
Abstract
Telomeric repeat-containing RNAs (TERRAs) are expressed from subtelomeric regions, as long non-coding RNAs responsible for maintaining telomere length and stabilizing the genome. After TERRA is transcribed (f-TERRA) from subtelomere regions, it hybridizes (h-TERRA) into telomeres and intergenic regions to maintain genome and telomere stability. Here, we separately determine changes in two TERRA fractions, f-TERRA and h-TERRA levels in relation to telomere length (TL) in first time meningioma patients with preoperative and postoperative comparisons with the control group. Since there is a lack of established biomarkers for monitoring meningiomas despite their high prevalence among primary brain tumors, this study was designed. Fifty patients and 44 healthy controls were included in this study. Real-time quantitative PCR (q-PCR) reactions were performed to determine telomere length (TL), f-TERRA and h-TERRA levels. Statistically significant differences were observed between the levels of f-TERRA, h-TERRA, telomere length (TL), compared with the healthy control group and patients. When postoperative blood h-TERRA levels were compared between the patient group and the control group, no statistically significant differences were observed. However, in the correlation analysis between postoperative tumor volume and postoperative blood h-TERRA levels, a positive, moderate and statistically significant relationship was found. This study highlights the importance of presenting the results by means of preoperative and postoperative comparisons of meningiomas. Based on the available information, we suggest that the levels of f-TERRA and h-TERRA could also be potential biomarkers for diagnostic, therapeutic, and following of meningiomas.
Similar content being viewed by others


Introduction
Meningiomas are slowly growing, primarily benign tumors that arise from cells of the arachnoid cap. They constitute 13–30% of all primary brain tumors and 25% of spinal cord tumors1,2. Several treatment options are considered, but frequent recurrences and adverse effects of treatment constitute major problems3. Additionally, depending on the position and the size of the growing cell foci; there is a risk of progressive malignancy and tumor recurrence4. Additional studies are essential to define the stages of their progressive malignant transformation, identify the biomarkers (TERT, TRAF7, BAP1, PTEN etc.) involved in tumor progression to consider treatment mechanisms, and understand their potential adverse effects.
To trace the progressive steps toward malignancy, here we focus on telomeres as molecular tools already known to be altered during tumor development. Telomeres are the end regions of chromosomes that contain a complex structure of hybrid DNA/RNA and proteins (i.e. Shelterin)5. Telomeres provide genome stability at the ends of chromosomes in eukaryotes, ensure chromosome placement, and regulate cell lifespan.
Telomerase (non-coding RNA TERC + protein TERT) maintains the length of chromosome ends and thus ensures the continued and safe proliferation of cells. However, even in slow-growing meningiomas, telomeres shorten as cells divide, and once they become critically short, cell division ceases. The ends of chromosomes become vulnerable, and cells die. On the other hand, it is also observed that in most human cancers, telomerase is activated6.
Activation of the telomere maintenance mechanism leads to cellular immortality, a condition that has been identified as one of the key characteristics of cancer cells7,8. Tumors use two types of telomere maintenance mechanisms: one is based on telomerase activity, and the other is a telomerase-independent mechanism of alternative lengthening telomere (ALT)9. Decreased telomerase activity results in shortening of telomeres with each cell cycle, thereby limiting cell division and proliferation in most non-neoplastic tissues10. To date, numerous studies have examined the relationship between cancer prognosis and telomere homeostasis and concluded that differences in telomere length (TL) or telomerase activity are associated with metastatic progression of tumors. Telomere homeostasis has been recognized as a critical determinant of the metastatic capacity of cancer cells11. Recently transcriptional activity from telomeric regions has been observed producing Telomeric Repeat Containing RNA (TERRA), which is a long non-coding RNA (lncRNA), functional to maintain TL and genome stability12. TERRA is a transcript expressed from all subtelomeric and telomeric repeat sequences by RNA polymerase II and has been found as free TERRA molecules (f-TERRA) and as DNA/RNA hybrids in all eukaryotes tested to date13. In human cells, TERRA is expressed at the G1-S transition and its expression level reaches its highest level in S phase. Then, its expression decreases again towards the end of the S phase as cells complete their replication and pass to the G2 and M phases of the cell cycle. However, some expressed TERRAs remain in telomeric regions and forms DNA-RNA hybrids. The levels of TERRA are controlled both transcriptionally by its promoters in the CpG islands-rich subtelomeric region, via the regulation of DNA-RNA hybrids of TERRA molecules and post-transcriptionally14. The TERRA function is therefore at the level of expression and localization. Although the expression level of f-TERRA could be normal, the levels of TERRA as DNA/RNA hybrids (h-TERRA) can vary and is therefore crucial15.
Studies have shown that both increases and decreases in f-TERRA levels are closely associated with TL regulation, reflecting disruptions in telomere homeostasis that can lead to genomic instability, uncontrolled cell division, or cellular aging12. However, no studies have reported TERRA (f-TERRA and h-TERRA) levels in steps of slow growing cells in meningioma patients12. Here, we track TERRA levels in two RNA fractions, TERRA extracted from total free fraction (f-TERRA) and DNA/RNA hybrids (h-TERRA), from different histopathological tumor grades of meningioma cells in relation to changes in TL over time from the preoperative period to the postoperative period in blood and tissue samples. The primary research question guiding this study asks whether the levels of f-TERRA and h-TERRA can serve as reliable biomarkers for monitoring meningioma patients in relation to TL and tumor progression. The study specifically investigates the variations in these biomarkers in blood between preoperative and postoperative phases and examines their association with key clinical variables such as tumor volume, histopathological grade, presence of systemic diseases, peritumoral edema, and the extent of surgical resection.
