, biological and radioactive agents), and with no adverse health effects through long-term consumption. Accordingly, adequate, safe, and accessible drinking water must be supplied for all. Many pollutants, including inorganic, organics and heavy metals may exist in waters and induce human risks1.Through some environmental control measures water quality can preserved from the source2. Among the various inorganics considered in drinking water quality, fluoride and nitrate are of noticeable elements due to their assigned adverse human health effects.
Fluoride is an essential element for human at recommended values. It can effectively reduces dental caries without harmful effects at allowable levels, but, at extra levels it can cause serious dental and sclerosis disorders3. Fluoride also may cause adverse effects on brain, decrease intelligence quotient (IQ) and increase blood hypertension4,5. However world health organization recommended a guideline vale of 0.5–1.5 of fluoride in drinking waters3.
Fluoride may occur naturally in waters or it may be added to drinking water in controlled amounts in some areas. Fluoride can be found in drinking waters, foods6,7,8,9,10,11. Ingestion is considered as the main source of intake through drinking12. Many studies have reported different levels of fluoride in drinking waters and the related health effects around the world. In some regions, fluoride content has been reported as high as 2800 mg/L and consequent related obvious skeletal fluorosis13,14,15,16,17,18,19,20,21,22. Such waters should be defluoridated using proper methods23,24.
Nitrate is also a harmful compound that can enter the body through water consumption. Although other sources of nitrate exposure are considered but drinking, water is mainly considered for different groups of population. Nitrate through a process can disorder in blood red cell function and produce methhemoglobinemia (metHb) and resulting in blue baby especially in children3. Other adverse possible risks related to nitrate intake have been reported in some parts due to elevated nitrate intake especially through drinking waters25. Nitrate in drinking water can cause many problems, while some cancers are also possible3,26.
In recent decade, bottled water consumption has dramatically increased worldwide due to many reasons. Bottled water has been considered as the main source of drinking water supply in some arid and semiarid countries. Bottled water consumption has attracted due to better taste and higher clearness. It is estimated that global growth rate of bottled water consumption is about 7%. About 89 billion liter bottled drinking water consumed in 2006 27. Although the main consumers are currently European, consumption rates have also increased in Asia, and the Pacific is increasing faster, by approximately 15% 28. In areas where drinking water of good quality is not available and water purification facilities are not available, the probability of bottled water use is higher. Meanwhile, the United States and European countries account for more than 35% of the world’s bottled water market (14). This amount of bottled water can cause problems if there is no monitoring of their quality and the amount of some substances in them is higher. Safe drinking water supply is the primary and essential community public health concern. For this, water quality assessment is usual and necessary. Accordingly, many studies have been conducted to investigate the quality of drinking waters. In various studies, biological factors, micro plastics and chemical have been investigated29,30,31,32. Different works have also been performed for nitrate and fluoride content in bottled waters different areas mainly in standard range8,33,34,35,36,37,38,39. As bottled water are different origins and sources and may some treatment processes may be conducted on them so their quality may differ from one brand to another bottled treated drinking waters and mineral bottled water are in some places are categorized and sold with different qualities.
Human health risk assessment (HRA) serves as a key tool in public health management and can help enhance the quality of life and public health. HRA is a helpful methodology used to estimate the possible and elevated of adverse effects caused by hazardous parameters in human health. Furthermore, HRA contain the scientific experiments and assessment of data12,40. In addition, HRA has been widely employed in many studies to evaluate health risk of various agents and bottled waters quality and possible health risks29,30,34,36,37,38,41,42,43.
Bottled water consumption has increased in Kermanshah city in recent years. In public meeting and large ceremonies, people mainly used bottled water. In some parts of the city people regularly used bottled water due to low water quality, lack of water and other health reasons. Regarding the importance of drinking water quality monitoring is necessary as an important way for receiving fluoride and nitrate, evaluation of fluoride content in water resources. Accordingly, this study was conducted to evaluate fluoride and nitrate content is bottled waters consumed in Kermanshah and assesses the related risk health among various age groups (namely; children, teenagers, and adults).
Materials and methods
Samples collection and study area
Kermanshah city is located in west of Iran (Fig. 1), with a population of about 1,000,000 people and in mountainous area. The main sources of water supply are ground waters and dam reservoirs. Nevertheless, in last decades with an increase in city development the water demand has increased due to some reasons. The summers are nearly warm with annual precipitation of 456.8 mm and average temperature of 14 oC. In this work 22 brands of mostly consumed bottled water, (treated bottled water, and minerals bottled water), were collected from the main markets throughout the city. The samples were collected in triplicate for accurate results. The samples were analyzed for fluoride and nitrate content and the averages of the measurements were reported and used for HRA.
