
Abstract
Congenital heart disease (CHD) has severe impact on people’s health status and disease burden worldwide. Little is known about the disparities of the CHD burden in the western China. We aimed to analyze the disparities in sex, age, ethnic, marital status, and medical insurance so that we can improve the equity and reduce the disease burden among patients. We did a hospital-based cross-sectional study using data from a specialized cardiovascular hospital in western China, including health status, demographic and medical information. Logistic regression models were used in order to explore the association between CHD and sex, age, marital status, ethnic and medical insurance. Probit regression model was also used in sensitivity analysis. Female patients were more like to have CHD than their male counterparts (OR = 0.667; 95%CI = 0.515, 0.863; P = 0.002). Using people who aged less than 10 years old as reference, we found people aged between 10 and 19 years old, 20 to 29 years old, 30–39 years old, 40–49 years old had higher probability to suffer from CHD (OR = 11.051; 95%CI: 5.526, 22.097; P < 0.001; OR = 7.534; 95%CI: 3.528, 16.092; P < 0.001; OR = 3.479; 95%CI: 1.551, 7.803; P = 0.002; OR = 2.778; 95%CI: 1.313, 5.874; P = 0.008; respectively). Compared with no medical insurance, people use Urban Employee Basic Medical Insurance and Urban Resident Basic Medical Insurance have lower CHD prevalence (OR = 0.478; 95%CI: 0.274, 0.834; P = 0.009; OR = 0.408; 95%CI: 0.251, 0.663; P < 0.001; respectively). However, people with New rural cooperative medical insurance have higher CHD prevalence (OR = 1.985; 95%CI: 1.188, 3.316; P = 0.009). We also found significant relevance between marital status and the prevalence of CHD, married people had lower CHD prevalence compared with divorced or widowed respondents (OR = 0.492; 95%CI: 0.268, 0.904; P = 0.022). In this study, significant disparities were found in disease burden of CHD among different sex, age, marital status and medical insurance types. Our findings underscore the need for government and healthcare providers to prioritize early detection and proactive measures for CHD, with a particular focus on the demographic factors of sex and age. Additionally, enhancing the accessibility and coverage of public medical insurance is highlighted as a critical area for future improvement to mitigate the disease burden.
Similar content being viewed by others

Introduction
Heart disease is one of the leading causes of death worldwide1. Congenital heart disease (CHD) is a structural abnormality of the heart and great vessels that is present at birth2. This global health problem attracts much attention in recent years. Previous publications have estimated 250,000 annual CHD deaths globally, with 1.35 million annual births of neonates with CHD, which means 1 in 100 new born infants is defected by CHD3. CHD might cause shortness of breath and limited ability to do exercise, fatigue, abnormal sound of heart as heart murmur4. More seriously, people with CHD have higher possibility to die than others5. During the COVID-19 pandemic, cardiovascular disease is also proven to be the risk factor for death6. Compared with high income countries, the low-income and middle-income countries (LMICs) with severe forms of CHD and without access to surgical treatment are more likely to die before their fifth birthday7,8. Previous studies proved that the mortality from CHD declined in the United States, it still increased in China during the recent years9. Meanwhile, racial/ethnic and socioeconomic disparities exist in outcomes for children with congenital heart disease10. In China, research also showed that CHD also had severe impact on people’s health status and caused heavy disease burden among patients11,12,13.
The Sustainable Development Goals (SDGs) aim to reduce the mortality of neonates to less than 12 deaths per 1000 live births and the mortality of children to less than 25 deaths per 1000 live births. The SDGs also hope to reduce premature mortality due to non-communicable diseases (NCDs) by one-third by 20308. As the CHD accounts for about one-third congenital birth defects, analyzing the prevalence and disparities of CHD is essential to achieving the SDGs.
As proved in previous research, the diagnosis and treatment of CHD in the childhood could reduce the mortality rate of patients14. The etiology of CHD has also been considered to be multifactorial, due to both genetic predisposition and environmental influences, profoundly influenced by conditions in fetal and early life15. Studies showed that heart disease was affected by many determinants such as race and sex in the United States16,17.
