
Abstract
Hepatitis B-related acute-on-chronic liver failure (HBV-ACLF) could result in disrupted glucose and lipid homeostasis, but its associations with ACLF is not fully defined. Here, we incorporated biomarkers associated with HBV-ACLF prognoses into a predictive nomogram, and examined its short- and long-term predictive capabilities. Eight hundred sixty-one HBV-ACLF, 20 healthy, and 54 chronic hepatitis B (CH) patients were recruited; the 4 characteristics most strongly associated with HBV-ACLF prognoses (age, glycosylated serum protein [GSP], high-density lipoprotein cholesterol [HDL-c], international normalized ratio), identified by logistic regression (uni-, multivariate) and machine-learning based analyses, were incorporated into the predictive nomogram. The nomogram was, under receiver operating characteristic and calibration curve analyses, highly accurate in identifying ACLF patients with worse prognoses after 28- and 90-days; it also demonstrated good clinical utility under decision curve analysis. Furthermore, higher GSP/HDL-c (GHR) was associated with worse ACLF prognoses, plus higher 28- and 90-day cumulative risk of death under Kaplan-Meier analysis. Therefore, the nomogram was able to accurately identify ACLF patients, who also had high GHR, at high risk for adverse prognosis; consequently, both glucose and lipid metabolism indicators are equally important for determining ACLF prognoses, and could serve as valuable early diagnostic tools for tailored ACLF interventions.
Similar content being viewed by others

Introduction
Hepatitis B-related acute-on-chronic liver failure (HBV-ACLF) is a clinical syndrome, comprising of acute liver failure in the context of pre-existing chronic liver disease or cirrhosis1. Its prognosis is poor, and mortality high, ranging from ~ 30–70%2. HBV-ACLF treatment initially involves the application of supportive therapies, such as the antivirals tenofovir, tenofovir alafenamide or entecavir, all of which are nucleoside analogues that could lower HBV DNA levels3, as well as antibiotics to counteract against concurrent bacterial infections3. Additionally, an artificial liver support system (ALSS), which operates similarly to kidney dialysis machines in removing toxins from plasma, has been observed by Lan et al. to increase 1-year survival rates for HBV-ACLF4. However, these therapies may not be effective in stabilizing the conditions of ACLF patients. As a result, the sole effective treatment for ACLF, particularly for those where supportive treatment have failed, is liver transplantation5,6, but its application has been limited owing to donor organ shortages, surgical difficulties, and multiple post-operative complications7. Therefore, early prognostic assessment of ACLF is essential for developing effective treatment regimens, which would be greatly aided by identifying strongly predictive biomarkers, enabling clinicians to discriminate between different types and risk levels of LF. In recent years, proteomics and metabolomics have been widely used to identify those biomarkers and aid in the prognostic assessment of LF patients8,9,10.
One such potential biomarker is semaphorin-6B, whose expression was observed by Yang et al. to be significantly higher among HBV-ACLF patients, particularly in liver macrophages and hepatocytes. This increased expression was associated with increased macrophage inflammatory responses, along with apoptosis in hepatocytes, both of which contributed to lowered liver regenerative capabilities and increased dysfunction after HBV infection, and subsequently ACLF pathogenesis11. The association between increased inflammation and HBV-ACLF occurrence was further supported by Zhang et al., who found that HBV-ACLF patients had significantly increased NOD-like receptor protein 3 (NLRP3) inflammasome activation, which could be counteracted by rapamycin-induced autophagy12. Additionally, increased hepatocyte apoptosis, in turn, results in lowered fibroblast growth factor 21 (FGF21), which, along with increased growth differentiation factor 15 (GDF15) from macrophages, have been linked to increased mitochondrial dysfunction13. This dysfunction results in lowered ATP production and pathogenic metabolic remodeling, the latter owing to dysfunctional mitochondria being less able to produce ATP from glucose, fatty acids, and proteins via oxidative phosphorylation. All these pathological molecular and cellular changes may ultimately contribute to metabolic dysfunction and alterations in indicators. In fact, it is well-known that cirrhosis patients often suffer from malnutrition and energy metabolic disorders. In particular, protein malnutrition increases mortality risk and lowers survival rates14,15,16,17. However, despite the presence of an association between dysfunctional metabolism and ACLF, the specific roles of lipid and glucose metabolism still have not been fully elucidated, though a study from Fan et al. found that ACLF patients had lower resting energy expenditure and increased lipid oxidation18.