The samples were measured for both fluoride and nitrate using spectrophotometric methods as follows. Nitrate concentration was determined via DR 5000 spectrophotometer (Hach, Germany) at wavelengths of 220 nm. To remove the possibility of interference of organic substances in the method, a correction was made at wavelength of 275 nm according to standard methods44. In addition, HCl (1 N) used to remove the interference of alkalinity in the samples. SPANDS method was used to determine fluoride level in the samples at 507 nm using DR 5000 spectrophotometer44. The results of fluoride and nitrate concentration were illustrated using Microsoft Excel.

Kermanshah city location in Iran.
Health risk assessment
Concerns relating to drinking water contaminated with fluoride and nitrate is increasing in Iranian pupation due to elevated public awareness. HRA is a known method to assess the possible adverse effects on human health over a specific period of time [33]. Due to different physiological functions of the population, the target groups were categorized into 4 age groups. In this study HRA used as a scientific and useful method to document and answer the public concerns. For this, HRA was performed for 4 groups of the different exposed people, namely infants (< 2 years), children (> 2 and < 6 years), adolescents (> 6 and < 16 years) and adults (> 16 years)45,46. The daily consumption of nitrate and fluoride were calculated following Eqs. 29.
The reference dose (RfD) for an individual contaminant is expressed in mg/kg of body weight (BW) per day. RfD is an important factor in HRA. In present work, RfD value for nitrate and fluoride were 1.6 (mg/kg/day) and 0.06, respectively48. The parameters definitions, unit, and values for HQ calculation for different groups are shown in Table 1.
From the table (Table 1), EDI is daily intake of nitrate and fluoride (mg/kg), C is nitrate and fluoride concentration in potable bottled water (mg/L), IR is the daily consumption of drinking water, EF is exposure frequency, AT is average exposure time and BW is body weight (kg) for each exposed group.
Monte Carlo simulation and sensitivity analysis
Monte Carlo Simulation as a known computer-driven approach, applies repeatedly random sampling and analytical methods to obtain a probabilistic estimation for calculating outcome models49. Generally, risk assessments contain some levels of uncertainties needs to be considered to obtain consequent risk management action48,49. The Monte Carlo Simulation method combines an extensive array of model and parameter assumptions to predict the overall probability distribution of exposure variables, moving beyond mere upper-bound single-point estimates or specific values. This approach results in a robust risk distribution outcome49.
To minimize the uncertainty level, Monte Carlo simulation has been used to achieve an acceptable risk assessment. Therefore, wide variety of variables is commonly applied in place of a single-point value thereby allowing the estimation process to be conducted with multiple levels of reliability49.
Nitrate and fluoride contents (C), duration of exposure(ED), body weight (BW), and intake rate (IR) were applied to calculate the potential distribution or uncertainty50. For this, a large range of the values with a large random trails (10000) were applied for a range of confidence (1 to 99%)50. Thus, the modifications in incidence rates within this study were taken into account for each population, which helps to reduce uncertainty and enhance the accuracy of health risk outcomes.
These probability distributions are used as the input distributions for exposure model parameters. During a single trial, values are randomly selected from the defined possibilities (the range and shape of the distribution) for each uncertain variable and then the output of the model is calculated49. If a simulation run for 10,000 trials 10, 000 forecasts (or possible outcomes) are created compared to the single outcome obtained in the deterministic approach50,51. The probability distribution resulted from exposure to each compound is subsequently utilized to assess the Hazard Quotient (HQ) and consequently hazard index (HI) values.
Sensitivity analysis
Sensitivity analysis is commonly performed to determine which variable significantly affects the results of risk assessment. In other words, Sensitivity analysis examines how variations in the input variables of a mathematical model influence the outputs, finally establishing a relationship between input parameters and output variations49.In this study, Crystal Ball (version 11.1.2.4, Oracle, Inc., USA) for Monte Carlo simulation and sensitivity analysis via 10,000 repetition46,50,51. The parameters for sensitivity analysis as applied for the Monte Carlo Simulation are outlined in Table 1 the probability distribution for functions applied in the Monte Carlo simulation and sensitivity analysis were acquired as applied in other works46,51,52.
Hazard index
The Hazard Index (HI) is applied by the Environmental Protection Agency (EPA), particularly within the Superfund program, to assess health risks addition linked to mixture of component and as a screening-level check for potential health risks53,54. The HI is determined by adding hazard quotients (HQs) for the individual component in the mixture50,55. A HQ is the ratio of a chemicals exposure level to related reference dose, Eq. 1.
In this work, health risk effects related to sum of nitrate and fluoride hazard was calculated in term of HI for four age groups, namely infants, children, teenagers, and adults using Eq. (3) 54.
