
Abstract
Unmet family planning needs are a critical public health problem in developing countries, particularly in Sub-Saharan Africa. An estimated 225 million women in developing countries who want to postpone, space, or avoid becoming pregnant do not use effective contraception methods, resulting in over 75 million unintended pregnancies each year, accounting for 84% of unintended pregnancies in developing countries. Thus, this study aimed to assess the determinants of the unmet need for family planning in Meyu Muluke District, Eastern Ethiopia. A community-based cross-sectional study was conducted from February 1 to 28, 2018, among 436 randomly selected currently married women of the reproductive age group in Meyu Muluke district, Eastern Ethiopia. Data were entered using Epidata version 3.1 and analyzed using Statistical Package for the Social Sciences (SPSS) version 25. Multivariate logistic regression was used to identify factors associated with the outcome variable, and a 95% confidence interval was used to declare statistical significance at a p-value of < 0.05. Overall, the magnitude of unmet need for family planning among currently married women was 36.02% (95% confidence interval (CI) 32.5–39.2%). Ages 25 to 29 years old [adjusted odds ratio (AOR) = 1.95, 95% CI (1.09–7.35), no formal education [AOR = 1.91, 95% CI (1.11–4.57)], middle wealth quintiles [AOR = 1.50, 95% CI (1.54–12.26)], some living children [0–1 and 2–3] [AOR = 1.47, 95% CI (1.33–8.83 [AOR = 0.67, 95% CI (1.26–18.80)], respectively], intending to use family planning in the future [AOR = 6.55, 95% CI (5.49–18.59)], and less than ten minutes to get to the family planning source [AOR = 2.33, 95% CI (1.15–4.72–2.92)] statistically significant to the unmet need for family planning. The study’s findings suggested that eight out of every twenty-five married women in Meyu Muluke District, Eastern Ethiopia, have unmet family planning needs. Age, education, children, intention, and time taken were significantly associated with the unmet need for family planning. Focusing on strategies that allow intervention in these factors is helpful to women because they, directly and indirectly, affect women’s health and educational achievement.
Similar content being viewed by others

Introduction
Unmet family planning needs are a critical public health problem in developing countries, notably in Sub-Saharan Africa1. An estimated 225 million women in developing countries who want to postpone, space, or avoid becoming pregnant do not use effective contraception methods, resulting in over 75 million unintended pregnancies each year, accounting for 84% of unintended pregnancies in developing countries. Furthermore, 57% of women in Sub-Saharan Africa and Southern Asia have an unmet need for modern contraception2,3. The unmet need for family planning is a measure of the proportion of sexually active women who want to postpone their next childbearing (spacers) or cease childbirth (limiters) but are not using any form of contraception4,5.
According to Sully et al., unintended pregnancy, unsafe abortions, and maternal mortality would be decreased by approximately two-thirds of all women in low- and middle-income countries (LMICs) who want to avoid pregnancy. They utilized modern contraception, and all pregnant women got treatment that matched international standards6. Furthermore, minimizing women’s exposure to the risks of pregnancy, unwanted, closely spaced pregnancies, infant and child mortality, expanding women’s education, work, and productivity, and improving women’s social position were all agreed-upon benefits of family planning for women7,8.
Global and regional initiatives have attempted to boost contraceptive use. Contraceptive prevalence and unmet demand for family planning are critical indicators for monitoring progress in reproductive health access, as stated in the 2030 Agenda for Sustainable Development under Objective 3.79. Family Planning 2020 is a global coalition that was founded in 2012 to increase the use of modern contraception by 120 million people in the 69 poorest nations in the world by the year 20202.
Religion, women’s age, number of living children, respondent’s place of residence, respondent’s education, knowledge of family planning, respondent’s work status, partner discussion, age at marriage of women, being visited by a family planning worker, parity, and the number of children at the time of first contraceptive use were all factors associated with unmet need for family planning, according to studies conducted around the world10,11,12,13,14,15,16,17.
The major consequences of unmet demand for family planning (FP) are high fertility, unexpected pregnancy, and unsafe abortion12. Every year, nearly 80 million unplanned pregnancies occur throughout the world, affecting mothers, children, and society as a whole18. Women in low- and middle-income nations continue to experience unplanned pregnancies despite numerous efforts to avoid unwanted pregnancies19,20.
Despite Ethiopia’s overall fertility rate of 4.6 children per woman and the availability of family planning services in practically all public and private institutions, only 41% of married Ethiopian women use contraception, and the unmet demand for family planning in Ethiopia remains significant, with a magnitude of 22%21,22. The prevalence and drivers of unmet family planning needs support each country in resolving its issues23. By minimizing the unmet demand for FP, it is possible to save over a million infant deaths and 54 million unintended pregnancies2. Furthermore, it improves women’s health, autonomy, and educational achievement. This study contributes to the area of family planning in Ethiopia by identifying determinants of unmet demand for FP at both the personal and social levels. This finding is crucial for policymakers and program planners to understand the importance of family planning for women in developing countries. Therefore, the goal of this study was to evaluate the factors that contribute to the unmet demand for family planning among married women in the Meyu Muluke district, Eastern Ethiopia.