In this study, we aimed to establish a comprehensive, effective model for early prediction of Hepatitis B-related ACLF prognoses, via examining the association of multiple patient characteristics, particularly lipid and glucose metabolism indicators, with different prognoses. We identified the 4 most predictive indicators, and incorporated them into a predictive nomogram, which was highly accurate and had great clinical utility for identifying patients more at risk for adverse ACLF prognoses, over both 28- and 90-day examination periods. Furthermore, for the first time, we examined the linkages between glucose and lipid metabolism disorders, with respect to ACLF prognosis, and found that the ratio between long-term blood glucose levels, as represented by glycosylated serum protein (GSP), and high-density lipoprotein cholesterol (HDL-c) was associated with poorer prognoses and higher mortality. Therefore, this predictive nomogram and GSP/HDL-c ratio could serve as valuable early diagnostic tools to flag ACLF patients at risk for adverse prognoses.
Materials and methods
Patient recruitment, inclusion, and exclusion criteria
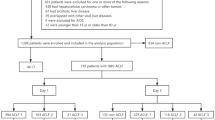
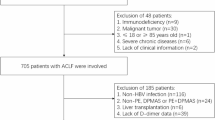
A total of 861 patients with Hepatitis B-related ACLF, as well as 20 healthy patients and 54 patients with chronic hepatitis B (CH), who visited the Department of Infectious Diseases of the First Affiliated Hospital of Nanchang University from January 2013-December 2023, were recruited. ACLF was diagnosed based on the following Asia-Pacific Association for the Study of the Liver (APASL)19 diagnostic criteria: acute liver injury manifesting as severe jaundice (serum bilirubin [Bil] ≥ 5 mg/dl) and coagulopathy (international normalized ratio [INR] ≥ 1.5 or prothrombin activity [PTA] ≤ 40%). Aside from (1) ACLF, other inclusion criteria were (2) Patients with previously diagnosed or undiagnosed chronic liver disease, along with having hepatic encephalopathy and/or ascites within 4 weeks prior to hospitalization. Exclusion criteria were as follows: (1) Other systemic diseases, such as cancer, HIV, previous renal insufficiency or heart failure, (2) Other chronic liver diseases, such as autoimmune or hereditary metabolic liver disease, (3) Pregnant, breastfeeding, or childbearing-aged women not taking contraceptives, or (4) Incomplete clinical data. The 861 ACLF patients were randomly divided in a 7:3 ratio into training (603) and validation (258) datasets.
Data collection, biomarker measurement, and classifying ACLF prognoses
All patient data were obtained from electronic medical records, including general clinical information upon first admission: name, gender, age, admission and discharge times, hospitalization length, past medical history, and secondary complications. During hospitalization, fasting venous blood was collected from all patients, and serum levels of alanine aminotransferase (ALT), aspartate aminotransferase (AST), total Bil (TBil), direct Bil (DBIL), albumin (ALB), globulin (GLB), γ-glutamyl transferase (GGT), creatinine (Cr), fasting blood glucose (FBG), GSP, total cholesterol (TC), triglycerides (TG), HDL-c, low-density lipoprotein cholesterol (LDL-c), as well as Na+, prothrombin time (PT), PTA, INR, white blood cell (WBC), hemoglobin (HGB), platelet (Platelet), neutrophil (NEUT), and lymphocyte counts, plus α-fetoprotein (AFP) were measured. Additionally, AST/ALT ratio was defined as AAR, and Model for End-Stage Liver Disease (MELD) score was calculated with the following formula20: 3.78×LN(TBil[mg/dL]) + 11.2×LN(INR) + 9.57×LN(Cr[mg/dL]) + 6.43 × 0 or 1 for respectively, cholestatic/alcoholic liver disease, or all other causes.