Results and discussion
Fluoride content
As shown in Table 2, fluoride concentrations ranged from 0.01 mg/L to 0.71 mg/L (0.32 ± 0.18). According to the results shown in Fig. 2, the maximum concentrations of fluoride were assigned to B3 and B15. Generally, 3 out of the 22 brands were within the standard range recommend by WHO (0.5–1.5 mg/L) and about 86% of the samples are less than minimum value (0.5 mg/L) suggested by WHO. 8 samples have not labeled the fluoride concentration although the measured fluoride content is lower than standards. More inspection and control on the labeled list values are important by official organization for further assessment. 8 of the collected samples were mineral waters (MW) and 16 samples were drinking bottled water (DW). MW are mainly take from ground waters (e.g. springs) and bottled without further purification. However, drinking waters are treated water via purifications methods. Many other works conducted on bottled water quality for fluoride reveled the same levels of fluoride31,32,35,36,51,57,58. Nevertheless, the levels for fluoride in non-bottled waters are varies in, higher levels than WHO guideline, up to 10 mg/L, have also been reported in Iran59,60.
Fluoride health risk assessment
Health risk assessment (HRA) of fluoride in bottled waters consumed in Kermanshah was assessed using HQ as a non-carcinogenic risk approach. Levels of fluoride exposure were calculated for the four group categories. The average of EDI values for infants, children, teenagers and adults are 0.03 (mg/kg.day), 0.02(mg/kg.day), 0.01 (mg/kg.day), and 0.01 (mg/kg.day), respectively.
From the results, infants and children showed higher level of EDI compared to teenagers and adults. Therefore, these groups are supposed to be at higher risk. The same finding was previously reported54.
From USEPA, exposure of children to fluoride at values of higher than reference dose (0.06 mg/kg.bw day) may cause dental fluorosis48. From the results, two brands (B3 and B15) can cause higher EDI than 0.06 and increase the risk of dental fluorosis in infants. It has been reported that, at estimated exposure dose of 0.3 mg F kg − 1 bw the reveled primarily health signs61. In this work, none of the target groups exposed this value. The hazard quotient (HQ) for fluoride exposure was calculated for four age groups. The HQ values beyond 1 signify that the population in the studied area is exposed to higher risk levels of developing non-carcinogenic disorders. As shown in Table 2, HQ values related to 2 brands (B3 and B15) were higher than 1 for infants. HQ assigned to other brands for all groups were less than 1, such the values less than 1 are not of potential concern. The HRA of fluoride for exposed target groups was ordered as infants > Children > Teenagers > Adults. Based on the obtained data, infants and children are more likely to suffer from adverse health effects associated with the consumption of fluoride-content water. In an high consistency, it has been reported that children risk to fluoride exposure id higher in children group62. It has been clarified that Infants and children with lower body weight is the main affecting factor for this as previously mentioned for Fluoride29,62,63. Based on the calculated HQs the result of present work showed that, the risk of dental fluorosis for the all the age groups are not considerable. It should be noticed that the results are based on bottled water consumption, but overall, as the fluoride intake is happened through other main sources like distribution drinking water sources, foods, beverages, tea meat and fluoride supplements so on the cumulative risk can be higher and the risk can increase the risk. Importantly, the acceptable level of fluoride in drinking water should be mentioned with including other intake sources.
Nitrate content
As shown in Table 2, Nitrate concentrations ranged from 0 to 5 mg/L (2.3 ± 1.14). According to the results shown in Fig. 2, the maximum concentration of nitrate was assigned to B5. None of the samples exceeded the guideline value recommend by WHO (45 mg/L). 3 samples have not labeled the nitrate content although the measured nitrate content is lower than WHO guideline and Iranian standard (50 mg/L). through the studies review, it has been reported that nitrate content was higher than that labeled in many cases, and not in many cases not labeled in Iranian bottled water64.More inspection and control on the labeled list values are necessary by officials for further assessment. As mentioned previously, 8 of the collected samples were mineral waters (MW) and 16 samples were drinking bottled water (DW). The mineral water are mainly take from ground waters (e.g. springs) and put in a bottle without further purification. Nevertheless, drinking bottled waters are treated via purifications methods. As the main sources of water and purification process are not clarified by the factories, it is difficult to speak about the efficiencies and possible default through the water processing. Many other works conducted on bottled water quality for nitrate reveled the levels less than Iranian standard of nitrate in many samples33,34,38,39,51,65. However, the ranges for nitrate contents in non-bottled waters vary with high levels26,64.
Nitrate health risk assessment
Health risk assessment (HRA) of nitrate in bottled waters consumed in Kermanshah was assessed using HQ as a non-carcinogenic risk approach. Levels of nitrate exposure were calculated for the four categories. The average of EDI values for infants, children, teenagers and adults ere 0.21 (mg/kg.day), 012(mg/kg.day), 0.09 (mg/kg.day), and 0.08 (mg/kg.day), respectively.
From the results, infants and children showed higher level of EDI compared to teenagers and adults. Therefore, these groups are supposed to be at higher risk. However, this vales compare to other sources intake is low. For instance, Rezaei et al., reported higher EDI (1.14 mg/kg.day) for children than adults in water distribution30. Qasemi et al., reveled the same order (infants > children > adults)54.