Methods
Selection of patients and control group and evaluated parameters
Gazi University Clinical Research Ethics Committee approved this prospective cohort study, dated 29.11.2021, with the decision number 21/128. All participants signed an informed consent form before joining the study. This research has been performed in accordance with the Declaration of Helsinki and its later amendments.
Fifty patients who were diagnosed with tumors compatible with intracranial meningiomas and pathologically confirmed to have meningioma after surgery, and 44 completely healthy individuals who agreed to participate in the study and were matched with the patients in terms of age and gender were included in the study as a control group.
Clinical findings of the patients, such as age, gender, systemic disease, and radiosurgery/surgery history, were recorded in the preoperative period. In addition, tumor localizations, presence of peritumoral edema, severity of peritumoral edema, number of tumors and tumor volumes of the patients whose preoperative radiological images were examined were determined.
Peritumoral edema severity was evaluated at 3 degrees. Edema smaller than the tumor volume was considered 1st degree, edema larger than the tumor volume and limited to a single lobe was considered 2nd degree, and widespread edema affecting more than one lobe was considered 3rd degree edema.
In the postoperative period, histopathological subtype, tumor grade, and Simpson Grade were determined. During the patient follow-up at approximately 6 months, postoperative radiosurgery/surgery history, residual status, residual tumor volume and edema were evaluated.
Tumor volume measurement method
Contrast-enhanced cranial MR images were uploaded to the 3D Slicer 5.2.2 16 program with the ‘DICOM (digital imaging and communications in medicine)’ format. Preoperative and postoperative tumor volumes were segmented manually by a single investigator after the images were standardized (Fig. 1).

Axial, coronal, sagittal and 3D images of the tumor segmented in the 3D Slicer program.
Collection of blood and tissue samples
The patients’ blood was taken into 2 tubes with EDTA in the preoperative period. Blood samples of healthy controls matched for age and gender with patients were collected into 2 tubes with EDTA. Tumor tissues taken during the intraoperative period were placed in 1.5 ml Eppendorf tubes and then Trizol (Biorad, USA, CA, Cat No: 7326890) was added and placed in the − 800C freezer. Then, it was transferred under appropriate temperature conditions. Blood samples were taken from patients again at 6 months after surgery to assess f-TERRA, h-TERRA levels, and TL. Firstly, DNA and total RNA samples were isolated from tissue and blood samples. Hybrid RNA samples were isolated from the DNA samples obtained. f-TERRA levels were determined from total RNA samples, and h-TERRA levels were determined from hybrid RNA samples isolated from DNA.
Total RNA isolation
The collected tissues with Trizol were used for RNA isolation. Tissues were homogenized with a 2 ml syringe. For blood samples, 500 µl Trizol (Biorad, USA, CA, Cat No: 7326890) were added into 500 µl blood samples. Subsequently, total RNA isolation was carried out according to our previous study and the manufacturer’s instructions17.
DNA isolation from blood and tumor tissue
After RNA was isolated, all remaining blood samples were taken into a 50 ml falcon and Red Cell Lysis, three times the blood volume, was added. After vortexing thoroughly, it was kept at + 4 °C for 20 min. It was then centrifuged at 4000 rpm for 20 min. After centrifugation, the supernatant was decanted. Then, 2 times the initial blood volume of Red Cell Lysis was added. Then, it kept at + 4 °C for 10 min and centrifuged at 4000 rpm for 10 min. After centrifugation, the supernatant was discarded and the pellet was cleared, then Cell Lysis buffer and 80 µl proteinase K equal to the first blood volume were added and incubated at 37 °C overnight. The next day, DNA isolation was performed according to manual ammonium acetate method. For tumor tissue, each tissue was placed in 600 µl Cell Lysis Buffer containing 1 M Tris, 14% SDS, 0.1 M EDTA and Proteinase K and vortexed thoroughly. It was then incubated at 56 °C overnight. The next day, two Eppendorf tubes were prepared for each tissue, and 300 µl was dispensed into each Eppendorf tube from the tissue we incubated overnight, one tube for DNA isolation and one tube for DNA: RNA hybrid isolation. Then, DNA isolation was performed according to manual ammonium acetate method. Then, DNA: RNA hybrids concentrations were determined by measuring on the NanoDrop device (Shimadzu, Cat No: 2062630042; Kyoto, Japan)18.
DNA-RNA hybrid isolation
75 µl DNA Digestion Buffer and 5 µl DNase was added to each of the DNA samples isolated from blood and tissues in the previous steps and vortexed for 10–15 s. Then, it was incubated at room temperature for 15 min. After incubation, 300 µl Trizol and 180 µl chloroform were added and vortexed for 10 s. Then, all the other procedures were performed according to the manufacturer’s instructions. Then, DNA: RNA hybrids concentrations were determined by measuring on the NanoDrop device18.
cDNA synthesis
Isolated total RNA and DNA-RNA hybrid samples are reverse transcribed into complementary DNA (cDNA) using Evoscript universal cDNA master kit (Roche, Germany, Mannheim, Cat No: 07912439001) in final reaction volumes of 20 µL. All reactions were performed as specified in the manufacturer’s protocol. All these steps were carried out in a single cycle. cDNA samples were stored at -80oC until they were run in Q-PCR18.
Q-PCR
Quantitative real-time PCR reactions (q-PCR) were performed using the High-throughput Light Cycler 480 II Real-Time PCR system (Roche, Germany, Mannheim). cDNAs were diluted with nuclease free water in 1:5 ratios. Syber Green Master (Roche, Germany, Mannheim, Cat No: 04707516001) was used to determine TERRA levels in total RNA and DNA-RNA hybrids.