Methods and materials
Study design
A community-based cross-sectional study.
Study period
A study was conducted from February 1 to 28, 2018.
Study setting
Mayu Muluke is situated in eastern Ethiopia, 557 km from the capital city of Ethiopia, Addis Ababa. Meyu Muluke woreda (district) is one of the 19 woredas in East Hararghe province in the Oromia Zone (region with 180 woredas) of Ethiopia. Meyu Muluke woreda comprises approximately 124 villages (divided into 19 kebeles). It is composed of approximately 124 villages (divided into 19 kebeles). According to the data from the 2016 EDHS, the total population for this woreda was 54,496, of whom 23,400 were men and 22,810 were women; 3,186, or 6.9%, of its population were urban dwellers. The Dinkas and Luo tribes are the predominant ethnic group inhabiting Meyu Muluke woreda. Pastoral and agro-pastoral communities continue to face food insecurity from reoccurring drought and subsequent livestock losses. Regarding the health facility of Meyu Muluke Woreda, all kebeles have HP, and at each HP there are two health extension workers (HEWs), so in Meyu Muluke Woreda there are 19 HP and 5 health centers (HC). Most residents make their living through farming and small-scale trading. The study was conducted in one urban and two rural kebeles in Mayu Muluke, Ifa-bas, and Finta-bas. Of these, reproductive age groups account for a total population of 817424.
Population
Source population: All currently married reproductive-age women in Meyu Muluke District.
Study population: Randomly selected in the reproductive age group women who were in Meyu Muluke District using the sampling technique who were available during the data collection period. We used the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) cross-sectional checklist when writing our report25.
Eligibility criteria
All childbearing-age women who were urban and rural dwellers in the Meyu Muluke district were the source population, whereas the study population consisted of randomly selected currently married women of childbearing age (15–49). Reproductive age group women were not living in union and not fecund, and if they were married 5 + years ago, had no children in the past 5 years, and never used contraception, those who were critically ill and unable to provide the required information during data collection were excluded from the study.
Data collection methods
An interviewer-administered, pretested, structured questionnaire adapted from related published literature contextualized the study objectives3,14,20,26,27,28,29,30. It includes information about the research participants’ knowledge, attitudes, and sociodemographic characteristics, as well as reproductive and socioeconomic backgrounds. Seven BSc Nurse Health professionals who speak Afaan Oromo fluently gathered the data. The lead investigator and two public health specialists were acquainted with the study’s environment and oversaw the work. Using data collection protocols, supervisors and data collectors received 4 days of training. We translated it with the intention of the questions and the goal of the survey in mind. Members of the group who are fluent in both languages translated it. The questionnaire was translated back into English by a person who was not familiar with the original text and the context of the questions in order to guarantee the correctness of the translation. The back-translated version is then compared to the original, and any meaning differences are corrected. We then attempted to interview a group of respondents in English and a second group in the local tongue, such as Afaan Oromo, in order to assure cross-validity. Then, discrepancies in their comprehension were found by comparing their responses. Lastly, pretesting was done to find questions that are unclear, difficult to understand, or cause unfavorable or other unwelcome answers.
We attempted to conduct a pretest using the already-translated questionnaire. We made an effort to carry out every stage of the pretesting process, including getting a questionnaire’s assessment and putting the updated version to the test on friends, coworkers, and other individuals. Furthermore, validity and reliability must be considered while selecting a tool. Reliability is the degree to which an instrument consistently yields the same outcomes during several trials. Validity is the extent to which an instrument measures what it was intended to measure. We calculated Cronbach’s alpha statistically, which is a metric used to evaluate the calibre of the equipment we utilized. The result was 0.89, which was within an acceptable range.
Variables and their measurements
Outcome variables
Unmet need for family planning (Yes, No).