The hazard quotient (HQ) for nitrate exposure was calculated for four age groups. The HQ values exceed 1 clarify that the exposed groups to higher health risk levels of non-carcinogenic effects. Table 3 presents the results of HQ related to Fluoride, nitrate for different age groups. From the results, the average of HQ values for infants, children, teenagers, and adults ere 0.13, 0.07, 0.06, and 0.05, respectively. From this study, HQ values related to nitrate were not higher than 1 for the groups. Generally the HRA of nitrate for exposed target groups was ordered as infants > Children > Teenagers > Adults for the collected samples. Although HQ for all the group ages is less than 1 (HQ < 1) indicates that no adverse health effects. From the results, infants and children revealed higher HQ compared to teenagers and adults. Therefore, these groups (infants and children) are comparably at higher risk. However, HQ values compare to other sources intake are low. For instance, Rezaei et al., revealed mean of HQ for infants > children > teenagers > adults in public water distribution30. Based on the obtained data, infants and children are more likely to suffer from adverse health effects associated with the consumption of nitrate-content water It has been clarified that Infants and children with lower body weight is the main affecting factor for this as previously mentioned for nitrate reference29,51,62,63.
As noted previously it should be mentioned that the results are from bottled water consumption, but as the nitrate is ingested from other main source like public water distribution systems, wells, beverages and so on, the cumulative related health risk could be higher.

Fluoride and nitrate concentration in different bottled water brands.
Hazard index (HI)
Hazard Index is used for sum of non- carcinogenic risk quotients of fluoride and nitrate. The HI values are presented in Fig. 3. HI ranges for infants, children, teenagers and adults varied from 0.08 to 1.25 (mean 0.64), 0.04 to 0.69 (mean 0.36), 0.03 to 0.53 (mean 0.27), and 0.03 to 0.46 (mean 0.24), respectively. From the finding (Figs. 3), 2 brands, namely, B3 and B15, exceed revealed HI > 1 for infants. For the other groups, HI values are less than 1, revealed no added risk related to sum of fluoride and nitrate non carcinogen risk for the studied bottled waters. In a comparison, HI values for all groups and the brands are as infants > children > teenagers > adults. Qasemi et, al. showed, HI for groundwater in 3.3%, 100%, and 100% of studied samples were more than 1 (HI > 1) for adults, children and infants, respectively, indicated non-carcinogen risks in infants, children, and adults through drinking water in most of the samples54. It has been reported that HI for sum fluoride and nitrate ranged from 0.02 to 7.66 (average of 2.96) in children and from 0.01 to 5.67 (average 2.19) in adults. Therefore, children were at higher risk compare to other groups66. Golaki et al. also reported the highest HI value for Kazerun children intaking nitrate, nitrite and fluoride from drinking water56.

Hazard index value related to fluoride and nitrate concentration calculated for different bottled water brands and groups.
Monte Carlo simulation and sensitivity analysis
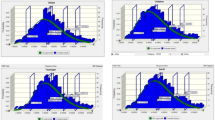
The Monte Carlo approach was applied to calculate uncertainties during risk assessment. Beside Monte Carlo simulations, other uncertainties were addressed especially the parameters that revealed by the sensitivity analysis. Fluoride concentration in samples collected from drinking bottled water in Kermanshah. To increase the validity of measurements, the experiments were conducted three times. Besides the application of single point estimation (calculated through Eqs. (1) and (2)), in this work, Monte Carlo simulation with 10,000 trials was conducted using Oracle Crystal Ball software to estimate the variance of HQ values. For this, the likelihood-based approach was utilized to evaluate nitrate and fluoride levels in the exposed groups. This method try to correct distribution of variables such as nitrate and fluoride concentration, ingestion rate (IR), and body weight (BW). The applicable values for infants, children, teenagers, and adults are presented in Table 1. The results are presented on the histograms in Fig. 4(a, b, c, and d). From the Fig. 4(a, b, c, and d), the fluoride-HQ values for the 95th percentile in infants, children, teenagers, and adults were 0.18, 0.1, 0.08, and 0.07 respectively. Although the values are significantly lower than 1, but comparatively, This amount is higher in infants than other groups, indicating that this age group is exposed to non-carcinogenic risks relating to nitrate, which is likely because of comparably less weight of his group46,67. In addition, histograms for simulating HQ results of nitrate in four exposed groups are displayed in Fig. 5(a, b, c, and d). According to Fig. 5, nitrate HQ for the 95th percentile in infant, children, teenager and adult age groups were 0.04, 0.02, 0.02 and 0.02, respectively, which indicates a non-carcinogenic risk for these groups. The highest 95th percentile of the calculated nitrate HQ was 0.04 for infants, compare to other groups. These results showed that HQ for nitrate for all groups are significantly lower than risk limit value (QH < 1) indicating negligible risk of developing non-carcinogenic effects, for the studies groups.

HQ value related to fluoride concentration calculated for different groups (a: infants, b: children, c: teenagers, c: adults).

HQ value related to nitrate calculated for different groups (a: infants, b: children, c: teenagers, c: adults).
