
Abstract
Diagnosis-related groups (DRG) is emerging as an effective tool for measuring the quality and efficiency of medical services. This study aims to explore a DRG combination scheme for control the hospitalization costs in patients with uterine leiomyoma (UL). This study enrolled a total of 3087 UL patients from a tertiary hospital in Chongqing between year 2017 and 2021. The data of front sheet of the medical record of each UL patient were retrospectively extracted. Mann-Whitney U test and Kruskal-Wallis H test, and subsequent multivariate logistic regression analysis were used to identify the significant factor influencing the hospitalization cost. Then, a decision tree model was performed to establish the DRG case mix model, and to calculate the payment standards and cost caps for each DRG group. The average age of all patients was 43.03 years old, the average length of stay (LOS) was 6.66 days, and the average total hospitalization cost was 22,436.11 yuan. The highest proportion of the total hospitalization cost was treatment cost (29.46%), followed by diagnostic cost (28.98%), consumable cost (26.01%), etc. Factors including surgery type, LOS, and complications or comorbidities had significant impact on hospitalization costs, among which surgery type were the main influencing factor. Using the three factors as classification nodes, a total of 10 DRG groups were established by a decision tree model. The value of reduction in variance was 0.68, indicating significant heterogeneity between groups. The coefficient of variation for hospitalization costs ranged from 0.08 to 0.44, indicating minimal variation and reasonable grouping result. The established hospitalization cost scheme for patients with UL is reasonable in this study. It provides a reference for the advancement and implementation of DRG payments in local area.
Similar content being viewed by others

Introduction
Uterine leiomyoma (UL) is the most common benign tumor in female reproductive system1, and it occurs frequently in women aged 30 to 50 years old. Although UL is usually asymptomatic, it can cause abnormal uterine bleeding, infertility, pelvic pain, and even miscarriage2,3. These symptoms can negatively impact the patient’s daily quality of life, as well as cause significantly direct and indirect economic costs.
Diagnosis-related groups (DRG), as a modern case-mixing scheme, is recognized as one of the most advanced payment methods globally4,5. It serves as a crucial tool for measuring the quality and efficiency of healthcare services, as well as for health insurance reimbursement6. Based on the principle of prioritizing clinical similarity while considering the similarity in resource utilization, DRGs classify patients into diagnosis groups based on primary clinical diagnosis and surgeries, taking into account factors such as age, length of stay (LOS), comorbidities and complications (CCs), and surgery type, etc. Each diagnosis group is then assigned a code, which determines the corresponding reimbursement standards.
DRG not only balances the interests of governments, healthcare institutions, and patients but also helps achieve an optimal balance between healthcare quality and cost. As a result, it is widely utilized in healthcare resource allocation, healthcare institution pricing, performance management, quality control, and more7. Whether in meeting DRG payment requirements or ensuring medical quality, safety, and efficiency, strengthening clinical pathway management and promoting the standardization of clinical pathways are essential. Refining DRG groupings further optimizes medical service processes, improves patient satisfaction, and supports the healthy development of the healthcare industry8.
The exhaustive chi-square automatic interaction detection (E-CHAID) algorithm is an advanced modification of the traditional CHAID algorithm and is widely used in analyzing classified quantitative data. A study indicates that E-CHAID demonstrates superior performance in identifying the most significant grouping factors compared to CHAID, while also exhibiting enhanced segmentation capabilities over the CART algorithm9.
This study is based on the hospitalization costs of patients with uterine fibroids to explore the DRG groups scheme for inpatients with uterine fibroids and to formulate a reference standard for the hospitalization costs of patients with uterine fibroids, providing a basis for the reasonable control of hospitalization costs for patients with uterine fibroids in local city (Chongqing).
Materials and methods
Data source and selection
According to the International Classification of Diseases (ICD-10) standard, all patients with UL (ICD-10: D25.-) hospitalized between 2017 and 2021 were enrolled from a tertiary hospital. The data of front sheet of the medical record of each UL patient were retrospectively extracted, including the patient’s personal information, diagnosis and treatment information, and cost information.