From the MELD score, the following formula was used to calculate i-MELD21: MELD score + 0.3×age–0.7×Na++100.
Patients were examined 28-and 90-day periods, and poor ACLF prognoses were defined as voluntary discharge, death, or liver transplantation.
Constructing the predictive nomogram and statistical analyses
All statistical analyses were performed with R software (version 4.1.3, URL:https://cran.r-project.org) and GraphPad Prism (version 8.0.2, URL:http://www.graphpad.com). Quantitative data were expressed as mean ± standard deviation (SD) if normally distributed, and median (25–75% quartile) if not. Categorical data were expressed as frequencies and proportions. Data analyses between 2 groups were carried out using either the Student’s t test or the non-parametric Mann-Whitney U test. P < 0.05 was considered statistically significant.
To identify the key metabolic indicators associated with HBV-ACLF, univariate logistic regression analysis was first used, and indicators with statistical significance were subsequently incorporated into the multivariate logistic regression analysis, as well as by 3 machine learning-based analyses: (1) Least absolute shrinkage and selection operator (LASSO) regression analysis, which is used for regularizing data, thereby improving prediction accuracy and model comprehensibility, as well as enabling variable selection22; this was performed by the glmmet package of R software. (2) Random forest (RF) analysis, using the eponymous package in R software, which possess the advantages of being unrestricted in terms of variable conditions, as well as higher accuracy, sensitivity, and specificity23. Based on identifying the optimal value for RF “trees”, 1000 were selected for analysis. (3) Support vector machine (SVM) analysis, performed by the kernlab package of R software, which is a powerful method that aims to establish a threshold value between 2 categories, thereby allowing label prediction based on single or several featured vectors24. Cross-indicators among the 3 machine-based learning analyses thus were considered as key predictive indicators for HBV-ACLF prognoses, which were then incorporated into the predictive nomogram constructed using the rms package of R. The discriminatory abilities of that nomogram for patients at risk for HBV-ACLF were evaluated using receiver operator characteristic (ROC) analysis by the pROC package, in which higher accuracy corresponded to areas under the curve (AUC) values closer to 1. The extent of agreement between predicted and actual ACLF occurrence was evaluated by calibration curve analysis, while decision curve analysis (DCA) examined the clinical utility of the nomogram. Cumulative risk of death over the 28- and 90-day evaluation periods were analyzed by Kaplan-Meier and verified using the log-rank test.
Results
Clinical characteristics of the subjects
Table 1 compares patient characteristics between 20 healthy controls, 54 CH, and 861 patients with Hepatitis B-related ACLF. We found that significant differences between the 3 groups in terms of the proportion of males, with ACLF having the highest percentage (35 vs. 70 vs. 87.6%). Additionally, for liver functional indicators, ACLF had significantly higher ALT, AST, TBil, DBIL, and GGT, along with lower ALB and GLB than Control and CH. With respect to coagulation functional indicators, ACLF, compared to Control and CH, had significantly higher PT and INR, along with lower PTA; the worsening of those indicators was consistent with acute liver injury characteristics. In terms of glucose metabolism, ACLF had significantly lower FBG, but higher GSP than for Control and CH, while for lipids, significantly lower TC, TG, HDL-c, and LDL-c levels were present in ACLF, compared to Control and CH. Furthermore, ACLF had the highest MELD and i-MELD scores versus the other 2 groups. All these findings thus indicate that alterations in glucose and lipid metabolism may be associated with ACLF prognoses.