Sensitivity analysis
Sensitivity analysis was carried out to pinpoint the most effective variables in HRA for the exposed groups to show uncertainty of the output response29,62. The results of sensitivity analysis for non-carcinogenic risk assessment in the different age groups (infants, children, teenagers, and adults) are depicted as pie charts in Fig. 6 (a, b, c, and d) for fluoride. For all the groups, among the influencing parameters (i.e. drinking water intake rate (IR), fluoride concentration (C), and exposure frequency (EF)), Fluoride concentration (C-F) showed the highest role for all the groups. Accordingly, the values of IR were 94.1%, 93.5%, 93.9%, and 93.8% for infants, children, teenagers, and adults respectively. These findings showed that fluoride concentration (C-fluoride) has a substantial impact on risk estimates for the four exposed groups. Moreover, compared to other variables, bw and IR have a less impact (≤ 3% for each variable) on the risk for exposure to fluoride for each group. Bazeli et al., Badeenezhad et al. and Revani et al. analysis showed the same finding for the crucial effect of fluoride concentration for same groups exposed46,51 while Ghahramani et al. revealed more effective role of IR than other factors for all the studied groups29,50.
The results of sensitivity analysis for non-carcinogenic risk assessment in the different age groups (infants, children, teenagers, and adults) are depicted as pie charts in Fig. 7 (a, b, c, and d) for nitrate. For all the groups, among the influencing parameters (i.e. drinking water intake rate (IR), fluoride concentration (C), and exposure frequency (EF)), Fluoride concentration (C-F) showed the highest role for all the groups. Accordingly, the values of IR were 94.6%, 94.8%, 94.4%, and 93.9% for infants, children, teenagers, and adults, respectively. These results showed that nitrate concentration (C-nitrate) has the most influence on risk estimates for all the exposed groups. In addition, compared to other factors, bw and IR have a less impact (≤ 3.2% for each variable) on the risk for exposure to nitrate for each group. Bazeli et al. and Badeenezhad et al. showed the same finding for the crucial effect of nitrate concentration for same groups exposed46,50. Therefore, the most crucial factor in the non-cancerous health risk due to nitrate and fluoride was ions content in bottled water. Therefore, reducing the concentration of nitrate and fluoride can lower the possibility of health risks.

Sensitivity analysis of fluoride exposure for different 4 groups (a: infants, b: children, c: teenagers, d: adults).

Sensitivity analysis of nitrate exposure for 4 different groups (a: infants, b: children, c: teenagers, d: adults).
Conclusion
This study aimed to investigate nitrate and fluoride content in bottled water consumed in Kermanshah city and evaluate related health risks. In this study, fluoride and nitrate concentrations of all analyzed bottled waters were less than maximum WHO guideline and national Iranian standards. Among the different studied age groups, infants were proportionally at higher risk to health effects for both fluoride and nitrate exposure through bottled water. Although the risk of non-carcinogenic hazard in term of HQ was mostly less than 1 for fluoride exposure, the HQ values for only 2 brands of the bottled water were > 1 for infants group. In other hand, HQ was less than 1 for nitrate in all the age groups revealed non-carcinogen risks. However, the calculation of the HI, as an indication of sum effects of the two studied ions on the studied age groups, revealed that infants were proportionally at the higher risk compare to other groups. Estimated HI values for only 2 brands of bottled water were > 1 for infants group. Through Monte Carlo simulation showed that 95th Percentile for nitrate and fluoride exposure was less than 1 for all age groups, indicating a non-carcinogenic risk of nitrate and fluoride for 95% of the studied groups. Moreover, sensitivity analysis showered that concentration of fluoride and nitrate had the highest effect on HQ than other variables for all the groups. Finally, considering the other foods and beverages containing fluoride and nitrate can help the better estimating the risks and hazard index. However, continue monitoring of fluoride and nitrate levels in drinking waters should be conducted as possible preventive measures.
Data availability
All data has been provided in the manuscript.
References
Cai, S., Zeng, B. & Li, C. Potential health risk assessment of metals in the muscle of seven wild fish species from the Wujiangdu reservoir, China. Qual. Assur. Saf. Crops Foods. 15, 73–83 (2023).
Xiao-Mei, H., Jin, Y., Chao, L., Xiao-Jun, F. & Yuan, Z. Impact of watershed habitat quality based on land use: a case study of taking Ciyao River Basin. Qual. Assur. Saf. Crops Foods. 15, 18–31 (2023).
WHO Guidelines for drinking-water quality. WHO Chron. 38, 104–108 (2011).
Veneri, F. et al. Fluoride exposure and cognitive neurodevelopment: systematic review and dose-response meta-analysis. Environ. Res. 115239 (2023).
Davoudi, M. et al. Relationship of fluoride in drinking water with blood pressure and essential hypertension prevalence: a systematic review and meta-analysis. Int. Arch. Occup. Environ. Health. 94, 1137–1146 (2021).
