
Abstract
The forearm function in children is influenced by several factors, with the length relationship between the ulna and radius being particularly important. However, due to the underdevelopment of cartilage in children, assessing this length relationship through imaging techniques is challenging. This study aims to identify a reliable method for evaluating the lengths of the ulna and radius in children, establish normal values for the ratio of the epiphyseal plate lengths of these bones, examine this ratio in children with Monteggia fractures, and investigate its role in determining forearm function in the pediatric population. This multicenter study involved 432 normal children under 15 years of age as controls. A retrospective analysis was conducted on anteroposterior and lateral radiographs from 58 children with Monteggia fractures after surgery. The correlation between the inner-epiphysis ulna-radius length ratio, postoperative Mayo elbow joint function score, and radiographic reduction quality of the brachioradial joint was analyzed. The mean inner-epiphysis ulna-radius length ratio was 1.094, with a standard deviation of 0.024. The maximum value ranged from 1.0336 to 1.168. The medical reference range, with a 95% confidence level, was calculated as 1.047 to 1.141. In children with Monteggia fractures, the postoperative inner-epiphysis ulna-radius length ratio showed significant correlations (P < 0.05) with postoperative imaging reduction quality, as well as the range of pronation, supination, flexion, and extension, and the Mayo elbow score. In normal children, the inner-epiphysis ulna-radius length ratio ranges from 1.0336 to 1.168, with a medical reference range of 1.047 to 1.141 at a 95% confidence level. Restoring this ratio (1.047–1.141) in children with Monteggia fractures can improve elbow function and radiographic radiocapitellar joint reduction quality.
Similar content being viewed by others

Introduction
Among children’s fractures, radius/ulna fractures are the most frequently observed1,2. Due to the abundance of cartilage in children, radiographic development is not fully visible on X-rays. As a result, the rate of missed or misdiagnosed fractures in children is higher than in adults, ranging from 16 to 33%3. Incorrect or delayed diagnosis of pediatric fractures can severely affect bone growth and development, leading to functional impairments, growth disturbances, and deformities4,5.
Monteggia fracture is a rare type of forearm fracture in children, representing about 1% of all forearm fractures6. It involves complex injuries to the ulna, often accompanied by dislocation or fracture of the radial head in multiple directions. The clinical classification proposed by Bado highlights the direction of radial head dislocation, offering important guidance for treatment and prognosis7. If acute Monteggia fractures are not treated correctly within 3 weeks, they may result in Missed Monteggia fractures (MMF)8. Gopinathan suggests that children with chronic Monteggia fractures frequently exhibit abnormal ulna-to-radius length ratios, which can affect growth and forearm stability9. Ring proposes that an imbalance in ulna and radius length in children can lead to wrist joint deviation, cubitus varus or valgus, limited pronation or supination, and other deformities that impair both the appearance and function of the forearm10. Fu recommends ulna osteotomy between the proximal 1/3 and 1/5 as a safer and more stable method for managing MMF and stabilizing the radio-capitellar joint11.
Currently, the general consensus is that osteotomy and external fixation may improve the abnormal ulna-to-radius ratio; however, a standardized method for calculating the exact extension distance is lacking12. Furthermore, due to the presence of the epiphysis and cartilage, accurately measuring the complete length of the ulna and radius from imaging remains difficult. The objective of this study is to identify an appropriate method for evaluating ulna and radius length in healthy children, establish normal values for the inner-epiphysis ulna-radius length ratio, validate this ratio in children with Monteggia fractures, and investigate its role in forearm function in the pediatric population. In this study we collected anteroposterior and lateral forearm radiographs of 432 children to investigate the ratio and range of the inner-epiphysis ulna-radius length. And we validate this ratio on anteroposterior and lateral radiographs from 58 children with Monteggia fractures after surgery.