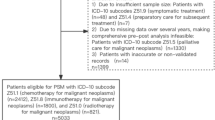
After sorting out and checking the data quality of all UL cases, a total of 3708 cases were identified. Subsequently, those with the following criteria were excluded, including cases with missing or leaked items, or logical errors (2 cases), cases with a length of stay (LOS) shorter than 2 days or longer than 60 days (671 cases), case with hospitalization costs over the range of X ± 3s (47 cases). After exclusion, a total of 3087 valid cases were ultimately included in the study, with an effective inclusion rate of 81.09%. This study was performed under the guidelines established by the Declaration of Helsinki. As this is a retrospective analysis of deidentified data, the ethical approval and informed consents of patients were waived by ethics committee of Chongqing Medical University.
Statistical analysis
Univariate analyses of factors affecting the hospitalization costs in UL patients were performed by Mann-Whitney U test or Kruskal-Wallis H test. Then, those factors with a P < 0.05 were included for further multivariate logistic regression analysis to identify the main influencing factors of hospitalization costs. A significance level of P < 0.05 was used to determine statistical significance.
The decision tree model was constructed using E-CHAID. Independent variables were selected based on their impact on hospitalization costs and statistical significance, while the dependent variable was the total hospitalization costs of patients with UL to group DRG cases.
Evaluation index
The heterogeneity between groups was evaluated using the non-parametric Kruskal-Wallis H test and reduction in variance (RIV), while the homogeneity within groups was evaluated using the coefficient of variation (CV)9,10. The rationality and validity of the grouping were tested based on the data distribution. RIV was calculated using the formula: RIV = sum of squared deviations of subsets/sum of squared deviations of populations, and CV was calculated using the formula: CV = standard deviation/mean. The larger RIV indicates greater heterogeneity between groups, resulting in better grouping. The smaller CV indicates smaller within-group variation, which leads to better grouping. The data was analyzed using SPSS 26.0 software, and a significance level of P < 0.05 was used.
Results
Basic information of patients with UL
A total of 3087 eligible UL cases were enrolled in this study, with an average age of 43.03 years old and a median age of 44.00 years old. The age distribution showed that 29.58% of patients were aged ≤ 39 years, 53.97% were aged 40–49 years, and 16.46% were aged ≥ 50 years. The vast majority of patients were of Han ethnicity (98.06%) and married (93.85%). Approximately 96.7% of patients were covered by Medicare, while 3.3% were self-paying. The average LOS was 6.66 days, and 62% of all had a LOS ≤ 7 Days. The most common surgery type was hysteroscopic surgery (42.47%), followed by high-intensity focused ultrasound (26.17%) and general operation (22.55%). The average total hospitalization cost was 22,436.11 yuan and the median was 22,825.74 yuan. Detailed demographic characteristics and clinical features were presented in (Table 1).
Composition of hospitalization costs
In order to eliminate the effect of inflation, the 2021 hospitalization costs for patients with UL were used as the baseline, and the hospitalization costs for patients with UL were also adjusted before and after the DRG payment according to the consumer price index for healthcare residents in Chongqing, as published by the national bureau of statistics. The highest proportion of the total hospitalization cost was treatment cost (29.46%), followed by diagnostic cost (28.98%), consumable cost (26.01%), drugs cost (9.00%), service cost (5.92%) etc. (Table 2). The cost of treatment, diagnosis and consumables accounted for 84.45% of the total cost.
Univariate analysis of the influencing factors on hospitalized costs
The dependent variable for this study was the hospitalization cost for UL. The independent variables included age, nationality, marital status, type of medical insurance, admission method, admission condition, medical advice discharge, 31-day readmission schedule, Therapeutic effects, LOS, surgery type, and CCs. The Mann-Whitney U test or Kruskal-Wallis H test were performed the analysis. The results turned out that, except nationality, all other factors had a significant impact on the hospitalization costs in patients with UL (Table 1).
Multiple regression analysis of the influencing factors on hospitalized costs
Since the hospitalization costs for UL did not follow a normal distribution, we employed binary logistic regression analysis for logistic regression analysis. Patients were stratified into two categories based on the median cost of hospitalization, which was determined to be 22,436.11 yuan. This categorization resulted in the identification of a high-cost group (costs more than 22,436.11 yuan, coded as 1) and a low-cost group (costs less than 22,436.11 yuan, coded as 0). A binary logistic regression model was constructed with the hospitalization costs group for patients with UL as the dependent variable and the results of univariate analysis as independent variables. For unordered multinomial categorical variables, dummy variables were created with the first category at each factor level serving as the reference. The variance inflation factor of all predictors used in the model was tested to be less than 3 indicating that there is no multicollinearity among the independent variables. The findings revealed that age, surgery type, LOS, and CCs significantly influenced the hospitalization costs in UL patients (Table 3).