Independent variables
Socio-demographic variables were the age of the woman (recoded as 15–19, 20–24, 25–29, 30–34, and 35 and above), place of residence (urban and rural), ethnicity (Oromo and Amhara), religion (Muslim and Christian), education level of the respondent (recoded as none formal education, primary school, secondary school, and above), respondent’s occupation (housewife, farmer, daily laborer, government employee, and merchant), wealth index (categorized as low, middle, and high), and family size (2–3, 4–5, and 6 and above). Reproductive variables were age at first marriage, number of living children, age at first pregnancy, current pregnancy status, and pregnancy type. Knowledge and attitude variables were hearing any contraceptive, knowledge of any method of contraceptive, source of information on contraceptives, Reason for use of contraceptives, Women’s attitude toward contraceptives, Discussion with health extension worker: who decides for you to use contraceptives? Does your husband know whether you use contraceptives or not? Discuss with your partner how to use contraceptives. Frequency of discussion with a partner and time taken to space birth of one child to another. In terms of wealth index as a factor in this study, this was computed data that includes ownership of certain consumer items, which ranges from ownership of a car or bicycle to television, availability of clean drinking water, type of material used in building houses, especially the floor material, the type of and availability of sanitation facilities, and other dwelling characteristics31. The household score for each member of the respective household was formed using the national-level wealth quintiles (that is, from lowest wealth to highest wealth) after the index was computed. Each person in the population was ranked with that score, while the ranking was divided into five categories comprising of 20% each31. However, the wealth index was further considered as low (poorest + second category), middle (middle category alone), and high (fourth + richest category) based on the specifications earlier highlighted and also cited in some previous studies32,33. The data file succinctly reported both limiting of children bearing and unmet need for spacing, including some other related variables. The unaddressed need to restrict childbearing and spacing was added such that the total unmet need for FP was obtained. The other related variables of the said category were summed up to form the total number of met needs category32,33,34.
Currently married reproductive age group women: women of reproductive age group (15–49 years) who are married.
Unmet need refers to those women who are fecund and sexually active but are not using any method of contraception and report not wanting any more children or wanting to delay the birth of the next child (WHO, 2018).
Current users are women who were using contraception at the time of the interview.
Met need for contraception refers to those currently married women who want to space births or limit the number of children and are using contraceptive methods to avoid unwanted or mistimed pregnancies9.
Infecund women who are considered fecund if they were married 5 + years ago, had no child in the past 5 years and never used contraception; or said “can’t get pregnant” on the wanting of future children; or said “menopause/hysterectomy” on reason for not using contraception; or response time since last period is ≥ 6 months or “never menstruated; or response to time since last period is “last period was before last birth” and last birth 5 + years ago.
Fecund women refers to women who have been reported as capable of reproducing or who have no infecundity criteria.
Postpartum amenorrhea: refers to the interval between childbirth and resumption of menstruation up to 0–23 months, a period during which a woman is temporarily infecund.
Knowledge of contraception: awareness of at least one method of contraception (mention at least the name of one modern contraception method).
Favorable attitude: A woman whose cumulative sum value for 11 attitudinal statement responses was lower than the summed mean score values of all women.
Unfavorable attitude: A woman whose cumulative sum value for 11 attitudinal statement responses was greater than or equal to the summed mean score value of all women.
Bias
Although certain biases were present during the study process, the researcher took specific precautions to prevent them. The researcher tried to prevent social desirability and recall bias by rephrasing the questions in a way that was not acceptable to society and by trying to hint at the intended question that needed to be answered.
Sample size determination
The sample size was determined by using a single population proportion formula, considering the following assumptions: n = (z (alpha/2)2*p*(1 − p))/d2.
Where n = minimum sample size required for the study, Z = standard normal distribution (Z = 1.96), with a confidence interval of 95% and ⍺ = 0.05, P = proportion of unmet need for family planning (22%) from the previous study26, d = maximum acceptable margin of sampling error (d) = 5% = 0.05, and design effect = 1.5. Then, after adding contingency (10%) for the non-respondent rate, the minimum total sample size for the study became 436.
Sampling technique and procedure
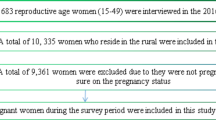
A multistage sampling technique was used to sample the study participants. Meyu Muluke district has one urban and 18 rural kebeles. Then, considering the homogeneity of the rural kebeles, two rural kebeles were selected using a simple random sampling technique, and only one urban kebele was included in the study by default. The data collectors numbered all the households in the chosen kebeles; there were 3270 households. For every chosen kebele, households were distributed proportionately. A systematic random selection procedure with a k value of 6 was used to choose each family. The lottery method was used to select the first household, and the eligible individual inside that household was then enrolled in the research. In cases where no eligible respondent was found in the selected household, the data collectors have gone to the next household. By using this method, 436 homes’ worth of research participants were identified (Fig. 1).

Schematic presentation of sample selection procedure of reproductive characteristics among currently married women in respondents in Meyu Muluke District, Eastern Ethiopia, 2018.
Data quality control
The questionnaire was prepared in English and then translated into the local language by a bilingual expert (Afaan Oromo). Then, it was translated back into an English version to ensure consistency. The data collectors and supervisor received training on the data collection tool and procedures. Before the study data collection, a pretest was conducted among 10% of the study participants in similar settings. The investigators and experienced research supervisors provided regular supervision.