The reaction mix was prepared according to the manufacturer’s instructions. All samples were runduplicate and Human beta-actin (ACTB) was used as the reference gene. Changes in f-TERRA and h-TERRA levels were determined using the 2−ΔΔCt method of relative quantification in all groups. The primers used in the study are listed in (Supplemental Table 1)18.
TL measuring
For the determination of TL using DNA isolated from tissues and bloods, the telomere standard and 36B4 standard were calculated by Real Time PCR method using the Syber Green I Master mix (Roche, Germany) kit via telomere and 36B4 primers, given in the (Supplemental Table 1). Two separate mixes for the number of samples and standards were created in separate tubes for telomeres and 36B4 primers. The reaction mix was prepared according to the previous study and the manufacturer’s instructions. Six separate standard series were created by diluting stock telomere and 36B4 standards. 1 µl PGL3 Basic Vector (Promega, USA, Cat No: E1751) plasmid was put into all standards prepared. After the reaction mix was distributed into the wells, 4 µl of the prepared standards were added sequentially. Thermal cycling conditions were set according to the manufacturer’s protocol. The standard curve was drawn with Ct’s obtained for telomere standard and 36B4 standard obtained because of PCR. Using the method suggested by18,19, TL was calculated with the Ct’s of each tissue.
Statistical analysis
In evaluating the data obtained in the study, “statistical package for social sciences” (SPSS) software package version 23.0 (New York, NY) was used for statistical analysis. In the analyses, descriptive statistics were expressed as numbers and percentages, and distribution statistics were expressed as mean, standard deviation, median, smallest and largest value. The compliance of continuous variables with normal distribution was checked by visual (histogram and probability graphs) and analytical methods (skewness, kurtosis values and Shapiro Wilk test and coefficient of variation). For categorical variables, differences between groups were evaluated with the Chi-Square test. Analysis of continuous variables and categorical variables that were not found to be normally distributed were evaluated with the Mann-Whitney U test. Analysis of continuous variables of dependent groups that were not found to be normally distributed was evaluated with the Wilcoxon paired two-sample test. In cases where there were more than two groups, the Kruskal Wallis test was used when parametric test assumptions were not met. In the group analysis that creates differences between groups, Mann-Whitney U test was used in pairwise comparisons when parametric test assumptions were not met. To test the compatibility between continuous variables, first the suitability for normal distribution was evaluated, it was seen that it did not comply with the normal distribution, and then Spearman correlation analysis was performed. According to Cohen’s classification, “0.10–0.29 = low, 0.30–0.49 = medium and 0.50-1.0 = high” indicates a correlation, and the evaluation of correlation levels was made in accordance with this classification20. The results were evaluated with a 95% confidence interval, with significance accepted at p ≤ 0.0521. The GraphPad Prism program (version 8) was used to evaluate data and graphs.
Results
Characteristics of the patients and the tumor
Thirty-five patients included in the study were women, and 15 were men. The control group consists of 24 women and 20 men. The average age of the patients is 56.28 ± 14.03, the lower limit is 23 years, and the upper limit is 79 years. The average age of control group participants is 52.30 ± 13.49, the lower limit is 22 years, and the upper limit is 76 years (Table 1). When the patient and control groups in the study were compared in terms of age and gender, no statistically significant difference was observed between the groups (p = 0.12, p = 0.08).
The majority of patients participating in the study, 88%, underwent their first operation. Multiple meningiomas were present in 12% of the patients. Before the first surgery, gamma knife surgery (GKS) was administered to 10% of the patients. Cyber Knife surgery was performed on 4%, and Radiotherapy (RT) was performed on 2%. In the postoperative period, GKS was used for 6% of the patients, and RT for 22% (Table 1).
Among the patients with multiple tumors, the tumors of three patients located in two different regions were completely removed in a single surgery. Consequently, measurements of f-TERRA, h-TERRA levels, and TL were conducted in 53 tissues. For the other three patients with multiple tumors, a second surgical session was planned for one, while the remaining two were scheduled for RT targeting the mass that was not planned for surgery (Table 1).
Edema was present in 58.5% of the patients. Among the 31 patients with edema, a severity level of 1 was determined in 45.2% of them. Meningiomas were found on the left side in 49.1% of the cases. Convexity was the most common site of meningioma placement, accounting for 22.6% of the cases. Meningiomas located in the sphenoid wing were the second most frequent, constituting 20.8% of the cases. The meningothelial subtype was the most common among Grade I histopathological types of meningiomas, representing 22.6% of them. All Grade II meningiomas were of the atypical subtype, comprising 37.7% of the total group. Pathological Grade I was observed in 60.4% of all meningiomas. Simpson Grade 2 resection was achieved in 41.5% of the meningiomas (Table 1).
Longer telomeres with lower TERRA expression levels in patients compared to control group
We compared the blood f-TERRA, h-TERRA levels, and TL of the patients in the pre- and post-operative periods with the healthy control group. The preoperative f-TERRA levels were significantly lower in patients compared to controls (p < 0.001) (Table 2; Fig. 2A). Similarly, postoperative f-TERRA levels in patients remained significantly lower than those of the control group (p < 0.001) (Table 2; Fig. 2A). For preoperative h-TERRA blood levels were significantly lower in patients compared to controls (p = 0.02) (Table 3; Fig. 2B). Postoperatively, h-TERRA levels did not show a statistically significant difference compared to controls (p = 0.25) (Table 3; Fig. 2B). TL was significantly longer in the blood of patient group both preoperatively and postoperatively compared to controls (p = 0.01 and p < 0.001, respectively) (Table 4; Fig. 3).