Mahvi, A. H., Zazoli, M. A., Younecian, M., Nicpour, B. & Babapour, A. Survey of fluoride concentration in drinking water sources and prevalence of DMFT in the 12 years old students in Behshar City. J. Med. Sci. 6, 658–661 (2006).
Zazouli, M. A. & Mahvi, A. H. Assessment of fluoride content in several brands of Iranian teas (Camellia sinensis) and Tea Liquor. Toxicol. Lett. 180 (Supplement), S207–S208 (2008).
Dobaradaran, S., Mahvi, A. H. & Dehdashti, S. Fluoride content of bottled drinking water available in Iran. Fluoride 41, 93 (2008).
Mahvi, A. H., Zazoli, M. A., Younecian, M. & Esfandiari, Y. Fluoride content of Iranian black tea and tea liquor. Fluoride 39, 266 (2006).
Nouri, J., Mahvi, A. H., Babaei, A. & Ahmadpour, E. Regional pattern distribution of groundwater fluoride in the Shush aquifer of Khuzestan County, Iran. Fluoride 39, 321 (2006).
Dobaradaran, S., Fazelinia, F., Mahvi, A. H. & Hosseini, S. S. Particulate airborne fluoride from an aluminium production plant in Arak, Iran. Fluoride 42, 228 (2009).
Emergency, U. & Response, R. Risk Assessment Guidance for Superfund (Office of Emergency and Remedial Response, US Environmental Protection Agency, 1989).
Bo, Z. et al. Distribution and Risk Assessment of Fluoride in drinking Water in the West Plain Region of Jilin Province, China. Environ. Geochem. Health. 25, 421–431 (2003).
Wang, S. X. et al. Arsenic and fluoride exposure in drinking water: children’s IQ and growth in Shanyin County, Shanxi Province, China. Environ. Health Perspect. 115, 643 (2007).
Reimann, C. et al. Drinking water quality in the Ethiopian section of the East African Rift Valley I—data and health aspects. Sci. Total Environ. 311, 65–80 (2003).
Moturi, W., Tole, M. & Davies, T. The contribution of drinking Water towards Dental Fluorosis: a case study of Njoro Division, Nakuru District, Kenya. Environ. Geochem. Health. 24, 123–130 (2002).
Wondwossen, F., Åstrøm, A. N., Bjorvatn, K. & Bårdsen, A. The relationship between dental caries and dental fluorosis in areas with moderate- and high-fluoride drinking water in Ethiopia. Commun. Dent. Oral Epidemiol. 32, 337–344 (2004).
Suthar, S. et al. Fluoride contamination in drinking water in rural habitations of Northern Rajasthan, India. Environ. Monit. Assess. 145, 1–6 (2008).
Awadia, A., Birkeland, J., Haugejorden, O. & Bjorvatn, K. Caries experience and caries predictors – a study of Tanzanian children consuming drinking water with different fluoride concentrations. Clin. Oral Invest. 6, 98–103 (2002).
Dobaradaran, S., Mahvi, A. H. & Dehdashti, S. Ranjbar Vakil Abadi, D. drinking water fluoride and child dental caries in Dashtestan. Iran. Fluoride. 41, 220–226 (2008).
Rahmani, A., Rahmani, K., Mahvi, A. H. & Usefie, M. Drinking water fluoride and child dental caries in Noorabademamasani, Iran. Fluoride 43, 187 (2010).
Fawell, J. et al. Fluoride in Drinking-Water (World Health Organization (WHO), IWA Publishing, 2006).
Kamarehie, B. et al. Data on the fluoride adsorption from aqueous solutions by metal-organic frameworks (ZIF-8 and Uio-66). Data Brief. 20, 799–804 (2018).
Jafari, A., Mahvi, A. H., Godini, H., Rezaee, R. & Hosseini, S. S. Process optimization for fluoride removal from water by moringa oleifera seed extract. Fluoride 47, 152–160 (2014).
Ward, M. H. et al. Drinking water nitrate and human health: an updated review. Int. J. Environ. Res. Public Health. 15, 1557 (2018).
Essien, E. E. et al. Drinking-water nitrate and cancer risk: a systematic review and meta-analysis. Arch. Environ. Occup. Health. 77, 51–67 (2022).
Wilk, R. Bottled water: the pure commodity in the age of branding. J. Consumer Cult. 6, 303–325 (2006).
Ferrier, C. Bottled water: understanding a social phenomenon. AMBIO: J. Hum. Environ. 30, 118–119 (2001).
Ghahramani, E. et al. Fluoride content in drinking water of the rural areas of Divandarreh City, Kurdistan Province, Iran: a non-carcinogenic risk assessment. Int. J. Environ. Anal. Chem. 103, 341–353 (2023).
Rezaei, H. et al. Health-risk assessment related to the fluoride, nitrate, and Nitrite in the drinking water in the Sanandaj, Kurdistan County, Iran. Hum. Ecol. risk Assessment: Int. J. 25, 1242–1250 (2019).