Data processing and analysis
The collected data were coded and entered into Epi-data 3.1 and then exported to SPSS version 25 for analysis. We conducted and reported descriptive and summary statistics using frequency tables and figures. Bivariable variable logistic regression was carried out to select a candidate for multivariate logistic regression analysis with a p-value < 0.2535 at a 95% confidence level. Then, a candidate variable was entered into a multivariable logistic regression model to identify the statistically significant factors for the unmet need for family planning. With all regression assumptions fulfilled [i.e., model prediction of variables improved from the beginning block (from 66.7 to 72.5%), better prediction of variables than constant-only model (omnibus test of coefficients at p < 0.001)], the dependent variable is well explained by the independent variables in the model summary. The goodness-of-fit of the model was assessed using the Hosmer–Lemeshow. It is Hosmer–Lemeshow test with a non-significant (p-value = 0.344), representing a good-fit model. Thus, the value of the variance inflation factor (VIF) was 0.951. The degree of association between dependent and independent variables was assessed using an adjusted odds ratio, and statistically significant factors were declared at 95% of a confidence interval and a p-value of less than 0.05. Multi-collinearity was checked for all variables entered into the model.
Results
Socio-demographic characteristics
A study shows that a total of 436 married reproductive-age women were involved, yielding a response rate of 100%. The mean (± SD) ages of the study participants were 24.5 (± 5.557). More than a quarter of the study participants, 117 (26.8%) and 115 (26.4%), were in the age range of 20–24 and 25–29, respectively. Three-quarters of the respondents, 327 (75%), came from rural areas. Most of the respondents, 425 (97.5%), were Oromo by ethnicity, and 420 (96.3%) were Muslims. In terms of educational status, 283 (64.9%) of the respondents attended formal education, and 260 (59.6%) were housewives. In terms of family size, 191 (43.8%) had six or more children (Table 1).
Reproductive history of study participants
More than a quarter of the respondents, 117 (26.6%) and 115 (26.4%), were married between the ages of 20–24, and 25–30, respectively. The mean age of women at marriage was 21.5 ± 2.4 SD years. More than half of the respondents, 247 (56.7%), got pregnant at ages 19–24. The mean age for the first pregnancy was 26.47 ± 2.57 SD years. Regarding the number of living children, 166 (38%) respondents had two or three children. Regarding current pregnancy status, forty-six (10.6%) study participants were pregnant, of which 20 (4.6%) were intended (Table 2).
Knowledge and attitudes to contraceptives
Regarding information about any kind of contraception, 340 (78%) study participants reported hearing information about contraceptives, and of those, over three-fifths (59.4%) replied hearing it from healthcare professionals. Out of those who knew about contraceptives, 167 (38.3%) replied that they knew about pills. Interims of reasons for contraceptive use 197 (45.1%) study participants mentioned that they used it for spacing births. According to this study, 159 (36.5%) study participants have had a discussion with partners to use contraceptives, and of those, 71 (16.3%) had a discussion only once. Regarding the decision-making role, 43 (9.9%) respondents replied that they had a joint decision for the use of contraceptives (Table 3).
Reasons that hinder to use contraceptives
As shown in the figure below, 70 (16.1%) did not use it because of fear of side effects, whereas 12 (2.8%) did not use it due to a perceived risk of pregnancy and a lack of knowledge (Fig. 2).

Showing the reasons that hinder to use contraceptives services among currently married women in respondents in Meyu Muluke District, Eastern Ethiopia, 2018.
Unmet need for family planning
The level of unmet demand for family planning was further examined among married women between the ages of 15 and 49 using the West off model36. In the Meyu Muluke district, there are 157 (36.02%) unmet contraceptive needs in total, of which 86 (19.72%) are for spacing and 71 (16.28%) are for limiting (see Fig. 1). The combined demand for contraception was 80.32% (current usage 44.3% + unmet need 36.02%). Of those, 64.1% had used contemporary contraceptives to meet demand. For modern methods, there was a 44.3% unmet need (Fig. 3).

Unmet need for family planning among currently married women in respondents in Meyu Muluke District, Eastern Ethiopia, 2018.
Factors associated with unmet need for family planning
A multivariable logistic regression analysis revealed that the unmet need for family planning was significantly correlated with the age of the women, who ranged from 25 to 29 years old; the number of living children; the women’s lack of formal education; and the time spent traveling to the family planning source, which was between 11 and 30 min and less than 10 min. Study participants in the age range of 25–29 years old 1.95 times [AOR = 1.95, 95% CI (1.09–7.35)] had higher odds of unmet need for family planning than those whose age was greater than or equal to 35 years. Likewise, women with no formal education 1.91 times [AOR = 1.91, 95% CI (1.11–4.57)] had a greater likelihood of experiencing an unmet need for family planning compared to those who were in secondary and above education. Furthermore, women who had a middle wealth quintile were 1.5 times more likely to experience an unmet need for family planning than those who had a high wealth quintile [AOR = 1.50, 95% CI 1.54–12.26].