Comparison of preoperative and postoperative blood f-TERRA (A) and h-TERRA levels (B).

The blood TL of patients varies from preoperative to postoperative stage and is longer than that of the control group.
Treatment-dependent variations of in patients
Meningioma is a benign tumor and the probability of recurrence at 6 months after total tumor excision is very low. However, patients also underwent brain MRI for control purposes at 2 months after surgery and no recurrent tumor was detected during follow-up.
Six months after surgery, h-TERRA levels measured in patients’ blood cells with tumor elsewhere due to residual tumor or multiple tumors were statistically significantly higher than in patients without residual tumor (p = 0.005), (Table 5; Fig. 4).

Postoperative blood levels of h-TERRA in patients with residual tumors or tumors located elsewhere are higher than those without tumor detected in the postoperative period.
When comparing groups based on the degree of Simpson grade resection, patients who had two different Simpson grade resections in the same session and patients with tumors elsewhere even if a Simpson grade 1 resection had been achieved during surgery, were excluded from the evaluation. The relationship between postoperative h-TERRA levels of groups depending on the degree of Simpson grade resection in the study was found to be statistically significant (p = 0,01) (Table 6).
The relationship between postoperative h-TERRA levels of the Simpson grade groups in the study was examined. When postoperative blood h-TERRA levels were compared between the Simpson grade 1/grade 2 groups and the Simpson grade 1/grade 4 groups, a statistically significant difference was found (p = 0,002 and p = 0,02 respectively). The postoperative score of the Simpson grade 1 group (mean rank = 4.40) is lower than that of the Simpson grade 2 group (mean rank = 14.63) and the Simpson grade 4 group (mean rank = 12.27) (Fig. 5).

Postoperative h-TERRA levels of Simpson grade groups in the study.
When preoperative and postoperative blood h-TERRA levels were compared in Simpson grade 1 and grade 4 groups, the difference in relationship between them was found to be statistically significant (respectively p = 0,04 and p = 0,005) (Table 7; Fig. 6).

Blood levels of h-TERRA only decrease in stages 1 and 2, from preoperative to postoperative period, and do not change or increase in stages 3 and 4 of patients according to Simpson grade groups.
Blood levels of f-TERRA in patients with preoperative of RT/GKS/Cyber knife application status are lower than in patients who did not receive it. Likewise, the levels of f-TERRA in patients who received radiosurgical treatment during the preoperative period are statistically significant and lower than that in patients who did not receive it (Table 8; Fig. 7).

The blood levels of f-TERRA between the group that received RT/GKS/cyber knife preoperative and the group that did not.
Blood TL in 14 patients who underwent RT or GKS in the postoperative period was statistically significant and lower than in those who did not receive RT or GKS (p = 0.049) (Table 9; Fig. 8).

Postoperative blood TL between the group that received postoperative RT or GKS and the group that did not apply.
Correlation analyzes
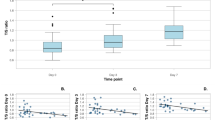
Correlation analysis between postoperative tumor volume and postoperative blood h-TERRA levels, a positive, moderate and statistically significant relationship was found (r = 0.38, p = 0.008). Furthermore, a positive, moderate, statistically significant relationship was found between the tissue levels of f-TERRA and h-TERRA (p = 0.001). A negative, moderately statistically significant relationship was found between age and preoperative blood TL (r = -0.47, p = 0.001). In blood, a negative, weak, statistically significant relationship was found between postoperative f-TERRA levels and postoperative TL (p = 0.04).
Comparisons between preoperative and postoperative periods
The preoperative and postoperative blood f-TERRA, h-TERRA levels and TL of the patients were compared, but the results were not statistically significant (respectively, p = 0.56, p = 0.31, p = 0.09) (Table 10) (Fig. 3).
Other results
When the relationship was investigated among patients in the study regarding the presence of systemic disease, preoperative tumor volume, presence and severity of edema, tumor location, histopathological subtype, pathological grade, presence of multiple masses, number of operations, and blood levels of f-TERRA and h-TERRA, as well as TL, no statistically significant result was found.
Discussion
In this study, we examined how lncRNA TERRA fractions in blood cells vary throughout the surgical process of meningioma, the most common primary benign brain tumor, by comparing preoperative and postoperative stages. Our work shows that global changes in the levels of free (f-TERRA) versus hybrid (h-TERRA) TERRA are involved in meningioma development and that their levels affect TL. In other studies, it has been shown that TL is mainly regulated by telomerase activation and regulation induced by alterations in TERRA levels22.
We showed that, especially with regard to TERRA levels (decrease), this indicates that it could serve as an important biomarker in the monitoring of patients with meningioma. We established that blood TERRA levels can be affected by surgery. Furthermore, it is likely that there are other mechanisms, beyond telomere function, to decrease TERRA transcription in response to overall tumor progression23. For example, depleting f-TERRA could release h-TERRA, which would then reduce its transcription. Importantly, we demonstrated that, despite widespread TERRA decay, the cells retain the capacity to increase malignancy, particularly TL. Although we previously found that telomerase activity increased slightly (see below), our observations of decreased TERRA suggest that h-TERRA may be important in triggering its transcriptional signaling and potentially controlling TL.
Our results confirm this synergy by showing that TERRA downregulation occurs in both fractions free and in DNA/RNA hybrids. Given that transcriptional deficiency can have serious health consequences related to telomerase upregulation, it is possible that loss of this dual branch weakens other branches of the genome stability response triggered independently by TERRA.