Yari, K., Leili, M., Zolghadrnasab, H., Mohammadi Bolban, S. & Rahmani, S. The assessment of physical, chemical and microbial quality of bottled water in Hamadan, Iran in 2016. J. Sabzevar Univ. Med. Sci. 27, 93–100 (2020).
Shams, M., Qasemi, M., Afsharnia, M., Mohammadzadeh, A. & Zarei, A. Chemical and microbial quality of bottled drinking water in Gonabad City, Iran: Effect of time and storage conditions on microbial quality of bottled waters. MethodsX 6, 273–277 (2019).
Amouei, A. et al. Nitrate and nitrite in available Bottled Water in Babol (Mazandaran Iran) in summer 2010. J. Babol Univ. Med. Sci. 14, 64–70 (2011).
Akbari, H. et al. Data on investigating the nitrate concentration levels and quality of bottled water in Torbat-e Heydarieh, Khorasan Razavi province, Iran. Data Brief. 20, 463–467 (2018).
Heidariyeh, A. et al. Concentration of Nitrate, Nitrite and Fluoride in Drinking Water and Bottled Water in Semnan City. (2019).
Alimohammadi, M. et al. Data on assessing fluoride risk in bottled waters in Iran. Data Brief. 20, 825–830 (2018).
Fard, R., Daraii, H., Mirzaei, N., Ghahramani, E. & Jafari, A. Evaluation of fluoride content in Sanandaj bottled water, Iran. Fluoride 45 (2012).
Alimohammadi, M. et al. Determination of nitrate concentration and its risk assessment in bottled water in Iran. Data Brief. 19, 2133–2138 (2018).
Jahed, K. G. R., Mahdavi, M., Ghasri, A. & Saeidnia, S. Investigation of Nitrate Concentrations in Some Bottled Water Available in Tehran. (2008).
Järup, L., Elinder, C. G., Berglund, M. & Organization, W. H. (World Health Organization, (2001).
Naseri, M., Vazirzadeh, A., Kazemi, R. & Zaheri, F. Concentration of some heavy metals in rice types available in Shiraz market and human health risk assessment. Food Chem. 175, 243–248 (2015).
Khillare, P. S., Jyethi, D. S. & Sarkar, S. Health risk assessment of polycyclic aromatic hydrocarbons and heavy metals via dietary intake of vegetables grown in the vicinity of thermal power plants. Food Chem. Toxicol. 50, 1642–1652 (2012).
Rezaei, H. et al. Health-risk assessment related to the fluoride, nitrate, and Nitrite in the drinking water in the Sanandaj, Kurdistan County, Iran. Hum. Ecol. Risk Assessment: Int. J. 25, 1–9 (2018).
Rice, E. W., Bridgewater, L. & Association, A. P. H. Standard Methods for the Examination of Water and Wastewater. Vol. 10. (American Public Health Association, 2012).
Ghanbarian, M., Ghanbarian, M., Tabatabaie, T., Ghanbarian, M. & Ghadiri, S. K. Distributing and assessing fluoride health risk in urban drinking water resources in Fars Province, Iran, using the geographical information system. Environ. Geochem. Health 1–11 (2021).
Bazeli, J. et al. Health risk assessment techniques to evaluate non-carcinogenic human health risk due to fluoride, nitrite and nitrate using Monte Carlo simulation and sensitivity analysis in Groundwater of Khaf County, Iran. Int. J. Environ. Anal. Chem. 102, 1793–1813 (2022).
Ashrafi, S. D., Jaafari, J., Sattari, L., Esmaeilzadeh, N. & Safari, G. H. Monitoring and health risk assessment of fluoride in drinking water of East Azerbaijan Province, Iran. Int. J. Environ. Anal. Chem. 103, 1–15 (2023).
USEPA Guidelines for carcinogen risk assessment. Fed. Reg. 70, 17765–18717 (2005).
Kissell, R. Algorithmic Trading Methods: Applications Using Advanced Statistics, Optimization, and Machine Learning Techniques (Academic, 2020).
Badeenezhad, A. et al. Temporal distribution and zoning of nitrate and fluoride concentrations in Behbahan drinking water distribution network and health risk assessment by using sensitivity analysis and Monte Carlo simulation. Int. J. Environ. Anal. Chem. 103, 3163–3180 (2023).
Rezvani Ghalhari, M., Kalteh, S., Asgari Tarazooj, F., Zeraatkar, A. & Mahvi, A. H. Health risk assessment of nitrate and fluoride in bottled water: a case study of Iran. Environ. Sci. Pollut. Res. 28, 48955–48966 (2021).
Badeenezhad, A. et al. Factors affecting the nitrate concentration and its health risk assessment in drinking groundwater by application of Monte Carlo simulation and geographic information system. Hum. Ecol. Risk Assessment: Int. J. 27, 1458–1471 (2021).
Jafari, A., Kamarehie, B., Ghaderpoori, M., Khoshnamvand, N. & Birjandi, M. The concentration data of heavy metals in Iranian grown and imported rice and human health hazard assessment. Data Brief. 16, 453–459 (2018).