Methods
The anteroposterior and lateral X-ray images of normal radius and ulna were retrospectively analyzed in this study. These images were collected from outpatients suspected of having fractures or deformities, with final negative results, from the Department of Radiology at Hunan Provincial People’s Hospital, Ningxiang People’s Hospital, Dongan People’s Hospital, and Yuanling People’s Hospital between January 2019 and December 2023. Inclusion criteria: (1) Age 1–15 years; (2) Normal forearm X-rays; (3) Standard anteroposterior and lateral forearm radiographs. Exclusion criteria: (1) Age less than 1 year or greater than 15 years; (2) Positive findings (fracture, dislocation, infection, deformity, etc.) in the forearm X-rays; (3) Non-standardized X-ray images.
When the normal cases were collected, the ratio of ulna to radius in each age group was check if the ratios in each age group were constant, and then we evaluated the Monteggia fracture cases by dividing them into groups that fell within this normal value(define as 95% confidence interval of measured values) and those that did not. Patients diagnosed with acute Monteggia fractures and who underwent surgery between January 2019 and December 2023 were included in Group A. Inclusion criteria: (1) Age 1–15 years; (2) Diagnosis of acute Monteggia fracture with a clear trauma history and injury duration of no more than 3 weeks; (3) Standard anteroposterior and lateral forearm radiographs taken postoperatively; (4) Received reduction treatment. Exclusion criteria: (1) Unclear trauma history, injury duration exceeding 3 weeks, pathological forearm fracture, or congenital deformity; (2) Systemic diseases such as bone growth disorders; (3) Severe vascular or nerve injury; (4) Non-standardized forearm position on X-ray films; (5) Loss to follow-up or follow-up duration less than 6 months.
Patients diagnosed with chronic Monteggia fractures and who underwent surgery between January 2019 and December 2023 were included in Group B. Inclusion criteria: (1) Age 1–15 years; (2) Diagnosis of chronic Monteggia fracture with deformity present for more than 3 weeks; (3) Radiographs, including standard anteroposterior and lateral forearm views. Exclusion criteria: (1) Pathological forearm fracture or congenital deformity; (2) Systemic diseases such as bone growth disorders; (3) Vascular or nerve injury; (4) Non-standardized forearm position on X-ray films; (5) Loss to follow-up or follow-up duration less than 6 months.
Surgical technique
All procedures were performed by qualified pediatric orthopedic surgeons. Patients in both Group A and Group B were positioned supine with the affected limb securely immobilized on the arm table. To minimize the risk of hemorrhage, tourniquets were commonly used during surgery. Under general anesthesia, patients with acute Monteggia fractures underwent ulna reduction and internal fixation (using Kirschner wire, elastic intramedullary nail, or plate) to restore the ulna to its anatomical position, followed by radial head reduction. Patients with chronic Monteggia fractures were treated with ulna posteriorly convex osteotomy and lengthening, with internal fixation using a plate. Simultaneously, the radial head was reduced, and the annular ligament was reconstructed. Kirschner wire fixation was used for the radius based on the stability of the radial head reduction. After fixation, construct stability was assessed using fluoroscopy. The affected limb was then immobilized in a tubular cast, flexed at 70–90 degrees, and the forearm placed in the supination position for 4 weeks. After cast removal, patients were instructed to undergo elbow function rehabilitation under the guidance of a rehabilitation physician.
Follow up
All patients in Groups A and B underwent anteroposterior and lateral X-rays every 3 months after surgery as part of routine follow-up. Elbow function was also evaluated at each follow-up. Outcome parameters and complications were recorded and analyzed.
Parameters of outcomes
Imaging evaluation
The reduction quality of the radial head was assessed using the X-ray taken at the last follow-up after removal of the internal fixation (follow-up time > 1 year). The reduction quality was classified into three grades based on the position of the radiocapitellar line (RCL) of the proximal radius: excellent (the long axis of the proximal radius passed through the middle third of the capitellum on both anteroposterior and lateral radiographs), good (the long axis of the proximal radius passed through the capitellum but not the middle third), and poor (the long axis of the proximal radius did not pass through the capitellum on both anteroposterior and lateral radiographs)13.