Interestingly, our data also suggests that TL increases in the limited amount of TERRA, in the absence of regulation. This is consistent with previous reports showing that in addition to TERRA, another factor can activate telomerase and that it is independent of TERRA activities. As already noted, a possible explanation is alternative way form of TL, in which telomerase activates the recombination responsible for ALT mechanisms24.
One possible explanation for this apparent decrease effect of TERRA on transcription of its own transcript is that the availability of the polymerase is due to the general reduction of the hybrid form, as noted above. Another possibility is that, as we have shown previously, decreasing in the DNA/ RNA hybrids lead to a decrease in the proportion of transcripts25.
Since TERRA originates from telomeres, we postulate that a decrease in the amount of TERRA could contribute to uncontrolled telomeres elongation. This is particularly relevant since telomeres are already being used or tested in cancer treatment.
TL in meningioma
Muskens et al., demonstrated that an increase in TL of genetically modified leukocyte is associated with a higher risk of developing meningiomas26. Our research confirms and reveals that meningioma patients have significantly longer TL in preoperative and postoperative blood samples compared to a control group. Interestingly, although the preoperative period showed no significant correlation between TL and age, such correlation was absent postoperatively, implying that surgical treatment could influence TL regardless of the age of the patient. Despite the postoperative TL of the patients close to that of the control group, it remained significantly high, suggesting the persistent effect of the tumor or the surgical procedure on the TL. The lack of significant difference in TL between preoperative and postoperative stages could be attributed to factors such as the small sample size, the presence of residual tumor, or the relatively short follow-up period of 6 months.
Studies on TL are contradictory on certain points. For example, Yamakawa et al. use a quantitative in situ hybridization method to study the relationship between meningioma grade and TL. They report a shorter TL in grade III meningiomas compared to grades I and II, with no significant difference between grades I and II27. Similarly, Chen et al. identified longer TL in a subset of patients with the more aggressive meningiomas, while Kheirollahi et al. observed shorter TL in all grades of meningioma and astrocytoma compared to controls, but no variation across tumor grades28,29. Our results are consistent with previous studies by Yamakawa et al. and Kheirollahi et al., reinforcing the lack of significant difference in TL between grade I and II meningiomas. We found no significant difference in TL between different grades, although our study was limited by the inclusion of only one grade III patient.
Here, we observed that TL measured from blood samples during the postoperative period was significantly reduced in 14 patients who underwent radiosurgery treatments, such as RT or GKS, compared to those who did not receive such treatments. This reduction in TL was observed regardless of the presence of residual tumor, highlighting that the effect of radiosurgery on TL is independent of tumor volume. Notably, four of these patients had no detectable residual tumor after surgery, but they underwent RT due to their diagnosis of grade II meningioma, in accordance with the European Association of Neuro-Oncology guidelines for an approach therapeutic approach. In contrast, seven patients with postoperative residual tumors or tumors located elsewhere did not receive radiosurgery within 6 months postoperative for various reasons, including planned surgeries for other tumor tissues. This distinction between patients receiving postoperative radiosurgery and those with postoperative tumors highlights that the observed changes in TL are directly attributable to radiosurgery rather than the sole presence of tumor tissue, supporting existing literature indicating that radiotherapy and gamma rays contribute to the shortening of the TL30.
Reduced f-TERRA levels in patients of meningioma
Our results show that preoperative blood levels of f-TERRA (total RNA samples extracted) in patients was statistically significantly lower than that of the control group. No studies in the literature have examined f-TERRA levels in the blood or tissue of meningioma patients. However, studies have compared f-TERRA levels in tumor tissues to that in normal tissues of different malignancies. The levels of f-TERRA were found to be lower in various types of tumor tissues than in normal tissues, associated with telomerase activity31,32. Decreased tissue levels of f-TERRA were significantly associated with poor prognosis in patients with hepatocellular carcinoma. It has also been reported that f-TERRA suppresses cell proliferation, metastatic abilities, and induces cell apoptosis in hepatocellular carcinoma by inhibiting telomere elongation33. Vitelli et al. reported that head and neck squamous cell carcinoma patients with low levels of f-TERRA had poorer clinical outcomes than those with high levels of f-TERRA32. Additionally, f-TERRA levels further decrease as tumor grade increases31. f-TERRA has also been shown to be a direct target of key tumor suppressors such as p53. The levels of f-TERRA are positively regulated by p53 to maintain genome integrity31,32,34,35. Another study demonstrated that inactivation of the tumor suppressor gene Rb1 resulted in decreased f-TERRA levels in cells, and this effect was reversed after restoration of Rb1 expression36. In our study, no statistically significant differences were observed when comparing the levels of f-TERRA in tumor tissue. Comparing tumor tissue with other normal tissues as a control, apart from brain tissue, could be misleading. Levels of f-TERRA and TL are known to vary between tissues. However, the presence of tumor tissue can affect both blood f-TERRA levels and blood TL. Our results, therefore, confirm the conclusions of these studies in literature. Nonetheless, conflicting results have also been reported, showing that f-TERRA levels are increased in various types of human cancer, such as ovarian cancer and medulloblastoma34. These results suggest that the levels of f-TERRA may change during tumor progression in a possibly tumor type-specific manner.
In the preoperative period, the preoperative blood levels of f-TERRA of 8 patients who received RT, GKRS or Cyber Knife treatment before tumor surgery were statistically significantly lower than those of other patients. The prognosis of these patients, whose tumor growth continues despite radiotherapy, is poorer, and tumor progression persists despite radiosurgical treatment. Therefore, it can be said that the levels of f-TERRA are diminished and weak in these cases.