However, based on previous study, we found that although much research about the prevalence (especially birth prevalence) of CHD, there is still a lack of study about the prevalence of CHD in the most recent years and the disparities especially sex, ethnic, medical insurance and so on in China. Meanwhile, most of research mainly focus on the general CHD prevalence in China or some developed provinces or districts12,13,18,19. Heart related diseases and death outcome are proven to be associated with sex, ethnicity, race, and geographic location16.
The unequal allocation of medical resources served as a primary rationale. The geographic distribution of a healthcare delivery system is an important component of healthcare access. In China, the distribution inequality in healthcare delivery system has been identified as a significant concern, resulting in limited access to healthcare and excessive workloads for healthcare providers20. Some studies indicated that hospitals in wealthier regions could afford to invest in healthcare resources such as equipment and personnel, but provinces in western China experienced the least equitable resource distribution21. The shortage of healthcare providers, particularly primary healthcare providers in rural areas of western China, have posed a threat to the health promotion in western China. In this study, we aimed at analyzing the disparities in sex, age, ethnic, marital status, and medical insurance so that we can improve the equity and reduce the disease burden among patients in western China. The same with other developing countries and areas, China also faces several challenges in the prevention and treatment of CHD, such as insufficient diagnostic capabilities and unqualified consultation services in some regions and rural areas22. Meanwhile, people in western China deserve insufficient healthcare resources and are faced with more severe disease risks.
The present investigation was designed to ascertain the prevalence of CHD within a substantial sample of over 150,000 subjects and to elucidate the disparities in the disease’s epidemiological burden. Our analysis is anticipated to augment the corpus of empirical data pertaining to the epidemiological landscape of CHD across China, offering a robust foundation for the refinement of therapeutic strategies tailored to the regional context. Consequent to the synthesis of our data, we proffer recommendations that advocate for the intensification of prenatal screening mechanisms for CHD. This approach is underscored by the potential to significantly mitigate the incidence of the disease and to ameliorate the overall life quality for the affected populace. Furthermore, we contend that the expansion and improvement of public medical insurance frameworks are imperative to ensure comprehensive and equitable access to healthcare services for individuals with CHD, thereby attenuating the socio-economic impact of the condition.
Materials and methods
Data collection and study design
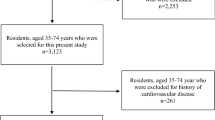
Data in this study are obtained from a specialized cardiovascular hospital in western China, which receives patients from the province it belongs to and other nearby provinces. The diagnosis and treatment scope of this hospital covers Yunnan, Gansu, Sichuan, Qinghai, Tibet, Guizhou and Chongqing. All data are from the electronic medical record system, which includes information about identity information, medical payment method, sex, date of birth, marital status, nationality, illness, etc. These data were collected from September 1st in 2017 to December 31st in 2024, including 150,488 respondents.
Research ethnics
Ethical approval
for this study was granted by the Center for Health Policy Research and Evaluation, Renmin University of China (No. RUC00000022-10001-1). All subjects gave written informed consent in accordance with the Declaration of Helsinki. All subjects were free to choose whether they were willing to participate in the research.
Measures
The dependent variable, which is the prevalence rate of CHD, is measured by the number of people with CHD divided by all respondents multiplied by 100%. Characteristics to measure disparities in disease burden included sex (0 = female, 1 = male), ethnic (0 = Han, 1 = Yi, 2 = Bai, 3 = Hui, 4 = Zang, 5 = Zhuang, 6 = Dai, 7 = others), age (0 = < 10, 1 = 10–19, 2 = 20–29, 3 = 30–39, 4 = 40–49, 5 = 50–59, 6 = 60–69, 7 = > 69), medical insurance (0 = no medical insurance, 1 = Urban Employee Basic Medical Insurance, 2 = Urban Resident Basic Medical Insurance, 3 = New rural cooperative medical insurance, “Xinnonghe”, 4 = other social insurance) and marital status (0 = divorced or widowed as reference, 1 = married, 2 = unmarried).