DRG grouping: a decision tree model to construct the case combination and the hospitalization cost of each group
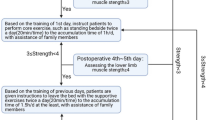
The hospitalization costs was used as the dependent variable, and the significant factors including age, LOS, surgery type, and CCs were used as the independent variables, which were included in the decision tree model. The parameters used in this study are as follows:11,12 the maximum depth of the decision tree model is 3, the minimum sample size of the parent node is 100, the minimum sample size of the child node is 50, and the significance level of the split node is α = 0.05. A total of 10 groups were identified (Fig. 1). After grouping, the Kruskal-Wallis non-parametric test was used to test the cost differences between groups. The results showed that the cost distribution of the 10 groups were not identical (Chi-square value was 2152.551, P < 0.05), indicating a good heterogeneity among the different DRG groups and statistically significant differences.
To enhance the comprehensibility of the cost of each DRG group, we included the original value of hospitalization costs in the analysis. As hospitalization costs are abnormal distribution, we used the median as the standard cost of medical resource consumption for UL cases. The calculated RIV value was 0.68, indicating significant heterogeneity between groups and significant classification. The CV for hospitalization costs ranged from 0.08 to 0.43, indicating minimal variation and reasonable grouping result. To establish cost control measures, the warning cost was set at 75(th) quantile of the inpatient cost for each DRG group, while the upper limit was set at 75(th) quantile plus 1.5 times the interquartile distance (P75 + 1.5Q). The results revealed that 40 cases (1.30% of the total) exceeded the upper limit in each DRG group (Table 4).

Decision tree diagram of influencing factors of hospitalization costs of uterine leiomyoma.
Discussion
Through the decision tree model, we found that the surgery type was the most significant factor associated with the hospitalization cost in UL patients. Other significant factors included the LOS and CCs. The classification node of the decision tree model in the first layer was the surgery type, this is directly related to the recovery effect of patients and also has a significant impact on their economic burden during hospitalization. In order to improve the quality of medical services and reduce the financial burden on patients, doctors should take full account of patients’ actual situations and formulate personalized treatment plans13. The second level classification node was the LOS, which is an important temporal indicator of healthcare resource consumption, and the results show that the higher the LOS the higher the hospitalization costs of the patients. On the basis of ensuring the quality and safety of medical services, reducing LOS is an effective way of controlling hospitalization costs, which not only reduces the cost of hospitalization for patients and alleviates their financial burden14,15but also improves the turnover rate of hospital beds and the efficiency and effectiveness of medical services16,17. CCs was the third factor to consider. Having CCs means that the patient’s condition is more complex and requires more extensive examinations and treatments; these additional examination items and treatments will increase the patient’s hospitalization costs. In addition to the complexity of the condition, patients may require longer LOS for observation and treatment, which will naturally increase the basic costs such as bed and nursing fees during hospitalization18; hospitals should fully consider patients’ CCs when providing medical services, and adopt reasonable treatment plans and management measures to reduce hospitalization costs and alleviate patients’ financial burden. At the same time, hospitals should also strengthen their internal management, improve the efficiency and quality of medical services, and provide more high-quality, efficient and economical medical services to patients.
Although age was less influential compared to surgery type, LOS, and CCs, it still played a significant role in hospitalization costs among UL patients. Age can impact patients’ overall health status, and improving health conditions can significantly reduce the incidence of age-related diseases and associated medical costs. Therefore, measures such as strengthening disease prevention, optimizing resource allocation, enhancing healthcare coverage, and reinforcing supervision can effectively reduce hospitalization costs and improve the quality of life for elderly patients.
Conclusion
This study identified the factors that affect hospitalization costs in UL patients and constructed DRG payment groups based on the E-CHAID algorithm. The use of DRG grouping to establish hospitalization costs standards is advantageous for the rational allocation of medical resources, enhancing medical quality and efficiency, and reducing the economic burden on patients and society19. At the same time, it can provide a theoretical basis and verification methods for fully implementing DRG payment in the region.
Data availability
The datasets for this study can be obtained from the corresponding author upon any reasonable request.
References
Borah, B. J. et al. Association between patient characteristics and treatment procedure among patients with uterine leiomyomas. Obstet. Gynecol. 127 (1), 67–77 (2016).