Qasemi, M. et al. Spatial distribution of fluoride and nitrate in groundwater and its associated human health risk assessment in residents living in Western Khorasan Razavi, Iran. Desalin. Water Treat. 170, 176–186 (2019).
Kaur, L., Rishi, M. S. & Siddiqui, A. U. Deterministic and probabilistic health risk assessment techniques to evaluate non-carcinogenic human health risk (NHHR) due to fluoride and nitrate in groundwater of Panipat, Haryana, India. Environ. Pollut. 259, 113711 (2020).
Golaki, M., Azhdarpoor, A., Mohamadpour, A., Derakhshan, Z. & Conti, G. O. Health risk assessment and spatial distribution of nitrate, nitrite, fluoride, and coliform contaminants in drinking water resources of kazerun, Iran. Environ. Res. 203, 111850 (2022).
Radfarad, M. et al. Desalination and water treatment health risk assessment to fluoride and nitrate in drinking water of rural residents living in the Bardaskan city, arid region, southeastern Iran. Desalin. Water Treat. 145 (2019).
Mahmoodlu, G., Raghimi, M., Ramezani Mojaveri, M. & M. & Investigating the relationship between the fluoride concentration in groundwater and spatial distribution of loess deposits in the Gorgan Plain. J. Res. Environ. Health. 8, 378–391 (2023).
Battaleb-Looie, S., Moore, F., Malde, M. & Jacks, G. Fluoride in groundwater, dates and wheat: estimated exposure dose in the population of Bushehr, Iran. J. Food Compos. Anal. 29, 94–99 (2013).
Yousefi, M., Ghoochani, M. & Mahvi, A. H. Health risk assessment to fluoride in drinking water of rural residents living in the Poldasht city, Northwest of Iran. Ecotoxicol. Environ. Saf. 148, 426–430 (2018).
Akiniwa, K. Re-examination of acute toxicity of fluoride. Fluoride 30, 89–104 (1997).
Huang, D. et al. Probabilistic risk assessment of Chinese residents’ exposure to fluoride in improved drinking water in endemic fluorosis areas. Environ. Pollut. 222, 118–125 (2017).
Emenike, C. P., Tenebe, I. T. & Jarvis, P. Fluoride contamination in groundwater sources in Southwestern Nigeria: Assessment using multivariate statistical approach and human health risk. Ecotoxicol. Environ. Saf. 156, 391–402 (2018).
Marhamati, M., Afshari, A., Kiani, B., Jannat, B. & Hashemi, M. Nitrite and nitrate levels in groundwater, water distribution network, bottled water and juices in Iran: a systematic review. Curr. Pharm. Biotechnol. 22, 1325–1337 (2021).
Ghalhari, M. R. Bashardoust P, Khoshnamvand N & Mahvi, A. H. Quantitative probabilistic risk assessment of fluoride, nitrate and nitrite intake from bottled water in west Iranian consumers. Res. Rep. 55, 363–387 (2022).
Karunanidhi, D., Aravinthasamy, P., Subramani, T., Wu, J. & Srinivasamoorthy, K. Potential health risk assessment for fluoride and nitrate contamination in hard rock aquifers of Shanmuganadhi River basin, South India. Hum. Ecol. Risk Assessment: Int. J. 25, 250–270 (2019).
Fallahzadeh, R. A., Almodaresi, S. A., Ghadirian, D. & Fattahi, A. Spatial analysis and probabilistic risk assessment of exposure to nitrate in drinking water of Abarkouh, Iran. J. Environ. Health Sustain. Dev. 4, 744-752 (2019).
Acknowledgements
The authors hereby express their gratitude to the Student Research Committee of Kermanshah University of Medical Sciences for any support (Project No 50004409, Ethical Code: (IR.KUMS.REC.1403.407)).
Author information
Authors and Affiliations
Contributions
A. J: Supervision, original idea, reviewing-editing manuscript and improving manuscript quality, review and editing manuscript. H. Y: Writing—first draft, Data collection, Review and editing tables L. A:, Writing—first draft , Data collection, N. N: Writing—first draft, Data collection, Review and editing tables All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
Ethically approved.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mianeh, H.Y., Amiri, L., Jafari, A. et al. Health risk assessment via Monte Carlo simulation and sensitivity analysis for fluoride and nitrate content in bottled waters consumed in Kermanshah city, Iran. Sci Rep 15, 5008 (2025). https://doi.org/10.1038/s41598-025-89439-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-89439-6
Keywords
This article is cited by
-
Evaluation of Hydrogeochemical Characteristics of Groundwater Resources in the Kuju Coal Mining Area of Ramgarh District, Jharkhand
Water, Air, & Soil Pollution (2026)
-
Source apportionment, drinking water quality prediction and health risk appraisal of groundwater nitrate using hydrochemistry, machine learning and Monte Carlo simulation - A case study from the Suruliyar River basin, South India
Environmental Geochemistry and Health (2026)