Identifying the predictive metabolic indicators associated with HBV-ACLF prognoses
To identify the indicators most predictive of 28-day HBV-ACLF survival, univariate logistic regression analysis on the 603 training set patients was first used, in which 13 statistically significant indicators were identified (Table 2). Multivariate logistic regression analysis was then used on those 13 indicators (age, Cr, GSP, TG, HDL-c, Na+, PT, PTA, INR, WBC, MELD score, bacterial infection, artificial liver treatment), in which 8 were still statistically significant: age, Cr, GSP, HDL-c, INR, WBC, MELD score, and bacterial infection (Table 2). In terms of the 3 machine-learning analyses, LASSO identified 6 (age, GSP, HDL-c, Na+, PT, and INR; Fig. 1A-B), RF identified 9 (PTA, PT, INR, Na+, MELD, HDL-c, age, WBC, and GSP; Fig. 1C-D), based on its calculation of the importance of each indicator, and SVM identified 12 indicators (age, Cr, GSP, HDL-c, Na+, PT, PTA, INR, WBC, MELD, infection, and artificial liver treatment; Fig. 1E). From those 4 analyses of multivariate logistic regression, LASSO, RF, and SVM, 4 indicators: age, GSP, HDL-c, and INR were shared by all of them (Fig. 1F).

Applying the 3 machine-learning analyses to identify the predictive metabolic indicators associated with Hepatitis B-related acute-on-chronic liver failure (ACLF) prognoses. (A) Least absolute shrinkage and selection operator (LASSO) regression with 13-fold cross-validation, corresponding to the 13 statistically significant ACLF patient indicators found from univariate logistic regression analysis, was used to reduce the dimension of the grouping characteristics. (B) 6 indicators corresponded to the minimum error: age, glycosylated serum protein (GSP), high-density lipoprotein cholesterol (HDL-c), Na+, prothrombin time (PT), and international normalized ratio (INR). (C) 13-fold cross-validation error plot from random forest (RF) analysis. (D) 9 indicators were identified from RF, based on a cut-off threshold of 20: prothrombin activity (PTA), PT, INR, Na+, Model for End-Stage Liver Disease (MELD), HDL-c, age, white blood cell (WBC), and GSP. (E) Support vector machine (SVM) analysis identified 12 indicators: age, creatinine, GSP, HDL-c, Na+, PT, PTA, INR, WBC, MELD, infection, and artificial liver treatment. (F) Venn diagram showing the number of shared indicators between multivariate logistic regression, LASSO, RF, and SVM.
Constructing and validating the predictive nomogram for 28- and 90-day HBV-ACLF prognoses
The 4 factors identified by multivariate Cox, LASSO, RF, and SVM (age, GSP, HDL-c, INR) were all incorporated into the predictive nomogram for HBV-ACLF prognoses (Fig. 2). The discriminatory capabilities and accuracies of the predictive nomogram were subsequently evaluated using ROC curve analysis, in which for 28-day ACLF survival, the AUC was 0.763 (0.722–0.804; Fig. 3A), indicating high discriminatory capabilities and accuracy. DCA analysis also showed that the nomogram had great clinical utility, compared to not using the nomogram (Fig. 3B), and a high correspondence between predicted and actual probabilities for 28-day ACLF survival was found under calibration curve analysis (P = 0.810; Fig. 3C). Similar findings were found when applying the nomogram for predictive 90-day ACLF survival, in which the AUC was 0.764 (0.726–0.802) in the ROC curve analysis (Fig. 3D). Furthermore, good clinical utility was also present in the DCA analysis (Fig. 3E), as well as a high degree of correlation between predicted and actual prognoses (P = 0.850; Fig. 3F). The calibration curve results, for both 28-, at P = 0.810, and 90-day ACLF survival, at P = 0.850, thus indicated that the results from the nomogram matched, to a high degree, the actual ACLF prognoses, as no significant difference between predicted and actual probabilities were present. With respect to clinical utility, in DCA for both 28- and 90-day ACLF survival, the threshold probability for the nomogram was higher than for “all HBV-ACLF patients” or “no HBV-ACLF patients”, indicating that it had greater clinical utility than assuming that all, or no HBV-ACLF patients, would have worse prognoses over both 28- and 90-day periods. Moreover, the high accuracy of the predictive nomogram was further verified by the validation set, in which the AUC was 0.740 (0.670–0.810; Fig. 3G); additionally, just like for 28- and 90-day HBV-ACLF model, there was good clinical utility (Fig. 3H) and high correlation between predicted and actual prognoses (P = 0.938; Fig. 3I).