The variations of hTERRA levels in meningioma patients
The only study in the literature showing a relationship with transcripts is psoriasis18. No association between and any tumor has been demonstrated in the literature to date, making this study pioneering in this regard. Here, preoperative blood transcript levels were found to be statistically significantly lower than those in the control group. However, no significant differences were observed between postoperative h-TERRA levels and those of the control group after treatment. Additionally, h-TERRA levels measured in patients with tumor elsewhere due to residual tumor or multiple tumors were statistically significantly higher than in patients without residual tumor. A positive and moderate correlation was also found between postoperative h-TERRA levels and postoperative tumor volume.
When patients were compared between Simpson grade groups, postoperative levels of h-TERRA showed statistically significant differences between groups. When examining the differences between the groups individually, it was found that the postoperative transcripts in the Simpson grade I group were statistically significantly lower than those in the Simpson grade II and Simpson grade IV groups. Although differences were observed between Simpson grade I and grade III comparisons, the lack of significant difference could be due to the small sample size split between the two groups. These results indicate that h-TERRA levels are more sensitive than f-TERRA levels and TL for residual volume monitoring and 6-months tumor follow-up. This suggests its potential use as a biomarker in disease monitoring. Additionally, h-TERRA levels as well as TL and f-TERRA levels will support the diagnosis and monitoring of meningioma patients. This study is also the first to show a correlation between residual tumor volume and h-TERRA.
When the significant differences found in the comparison of preoperative/postoperative h-TERRA levels in patients with Simpson grade I and Simpson grade IV resection are examined separately, it is observed that postoperative h-TERRA levels in patients with Simpson grade I resection are statistically significant. However, in Simpson grade IV patients, postoperative h-TERRA levels are statistically significantly higher compared to the preoperative period.
The response of decreased transcripts in the Simpson grade I group, which is considered to have the best resection according to the Simpson grade assessment, and increased expression in the Simpson grade IV group with subtotal resection, may seem contradictory with studies linking a reduction in TERRA expression to poor prognosis. However, it is important to remember that our study did not only detect TERRA expression in tumors or blood; it followed the process of pre-treatment, treatment, and post-treatment process. Our working hypothesis related to this topic and the process is presented in (Fig. 9).

The results illustrate that blood levels of h-TERRA change over time due to various factors.
Depending on the scenario, during the pre-tumor formation phase (A period), transcripts may fluctuate under the influence of various factors but remain at a critical level. transcripts, indicating the functional levels of TERRA activity that hybridizes to protect telomeres, are increasingly suppressed following tumor formation and increased telomerase activity, denoted B period. It is assumed that the duration and intensity of this decrease may vary depending on the malignancy potential of tumors during period B. Initially, an increase followed by a decrease due to acute stress due to tumor activity may occur. However, due to the slow progression of meningiomas, it is often impossible to diagnose or operate during this time. Because meningiomas are slow-growing benign tumors, transcription may take longer to decline than other tumor types. Failure to respond to this suppression and chronic stress from tumor exposure may be associated with poor prognosis. In response to the presence of tumors during period B, attempts are made to increase the transcript level to combat the tumor, but the suppressive effect of telomerase activity is considered more dominant. Normally, the increases in transcript levels indicate replication stress and DNA damage.
After surgery, during period C, the decrease in h-TERRA levels in Simpson grade I resection patients indicates a reduction in replication stress and DNA damage response. In other words, chronically stressed cells reduce transcript levels after tumor resection, as the positive feedback stimulus created by the tumor disappears, represented by a green line in (Fig. 9). The blood we collected from our patients 6-month postoperatively could belong to any period C or D on the chart. The decrease in h-TERRA level following successful removal of tumor tissue could indicate the success of the applied treatment. Variations in transcript response in patients with Simpson grade II resection suggest that, despite complete macroscopic ablation of tumor tissue, coagulation applied to the site of tumor origin is sufficient in some patients and inadequate in others. Complete resection at the cellular level may not have been achieved, even in the presence of macroscopic total resection and dura mater coagulation in the grade II group. We hypothesize that patients in the Simpson grade II and III groups demonstrate a trajectory between the lines shown in green or red, depending on treatment success (Fig. 9).
The increase in h-TERRA levels observed in Simpson grade IV patients, in whom subtotal resection was performed, could be attributed to both surgery-induced stress and disruption of the balance between TERRA, telomerase activity, and TL established since development of the tumor, due to the effects of surgery. Ultimately, the disruption of the balance established over the years by surgery increases the activity of the tumor tissue, represented by a red line in (Fig. 9). The positive correlation between the residual tumor volume and h-TERRA supports this hypothesis. In this group of patients, the levels of h-TERRA checked at 6 months correspond to a time in period C or D. With the end of the therapeutic effect, that is to say the transition from period C to D, the reverse movement of h-TERRA levels is observed in Simpson grade I and IV. However, sampling at 6 months provides limited information on the timing of post-treatment. Thus, more comprehensive studies with sampling at different time points are needed to fully illuminate this mechanism. There are other mechanisms affecting h-TERRA levels, but the presence of a tumor and the stress it causes overshadows the effects of other factors.
f-TERRA versus h-TERRA levels in meningioma patients
Due to the lack of research in the literature demonstrating f-TERRA and h-TERRA levels in meningioma patients, we indirectly evaluated and compared our results through telomerase activity previously demonstrated in meningioma patients. TERRA binds to the core components of telomerase, including the RNA component of telomerase (TERC) and TERT. It is generally accepted that TERRA can inhibit telomerase activity37. In meningiomas, a few studies published over the past two decades have shown increased TERT expression and telomerase activity, particularly in higher-grade meningiomas. Langford et al. analyzed telomerase activity in 52 meningioma cases using the telomeric repeat amplification protocol. They found that 26 of the 52 tumors (50%) had detectable telomerase activity. Of the 22 meningiomas classified as malignant or atypical, 21 (95%) had detectable telomerase activity, and these patients were determined to have a poor clinical prognosis. In 30 patients with grade I meningioma, only 5 (17%) had telomerase activity. A significant correlation between the presence of telomerase activity in grade I meningiomas and poor prognosis has been observed38.