Those women who had some living children were found to be statistically significant in terms of the unmet need for family planning. Hence, women who did not have children and had one child 1.47 times [AOR = 1.47, 95% CI (1.33–0.83)] were more likely to experience an unmet need for family planning compared to those who had six and above living children. Similarly, women who had two or three living children were 33% less likely to encounter an unmet need for family planning than those who had six or more living children [AOR = 0.67, 95% CI 1.26–18.80].
Women who had a future intention to use family planning were 6.55 times more likely to experience an unmet need for family planning compared to their counterparts [AOR = 6.55, 95% CI 5.49–18.59]. The time taken to arrive at the source of family planning was found to be statistically significant for the outcome variables. Thus, those women whose travel distance was less than or equal to 10 min have a 2.33 times greater likelihood of experiencing an unmet need for family planning than those who travel greater than 1 h [AOR = 2.33, 95% CI 1.15–4.72]. Likewise, those women whose travel distance was 11–30 min were 25% less likely to experience an unmet need for family planning than those who traveled for more than 1 h [AOR = 0.75, 95% CI 0.57–2.92] (Table 4).
Discussion
This study was conducted to identify the prevalence of unmet needs for family planning and associated factors among reproductive-age women in the Meyu Muluke District, Eastern Ethiopia. The findings of this study revealed that the prevalence of unmet needs for family planning was 36.02% (95% CI 32.5–39.2%) in the study area. Thus, roughly more than one in every three childbearing-age women experienced an unmet need for family planning. Factors such as age of women whose range is between 25 and 29 years, women with no formal education, number of living children, those who have a future intention to use family planning, and time taken to the source of family planning less than 10 min and 11–30 min were significantly associated with an unmet need for family planning.
The prevalence of unmet needs for family planning in this study was in line with the study conducted in eastern Ethiopia, 34.6%30, Saudi Arabia, 32.6%37, and India, 39%38. On the other hand, the magnitude during the present study was lower compared to the previous studies conducted in Cameroon 46.6%39, and Angola 51.7%40. On the contrary, the findings of this study were higher than those of the studies carried out in Eastern Sudan 15.8%14, Ethiopia 16.2%11, Gambia 17.68%41, Hawella, Ethiopia 18.1%3, Mozambique 20.79%41, Zambia 21%42, Malawi 21%43, Bangladesh 22.4%44, Pakistan 23.5%45 and Indonesia 24%46. This disparity may be caused by variations in the accessibility of healthcare, knowledge of and attitudes toward family planning services, as well as sociodemographic and cultural factors. In addition, a difference in sample size may cause a significant difference in the report. Moreover, the larger prevalence of unmet needs for family planning in our study area was possibly explained by the residence of the participants, where 75% of the population resides in rural areas. This is because the composition of the sample size could have an enormous effect on the prevalence of the study outcome17,47,48.
The results of this study indicated a substantial correlation between the women’s age and their unmet demand for family planning. Thus, women aged between 25 and 29 years old have 1.95 times higher odds of having an unmet need for family planning than those whose age is greater than or equal to 35 years. This finding is consistent with studies carried out in different parts of the world, such as Nigeria49, Pakistan17, and Burundi16. The fact that, in comparison to their peers, this age group may have a strong intention and desire to utilize family planning to either limit or space out the pregnancy might be one of the probable explanations.
According to this study, the educational status of women has a significant association with an unmet need for family planning. The odds of no formal education for women with an unmet need for family planning were 1.91 times higher than those attending secondary or higher education. This finding was supported by the previous studies conducted in Hawella City, Ethiopia3, Enemay District, Northwest Ethiopia29, Toke Kutaye District, Ethiopia50, Nepal51, Pakistan17,45, and Ethiopia27. This might be explained by married women without formal education, who may not have a significant part in determining their FP requirements and who may lack the required level of financial independence due to their frequent unemployment. Furthermore, educated women explicitly have far better knowledge of the importance and use of family planning services, which in turn inevitably enable and boost their use of this pivotal service. Moreover, in addition to having fewer access to healthcare facilities, women without formal education may not be able to read and comprehend the majority of family planning messages found in print and on social media, which would expand their knowledge and expose them to new information sources.
Our study explicitly pointed out that wealth quintiles were one of the determinants of the unmet need for family planning. The odds of an unmet need for family planning were 1.50 times higher among those in the middle wealth quintile than those in the high wealth quintile. This finding contradicts the study conducted in Ethiopia52. Similar findings were found in a comparison of demographic health surveys conducted in 34 developing nations in 2014, which revealed that young married women in the highest wealth quintile had a significant unmet demand for contraception29. This shows that having a high wealth index does not ensure that family planning needs are addressed.