Predictive nomogram for 28- and 90-day HBV-ACLF prognoses.

Validation of the predictive nomogram for 28- and 90-day HBV-ACLF prognoses. (A) Receiver operating characteristic (ROC), (B) Decision (DCA), and (C) Calibration curve analyses of the predictive nomogram for 28-day HBV-ACLF prognoses, based on the training set. (D) ROC, (E) DCA, and (F) Calibration curve analyses of the nomogram for 90-day ACLF prognoses, based on the training set. (G) ROC, (H) DCA, and (I) Calibration curve analyses of the nomogram for the validation set.
Higher GSP/HDL-c index (GHR) was associated with worse HBV-ACLF prognoses
To further examine the effects of 2 major glucose and lipid metabolism indicators, GSP and HDL-c, on HBV-ACLF patient prognoses, GHR was calculated for all 861 patients; they were divided into 2 groups (Q1-2), based on whether they were below or above the median value of 3.36 (Table 3). Q2 (GHR > 3.36) patients had significantly higher occurrence of ACLF with adverse prognoses after the 28- and 90-day examination periods, as well as gastrointestinal bleeding, hepatorenal syndrome, and using artificial liver treatment (Table 3). These findings were consistent with them also having the highest MELD and i-MELD scores (Table 3). Indeed, the association between higher GHR and adverse ACLF prognoses were further supported by the Kaplan-Meier analysis, where Q2 patients had higher cumulative risk of death, over both 28- (Fig. 4A) and 90-days (Fig. 4B).

Kaplan-Meier analyses for (A) 28- and (B) 90-day examination periods.
Discussion
Severe damage to liver function results in LF, which manifests as coagulation dysfunction, hepatic encephalopathy, and other pathological conditions25. In China, LF make up most of the ~ 1 million/year liver disease deaths26. As LF is hard to treat27, effective and comprehensive prognosis assessment of LF patients, to facilitate early intervention, has become an issue of significant interest for clinicians. In this study, 861 Hepatitis B-related ACLF patients were recruited and found, consistent with ACLF diagnoses, to have worse liver and coagulative functional indicators, compared to healthy controls and patients with chronic Hepatitis B. We then conducted univariate logistic regression analysis of patient characteristics and found 13 significant indicators for adverse ACLF prognoses. Univariate logistic regression analysis was followed by multivariate logistic regression analysis, as well as the 3 machine-learning analyses LASSO, RF, and SVM; there, the number of indicators identified were, respectively, 8, 6, 9, and 12. Among those 4 analyses, age, GSP, HDL-c, and INR were common to all of them. These indicators were then incorporated into a predictive nomogram, in which they were highly predictive and possess great clinical utility for identifying patients prone to adverse ACLF prognoses after both 28- and 90-day examination periods. We also found that patients with higher GHR also had worse ACLF outcomes after those examination periods, as well as increased gastrointestinal bleeding, hepatorenal syndrome, plus MELD and i-MELD scores. In fact, this study is one of the first to link the glucose metabolism indicator GSP, and the lipid metabolism indicator HDL-c, to MELD score, which has long been used to predict adverse prognoses and mortality among ACLF patients. For instance, a study showed that Child-Turcotte-Pugh grade > 12 and MELD > 28 were independent predictors of ACLF mortality28. MELD-Na and i-MELD scores were then derived from MELD by other researchers after additional optimization29. As for age and INR, they have been widely accepted as key predictive indicators for adverse ACLF prognoses.
