
Abstract
Echinococcosis poses a significant health burden in China, yet previous studies have mainly concentrated on its prevalence rather than incidence trends. This study analyzes echinococcosis incidence from 2010 to 2021 and projects future trends to enhance prevention and control strategies. The annual percentage change (APC) and average annual percentage change (AAPC) were calculated to determine temporal trends, while the time series was decomposed to assess seasonal patterns. During this period, China documented 53,141 new echinococcosis cases (excluding Hong Kong, Macao, and Taiwan), averaging 0.320 cases per 100,000 annually. The AAPC indicated a non-significant decline of -2.718%. The analysis identified two critical inflection points in 2014 and 2017, leading to three distinct trends: a non-significant decline from 2010 to 2014, a significant rise from 2014 to 2017, and a significant decrease from 2017 to 2021. Cases peaked in December, and predictions from the Seasonal Autoregressive Integrated Moving Average (SARIMA) model suggest a slight rise in incidence from September 2022 to August 2025, advising intensified efforts in preventive measures to prevent resurgence.
Similar content being viewed by others

Introduction
Echinococcosis is a globally prevalent zoonotic disease caused by the Echinococcus tapeworm. Of particular medical and public health significance are two major species: Echinococcus granulosus and Echinococcus multilocularis, which are responsible for cystic echinococcosis (CE) and alveolar echinococcosis (AE), respectively. Both diseases present significant threats to public health1. The disease course of CE is characterized by a protracted duration, often spanning several decades, and typically exhibits a low mortality rate. Conversely, if not adequately managed, AE can manifest with a mortality rate exceeding 90% within a decade2. The impact of echinococcosis extends beyond human health, contributing to substantial economic losses and a considerable disease burden on society. The global annual disease burden of CE in humans is estimated at 1,009,662 disability-adjusted life years (DALYs), which corresponds to a financial loss of approximately $763,980,979 per year. The annual disease burden attributed to AE is estimated at 666,433 DALYs3. Canids serve as definitive hosts for Echinococcus and play a pivotal role in the propagation of the echinococcosis epidemic. Ungulates, rodents, and rabbits act as intermediate hosts for Echinococcus. While humans can serve as intermediate hosts, they are typically not directly involved in the transmission cycle of CE or AE4.
CE has a global distribution, affecting all continents and over 100 countries or regions. In contrast, AE is primarily found in the Northern Hemisphere, particularly in Central Europe, significant portions of northern and central Eurasia, and certain areas of North America5. In endemic regions, the incidence of echinococcosis can surpass 50 cases per 100,000 person-years. Notably, some areas in Peru, Argentina, East Africa, and China have reported prevalence rates ranging from 5 to 10% of the population6. The annual incidence of AE is approximately 18,235 cases, with 16,629 of these occurring in China3.
China is among the countries with the highest burden of echinococcosis worldwide, encompassing a total of 370 counties where this disease is endemic7,8. The prevalence of CE and AE was the highest in western China9. A sample survey conducted from 2012 to 2016 revealed that the prevalence of echinococcosis in the population was 0.28%, demonstrating a significant decrease compared to the prevalence observed in 2004. However, it is noteworthy that the Tibet Autonomous Region still exhibited a high prevalence rate of 1.66%. Additionally, Dari County in Qinghai Province displayed an alarmingly high prevalence rate of 12.38% 10. These findings indicate that the prevention and control of echinococcosis in China continue to face challenges.
In response to the public health threats posed by echinococcosis, academic research has focused on exploring its prevalence and determinants, enhancing the understanding of the epidemic. However, an analysis of prevalence alone has limitations, as it fails to fully capture the dynamic evolution of the disease. Assessing incidence trends and making predictions have significantly advanced research in this area. The Joinpoint regression model has been widely used to analyze time trend changes in chronic and infectious diseases due to its advantages, such as precise identification of trend change points, flexibility, applicability, and intuitive result display11,12. The SARIMA model plays a significant role in the field of time series prediction, owing to its robust capabilities in handling seasonality while delivering high prediction accuracy. Armin Orang and his team effectively utilized this model to predict the incidence of influenza in Canada for the years 2019–2020, while Zhang Li and her colleagues achieved accurate predictions of the incidence of foodborne diseases in Guizhou Province13,14.