Elbow function evaluation
At the last follow-up (follow-up time > 1 year), the range of pronation, supination, flexion, and extension were recorded, and elbow function was evaluated using the Mayo Elbow Performance Score (MEPS). The scoring system was completed objectively by senior residents based on follow-up results.
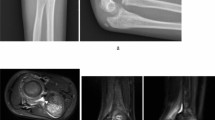
The Picture Archiving and Communication System (PACS) version used was AnnetPACS V 2.0.01. All imaging data were independently measured by a senior orthopedic resident who had undergone three months of systematic radiology training. To ensure the reliability of the measurement data, ten X-ray films were randomly selected and measured by both a senior associate chief orthopedic doctor and an attending doctor from the imaging department to authenticate the measurements. Three researchers used identical computer programs with consistent measurement software. The inner-epiphyseal ulna length (IEUL) was defined as the distance from the tip of the olecranon to the midpoint of the distal epiphyseal plate of the ulna (red line). The inner-epiphyseal radial length (IERL), represented by the yellow line in Fig. 1, was defined as the distance between the midpoints of the radial head epiphysis and the distal radius epiphysis. The inner-epiphyseal ulna-radius length ratio was calculated as follows:
\(Inner~epiphyseal~ulna~radius~length~ratio=\frac{{The~inner - epiphyseal~ulnar~length~\left( {IEUL} \right)}}{{The~inner - epiphyseal~radial~length~\left( {IERL} \right)}}\)
Pearson correlation analysis was used to examine the relationship between the reduction grade of the radial head, the range of pronation, supination, flexion and extension, the MEPS, and the inner-epiphyseal ulna-radius length ratio.

The inner-epiphyseal length of ulna and radius was measured in the anteroposterior and lateral view of the X-ray films, red line: ulna measurement method, yellow line: radial measurement method.
Statistical analysis
The data were processed using SPSS 26.0 software. Categorical data were expressed as frequencies, and continuous data with a normal distribution and homogeneous variance were presented as mean ± standard deviation (Mean ± SD). Independent sample t-tests were used to compare quantitative data, chi-square tests were used to compare categorical data, and Fisher’s exact test was applied for univariate analysis when the expected count was less than 5. Additionally, Pearson correlation analysis was used to examine the relationship between the reduction grade of the radial head, the range of pronation, supination, flexion and extension, the MEPS, and the inner-epiphyseal ulna-radius length ratio. A significance level of α = 0.05 was set, with P < 0.05 considered statistically significant.
Results
The inner-epiphysis ulna-radius length ratio in normal children
The epiphyseal plate and ossification center of the ulna do not develop proximally until 9 years of age, and the epiphysis is not visible on radiographs. As a result, it is difficult to measure the lengths of the ulna and radius radiologically, and all measurements excluded the ossification center and epiphyseal plate.
A total of 432 children aged 1–15 years with ulna and radius X-ray films were included, with a minimum of 30 children in each age group. There were 255 boys (59.0%) and 177 girls (41.0%). The left forearm was measured in 236 children (54.6%), while the right forearm was measured in 196 children (45.4%). The mean inner-epiphyseal ulna-radius length ratio was 1.094, with a standard deviation of 0.024, and the range of values was 1.0336 to 1.168. The 95% medical reference range was 1.047 to 1.141, both the ulna and radius lengths increased with age, their length ratio at the epiphyseal plate remained relatively constant across age groups (Fig. 2).

The relationship between Ulna/radius lengths and age, and the relationship between Ulna/radius lengths ratio and age. We can see that ulna and radius lengths increase with age(Left), the inner-epiphyseal length ratio remained relatively constant within different age groups (Right).
The role of inner-epiphysis ulna-radius length ratio in Monteggia fracture
A retrospective analysis was performed on postoperative anteroposterior and lateral radiographs of the forearm in pediatric patients with Monteggia fractures. The inner-epiphyseal ulna/radius length ratio was measured after surgery, and elbow joint function, forearm rotation range, and radiographic reduction quality of the brachioradial joint were assessed at the final follow-up. Correlations between these parameters were examined.