With respect to GSP and HDL-c, the liver has been noted to play an important role in glucose metabolism, and excess liver damage could disrupt proper glucose homeostasis, leading to hypoglycemia, impaired glucose tolerance, and diabetes in patients with severe liver disease30. Additionally, hypoglycemia and transient hyperglycemia can also occur in patients with severe acute hepatitis and acute LF31. However, the impact of these metabolism disorders on ACLF prognosis is still largely unknown32,33, though Hu et al. noted that glucose metabolism disorders in ACLF patients may be different than in cirrhosis, in that such disorders in ACLF may be caused by the stress response of liver function loss and acute systemic inflammation34. Additionally, in chronic Hepatitis B virus (HBV)-related ACLF, diabetes was associated with high mortality34. All these findings indicated that ACLF patients also tend to have complex glucose homeostasis disorders; for instance, hyperglycemia could increase mortality, but its strict control could result in hypoglycemia, which also increases mortality35. In line with those observations, our investigations found that ACLF patients had lower FBG levels compared to CH and healthy controls, which may be owed to short-term hypoglycemia upon initial admission. On the other hand, their GSP level, which reflects their longer-term blood glucose status, is significantly higher than for CH and healthy individuals. Therefore, ACLF patients, compared to CH or healthy ones, have greater instability in blood glucose levels, pointing to them developing complex glucose homeostasis disorders, which otherwise may be overlooked from just examining FBG levels. In fact, GSP was found to be more valuable than FBG in determining 28-day adverse prognosis likelihoods for HBV-ACLF patients. Therefore, GSP is more reliable as an indicator of the longer-term glucose metabolic state of a patient, compared to merely testing FBG at a specific time point, for predicting HBV-ACLF prognoses.
Lipid metabolism, compared to glucose, has been more documented as a subject of analysis for evaluating ACLF prognosis. Indeed, our study found that compared to healthy individuals, HBV-ACLF patients had lower TC and TG, which may be related to malnutrition. Furthermore, we found that HDL-c levels were an independent risk factor for ACLF prognosis, in which lower levels were associated with worse prognoses, which were in accordance with previous studies, such as one involving 530 HBV-ACLF patients, which showed that HDL-c levels had some prognostic potential, where higher levels were associated with higher survival rates36. Similarly, in a retrospective cohort study of 200 HBV-ACLF patients, significant differences in HDL-c levels were found between dead patients versus those who survived the 28-day examination period37. All these findings have led to the likes of Trieb et al.38 to conclude that HDL-c is a powerful predictor of LF progression and survival, which may be due to it being involved in regulating ACLF patient immune function and infection responses39,40. More specifically, another study has shown that HDL-c regulates cell membrane cholesterol levels by removing excess cholesterol and other lipid substances, leading to reductions in inflammatory receptor signaling41. HDL-c could also lower cytokine production by binding to LPS. All this evidence indicates that reducing HDL-c levels could result in decreased anti-inflammatory activity, which may serve as the underlying basis behind HBV-ACLF patients having poor prognoses42,43,44.
Based on the wealth of previous findings, we thus examined whether any connections between both pathological glucose and lipid metabolism, with respect to ACLF prognosis, may be present. In fact, we found that higher GHR, obtained from the GSP to HDL-c ratio, was associated with worse laboratory indicators, higher incidence of complications, and poor prognosis after 28- and 90-days of examination, all of which contributes to the higher cumulative mortality risk found in the Kaplan-Meier analysis. Therefore, the combination of higher long-term blood glucose levels, as indicated by GSP, coupled with lower HDL-c, is a major predictive factor for more adverse HBV-ACLF prognoses.