In this study, we employed three key models to analyze the incidence of echinococcosis in China (excluding Hong Kong, Macao, and Taiwan) from 2010 to 2021. The Joinpoint regression model was utilized to reveal temporal trends, while Seasonal-Trend decomposition using Loess (STL) was employed to decompose seasonal patterns and trends. Additionally, the SARIMA model was used to forecast future incidences, contextualizing findings with prior insights. This multifaceted approach provides a comprehensive understanding of disease dynamics, thereby facilitating evidence-based public health interventions.
Materials and methods
Data source
Echinococcosis data were extracted from the monthly records of notifiable infectious diseases spanning January 2010 to August 2022, as published on the official website of the National Health Commission of People’s Republic of China (http://www.nhc.gov.cn). Demographic data from the National Bureau of Statistics (2010–2022) were utilized in this study (https://www.stats.gov.cn/sj/ndsj/).
Incidence rate = number of new cases / total population × 100,000.
Joinpoint regression analysis
Joinpoint regression analysis was employed to discern temporal trends in incidence. The model was fitted by connecting multiple line segments, known as joinpoints, on a logarithmic scale. The Monte Carlo permutation method was utilized for testing, and the final model selection involved the application of the weighted Bayesian information criteria method, along with recommendations provided by the Joinpoint software. The average annual percentage change(AAPC) in echinococcosis incidence was calculated by linear regression, which was the weighted average of the annual percentage change (APC)15. APC > 0 indicating an increase in the incidence during the study period and APC < 0 indicating the opposite. If there was no connection point during the study period, we assumed that the APC = AAPC, which meant that the overall trend of the data increased or decreased without changes.
Seasonal analysis
STL is a representative time series decomposition algorithm that partitions a time series into trend, seasonal, and residual components16. By analyzing the seasonal component, it becomes possible to ascertain the seasonal patterns in the incidence of echinococcosis17.
Incidence trend prediction based on the SARIMA model
The SARIMA model was used to predict the incidence of echinococcosis. A SARIMA model is typically defined by seven parameters, expressed as SARIMA (p, d, q) (P, D, Q) S. In this notation, (p, q) indicates the order of the non-seasonal autoregressive and moving average components, respectively, while (P, Q) corresponds to the order of the seasonal autoregressive and moving average components. The variables d and D represent the number of non-seasonal and seasonal differences, respectively, and the term S denotes the periodicity of the seasonal component18. The model was fitted using monthly incidence data of echinococcosis in China from 2010 to 2021 as the training set, whereas data from January to August 2022 were utilized as the prediction set. An automated SARIMA model was applied using maximum likelihood estimation (MLE) through an automated model selection process that included unit root tests and minimized both the Akaike Information Criterion (AIC) and the Bayesian Information Criterion (BIC). To further assess the presence of residual autocorrelation, the Ljung–Box Q-test was utilized13. Predictions were generated for the incidence of echinococcosis from January to August 2022, and the predictive effect was evaluated by comparing these predictions with observed values. Additionally, the model was used to forecast the incidence of echinococcosis from September 2022 to August 2025. The Mean Absolute Percentage Error (MAPE) was employed to assess both the fitting and prediction performance of the model, with smaller values indicating superior model performance14. Specifically, a MAPE value of less than 10% signifies extremely high prediction accuracy, between 10% and 20% indicates good prediction capability, between 20% and 50% suggests acceptable prediction accuracy, and a value exceeding 50% indicates unacceptable prediction accuracy19. The expression for MAPE is:
Where, yi represents the actual value, ŷi represents the predicted value, and n represents the number of data points.
Statistical analysis
The heatmap production was implemented using the “pheatmap” package in R software (version 4.2.1). The STL procedure was conducted through R software. The SARIMA prediction model construction utilized the “tseries” and “forecast” packages in the R software. Joinpoint regression analysis was performed using the joinpoint regression program software (version 5.2.0). The test level was α = 0.05.