Findings from this study showed that the number of living children had a statistically significant association with an unmet need for family planning. Hence, women who did not have children and had one child were 1.47 times more likely to experience an unmet need for family planning compared to those who had six or more living children. This study contradicts the study conducted in certain parts of southwest Ethiopia28. Furthermore, women who had two or three living children were 33% less likely to encounter an unmet need for family planning than those who had six or more living children. Findings from this study are in agreement with those conducted in different parts of Ethiopia28,53, Uganda54, and middle-income countries55. This might be because, as women have a high number of living children, their likelihood of using contraceptives may soar.
Furthermore, our study revealed that women who had a future intention of using family planning 6.55 times were more likely to experience an unmet need for family planning compared to their counterparts. This is supported by the study conducted in different parts of Ethiopia56. This is because the decision to use family planning in the future creates a supportive and conducive atmosphere for women to utilize contraceptives and pursue their goals for fertility. Finally, this study vividly pointed out that the time taken to arrive at the source of family planning was statistically significant for the outcome variables. Thus, those women whose travel distance was less than or equal to 10 min have a 2.33 times greater likelihood of experiencing family planning needs than those who traveled for more than 1 h. In a similar vein, women who traveled between 11 and 30 min had a 25% lower chance of having their family planning requirements unfulfilled compared to those who traveled more than an hour. This is explicitly because the further away the health facilities are from the user, the less likely the customer is to utilize the services57,58,59.
Strength and limitations of the study
It is important to use caution when interpreting the survey’s results. This survey’s cross-sectional design prevents the straightforward establishment of cause-and-effect linkages. We did not measure the unmet demand for family planning among single men and women in our study. This is significant since our findings indicated that the male partner has a significant influence on a woman’s decision to use contraception. Additionally, our study did not assess family planning practitioners’ expertise or the availability of contraceptive options among this demographic. The results, however, are in complete agreement with earlier study findings and were achieved following accepted scientific research standards and with sufficient methodology. Our study serves as a gauge for the local family planning requirements and supports the proper distribution of resources for the sector.
Conclusions
The study’s findings suggested that eight out of every twenty-five married women in Meyu Muluke District, Eastern Ethiopia, have unmet family planning needs. Age, education, children, intention, and time taken were significantly associated with the unmet need for family planning. Focusing on strategies that allow intervention in these factors is helpful to women because they directly and indirectly affect women’s health and educational achievement.
Data availability
All data generated and analyzed during this study are available from the corresponding author upon reasonable request.
References
Gahungu, J., Vahdaninia, M., Regmi, P.R.J.R.H. The unmet needs for modern family planning methods among postpartum women in Sub-Saharan Africa: a systematic review of the literature. 18, 1–15 (2021).
Singh, S., Darroch, J. E., Ashford, L. S. Adding it up: the costs and benefits of investing in sexual and reproductive health 2014. (2014).
Assefa, A. A. et al. Unmet need for family planning and associated factors among currently married women in Hawella Tulla subcity, Hawassa, southern Ethiopia: community-based study. Contracept. Reprod. Med. 8(1), 14 (2023).
Bongaarts, J. J., The impact of family planning programs on unmet need and demand for contraception. 45(2), 247–262 (2014).
Nations, U.J.O.d.t.D.o.e. and s. Affairs. Trends in Contraceptive Use Worldwide. (2015).
Sully, E.A. et al., Adding It Up: Investing in Sexual and Reproductive Health 2019. (2020).
Stover, J. & Ross, J. How increased contraceptive use has reduced maternal mortality. Matern. Child Health J. 14, 687–695 (2010).
Cleland, J. et al. Contracept. Health. 380(9837), 149–156 (2012).
Starbird, E. et al. Investing in family planning: key to achieving the sustainable development goals. Glob. Health Sci. Pract. 4(2), 191–210 (2016).
Kesetebirhan, A.J.F.D.R.o.E., Ministry of Health, National Guideline for Family Planning Services in Ethiopia. 20–23 (2011).
Tadele, A. et al. Predictors of unmet need for family planning among all women of reproductive age in Ethiopia. Contracept. Reprod. Med. 4(1), 1–9 (2019).
Shifa, G. T. & Kondale, M. J. High unmet need for family planning and factors contributing to it in southern Ethiopia: A community based cross-sectional study. Glob. J. Med. Res. 14, 20–32 (2014).
Mekonnen, W. & Worku, A. J. Determinants of low family planning use and high unmet need in Butajira District, South Central Ethiopia. Reprod. Health 8, 1–8 (2011).
Ali, A. A. A. & Okud, A. J. Factors affecting unmet need for family planning in Eastern Sudan. BMC Public Health 13, 1–5 (2013).
Worku, S. A. et al. Unmet need for family planning in Ethiopia and its association with occupational status of women and discussion to her partner: a systematic review and meta-analysis. Contracept. Reprod. Med. 5(1), 1–10 (2020).