There are a number of limitations in this study, one of which is that it is a single-center, retrospective one, which may not be fully representative of all ACLF patients; thus, future prospective studies, with larger sample sizes and multiple centers, should be carried out to verify the present findings. Another limitation is the lack of longer-term follow-up data, particularly in terms of the changes in indicators after 90-days. This is owed to HBV-ACLF having a high mortality rate during the short-term periods of 28- and 90-day follow-up periods, meaning that those who survive afterwards are more likely to have favorable prognoses. Indeed, Xiao et al. found that HBV-ACLF survival rates after 90 days was 48.8%; this rate only slightly decreased after 1, 5, and 8 years, with survival rates being, respectively, 46.1%, 43.8%, and 42.2%45, indicating that if an individual survives after 90 days, they are still likely to be alive afterwards, for up to 8 years. As a result, little change would be present for longer-term follow-up with respect to survival rates, and consequently their correlations with clinical indicators. Nevertheless, future studies should examine the associations between alterations in clinical indicators with longer-term HBV-ACLF prognoses. Additionally, the study did not fully investigate the role of cardiometabolic risk factors, such as insulin resistance, on HBV-ACLF prognoses, though it had been noted by Hu et al. that in a group of 96 ACLF patients, those with diabetics had significantly higher 90-day mortality rates34. Further studies should therefore be conducted to elucidate the influence of such cardiometabolic disturbances on ACLF prognoses. Likewise, the postulation that lower FBG levels reflect short-term hypoglycemia upon admission, while higher GSP reflects the longer-term metabolic state of an HBV-ACLF patient, requires further confirmation. Consequently, future studies should increase the number of cases for both control and CH groups, as well as monitor changes of glucose and lipid indexes at different times in the follow-up, thereby providing more matched comparisons among control, CH, and ACLF groups to minimize the influence of errors.
Conclusion
In summary, we found that our predictive nomogram, incorporating age, GSP, HDL-c, and INR, were highly accurate in identifying patients with adverse Hepatitis B-related ACLF prognoses, along with possessing great clinical utility, both after short- and long-term periods. Furthermore, high GHR levels were associated with worse ACLF prognoses and higher mortality risk. These findings thus indicate that both the predictive nomogram and GHR could be useful approaches to facilitate early intervention against ACLF. Furthermore, both glucose and lipid metabolism markers should also be accounted for when developing predictive HBV-ACLF models.
Data availability
The data used to support the findings of this study are available from the corresponding author upon request.
References
Shi, P. et al. Efficacy and predictive factors of glucocorticoid therapy for patients with hepatitis B virus-related acute-on-chronic liver failure. Acta Gastroenterol. Belg. 85(4), 593–600. https://doi.org/10.51821/85.4.10728 (2022).
Grek, A. & Arasi, L. Acute liver failure. AACN Adv. Crit. Care. 27, 420–429 (2016).
Luo, J. et al. Acute-on-chronic liver failure: far to go-a review. Crit. Care. (Lond., Engl.) 27(1), 259. https://doi.org/10.1186/s13054-023-04540-4 (2023).
Lan, X. et al. Artificial liver support system improves one-year prognosis of patients with hepatitis B virus-associated acute-on-chronic liver failure. J. Gastroenterol. Hepatol. https://doi.org/10.1111/jgh.16883 (2025).
Bernal, W. et al. Acuteon-chronic liver failure. Lancet 386(10003), 1576–1587 (2015).
Liu, X. Y., Peng, F., Pan, Y. J. & Chen, J. Advanced therapeutic strategies for HBVrelated acute-on-chronic liver failure. Hepatobiliary Pancreat. Dis. Int. 14(4), 354–360 (2015).
Lin, H. et al. Identification of key candidate genes and pathways in hepatitis B virus-associated acute liver failure by bioinformatical analysis. Med. (Baltim). 97(5), e9687. https://doi.org/10.1097/MD.0000000000009687 (2018).
Bajaj, J. S. et al. Serum levels of metabolites produced by intestinal microbes and lipid moieties independently associated with acute on chronic liver failure and death in patients with cirrhosis. Gastroenterology (2020).
Moreau, R. et al. Blood metabolomics uncovers inflammation-associated mitochondrial dysfunction as a potential mechanism underlying ACLF. J. Hepatol. (2019).
Lopez-Vicario, C. et al. Targeted lipidomics reveals extensive changes in Circulating lipid mediators in patients with acutely decompensated cirrhosis. J. Hepatol. 73, 817–828 (2020).
Yang, H. et al. SEMA6B induces macrophage-mediated inflammation and hepatocyte apoptosis in hepatitis B virus-related acute-on-chronic liver failure. Theranostics 14(13), 5200–5218. https://doi.org/10.7150/thno.97007 (2024).
Zhang, X. et al. IRGM/Irgm1 increases autophagy to inhibit activation of NLRP3 inflammasome in inflammatory injury induced acute liver failure. Cell. Death Discov. 10(1), 272. https://doi.org/10.1038/s41420-024-02052-w (2024).