In Group A, 30 cases of fresh Monteggia fractures were included, with an average age of 6.33 ± 2.72 years (range: 1–12 years). The mean follow-up duration was 25.07 ± 10.86 months. There were 22 cases of Bado type I, one case of Bado type II, seven cases of Bado type III, and no cases of Bado type IV. Closed reduction and Kirschner wire internal fixation were performed in seven children, closed reduction and elastic intramedullary nail implantation in nine children, and open reduction with plate internal fixation in 14 children. The average inner-epiphyseal ulna-radius length ratio was 1.091 ± 0.022. The average MEPS score at the last follow-up was 90.67 ± 3.41, the average pronation range was 79.67 ± 1.83, the average supination range was 83.67 ± 2.25, and the average flexion and extension range was 139.33 ± 4.69. All patients achieved excellent radial head reduction.
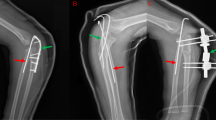
In Group B, there were 28 cases of chronic Monteggia fracture, with an average age of 7.68 ± 2.9 years (range: 1–14 years) and an average follow-up duration of 17.82 ± 10.50 months. Anterior dislocation of the radial head was observed in 24 cases, anterolateral dislocation in 3 cases, and posterolateral dislocation in 1 case. Twenty-one children underwent debridement of the humeroradial joint cavity, followed by ulna osteotomy and lengthening with plate internal fixation. Seven children received the same procedure, along with Kirschner wire fixation (typical case presented in Figs. 3 and 4). The average inner-epiphyseal ulna-radius length ratio was 1.070 ± 0.027. The average Mayo Elbow Performance Score (MEPS) at the last follow-up was 87.32 ± 7.26, the average pronation range was 71.61 ± 12.84, the average supination range was 77.14 ± 5.52, and the average flexion and extension range was 124.39 ± 12.32. All patients achieved excellent radial head reduction. Outcome parameters for both groups are summarized in Table 1.

A case of a 11-year-old boy who sustained a Bado type I Monteggia fracture at the age of 6. The patient underwent ulna osteotomy and plate internal fixation, Kirschner wire fixation, and annular ligament repair as part of preoperative diagnosis. However, post-surgery recovery did not restore inner-epiphysis ulna-radius length ratio to 1.047–1.141.

A case of a 12-year-old boy who sustained a Bado type I Monteggia fracture at the age of 10. The patient underwent ulna osteotomy, plate lengthening. The inner-epiphysis ulna-radius length ratio was restored to 1.047–1.141, the patient has an excellent recovery of elbow joint function at the 24-month follow-up.
The 95% confidence interval for the inner-epiphyseal ulna-radius length ratio was defined as 1.047 to 1.141. Significant differences were observed in radiographic reduction quality, pronation range, supination range, flexion and extension range, and MEPS scores between the normal and abnormal groups (P = 0.002, 0.007, 0.030, 0.045, < 0.001, respectively). We also performed a univariate analysis with Mayo elbow function evaluation as the outcome index. There was no correlation between the Mayo Score and gender, side, fracture type (P > 0.05). The elbow Mayo score in the normal inner-epiphyseal ulna-radius length ratio group was higher than abnormal group (P < 0.05). The elbow Mayo score of the group with injury to surgery time less than 6 months was higher than that of the group with injury to surgery time more than 6 months(P < 0.05) (Table 2). These findings indicate a statistically significant relationship (P < 0.05) between the postoperative inner-epiphyseal ulna-radius length ratio and postoperative imaging reduction quality, pronation range, supination range, flexion and extension range, and MEPS score.