Statistical analysis
We used Stata version 16.0 to conduct the statistical analyses. Descriptive statistical analysis, including frequency and percentage, was used to summarize and report the basic information of our dependent and independent variables.
The chi-squared tests were used to explore the association between the prevalence of CHD and each independent variable. A p value < 0.05 was considered as statistical significance in all analysis.
We also used logistic regression to test the association between demographic and socioeconomic characteristics (sex, ethnic, age, medical insurance and marital status) and the prevalence of CHD. Results from logistic regressions were presented as odds ratios (ORs) and 95% confidence intervals (CI). To assess the goodness-of-fit of our logistic regression model, we utilized the Hosmer-Lemeshow test, a statistical method that evaluates the calibration of the model by comparing the observed and expected outcomes.
Moreover, to examine the robust of the results, we concluded a sensitivity analysis by fitting different models to analyze the robustness of our findings. In our sensitivity analysis, we converted the multi-classified ethnic variable (0 = others, 1 = Han) into dichotomous variable and changed the classification criteria of medical insurance and marital status.
Results
Descriptive results
From the results we found that the prevalence of CHD among female respondents (0.50%) was much higher than male (0.20%). Among all ethnics, we found that Dai ethnic (1.60%) has higher level of CHD prevalence than other ethnics. When it comes to age group, people aged 10–19 years old had the highest prevalence of CHD (1.61%) and people aged between 20 and 30 years old had the second highest CHD prevalence (0.65%). More specific variations were shown in Supplementary Material 1. Among people with CHD, most of them choose to use New rural cooperative medical insurance to pay for the treatment of CHD (1.07%) (Table 1).
The results showed that demographic characteristics including sex, ethnic, age group, marital status was significantly associated with the prevalence of CHD (P < 0.001). Meanwhile, medical insurance as a socioeconomic characteristic, was also significantly associated with the prevalence of CHD (P < 0.001). The Hosmer-Lemeshow test was non-significant, indicating that our logistic regression model fits the data well.
Regression results
In Table 2, we conducted logistic regression to explore the association between congenital heart disease and demographic and socioeconomic determinants. From our results, sex, medical insurance, marital status and some types of age group were significantly associated with CHD using multivariate analysis. Female patients were more like to have CHD than their male counterparts (OR = 0.667; 95%CI = 0.515, 0.863; P = 0.002). Although the above descriptive results showed that Yi ethnic population had higher level CHD prevalence, it was not significant in logistic results (OR = 1.082; 95%CI = 0.569, 2.061; P = 0.809). Using people who aged less than 10 years old as reference, we found people aged between 10 and 19 years old, 20 to 29 years old, 30–39 years old, 40–49 years old had higher probability to suffer from CHD (OR = 11.051; 95%CI: 5.526, 22.097; P < 0.001; OR = 7.534; 95%CI: 3.528, 16.092; P < 0.001; OR = 3.479; 95%CI: 1.551, 7.803; P = 0.002; OR = 2.778; 95%CI: 1.313, 5.874; P = 0.008; respectively).
Compared with no medical insurance, people use Urban Employee Basic Medical Insurance (OR = 0.478; 95%CI: 0.274, 0.834; P = 0.009) and Urban Resident Basic Medical Insurance (OR = 0.408; 95%CI: 0.251, 0.663; P < 0.001) have lower CHD prevalence. However, people with New rural cooperative medical insurance have higher CHD prevalence (OR = 1.985; 95%CI: 1.188, 3.316; P = 0.009). We also found significant relevance between marital status and the prevalence of CHD, married people had lower CHD prevalence compared with divorced or widowed respondents (OR = 0.492; 95%CI: 0.268, 0.904; P = 0.022).