Result
Incidence and mortality of echinococcosis
From 2010 to 2021, a total of 53,141 new cases of echinococcosis were reported in China (excluding Hong Kong, Macao, and Taiwan), resulting in an average annual incidence rate of 0.320 per 100,000 individuals, with rates ranging from 0.242 to 0.494 per 100,000 individuals annually. The highest number of cases was recorded in 2017, with a total of 6,910 cases (incidence: 0.494 per 100,000 individuals). Conversely, the lowest number of cases was observed in 2021, with only 3,425 cases (incidence: 0.242 per 100,000 individuals). In addition to incidence trends, the mortality rate associated with echinococcosis in China during the same period was examined. A total of 14 patient deaths were recorded over 12 years, resulting in an average annual mortality rate of 0.0000843 per 100,000 individuals.
Furthermore, the monthly incidence of echinococcosis exhibited fluctuations ranging from 0.006 to 0.079 per 100,000 individuals. The construction of a heat map based on the monthly incidence data spanning from 2010 to 2021 (as shown in Fig. 1) revealed that the occurrence of echinococcosis remained consistently high throughout 2017, with December identified as the month with the highest annual incidence rate.

Heat map of monthly incidence distribution of echinococcosis.
Temporal trend characteristics
Joinpoint regression analysis showed that the incidence of echinococcosis in China decreased from 2010 to 2021, with AAPC of -2.718% (95% CI: -7.284 ~ 0.957%, P = 0.085). The entire time period exhibited two points of inflection, which occurred in 2014 and 2017, thereby dividing the interval into three distinct segments. From 2010 to 2014, the APC was − 4.065% (95% CI: -25.159%~10.497%, P = 0.221), but it was not significant. From 2014 to 2017, the APC was 19.868% (95% CI: 5.240%~36.408%, P = 0.016). From 2017 to 2021, the APC was − 15.650% (95% CI: -33.786%~-8.772%, P = 0.006) (Fig. 2 presents the results of the Joinpoint regression analysis).

Joinpoint regression trend.
Seasonal pattern
The STL algorithm effectively segmented the time series into trend, seasonal, and residual components. The seasonal component, as shown in Fig. 3, revealed a consistent pattern in echinococcosis incidence, with annual peaks occurring during the winter months, specifically in December of each year (also visible in Fig. 1).

Time series analysis of the incidence of Echinococcosis in 2020-2021, where (A) is the time series, (B) is the trend term, (C) is the periodic term, and (D) is the disturbance term.
Incidence trend prediction
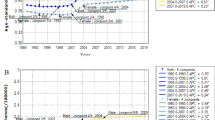
The monthly incidence data of echinococcosis in China from 2010 to 2021 served as the training dataset, while data from January to August 2022 constituted the prediction set for a comparative analysis of actual incidence rates. The stationarity of the data was assessed using the Augmented Dickey-Fuller (ADF) test, which revealed that the data were stationary (t = -3.45, p < 0.05). Through an automatic model selection process, the final fitted model identified was ARIMA (1,0,3) (1,0,0) [12], with minimum values for both the AIC (-984.6) and the BIC (-960.85). The model statistics indicated that the p-values of the Ljung-Box test were 0.937, exceeding 0.05, suggesting that no significant residual information remained. The fitting results indicated that all actual values fell within the 95% confidence intervals of the predicted values. The predicted results aligned with the actual trend and showed similar values, indicating a good fit of the model. The MAPE between the actual and predicted values was 10.420%, suggesting favorable predictive performance of the model (Table S1, Fig. 4). Subsequently, this model was employed to forecast the incidence of echinococcosis for a period of 36 months from September 2022 to August 2025. The results are presented in Table 1; Fig. 5, showing that the monthly incidence rate exhibited a slight upward trend, fluctuating within the range of 0.019 to 0.026 per 100,000 individuals.

Time series of actual and predicted incidence of echinococcosis from January to August 2022.

Prediction of echinococcosis incidence.