Discussion
The growth of the radius and ulna in children occurs primarily in the epiphysis at both ends. Ossification centers typically appear in the distal radius between 6 and 12 months of age, while osteogenic centers emerge in the distal ulna around 6 to 8 years of age14. Normal bone and cartilage development relies on appropriate contact pressure within the joint extremities15. Imbalanced growth between the radius and ulna can lead to abnormal contact pressure between the capitellum and radial head. Additionally, delayed development of the annular ligament relative to the elbow joint further exacerbates this imbalance in the length ratio. Previous studies have shown that loss of Hox11 function results in significant deformities on either the ulnar or radial side of the forearm by disrupting chondrocyte development, hindering the complete formation of growth plates, and limiting longitudinal bone growth16.
Common pediatric orthopedic conditions associated with abnormal ulna and radius length ratios include congenital radius dysplasia, congenital ulna dysplasia, congenital radioulnar joint fusion, congenital radial head dislocation, and other disorders17,18,19. These conditions exhibit asymmetric growth patterns as children develop, leading to increased limb dysfunction due to forearm deformities. Additionally, trauma or tumor-related factors can also cause abnormal ulna and radius length ratios. Acute loss of the ulna and radius length ratio occurs in common forearm fractures such as ulna and radius fractures or Monteggia fractures. Fractures involving the epiphyseal plate or bone diseases like multiple osteochondromas, osteomyelitis, or bone tumors that invade the epiphyseal plate can result in growth disorders and subsequent deformities, characterized by abnormal ulna-to-radius length ratios20,21. Therefore, restoring the proper inner-epiphyseal ulna-radius ratio is crucial for functional reconstruction surgery.
Due to the abundant cartilage in children, which is not visible on X-ray images, accurately measuring the full length of the ulna and radius before and after surgery, as well as during intraoperative fluoroscopy, often presents challenges. In this study, the observation index was defined as the length of the epiphyseal plate, which can be easily obtained through intraoperative fluoroscopy or X-ray imaging. To minimize potential human error, all measurements were performed by a single investigator, who assessed the line connecting the midpoints of the epiphyseal plates at both ends of the ulna and radius. However, identifying the midpoint of the proximal ulna was challenging due to overlap with the distal humerus; therefore, the midpoint was located at the most prominent point of the olecranon tip and coronoid process.
The most common pathological change in children with chronic Monteggia fracture is forearm deformity, primarily affecting the ulnar arch and resulting in a chronic imbalance in the length ratio between the ulna and radius epiphyseal plates. This imbalance leads to dislocation and hypertrophy of the radial head22, causing secondary valgus deformity of the elbow, limited flexion, and loss of forearm function. Dislocation of the radial head’s long stem leads to accelerated growth, resulting in radius lengthening and further disruption of the ulna-radius ratio23. Ning et al. observed a positive correlation between age and both radius and ulna growth in consistent proportions. In individuals with short-length types, the anterior ratio of radius to ulna (RLRU) ranged from 0.8941 to 0.9251, while the lateral ratio ranged from 0.8936 to 0.937524. The findings from this study emphasize that restoring a length ratio between 1.047 and 1.141 for the ulna and radius is essential for maintaining biomechanical stability after radial head reduction in the treatment of Monteggia fractures. By collecting imaging data from healthy children, we found that the length ratio between the ulna and radius remained relatively constant across different age groups. Consequently, we aimed to investigate whether these parameters could serve as reliable indicators to guide treatment strategies for Monteggia fractures. Some researchers suggest over-lengthening of the ulna25 to prevent ulnar variation or recurrence of radial head dislocation; however, the extent of over-lengthening remains uncertain due to reports of wrist joint and elbow joint impingement in some cases26.
We found that while both the ulna and radius lengths increased with age, their length ratio at the epiphyseal plate remained relatively constant across age groups (Fig. 2). In our study of acute Monteggia fractures in children, immediate restoration of the normal inner-epiphyseal ulna-radius ratio during surgery resulted in favorable elbow joint function outcomes and radiographic scores. In the pediatric chronic Monteggia fracture group, patients who achieved restoration of the radius-to-ulna ratio between 1.014 and 1.147 during surgery exhibited improved elbow function, joint range of motion, and radiographic scores. In contrast, inadequate restoration of this ratio resulted in poor elbow function and radiographic scores, leading to suboptimal treatment outcomes. Therefore, when performing ulna lengthening for forearm fractures, it is crucial to restore both ulna and radius lengths to the normal range through careful preoperative planning.