Sensitivity analysis
To conduct sensitivity analysis, we separated ethnic into Han and other ethnic minorities. Medical insurance was separated into no medical insurance, UEBMI, URBMI, and other medical insurance. Marital status was divided into two groups: unmarried, divorced or widowed and married grouop. In the results of sensitivity analysis (Table 3), we found that sex was also significantly associated with the prevalence of CHD after changed our measurement of ethnic, marital status and medical insurance. Female respondents have higher CHD risks (OR: 0.672; 95%CI: 0.519, 0.870; P = 0.003). People aged below 50 years old had higher CHD prevalence (OR: 10.052; 95%CI: 5.114, 19.755; P < 0.001 for 10–19 years old; OR: 7.264; 95%CI: 3.417, 15.443; P < 0.001 for 20–29 years old; OR: 3.454; 95%CI: 1.548, 7.707; P = 0.002 for 30–39 years old; OR: 2.775; 95%CI: 1.324, 5.814; P = 0.007 for 40–49 years old).
Consistent with logistic results in Table 2, people use Urban Employee Basic Medical Insurance (OR = 0.476; 95%CI: 0.274, 0.828; P = 0.009) and Urban Resident Basic Medical Insurance (OR = 0.413; 95%CI: 0.255, 0.670; P < 0.001) have lower CHD prevalence. However, people with New rural cooperative medical insurance have higher CHD prevalence (OR = 1.885; 95%CI: 1.162, 3.057; P = 0.010). We also found significant relevance between marital status and the prevalence of CHD, married people had lower CHD prevalence compared with single, divorced or widowed respondents (OR = 0.515; 95%CI: 0.314, 0.844; P = 0.008).
Moreover, in order to further estimate the robustness of our results, we used probit regression model in sensitivity analysis part (Table 4). The results were robust in this analysis. Women were also easier to be diagnosed with CHD than men (Coef = −0.147; 95%CI: −0.235, −0.059; P = 0.001). Meanwhile, we also found that people aged below 50 years old had higher CHD prevalence (Coef = 0.785; 95%CI: 0.579, 0.992; P < 0.001 for 10–19 years old; Coef = 0.649; 95%CI: 0.409, 0.890; P < 0.001 for 20–29 years old; Coef = 0.377; 95%CI: 0.130, 0.625; P = 0.003 for 30–39 years old; Coef = 0.325; 95%CI: 0.102, 0.548; P = 0.004 for 40–49 years old).
Consistent with logistic results in Tables 2 and 3, people use Urban Employee Basic Medical Insurance (Coef = −0.224; 95%CI: −0.413, −0.035; P = 0.020) and Urban Resident Basic Medical Insurance (Coef = −0.295; 95%CI: −0.470, −0.120; P = 0.001) have lower CHD prevalence. However, people with other medical insurance have higher CHD prevalence (OR = 1.885; 95%CI: 1.162, 3.057; P = 0.010). Meanwhile, married people had lower CHD prevalence compared with single, divorced or widowed respondents (Coef = −0.219; 95%CI: −0.374, −0.063; P = 0.006).
Discussion
Our study estimated the prevalence of CHD and the disparities in disease burden among more than 150,000 individuals in western China. From the results, the prevalence of CHD among respondents about 0.16%, which was lower than the prevalence of CHD in other areas in China (for example, 0.97% in Hebei province)23. The prevalence of CHD was significantly associated with sex, age, marital status, and medical insurance. Following a comprehensive sensitivity analysis, the robustness of our findings was confirmed. Specifically, the results of our study align with those of prior research, which has consistently demonstrated a significant association between coronary heart disease (CHD) and socioeconomic status24.
Meanwhile, there is an ongoing academic debate concerning sex disparities in the incidence and mortality of congenital heart disease (CHD). A body of research indicates that males have a higher prevalence and mortality rate, whereas alternative studies propose that women are disproportionately affected by CHD. Moreover, it is noteworthy that women and children encounter an elevated risk post-CHD surgery, suggesting a complex interplay of gender in the prognosis and management of CHD25,26. This study provides empirical evidence supporting the notion that the incidence of congenital heart disease (CHD) is higher in female patients compared to the male population.