Discussion
This study reveals that the average incidence of echinococcosis in China from 2010 to 2021 was 0.320 per 100,000 individuals, with the lowest rate recorded at 0.242 per 100,000 in 2021. This figure surpasses the incidence of 0.15 per 100,000 individuals observed in European Union (EU) countries20, indicating that there is still room for further improvement in the prevention and control of echinococcosis in China. Another study has shown that between 2004 and 2013, the average incidence rate of echinococcosis in China was 0.18 per 100,000, demonstrating a significant increasing trend (APC = 24.0%, 95% CI: 12.0–37.2%, P < 0.05)21. From 2004 to 2019, the average incidence rate of echinococcosis rose to 0.228 per 100,000, with an overall trend of initially increasing and then decreasing, peaking in 2017 22. This trend aligns well with the findings of our study, further confirming the prevalence of echinococcosis in China in recent years. It is noteworthy that, despite a decrease in the incidence rate of echinococcosis between 2019 and 2021, it still remains higher than the average for the period from 2004 to 2019. This indicates that the prevention and control efforts for echinococcosis in China continue to face significant challenges. Moreover, the incidence of echinococcosis varies greatly among provinces (cities and autonomous regions) in China. Studies have indicated that the incidence in southern Xinjiang and Qinghai Province is significantly higher than the national average23,24. In contrast, Yunnan Province, while being an endemic area for echinococcosis, has an incidence rate that is considerably lower than the national average25. The prevention and control of echinococcosis in Xinjiang and Qinghai Province still faces challenges.
Over the period from 2010 to 2021, the incidence of echinococcosis displayed a general downward trend, albeit at a gradual pace. Notably, the proactive initiation of the echinococcosis prevention and control program by the Chinese government in 2005 has led to noteworthy achievements, resulting in a measurable containment of the disease’s spread. However, despite these efforts, the increasing intensity of screening activities, coupled with the adoption of advanced diagnostic techniques, has led to the identification of a higher number of echinococcosis patients26,27. This observation underscores the fact that, while progress has been made, the disease remains prevalent in certain populations. Moreover, a persistent challenge lies in stemming the transmission of echinococcosis among wild canids, primarily due to the limited availability or inefficiency of effective intervention strategies. This obstacle highlights the need for further research and innovation in this area. Given the aforementioned factors, it is evident that, despite the implementation of various prevention and control measures, there has not been a marked reduction in the prevalence of echinococcosis. This underscores the complexity of the disease and the need for a comprehensive, multifaceted approach to tackle it effectively.
The trend from 2010 to 2014 remained consistent with the overall pattern observed throughout the study period, displaying a non-significant decrease in incidence. Notably, the implementation of the National Action Plan for Echinococcosis Control (2011–2015) yielded incremental success in both dog and patient management, consequently leading to an increase in cases detected through screening27. The incidence of echinococcosis increased significantly from 2014 to 2017. In 2016, the Chinese Center for Disease Control and Prevention carried out echinococcosis screening in nine provinces (autonomous regions), including Inner Mongolia, Sichuan, Tibet, Shaanxi, Gansu, Qinghai, Ningxia, Yunnan, and Xinjiang (including the Xinjiang Production and Construction Corps). Additionally, since 2016, the national echinococcosis surveillance system has been established, and these measures have facilitated the progressive identification of echinococcosis cases, resulting in an escalating incidence rate10,27.
The incidence of echinococcosis exhibited a significant declining trend from 2017 to 2021, which aligns with the findings reported by Kui Yan et al.28. The Tibet Autonomous Region has the highest prevalence of echinococcosis. In the period from 2017 to 2019, the regional government implemented a comprehensive three-year prevention and control strategy for echinococcosis, resulting in a significant reduction in transmission risk29. Due to the effective implementation of comprehensive prevention measures, the incidence of echinococcosis in Xinjiang has decreased since 2017 23. The period from 2015 to 2018 saw the implementation of an integrated prevention and control project in Shiqu County, which included comprehensive patient treatment and host management strategies, leading to initial successes in controlling the disease source30. Simultaneously, as a result of implementing the “National Echinococcosis and Other Key Parasitic Disease Control Plans (2016–2020),” coupled with intensified government efforts in prevention and control measures against echinococcosis and successful policy implementations, a declining trend in the incidence of echinococcosis has been observed in high-risk areas such as Qinghai Province, Sichuan Province, and the Tibet Autonomous Region31.