The inner-epiphyseal ulna-radius length ratio identified in this study can be applied in the correction of various forearm deformities in pediatric patients, including congenital radioulnar synostosis, congenital radial head dislocation, Madelung deformity, hereditary multiple exostoses, and other conditions requiring radius and ulna reconstruction. This ratio provides a foundation for extending the interosseous distance between the radius and ulna. Moreover, it offers guidance for using external frames to lengthen the distance between the ulna and radius in patients with ulnar and radial length imbalance caused by forearm epiphyseal injuries.
Although our findings are promising, we acknowledge the potential for bias. To further address this, we plan to explore the possibility of conducting a prospective multicenter study, which could offer more robust validation of the inner-epiphyseal ulna-radius length ratio.
Conclusions
A retrospective analysis was conducted on a cohort of 432 healthy children and 58 children with Monteggia fractures across four medical centers. In healthy children, the inner-epiphyseal ulna-radius length ratio ranged from 1.0336 to 1.168, with a 95% confidence interval for the medical reference range of 1.047 to 1.141. Restoring this ratio (1.047–1.141) in children with Monteggia fractures can improve elbow function and radiographic reduction quality. By adhering to appropriate ulna lengthening based on this ratio, it is possible to achieve better radiocapitellar joint reduction and favorable elbow function outcomes.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Loder, R. T. & Johnson, B. A. Changes in pediatric fracture patterns presenting to US emergency departments before, during, and after the COVID-19 pandemic. Heliyon 9 (11), e20953. https://doi.org/10.1016/j.heliyon.2023.e20953 (2023).
Antoon, S. F., Russo, S. A., Kozin, S. H. & Zlotolow, D. A. Evaluation of Monteggia fracture outcomes: Acute to Chronic. Hand (N Y). 19 (6), 961–966 (2024).
George, M. P. & Bixby, S. Frequently missed fractures in Pediatric Trauma: a Pictorial Review of Plain Film radiography. Radiol. Clin. North. Am. 57 (4), 843–855. https://doi.org/10.1016/j.rcl.2019.02.009 (2019).
Tougas, C. & Brimmo, O. Common and consequential fractures that should not be missed in children. Pediatr. Ann. 51 (9), e357–e363. https://doi.org/10.3928/19382359-20220706-05 (2022).
Samora, J. B. Distal Radius Physeal Bar and Ulnar Overgrowth: indications for treatment. J. Pediatr. Orthop. 41 (Suppl 1), S6–S13 (2021).
Arrigoni, C. & Catena, N. Chronic Monteggia in pediatric population: a narrative literature review. Pediatr. Med. Chir., 44. (2022).
Bado, J. L. The Monteggia lesion. Clin. Orthop. Relat. Res. 50, 71–86 (1967).
Rehim, S. A. et al. Monteggia fracture dislocations: a historical review. J. Hand Surg. Am. 39 (7), 1384–1394 (2014).
Gopinathan, N. R. et al. Management of missed Type-2 Monteggia Fracture Equivalent in a 9-Year-old child: a Case Report. JBJS Case Connect. 11 (1), e2000179 (2021).
Ring, D., Jupiter, J. B. & Waters, P. M. Monteggia fractures in children and adults. J. Am. Acad. Orthop. Surg. 6 (4), 215–224 (1998).
Fu, D., He, F. & Wang, D. Ulnar osteotomy between the proximal 1/3 and 1/5 provides a stable radiocapitellar joint in chronic Monteggia fracture. Transl. Pediatr. 13 (3), 427–435. https://doi.org/10.21037/tp-23-477 (2024).