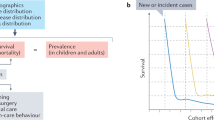
Studies from other countries have demonstrated a significant correlation between the incidence and treatment rates of congenital heart disease (CHD) and ethnicity, with minority groups facing greater disparities27. But we did not find significant difference of CHD prevalence among various ethnic groups. Although some progress has been made in the field of prevention and control of CHD, but the disease burden remains high among younger population in China28. Nowadays, with the decreasing mortality and increasing survival in all forms of congenital heart disease, the median age of patients has increased29,30. Reducing the impact on people with CHD in their later life is still a challenging problem16. Adults with CHD have been considered potentially high risk for COVID-19 mortality or other complications, which showed greater attention should be paid to those CHD patients31.
Individuals afflicted with CHD are inclined to rely on medical insurance to cover their healthcare expenditures. Prior research has demonstrated that those in possession of public medical insurance tend to exhibit a reduced likelihood of presenting with severe forms of CHD. This correlation suggests that public insurance may play a protective role in the early detection and management of critical CHD cases32. The evaluation of the impact of policy on CHD was critical to diminish health disparities33. Drawing from our research outcomes, we advocate that governmental entities, particularly the Medical Insurance Bureau, enhance their commitment to offering public medical insurance plans that encompass more extensive coverage.
Implications
Our research has yielded valuable insights into the prevalence of Congenital Heart Disease (CHD) within the western region of China, as well as the key determinants that influence its occurrence. This information is particularly beneficial for the targeted screening of individuals based on specific demographic criteria such as sex and age. Furthermore, our study offers constructive policy recommendations aimed at enhancing the care and support for those affected by CHD.
The findings underscore the importance of recognizing and addressing the varied risks associated with different gender identities, age groups, marital statuses, ethnic backgrounds, and types of medical insurance when it comes to the diagnosis and management of CHD. These disparities have a direct impact on health outcomes, access to healthcare, and the overall quality of services received.
The observation that women face a higher risk of congenital heart disease (CHD) underscores the imperative for a more vigilant approach towards the health monitoring of female newborns. It is crucial to integrate gender considerations into our healthcare strategies to address potential disparities in disease prevalence. This includes a proactive stance on identifying and mitigating factors that may contribute to the gender inequality in CHD incidence.
To tackle this issue effectively, it is essential to allocate medical resources and services equitably. This means ensuring that female patients have equal access to comprehensive disease prevention programs and advanced treatment options. Health policies should be designed to include gender-specific research and interventions that cater to the unique healthcare needs of women. Furthermore, raising awareness among healthcare providers about the gender differences in CHD is vital. This can lead to more accurate diagnoses and personalized treatment plans that take into account the distinct biological and physiological characteristics of female patients.
In the pursuit of health equity for the congenital heart disease community, it is crucial to not only acknowledge these differences but to also implement strategies that mitigate them. By doing so, we can work towards a healthcare system that provides equal opportunities for prevention, diagnosis, and treatment of CHD, regardless of an individual’s gender, age, marital status, ethnicity, or insurance coverage. This commitment to equity is essential for improving the lives of those with CHD and for fostering a more inclusive and effective healthcare environment.This requires strategic efforts to mitigate the impact of social determinants, systemic inequities, and structural racism that contribute to these health disparities34.
Limitations
Our study acknowledges several limitations that may influence its generalizability and interpretation. Firstly, the data were derived exclusively from the electronic medical records of a hospital, which inherently captures only patient-centric information. This exclusion limits the dataset’s scope, omitting critical variables such as the health status and educational levels of parents, the presence of prenatal examinations, and the living environment, which are known to be relevant to congenital heart disease risk factors. Secondly, the hospital’s specialization in cardiovascular care, situated in the western region, likely attracts a patient population with a higher prevalence of congenital heart disease. This selection bias suggests that the incidence rates reported in our study may overestimate the true rates within the general population, as our sample may not be representative of the broader demographic. Thirdly, the geographic focus of our study on western China means that our findings may not be directly applicable to residents of eastern or central China. Despite some demographic and environmental similarities, there may be underlying differences in genetic, socio-economic, and healthcare access factors that could alter the implications of our results for those populations. Fourthly, because of the absence of longitudinal data, it is not feasible to explore the causal relationship between CHD and socioeconomic factors. The study’s design and the available data do not permit the determination of whether socioeconomic factors influence the development of CHD or if there is a reverse causation, where CHD affects socioeconomic status.