Throughout the study period, the incidence of echinococcosis peaked in 2017. Two possible reasons for this phenomenon can be identified. Firstly, Xinjiang included echinococcosis in the national physical examination starting from that year, effectively expanding screening coverage and enhancing population detection rates23. Secondly, in 2017, the Tibet Autonomous Region conducted a comprehensive screening program targeting the entire population, achieving a coverage rate of over 90%. This extensive screening effort led to the highest detection rate of echinococcosis recorded29. The incidence of echinococcosis in 2021 reached its lowest point, largely attributed to the continuous decline observed since 2017, which can be primarily credited to the Chinese government’s unwavering commitment towards addressing this issue and implementing a comprehensive set of preventive and control measures.
This study also revealed that the peak incidence of echinococcosis consistently occurred in December each year, which can be attributed to the winter slaughter season observed in pastoral areas from November to December. During this period, domestic canines are at a heightened risk of infection due to their exposure to infected organs. Furthermore, empirical evidence suggests that domestic canines may exhibit heightened exposure to small mammalian species during the onset of winter, consequently leading to a substantial escalation in susceptibility to Echinococcus infection32,33. Foxes serve as the predominant definitive hosts for Echinococcus multilocularis, with their AE infections peaking during winter. Additionally, a significant positive correlation exists between the occurrence of human AE and the prevalence of foxes34,35,36. Research has also demonstrated that both AE infection in small mammals and CE infection in cattle exhibit a winter peak37,38, mirroring the potential seasonal pattern observed in human infections as intermediate hosts. The winter-induced decline in human immune function is likely to expedite the progression of Echinococcus tapeworm infection within the body, leading to the manifestation of associated clinical symptoms39. Furthermore, given the heightened prevalence of respiratory ailments during this season, patients may be identified through more frequent hospital admissions even before symptom onset40,41. Based on the consolidation of echinococcosis control effectiveness, this study recommends that relevant departments rigorously implement canid deworming measures during winter. Strengthening grassland management and implementing effective control measures for small rodent populations are also advised. Additionally, facilitating the establishment of centralized slaughterhouses while developing standardized regulations will ensure proper management practices within these facilities. This will enable the safe disposal of infected organs and prohibit their use as feed for dogs. In winter, enhancing nutritional intake, engaging in appropriate physical activity, and bolstering the body’s immune response are essential.
The SARIMA model has a simple structure, requires only morbidity information for prediction, is highly feasible, and has been widely used in healthcare42. Furthermore, research has demonstrated that the automated SARIMA model exhibits greater robustness in time series predictions compared to the manual SARIMA model13. The prediction results were largely consistent with observed trends, showing similar values. Additionally, the MAPE between the actual and predicted values was calculated to be 10.420%. The results indicated that the model displayed a strong fitting effect and had the capability to accurately forecast future incidences of echinococcosis. Based on the projected incidence, it is expected that the prevalence of echinococcosis will experience a slight increase from September 2022 to August 2025. By further strengthening prevention and control measures while consolidating existing effectiveness, it is anticipated that future incidences can be reduced.
Despite these advancements, this study exhibits several limitations. Firstly, the lack of comprehensive sociodemographic data and the absence of stratified analyses constrain our ability to explore the unique pathogenic characteristics of echinococcosis within the Chinese context. Although this study was unable to obtain these data, preventing further analysis of the epidemiological characteristics of echinococcosis across different populations in China, we conducted a preliminary exploration of this variability by introducing an analysis of echinococcosis in Tibet Autonomous Region. Our research findings indicate that between 2019 and 2023, the incidence of echinococcosis in females in Tibet Autonomous Region was significantly higher than that in males, with the incidence in the ≥ 60 years age group being notably higher than in other age groups, and showing a significant increasing trend from younger to older age groups (Table S2). This analysis suggests that there are indeed significant differences in the incidence of echinococcosis among populations of different genders and age groups. In future studies, we will endeavor to obtain more data on the sociodemographic characteristics of patients and conduct in-depth analyses of the associations between these factors and the incidence of echinococcosis. Secondly, the lack of specific incidence data at the provincial (city and autonomous region) level poses challenges in accurately assessing regional variations in disease burden and evaluating the impact of prevention and control strategies across diverse geographical areas. Finally, we acknowledge that potential issues within the reporting system, such as underreporting and misreporting, may lead to discrepancies between the reported incidence figures and the true prevalence of echinococcosis28. To address this issue, we propose several measures: firstly, conducting rigorous review and validation of data during the collection phase to ensure its accuracy and completeness. Secondly, strictly adhering to the diagnostic procedures for echinococcosis to minimize misreporting. Additionally, we recommend introducing automated data input tools to reduce human errors and omissions, while also providing regular training for data input personnel to enhance their accuracy and sense of responsibility. Lastly, we suggest establishing a data quality monitoring platform that visually displays cases of underreporting, enabling managers to take swift action.