Limitation of the study
We found that decreasing TERRA triggers the activation of telomerase, a known sensor of cell activation and growth. However, the exact mechanism by which TERRA depletion induce cell division remains ambiguous. Additionally, we observed a gradual decrease. It remains to be established whether decrease in TERRA levels due to environment or cancer induction evokes the same results.
Conclusions
This study, which is the first to investigate the impact of TERRA in meningioma patients, highlights the importance of presenting results through preoperative and postoperative comparisons. Particularly concerning patient results indicate that h-TERRA levels could serve as an important biomarker in the monitoring of meningioma patients. The significant differences in blood TERRA levels between patients and controls, as well as their correlation with tumor volume in patients, suggest a potential diagnostic utility. However, the therapeutic applicability of these markers requires further investigation. Future studies with larger cohorts are essential to determine their role in the treatment of meningioma.
Thus, modulating TERRA levels could be key to the safety and effectiveness of cancer treatments. Additionally, TERRA may play other roles in affecting transcription of target genes. The effects of TERRA on transcription may play an important role in enhancing or attenuating effects evoked by other RNA sensors, thereby highlighting connections between pathways responding to stress conditions. But TERRA-related therapies targeting telomeres could potentially affect rapidly dividing normal cells. However, tumor cells, including meningiomas, rely more heavily on telomerase activity or alternative lengthening of telomeres (ALT), offering a potential therapeutic window to minimize harm to normal tissues. The distinct telomere dynamics in meningiomas, as highlighted by our findings, suggest the possibility of tumor-specific targeting. Therapeutic strategies might focus on modulating TERRA levels to induce tumor cell senescence or apoptosis, though careful design is needed to avoid off-target events.
Data availability
The data in the current study are available from the corresponding author on reasonable request.
Abbreviations
- ALT:
-
Alternative lengthening telomere
- TL:
-
Telomere length
- TERRA:
-
Telomeric repeat containing RNA
- lncRNA:
-
Long non-coding RNA
- h-TERRA:
-
TERRA hybrid with DNA
- f-TERRA:
-
Total free fraction TERRA
- GKS:
-
Gamma knife surgery
- RT:
-
Radiotherapy
- cDNA:
-
Complementary DNA
- qPCR:
-
Quantitative real-time PCR
References
Kleihues, P. et al. The WHO classification of tumors of the nervous system. J. Neuropathol. Exp. Neurol. 61, 215–225 (2002).
Lamszus, K. Meningioma pathology, genetics, and biology. J. Neuropathol. Exp. Neurol. 63, 275–286 (2004).
San, A. et al. Health-related quality of life outcomes in meningioma patients based upon tumor location and treatment modality: a systematic review and meta-analysis. Cancers (Basel) 15, (2023).
Kwon, H., Lim, W. & Moon, B. I. Number of tumor foci as a risk factor for recurrence in papillary thyroid carcinoma: does it improve predictability? Cancers 14, 4141 (2022).
Fernandes, S. G. et al. Role of telomeres and telomeric proteins in human malignancies and their therapeutic potential. Cancers (Basel) 12, 1901 (2020).
Rossi, M. & Gorospe, M. Noncoding RNAs controlling telomere homeostasis in senescence and aging. Trends Mol. Med. 26, 422 (2020).
Colgin, L. M. & Reddel, R. R. Telomere maintenance mechanisms and cellular immortalization. Curr. Opin. Genet. Dev. 9, 97–103 (1999).
Hanahan, D. & Weinberg, R. A. The hallmarks of cancer. Cell 100, 57–70 (2000).
Neumann, A. A. & Reddel, R. R. Telomere maintenance and cancer—Look, no telomerase. Nat. Rev. Cancer 2, 879–884 (2002).
Artandi, S. E. & DePinho, R. A. Telomeres and telomerase in cancer. Carcinogenesis 31, 9–18 (2010).
Robinson, N. J. & Schiemann, W. P. Means to the ends: the role of telomeres and telomere processing machinery in metastasis. Biochim. Biophys. Acta 1866, 320–329 (2016).
Canale, P., Campolo, J., Borghini, A. & Andreassi, M. G. Long telomeric repeat-containing RNA (TERRA): Biological functions and challenges in vascular aging and disease. Biomedicines 11, 3211 (2023).
Chebly, A. et al. Telomeric repeat-containing RNA (TERRA): a review of the literature and first assessment in cutaneous T-cell lymphomas. Genes (Basel) 13, 539 (2022).
Nergadze, S. G. et al. CpG-island promoters drive transcription of human telomeres. RNA 15, 2186–2194 (2009).
Montero, J. J., de Silanes, I., Graña, O. & Blasco, M. A. Telomeric RNAs are essential to maintain telomeres. Nat. Commun. 7, 12534 (2016).
Kikinis, R., Pieper, S. D. & Vosburgh, K. G. 3D slicer: a platform for subject-specific image analysis, visualization, and clinical support. in Intraoperative Imaging and Image-Guided Therapy (ed Jolesz, F. A.) 277–289 https://doi.org/10.1007/978-1-4614-7657-3_19 (Springer, 2014).