Future prospects
In the future, we planned to use cross-country data to analyze the prevalence of CHD between different countries or regions. And we hope we could do some deeper research to evaluate the disparities in the disease burden of CHD such as economic disease burden and find out more constructive solutions to address related concerns. Other factors that may shadow congenital heart disease, such as the condition of parents suffering from heart disease, premarital medical examination, living environment, parents’ education, prenatal physical examination, etc., will also be studied and discussed. By addressing these multifaceted issues, we aspire to contribute to the development of targeted and effective measures that can alleviate the burden of CHD and enhance the quality of life for affected individuals across different societal contexts.
Conclusion
In this study, we analyzed the prevalence of CHD among residents in the west part of China and related influencing factors, including sex, age, marital status, ethnic and medical insurance. Significant associations were found between CHD and sex, age, marital status and medical insurance. We suggest that the government and healthcare facilities should pay more attention to prevent CHD and focus on demographic characteristics such as sex and age. Meanwhile, providing better coverage of public medical insurance for CHD is also an essential issue.
Research ethnics
The data utilized in this study include sensitive health information and the informed consent signed by the participants strictly prohibits the public release of the data due to ethical constraints.
Data availability
The data that support the findings of this study are available from Fuwai Yunnan Cardiovascular Hospital but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the corresponding author upon reasonable request and with permission of Fuwai Yunnan Cardiovascular Hospital.
Abbreviations
- CHD:
-
Congenital heart disease
- SDGs:
-
Sustainable Development Goals
- UEBMI:
-
Urban Employee Basic Medical Insurance
- URBMI:
-
Urban Resident Basic Medical Insurance
References
Saeed, H. et al. Demographic trends and disparities in mortality related to coexisting heart failure and diabetes mellitus among older adults in the united States between 1999 and 2020: A retrospective population-based cohort study from the CDC WONDER database. Int. J. Cardiol. Cardiovasc. Risk Prev. 23, 200326. https://doi.org/10.1016/j.ijcrp.2024.200326 (2024).
Triedman, J. K. & Newburger, J. W. Trends in congenital heart disease: the next decade. Circulation 133 (25), 2716–2733. https://doi.org/10.1161/CIRCULATIONAHA.116.023544 (2016).
van der Linde, D. et al. Birth prevalence of congenital heart disease worldwide. J. Am. Coll. Cardiol. 58 (21), 2241–2247. https://doi.org/10.1016/j.jacc.2011.08.025 (2011).
Sun, R., Liu, M., Lu, L., Zheng, Y. & Zhang, P. Congenital heart disease: causes, diagnosis, symptoms, and treatments. Cell. Biochem. Biophys. 72 (3), 857–860. https://doi.org/10.1007/s12013-015-0551-6 (2015).
Zomer, A. C. et al. Circumstances of death in adult congenital heart disease. Int. J. Cardiol. 154 (2), 168–172 (2012).
Li, J. et al. Defining heart disease risk for death in COVID-19 infection. QJM Int. J. Med. 113 (12), 876–882. https://doi.org/10.1093/qjmed/hcaa246 (2020).
Mavroudis, C. The natural and unnatural history of congenital heart disease. World J. Pediatr. Congenit Heart Surg. 1 (3), 411. https://doi.org/10.1177/2150135110379624 (2010).
Zimmerman, M. S. et al. Global, regional, and National burden of congenital heart disease, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet Child. Adolesc. Health. 4 (3), 185–200. https://doi.org/10.1016/S2352-4642(19)30402-X (2020).