Yu, O. et al. A US population-based study of uterine fibroid diagnosis incidence, trends, and prevalence: 2005 through 2014. Am. J. Obstet. Gynecol. 219 (6), 591 (2018).
Fortin, C., Flyckt, R. & Falcone, T. Alternatives to hysterectomy: the burden of fibroids and the quality of life. Best Pract. Res. Clin. Obstet. Gynaecol. 46, 31–42 (2018).
Zhao, C. et al. Diagnosis-related group (DRG)-based case-mix funding system, a promising alternative for fee for service payment in China. Biosci. Trends 12 (2), 109–115 (2018).
Yu, L. & Lang, J. Diagnosis-related groups (DRG) pricing and payment policy in China: where are we? Hepatobil. Surg. Nutr. 9 (6), 771–773 (2020).
Liu, X. et al. Path analysis on medical expenditures of 855 patients with chronic kidney disease in a hospital in Beijing. Chin. Med. J. (Engl.) 131 (1), 25–31 (2018).
Lang, X. et al. A bibliometric analysis of diagnosis related groups from 2013 to 2022. Risk Manag Healthc. Policy 16, 1215–1228 (2023).
Chang, W. F. et al. A study of the types and manifestations of physicians’ unintended behaviors in the DRG payment system. Front. Public. Health 11, 1141981 (2023).
Luo, A. J. et al. Diagnosis related group grouping study of senile cataract patients based on E-CHAID algorithm. Int. J. Ophthalmol. 11 (2), 308–313 (2018).
Gong, J. et al. Study of hospitalization costs in patients with cerebral ischemia based on E-CHAID algorithm. J. Healthc. Eng. 2022, 3978577 (2022).
Wu, S. W. et al. Research of medical expenditure among inpatients with unstable angina pectoris in a single center. Chin. Med. J. (Engl.) 130 (13), 1529–1533 (2017).
Wu, Y. et al. Evaluation of length of stay, care volume, in-hospital mortality, and emergency readmission rate associated with use of diagnosis-related groups for internal resource allocation in public hospitals in Hong Kong. JAMA Netw. Open. 5 (2), e2145685 (2022).
Su, F. Y. et al. Analysis of hospitalization costs related to fall injuries in elderly patients. World J. Clin. Cases. 9 (6), 1271–1283 (2021).
Zeng, S. et al. Cost control of treatment for cerebrovascular patients using a machine learning model in Western China. J. Healthc. Eng. 2021, 6158961 (2021).
Lu, J. et al. Performance assessment of medical service for organ transplant department based on diagnosis-related groups: a programme incorporating ischemia-free liver transplantation in China. Front. Public. Health 11, 1092182 (2023).
Wei, A., Ren, J. & Feng, W. The impact of DRG on resource consumption of inpatient with ischemic stroke. Front. Public. Health 11, 1213931 (2023).
Wu, S. W. et al. Research on 2041 cases of high inpatient expenditure and influence factors during 3 years in a single center. Chin. Med. J. (Engl.) 129 (19), 2325–2330 (2016).
He, Y., Chen, S. & Chen, Y. Analysis of hospitalization costs in patients suffering from cerebral infarction along with varied comorbidities. Int. J. Environ. Res. Public. Health 19 (22), 15053 (2022).
Zhang, L. & Sun, L. Impacts of diagnosis-related groups payment on the healthcare providers’ behavior in China: a cross-sectional study among physicians. Risk Manag Healthc. Policy 14, 2263–2276 (2021).
Funding
This research was funded by Chongqing Municipal Science and Technology Bureau’s Chongqing Talent Plan for 2022 (cstc 2022 ycjh-bgzxm 0015).
Author information
Authors and Affiliations
Contributions
Authors contributions: (I) Conception and design: D.D.(II) Administrative support: D.D.(III) Provision of study materials or patients: Z.Z., D.D.(IV) Collection and assembly of data: Z.Z., D.D.(V) Data analysis and interpretation: Z.Z.(VI) Visualization: Z.Z.(VII) Manuscript writing: All authors(VIII) Final approval of manuscript: All authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zou, Z., Deng, D. Diagnosis-related groups study of uterine leiomyoma patients based on E-CHAID. Sci Rep 15, 6460 (2025). https://doi.org/10.1038/s41598-025-89645-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-89645-2