Nzokirishaka, A. Determinants of unmet need for family planning among married women of reproductive age in Burundi: a cross-sectional study. Contracept. Reprod. Med. 3, 1–13 (2018).
Asif, M. F. & Pervaiz, Z. J. Socio-demographic determinants of unmet need for family planning among married women in Pakistan. BMC Public Health 19(1), 1–8 (2019).
Elweshahi, H. M. T. et al. Unmet need for postpartum family planning in Alexandria. Egypt. 54(2), 143–147 (2018).
Hindin, M. J. et al. Interventions to prevent unintended and repeat pregnancy among young people in low-and middle-income countries: a systematic review of the published and gray literature. J. Adolesc. Health 59(3), S8–S15 (2016).
Berta, M. et al. Utilization and associated factors of modern contraceptives during extended postpartum period among women who gave birth in the last 12 months in Gondar Town, northwest Ethiopia. Ethiop. J. Health Sci. 28(2), 207–216 (2018).
Arimond, M., Ruel, M. T. Progress in Developing an Infant and a Child Feeding Index: an Example Using the Ethiopia Demographic and Health Survey 2000. (2002).
Health., M. O., Federal Democratic Republic of Ethiopia. Health Sector Transformation Plan II (2021).
L, A., Unmet need for family planning: Recent trends and their implications for programs. Population Reference Bureau Washington, DC (2003).
ICF, C. Ethiopia Demographic and Health Survey 2016: Key Indicators Report. Addis Ababa, Ethiopia, and Rockville, Maryland, USA. (2016).
von Elm E, A.D., Egger, M., Pocock, S. J., Gotzsche, P. C., Vandenbroucke, J. P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies.
EDHS. Ethiopia Demograph Health Survey and Surviliance (2016).
Asmamaw, D. B. & Negash, W. D. Magnitude of unmet need for family planning and its predictors among reproductive age women in high fertility regions of Ethiopia: Evidence from Ethiopian Demographic and Health Survey. BMC Women’s Health 22(1), 408 (2022).
Bedhadha, S. T. Determinants of unmet need for contraception among currently married women in Oromia National Regional State; Evidence from Ethiopia Demographic and Health Survey Data. Int. J. Sci. Res. IJSR 5(12), 2319–7064 (2016).
Dejenu, G. A. M., Abajobir, A. A. Prevalence and associated factors of unmet need for family planning among married women in Enemay District, Northwest Ethiopia: A comparative cross-sectional study.). Glob. J. Med. Res. Interdiscip. 13(4) (2013).
Dingeta, T. et al. Unmet need for contraception among young married women in Eastern Ethiopia. Open Access J. Contracept. 10, 89–101 (2019).
EDHS, CSA and ICF: Central Statistical Agency (CSA) [Ethiopia] and ICF (2016) Ethiopia demographic and health survey 2016: Key indicators report. Addis Ababa, Ethiopia, and Rockville, Maryland, USA (2016).
Wulifan, J. K. et al. Determinants of unmet need for family planning in rural Burkina Faso: a multilevel logistic regression analysis. BMC Pregnancy Childbirth 17(1), 426 (2017).
Wulifan, J. K. et al. A scoping review on determinants of unmet need for family planning among women of reproductive age in low and middle income countries. BMC Women’s Health 16(1), 2 (2016).
Edietah, E. E. et al. Contraceptive use and determinants of unmet need for family planning; a cross sectional survey in the North West Region, Cameroon. BMC Women’s Health 18(1), 171 (2018).
Hosmer Jr, D.W., Lemeshow, S., Sturdivant, R. X. Applied Logistic Regression (Wiley, 2013).
Bradley, S.E. Revising Unmet Need for Family Planning (ICF International, 2012).
Khalil, S. N., Alzahrani, M. M. & Siddiqui, A. F. J. Unmet need and demand for family planning among married women of Abha, Aseer Region in Saudi Arabia. Middle East Fertil. Soc. J. 23(1), 31–36 (2018).
Bhattathiry, M. M. & Ethirajan, N. J. Unmet need for family planning among married women of reproductive age group in urban Tamil Nadu. J. Fam. Community Med. 21(1), 53–57 (2014).
Edietah, E. E. et al. Contraceptive use and determinants of unmet need for family planning; a cross sectional survey in the North West Region. Cameroon. 18, 1–8 (2018).
Yaya, S. & Ghose, B. Prevalence of unmet need for contraception and its association with unwanted pregnancy among married women in Angola. PLoS One 13(12), e0209801 (2018).
Yaya, S. et al. Determinants of unmet need for family planning in Gambia & Mozambique: implications for women’s health. BMC Women’s Health 21, 1–8 (2021).