Hu, Z., Yuan, X., Rao, K., Zheng, Z. & Hu, S. National trend in congenital heart disease mortality in China during 2003 to 2010: A population-based study. J. Thorac. Cardiovasc. Surg. 148 (2), 596–602e1. https://doi.org/10.1016/j.jtcvs.2013.08.067 (2014).
Peyvandi, S. et al. Socioeconomic mediators of Racial and ethnic disparities in congenital heart disease outcomes: A Population-Based study in California. J. Am. Heart Assoc. 7 (20), e010342. https://doi.org/10.1161/JAHA.118.010342 (2018).
He, Y., Xu, W., Su, Z., Liu, K. & Zhang, H. Addressing the rising burden of congenital heart disease in China. Lancet Child. Adolesc. Health. 4 (4), e7. https://doi.org/10.1016/S2352-4642(20)30061-4 (2020).
Zhao, L. et al. Birth prevalence of congenital heart disease in China, 1980–2019: a systematic review and meta-analysis of 617 studies. Eur. J. Epidemiol. 35 (7), 631–642. https://doi.org/10.1007/s10654-020-00653-0 (2020).
Zhao, Q. M. et al. Prevalence of congenital heart disease at live birth in China. J. Pediatr. 204, 53–58. https://doi.org/10.1016/j.jpeds.2018.08.040 (2019).
Scott, M. & Neal, A. E. Congenital heart disease. Prim. Care. 48 (3), 351–366. https://doi.org/10.1016/j.pop.2021.04.005 (2021).
Wong, P. et al. Early life environment and social determinants of cardiac health in children with congenital heart disease. Paediatr. Child. Health. 23 (2), 92–95. https://doi.org/10.1093/pch/pxx146 (2018).
Stegeman, R. et al. CeRebrUm and cardiac protection with allopurinol in neonates with critical congenital heart disease requiring cardiac surgery with cardiopulmonary bypass (CRUCIAL): study protocol of a phase III, randomized, quadruple-blinded, placebo-controlled, Dutch multicenter trial. Trials 23 (1), 174–174. https://doi.org/10.1186/s13063-022-06098-y (2022).
Vaughan, A. S., Quick, H., Pathak, E. B., Kramer, M. R. & Casper, M. Disparities in Temporal and geographic patterns of declining heart disease mortality by race and sex in the united States, 1973–2010. J. Am. Heart Assoc. 4 (12), e002567. https://doi.org/10.1161/JAHA.115.002567 (2015).
Pan, F. et al. Geographical and socioeconomic factors influence the birth prevalence of congenital heart disease: A Population-based Cross-sectional study in Eastern China. Curr. Probl. Cardiol. 47 (11), 101341. https://doi.org/10.1016/j.cpcardiol.2022.101341 (2022).
Jain, V. et al. Demographic and regional trends of heart Failure-Related mortality in young adults in the US, 1999–2019. JAMA Cardiol. 7 (9), 900–904. https://doi.org/10.1001/jamacardio.2022.2213 (2022).
Pan, J. & Shallcross, D. Geographic distribution of hospital beds throughout China: a county-level econometric analysis. Int. J. Equity Health. 15 (1), 179. https://doi.org/10.1186/s12939-016-0467-9 (2016).
Ao, Y., Feng, Q., Zhou, Z., Chen, Y. & Wang, T. Resource allocation equity in the China’s rural Three-Tier healthcare system. Int. J. Environ. Res. Public. Health. 19 (11), 6589. https://doi.org/10.3390/ijerph19116589 (2022).
Zhang, Y. et al. Current status and challenges in prenatal and neonatal screening, diagnosis, and management of congenital heart disease in China. Lancet Child. Adolesc. Health. 7 (7), 479–489. https://doi.org/10.1016/S2352-4642(23)00051-2 (2023).
Zhang, Q. et al. Associations between weekly air pollution exposure and congenital heart disease. Sci. Total Environ. 757, 143821. https://doi.org/10.1016/j.scitotenv.2020.143821 (2021).