Conclusion
From 2010 to 2021, the incidence of echinococcosis in China exhibited a general decline, albeit at a relatively gradual pace, with notable inflection points occurring in 2014 and 2017. The incidence initially increased before experiencing a subsequent decrease. Despite these successes, echinococcosis continues to represent a significant public health concern. Seasonal peaks noted in December highlight the necessity for targeted prevention efforts during the winter months. Projections indicate a slight increase in incidence from 2022 to 2025, underscoring the imperative for relevant departments to enhance their prevention and control strategies to effectively mitigate the risk of resurgence.
Data availability
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
References
McManus, D. P., Zhang, W., Li, J. & Bartley, P. B. Echinococcosis. Lancet 362, 1295–1304. https://doi.org/10.1016/s0140-6736(03)14573-4 (2003).
Zheng, C. et al. National Alveolar Echinococcosis distribution - China, 2012–2016. China CDC Wkly. 2, 1–7 (2020).
Torgerson, P. R., Keller, K., Magnotta, M. & Ragland, N. The global burden of alveolar echinococcosis. PLoS Negl. Trop. Dis. 4, e722. https://doi.org/10.1371/journal.pntd.0000722 (2010).
Wen, H. et al. Echinococcosis: Advances in the 21st century. Clin. Microbiol. Rev. 32 https://doi.org/10.1128/cmr.00075-18 (2019).
Eckert, J. & Deplazes, P. Biological, epidemiological, and clinical aspects of echinococcosis, a zoonosis of increasing concern. Clin. Microbiol. Rev. 17, 107–135. https://doi.org/10.1128/cmr.17.1.107-135.2004 (2004).
Pham, H., Kupshik, D., Kin, C. & Romano, P. Cystic echinococcosis. Appl. Radiol. 48, 42–43 (2019).
Xiao, N. Concept and mechanism innovations provide a sustainable driver for echinococcosis control in China]. Zhongguo Xue Xi Chong Bing Fang Zhi Za Zhi. 33, 329–333. https://doi.org/10.16250/j.32.1374.2021188 (2021).
Wang, L. Y. et al. Societal drivers of human echinococcosis in China. Parasit. Vectors. 15, 385. https://doi.org/10.1186/s13071-022-05480-8 (2022).
Wang, Z., Wang, X. & Liu, X. Echinococcosis in China, a review of the epidemiology of Echinococcus spp. Ecohealth 5, 115–126. https://doi.org/10.1007/s10393-008-0174-0 (2008).
Wu, W. P. et al. Sampling Survey Analysis of Echinococcosis in China from 2012 to 2016. Chin. J. Parasitol. Parasitic Dis. 36, 1–14 (2018).
Yang, A. et al. Trends in all-cause and cause-specific mortality in older adults with and without diabetes: a territory-wide analysis in one million older adults in Hong Kong. Diabetes Res. Clin. Pract. 210, 111618. https://doi.org/10.1016/j.diabres.2024.111618 (2024).
Molnar, A., Iancu, M., Radu, R. & Borzan, C. M. A joinpoint regression analysis of Syphilis and Gonorrhea Incidence in 15-19-year old adolescents between 2005 and 2017: A regional study. Int. J. Environ. Res. Public. Health 17 https://doi.org/10.3390/ijerph17155385 (2020).