Mulenga, J. N. et al. Determinants of unmet need for family planning among married women in Zambia. J. Public Health Afr. 11(1), 7 (2020).
Nkoka, O. et al. Multilevel analysis of factors associated with unmet need for family planning among Malawian women. BMC Public Health 20, 1–12 (2020).
Ferdousi, S. et al. Unmet need of family planning among rural women in Bangladesh. J. Dhaka Med. Coll. 19(1), 11–15 (2010).
Hameed, W. et al. Determining the factors associated with unmet need for family planning: a cross-sectional survey in 49 districts of Pakistan. Pak. J. Public Health 1(1), 21 (2011).
Wilopo, S. A. et al. Levels, trends and correlates of unmet need for family planning among postpartum women in Indonesia: 2007–2015. BMC Women’s Health 17, 1–14 (2017).
Hailemariam, A. & Haddis, F. Factors affecting unmet need for family planning in southern nations, nationalities and peoples region, ethiopia. Ethiop. J. Health Sci. 21(2), 77–89 (2011).
Korra, A. Attitudes Toward Family Planning and Reasons for Nonuse Among Women with Unmet Need for Family Planning in Ethiopia (Citeseer, 2002).
Oginni, A. B., Ahonsi, B. A. & Adebajo, S. J. Trend and determinants of unmet need for family planning services among currently married women and sexually active unmarried women aged 15–49 in Nigeria (2003–2013). Afr. Popul. Stud. 29(1), 1483–1499 (2015).
GMeskel, A. T., Desta, H. O. & Bala, E. T. Factors associated with unmet need for family planning among married reproductive age women in Toke Kutaye District, Oromia, Ethiopia. Int. J. Reprod. Med. 2021, 5514498 (2021).
Bhusal, C. K. & Bhattarai, S. J. Factors affecting unmet need of family planning among married Tharu women of Dang District, Nepal. Int. J. Reprod. Med. 2018, 1–9 (2018).
Tadele, A., Abebaw, D. & Ali, R. Predictors of unmet need for family planning among all women of reproductive age in Ethiopia. Contracept. Reprod. Med. 4(1), 6 (2019).
Ayele, W. et al., Trends and determinants of unmet need for family planning and programme options, Ethiopia. 2011 (2005).
Kisaakye, P.J.E.S.J. Determinants of unmet need for contraception to space and limit births among various groups of currently married women in Uganda. Eur. Sci. J. 9(19) (2013).
Wulifan, J. K. et al. A scoping review on determinants of unmet need for family planning among women of reproductive age in low and middle income countries. BMC Women’s Health 16, 1–15 (2015).
Korra, A. Attitudes toward family planning and reasons for nonuse among women with unmet need for family planning in Ethiopia. (2002).
Oldenburg, C. E. et al. Distance to primary care facilities and healthcare utilization for preschool children in rural northwestern Burkina Faso: results from a surveillance cohort. BMC Health Serv. Res. 21(1), 212 (2021).
Stock, R. Distance and the utilization of health facilities in rural Nigeria. Soc. Sci. Med. 17(9), 563–570 (1983).
Opaluwa, T. T. Effect of distance on utilization of health care services in Rural Kogi State, Nigeria. J. Hum. Ecol. 35, 1–9 (2017).
Acknowledgements
The authors would like to thank Haramaya University College of Health and Medical Science for its cooperation in providing the study. The authors would also like to express their gratitude to study participants in the region for their genuine cooperation during the data collection and throughout the study.
Author information
Authors and Affiliations
Contributions
N.Y. conceived and designed the study. N.Y., M.D., N.A., and I.M. drafted the manuscript, and N.Y. was the P.I. of the review. N.Y., M.D., N.A., and I.M. developed search strings. Both reviewers (N.Y., M.D., N.A., and I.M.) screened and selected studies. N.Y. and I.M. evaluated the quality of the studies. N.Y., M.D., N.A., and I.M. performed analyses and interpretations. Both authors have rigorously reviewed, read, and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
Ethical approval was obtained from the Institutional Health Research Ethics Review Committee (IHRERC) of Haramaya University, College of Health Sciences, by formal letter with a reference number. IHRERC/04/2018. Support letters from the College of Health Sciences were submitted to the selected kebeles where the study was conducted. After getting all permission letters from the responsible body and being informed, voluntarily, written informed consent was signed by study participants. Confidentiality was maintained by using codes instead of the participant’s name. Participants were also informed that they had the full right to refuse participation or withdraw at any time from the research. All methods were performed following relevant guidelines and regulations in the Declaration of Helsinki.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yigazu, N., Demene, M., Assefa, N. et al. Eight out of every twenty-five married women have an unmet need for family planning in Meyu Muluke District, Eastern Ethiopia. Sci Rep 15, 13761 (2025). https://doi.org/10.1038/s41598-025-91297-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-91297-1