Taheri, S. et al. The characterization of sex differences in hypoglycemia-induced activation of HPA axis on the transcriptomic level. Cell. Mol. Neurobiol. 42, 1523–1542 (2022).
Mehmetbeyoglu, E. et al. Decrease in RNase HII and accumulation of lncRNAs/DNA hybrids: A causal implication in psoriasis? Biomolecules 12, 368 (2022).
O’Callaghan, N. J. & Fenech, M. A quantitative PCR method for measuring absolute telomere length. Biol. Proc. 13, 3 (2011).
Cohen, J. Statistical power analysis for the behavioral sciences. Stat. Power Anal. Behav. Sci. https://doi.org/10.4324/9780203771587 (2013).
Fisher, R. A. Statistical methods for research workers. 66–70 https://doi.org/10.1007/978-1-4612-4380-9_6 (1992).
Chu, H. P. et al. TERRA RNA antagonizes ATRX and protects telomeres. Cell 170, 86–101.e16 (2017).
Vohhodina, J. et al. BRCA1 binds TERRA RNA and suppresses R-Loop-based telomeric DNA damage. Nat. Commun. 12, (2021).
Zhang, J. M. & Zou, L. Alternative lengthening of telomeres: from molecular mechanisms to therapeutic outlooks. Cell. Biosci. 10, (2020).
Şükranlı, Z. Y. et al. Head trauma impairs HPA-axis functions by increased R-loop structure and shortens telomeres. BioRxiv 596430 https://doi.org/10.1101/2024.05.29.596430 (2024).
Muskens, I. S. et al. Longer genotypically-estimated leukocyte telomere length is associated with increased meningioma risk. J. Neurooncol. 142, 479 (2019).
Yamakawa, K. et al. Telomere length was associated with grade and pathological features of meningioma. Sci. Rep. 12, (2022).
Chen, H. J., Liang, C. L., Lu, K., Lin, J. W. & Cho, C. L. Implication of telomerase activity and alternations of telomere length in the histologic characteristics of intracranial meningiomas. https://doi.org/10.1002/1097-0142(20001115)89:10 (2000).
Kheirollahi, M., Mehrazin, M., Kamalian, N. & Mehdipour, P. Alterations of telomere length in human brain tumors. Med. Oncol. 28, 864–870 (2011).
Li, P., Hou, M., Lou, F., Björkholm, M. & Xu, D. Telomere dysfunction induced by chemotherapeutic agents and radiation in normal human cells. Int. J. Biochem. Cell. Biol. 44, 1531–1540 (2012).
Sampl, S. et al. Expression of telomeres in astrocytoma WHO grade 2 to 4: TERRA level correlates with telomere length, telomerase activity, and advanced clinical grade. Transl Oncol. 5, 56–65 (2012).
Vitelli, V. et al. Telomeric repeat-containing RNAs (TERRA) decrease in squamous cell carcinoma of the head and neck is associated with worsened clinical outcome. Int. J. Mol. Sci. 19, (2018).
Oh, B. K., Keo, P., Bae, J., Ko, J. H. & Choi, J. S. Variable TERRA abundance and stability in cervical cancer cells. Int. J. Mol. Med. 39, 1597–1604 (2017).
Deng, Z. et al. Formation of telomeric repeat-containing RNA (TERRA) foci in highly proliferating mouse cerebellar neuronal progenitors and medulloblastoma. J. Cell. Sci. 125, 4383–4394 (2012).
Stögbauer, L., Stummer, W., Senner, V. & Brokinkel, B. Telomerase activity, TERT expression, hTERT promoter alterations, and alternative lengthening of the telomeres (ALT) in meningiomas—A systematic review. Neurosurg. Rev. 43, 903–910 (2020).
Gonzalez-Vasconcellos, I. et al. The Rb1 tumour suppressor gene modifies telomeric chromatin architecture by regulating TERRA expression. Sci. Rep. 7, (2017).
Cao, H. et al. Noncoding telomeric repeat-containing RNA inhibits the progression of hepatocellular carcinoma by regulating telomerase-mediated telomere length. Cancer Sci. 111, 2789–2802 (2020).
Langford, L. A. et al. Telomerase activity in ordinary meningiomas predicts poor outcome. Hum. Pathol. 28, 416–420 (1997).
Funding
This research was funded by Gazi University Scientific Research Projects Coordination Unit with the Grant Number TTU-2022-7616.
Author information
Authors and Affiliations
Contributions
MCS, ZYS, MR, ST, HE contributed to the conception and design of the study, and to the interpretation of the data. MCS, ZYS, AS, OYT, MBS was responsible for the acquisition of data and its analysis. MCS, ZYS, AS, OYT, MBS, BK played a major role in the statistical analysis and helped with the manuscript preparation. HE, ST, MR, EC supervised the project and revised the manuscript critically for important intellectual content. MCS, ST, HE provided the funding acquisition and technical support during the experiments. All authors have read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
In this study, planned as a prospective cohort, approval was received from the Gazi University Clinical Research Ethics Committee, dated 29.11.2021, decision number 21/128. The participants signed an informed consent form before joining the study. This research has been performed in accordance with the Declaration of Helsinki and its later amendments.
Consent for publication
All authors have provided their consent to publish the manuscript.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Sahin, M.C., Yilmaz Sukranli, Z., Sozer, A. et al. LncRNA TERRA in hybrid with DNA is a relevant biomarker for monitoring patients with meningioma. Sci Rep 15, 9011 (2025). https://doi.org/10.1038/s41598-025-90439-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-90439-9
Keywords
This article is cited by
-
Atypical R-loops in cancer: decoding molecular chaos for therapeutic gain
Journal of Translational Medicine (2025)