Orang, A. et al. Forecasting seasonal influenza activity in Canada-Comparing seasonal auto-regressive integrated moving average and artificial neural network approaches for public health preparedness. Zoonoses Public. Health. 71, 304–313. https://doi.org/10.1111/zph.13114 (2024).
Zhang, L. et al. Construction of Prediction Model of Foodborne Disease outbreaks and its Trend Prediction - Guizhou Province, China, 2023–2025. China CDC Wkly. 6, 408–412. https://doi.org/10.46234/ccdcw2024.079 (2024).
Li, R., Yuan, X. & Ou, Y. Global burden of rheumatoid arthritis among adolescents and young adults aged 10–24 years: a trend analysis study from 1990 to 2019. PLoS One. 19, e0302140. https://doi.org/10.1371/journal.pone.0302140 (2024).
Yao, T. et al. Deep evolutionary fusion neural network: A new prediction standard for infectious disease incidence rates. BMC Bioinform. 25 https://doi.org/10.1186/s12859-023-05621-5 (2024).
Song, Y. J. & Choi, H. Seasonality of syphilis in males through the 2011 to 2019 mandatory surveillance period: a cross-sectional study in South Korea. Med. (Baltim). 102, e36723. https://doi.org/10.1097/md.0000000000036723 (2023).
Kim, J. et al. Predicting antimicrobial resistance of bacterial pathogens using time series analysis. Front. Microbiol. 14, 1160224. https://doi.org/10.3389/fmicb.2023.1160224 (2023).
Cutrera, R. et al. Epidemiology of respiratory syncytial virus in a large pediatric hospital in Central Italy and development of a forecasting model to predict the seasonal peak. Ital. J. Pediatr. 50, 65. https://doi.org/10.1186/s13052-024-01624-x (2024).
The European Union One Health. Zoonoses report. Efsa J 20, e07666. https://doi.org/10.2903/j.efsa.2022.7666 (2022).
Yang, S. et al. Epidemiological features of and changes in incidence of infectious diseases in China in the first decade after the SARS outbreak: an observational trend study. Lancet Infect. Dis. 17, 716–725. https://doi.org/10.1016/s1473-3099(17)30227-x (2017).
Chen, C. et al. Zoonotic outbreak risk prediction with long short-term memory models: a case study with schistosomiasis, echinococcosis, and leptospirosis. BMC Infect. Dis. 24, 1062. https://doi.org/10.1186/s12879-024-09892-y (2024).
Zhang, Y. et al. Prevalence and spatial distribution characteristics of human echinococcosis: a county-level modeling study in southern Xinjiang. China Heliyon. 10, e28812. https://doi.org/10.1016/j.heliyon.2024.e28812 (2024).
Cai, J. et al. The impact of echinococcosis interventions on economic outcomes in Qinghai Province of China: evidence from county-level panel data. Front. Vet. Sci. 10, 1068259. https://doi.org/10.3389/fvets.2023.1068259 (2023).
Zi, J. R. et al. Epidemiological survey of cystic echinococcosis in southwest China: from the Qinghai-Tibet plateau to the area of Yunnan. World J. Hepatol. 16, 229–240. https://doi.org/10.4254/wjh.v16.i2.229 (2024).
Gu, H. et al. China’s prevention and control experience of echinococcosis: a 19-year retrospective. J. Helminthol. 98, e16. https://doi.org/10.1017/s0022149x24000014 (2024).
Yu, Q., Xiao, N., Han, S., Tian, T. & Zhou, X. N. Progress on the national echinococcosis control programme in China: analysis of humans and dogs population intervention during 2004–2014. Infect. Dis. Poverty. 9, 137. https://doi.org/10.1186/s40249-020-00747-7 (2020).
Kui, Y. et al. Analysis of Epidemiological and Issues encountered in Case reports on echinococcosis - China, 2022. China CDC Wkly. 6, 100–104. https://doi.org/10.46234/ccdcw2024.022 (2024).
Wang, L. et al. Assessment of echinococcosis control in Tibet Autonomous Region, China. Infect. Dis. Poverty. 11, 59. https://doi.org/10.1186/s40249-022-00987-9 (2022).