Liu, Y. et al. Ulnar osteotomy and monolateral external fixator for the treatment of chronic Monteggia fractures in children: comparison between gradual and acute radial head reduction. J. Pediatr. Orthop. B. 32 (6), 583–592. https://doi.org/10.1097/BPB.0000000000001047 (2023).
Ramirez, R. N. et al. A line drawn along the radial shaft misses the capitellum in 16% of radiographs of normal elbows. J. Pediatr. Orthop. 34 (8), 763–767 (2014).
Laor, T., Clarke, J. P. & Yin, H. Development of the long bones in the hands and feet of children: radiographic and MR imaging correlation. Pediatr. Radiol. 46(4). (2016).
Rahman, M., Sharifi Renani, M., Cil, A. & Stylianou, A. P. Musculoskeletal Model Development of the Elbow Joint with an experimental evaluation. Bioengineering 5 (2), 31. https://doi.org/10.3390/bioengineering5020031 (2018).
Pineault, K. M. et al. Hox11 genes regulate postnatal longitudinal bone growth and growth plate proliferation. Biol. Open 4 (11), 1538–1548 (2015).
Abe, M. et al. Idiopathic anterior dislocation of the radial head: symptoms, radiographic findings, and management of 8 patients. J. Shoulder Elb. Surg. 28 (8), 1468–1475 (2019).
Rutkowski, P. T. & Samora, J. B. Congenital Radioulnar synostosis. J. Am. Acad. Orthop. Surg. 29 (13), 563–570 (2021).
Abzug, J. M. & Kozin, S. H. Radial longitudinal deficiency. J. Hand Surg. Am. 39 (6), 118039 (2014).
Chung, R. & Xian, C. J. Recent research on the growth plate: mechanisms for growth plate injury repair and potential cell based therapies for regeneration. J. Mol. Endocrinol. 53 (1), T45–T61 (2014).
Houshian, S. et al. Remodeling of Salter Harris type II epiphyseal plate injury of the distal radius. J. Pediatr. Orthop. 24 (5), 472–476 (2004).
Al-Qattan, M. M., Abou Al-Shaar, H. & Alkattan, W. M. Pathogenesis Congenital Radial head dislocation/subluxation Gene. 586(1): 69–76. (2016).
Yi, Y. et al. What do we need to address when we treat neglected Monteggia fracture in children. Front. Pediatr. 12:1430549. https://doi.org/10.3389/fped.2024.1430549
Wu, C., Wang, D., Mo, Y., Zhang, Z. & Ning, B. Characteristics of the length of the radius and ulna in children. Front. Pediatr. 10, 737823. https://doi.org/10.3389/fped.2022.737823 (2022).
Eamsobhana, P. & Kaewpornsawan, K. Chronic Monteggia lesions treatment with open reduction and Z-lengthening technique with annular ligament reconstruction. J. Med. Assoc. Thai/ 95(9):S47-53. (2012).
Liu, Y. et al. To angulate or not to Angulate the Ulna during the progressive distraction period performed with a Monolateral External Fixator in Paediatric patients with a chronic Monteggia fracture? Medicina. 58 (11), 1666. https://doi.org/10.3390/medicina58111666 (2022).
Funding
This study was supported by Medical Alliance Scientific Research Project of Hunan Provincial People’s Hospital (No. 2023YLT031, 2023YLT032).
Author information
Authors and Affiliations
Contributions
SF, YY, ZS, JL and QZ contribute equally to this study, they shared co-first author. SF: Conceptualization, YY: Formal analysis, ZS: Investigation, JL: Methodology, QZ: Data curation, JW: Resources, SX: Validation, YL: Supervision. JW and SX contribute equally to this study, they shared co-corresponding author. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Feng, S., Yi, Y., Song, Z. et al. Correlation between inner epiphysis ulna radius length ratio and prognosis of Monteggia fractures in children: a multicenter study. Sci Rep 15, 5195 (2025). https://doi.org/10.1038/s41598-025-89751-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-89751-1