Davey, B., Sinha, R., Lee, J. H., Gauthier, M. & Flores, G. Social determinants of health and outcomes for children and adults with congenital heart disease: a systematic review. Pediatr. Res. 89 (2), 275–294. https://doi.org/10.1038/s41390-020-01196-6 (2021).
D’Alto, M. et al. Does gender affect the prognosis and risk of complications in patients with congenital heart disease in the modern era? Int. J. Cardiol. 290, 156–161. https://doi.org/10.1016/j.ijcard.2019.05.010 (2019).
Oliver, J. M. et al. Impact of age and sex on survival and causes of death in adults with congenital heart disease. Int. J. Cardiol. 245, 119–124. https://doi.org/10.1016/j.ijcard.2017.06.060 (2017).
Grines, C. L. et al. Racial and ethnic disparities in coronary, vascular, structural, and congenital heart disease. Catheter Cardiovasc. Interv. 98 (2), 277–294. https://doi.org/10.1002/ccd.29745 (2021).
Pan, F., Xu, W., Li, J., Huang, Z. & Shu, Q. Trends in the disease burden of congenital heart disease in China over the past three decades. Zhejiang Xue Xue Bao Yi Xue Ban J. Zhejiang Univ. Med. Sci. 51 (3), 267–277. https://doi.org/10.3724/zdxbyxb-2022-0072 (2022).
Webb, G. et al. The care of adults with congenital heart disease across the Globe: current assessment and future perspective: A position statement from the international society for adult congenital heart disease (ISACHD). Int. J. Cardiol. 195, 326–333. https://doi.org/10.1016/j.ijcard.2015.04.230 (2015).
Mazor Dray, E. & Marelli, A. J. Adult Congenital Heart Disease: Scope of the Problem. Cardiol Clin. ;33(4):503–512, vii. (2015). https://doi.org/10.1016/j.ccl.2015.07.001
Broberg, C. S. et al. COVID-19 in adults with congenital heart disease. J. Am. Coll. Cardiol. 77 (13), 1644–1655. https://doi.org/10.1016/j.jacc.2021.02.023 (2021).
Peiris, V. et al. Association of socioeconomic position and medical insurance with fetal diagnosis of critical congenital heart disease. Circ. Cardiovasc. Qual. Outcomes. 2 (4), 354–360. https://doi.org/10.1161/CIRCOUTCOMES.108.802868 (2009).
Salciccioli, K. B., Salemi, J. L., Broda, C. R. & Lopez, K. N. Disparities in insurance coverage among hospitalized adult congenital heart disease patients before and after the affordable care act. Birth Defects Res. 113 (8), 644–659. https://doi.org/10.1002/bdr2.1878 (2021).
Lopez, K. N. et al. Addressing social determinants of health and mitigating health disparities across the lifespan in congenital heart disease: A scientific statement from the American heart association. J. Am. Heart Assoc. 11 (8), e025358. https://doi.org/10.1161/JAHA.122.025358 (2022).
Funding
This work was funded by the National Natural Science Foundation of China (Grant Numbers 72042002, 72122001, 72061160491, 72211540398); 2022 top-notch innovative talent cultivation funding plan of Renmin University of China.
Author information
Authors and Affiliations
Contributions
Conceptualization, J.W., Y.B., and J.L.; methodology, J.W. Y.B., and J.L.; software, Y.B.; validation, J.W., Y.B., and J.L.; formal analysis, Y.B.; data curation, Y.B. and J.L.; writing—original draft preparation, J.W., Y.B., and J.L.; writing—review and editing, J.W., Y.B., H.Z., and J.L.; visualization, Y.B.; supervision, Y.B., H.Z., and J.L.; funding acquisition, J.W., Y.B. and J.L. All authors have read and agreed to the final version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Our study had been granted an exemption from requiring ethics approval by Medical Health and Human Resources Ethics Committee, Renmin University of China.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, J., Bai, Y., Zhou, H. et al. Disparities in disease burden of congenital heart disease among 150,488 individuals in Western China. Sci Rep 15, 30159 (2025). https://doi.org/10.1038/s41598-025-91256-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-91256-w