Liu, L. et al. Epidemiological analysis of cystic echinococcosis and alveolar echinococcosis in an extremely high prevalence region: Population-based survey and host animal monitoring in Shiqu County, China. Acta Trop. 221, 105982. https://doi.org/10.1016/j.actatropica.2021.105982 (2021).
Gong, Q. L. et al. Meta-analysis of the prevalence of Echinococcus in dogs in China from 2010 to 2019. PLoS Negl. Trop. Dis. 15, e0009268. https://doi.org/10.1371/journal.pntd.0009268 (2021).
Amarir, F. E. et al. Cystic echinococcosis in three locations in the Middle Atlas, Morocco: estimation of the infection rate in the Dog Reservoir. Vector Borne Zoonotic Dis. 20, 436–443. https://doi.org/10.1089/vbz.2019.2538 (2020).
Wang, Q. et al. Seasonal pattern of Echinococcus re-infection in owned dogs in tibetan communities of Sichuan, China and its implications for control. Infect. Dis. Poverty. 5, 60. https://doi.org/10.1186/s40249-016-0155-4 (2016).
Abdykerimov, K. K. et al. Environmental distribution of Echinococcus- and Taenia spp.-contaminated dog feces in Kyrgyzstan. Parasitology 151, 84–92. https://doi.org/10.1017/s003118202300118x (2024).
Otero-Abad, B., Rüegg, S. R., Hegglin, D., Deplazes, P. & Torgerson, P. R. Mathematical modelling of Echinococcus Multilocularis abundance in foxes in Zurich, Switzerland. Parasit. Vectors. 10, 21. https://doi.org/10.1186/s13071-016-1951-1 (2017).
Antolová, D. et al. Human alveolar echinococcosis in Slovakia: Epidemiology and genetic diversity of Echinococcus Multilocularis, 2000–2023. PLoS Negl. Trop. Dis. 18, e0011876. https://doi.org/10.1371/journal.pntd.0011876 (2024).
Liccioli, S., Kutz, S. J., Ruckstuhl, K. E. & Massolo, A. Spatial heterogeneity and temporal variations in Echinococcus multilocularis infections in wild hosts in a north American urban setting. Int. J. Parasitol. 44, 457–465. https://doi.org/10.1016/j.ijpara.2014.03.007 (2014).
Yang, X. B. et al. Meta-analysis of the prevalence of bovine cystic echinococcosis in China during decade. Res. Vet. Sci. 152, 465–475. https://doi.org/10.1016/j.rvsc.2022.09.004 (2022).
Baker, R. E., Yang, W., Vecchi, G. A., Metcalf, C. J. E. & Grenfell, B. T. Assessing the influence of climate on wintertime SARS-CoV-2 outbreaks. Nat. Commun. 12, 846. https://doi.org/10.1038/s41467-021-20991-1 (2021).
Azziz Baumgartner, E. et al. Seasonality, timing, and climate drivers of influenza activity worldwide. J. Infect. Dis. 206, 838–846. https://doi.org/10.1093/infdis/jis467 (2012).
Yang, F. et al. A combination of annual and nonannual forces drive respiratory disease in the tropics. BMJ Glob. Health 8. https://doi.org/10.1136/bmjgh-2023-013054 (2023).
Gao, Q. et al. Epidemiological characteristics and prediction model construction of hemorrhagic fever with renal syndrome in Quzhou City, China, 2005–2022. Front. Public. Health. 11, 1333178. https://doi.org/10.3389/fpubh.2023.1333178 (2023).
Acknowledgements
We would like to extend our sincere thanks to the contributing authors and reviewers for their dedication and hard work.
Author information
Authors and Affiliations
Contributions
All authors designed the study. J.J.A. prepared and analysed the data and wrote the draft manuscript. All authors contributed to interpretation of findings, and reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ai, J., Zheng, J., Zhu, C. et al. Analysis and prediction of the incidence temporal trends of echinococcosis in China from 2010 to 2021. Sci Rep 15, 6423 (2025). https://doi.org/10.1038/s41598-025-90207-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-90207-9
Keywords
This article is cited by
-
Pulmonale Echinokokkose
Zeitschrift für Pneumologie (2025)