Zhang, Y. et al. Mitochondrial dysfunction affects hepatic immune and metabolic remodeling in patients with hepatitis B virus-related acute-on-chronic liver failure. World J. Gastroenterol. 30(8), 881–900. https://doi.org/10.3748/wjg.v30.i8.881 (2024).
Guglielmi, F. W. et al. Nutritional state and energy balance in cirrhotic patients with or without hypermetabolism: multicentre prospective study by the ‘nutritional problems in gastroenterology’ section of the Italian society of gastroenterology (SIGE). Dig. Liver Dis. 37, 681–688 (2005).
Tajika, M. et al. Prognostic value of energy metabolism in patients with viral liver cirrhosis. Nutrition 18, 229–234 (2002).
Müller, M. J. Malnutrition and hypermetabolism in patients with liver cirrhosis. Am. J. Clin. Nutr. 85, 1167–1168 (2007).
Peng, S. et al. Body composition, muscle function, and energy expenditure in patients with liver cirrhosis: a comprehensive study. Am. J. Clin. Nutr. 85, 1257–1266 (2007).
Fan, C.-L. et al. Resting energy expenditure and glucose, protein and fat oxidation in severe chronic virus hepatitis B patients. World J. Gastroenterol. 14, 4365–4369 (2008).
Sarin, S. K. et al. Acute-on-chronic liver failure: consensus recommendations of the Asian Pacifc association for the study of the liver (APASL): an update. Hepatol. Int. 13(4), 353–390 (2019).
Forman, L. M. & Lucey, M. R. Predicting the prognosis of chronic liver disease: an evolution from child to MELD. Hepatology 33(2), 473–475 (2001).
Jalan, R. et al. Development and validation of a prognostic score to predict mortality in patients with acute-on-chronic liver failure. J. Hepatol. 61(5), 1038–1047 (2014).
Spruss, A. et al. Toll-like receptor 4 is involved in the development of fructose-induced hepatic steatosis in mice. Hepatology 50(4), 1094–1104 (2009).
Pérez-Hernández, A. I. et al. Mechanisms linking excess adiposity and carcinogenesis promotion. Front. Endocrinol. (Lausanne) 5, 65 (2014).
Giovannucci, E. Nutrition, insulin, insulin-like growth factors and cancer. Horm. Metab. Res. 35 (11–12), 694–704 (2003).
Mizuguchi, T. et al. Preoperative liver function assessments to estimate the prognosis and safety of liver resections. Surg. Today. 44(1), 1–10 (2014).
D’SOUZA, S. E. D. H. O. M. D. Viral hepatitis and acute liver failure: still a problem. Clin. Liver Dis. 22(2), 289–300 (2018).
LIN, H. et al. Identification of key candidate genes and pathways in hepatitis B virus-associated acute liver failure by bioinformatical analysis [J]. Medicine 97 (5), e9687 (2018).
Choudhury, A. et al. APASL ACLF working party. Liver failure determines the outcome in patients of acute-on-chronic liver failure (ACLF): comparison of APASL ACLF research consortium (AARC) and CLIF-SOFA models. Hepatol. Int. 11, 461–471 (2017).
Li, C. et al. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 26(8), 539–543. https://doi.org/10.3760/cma.j.issn.2095-4352.2014.08.003 (2014).
Hamed, A. E. et al. Diabetes association with liver diseases: an overview for clinicians. Endocr. Metab. Immune Disord Drug Targets. 19, 274–280 (2019).
Vilstrup, H., Iversen, J. & Tygstrup, N. Glucoregulation in acute liver failure. Eur. J. Clin. Invest. 16, 193–197 (1986).
Bianchi, G. et al. Prognostic signifcance of diabetes in patients with cirrhosis. Hepatology 20, 119–125 (1994).
Hagel, S., Bruns, T., Herrmann, A., Stallmach, A. & Schmidt, C. Abnormal glucose tolerance: a predictor of 30-day mortality in patients with decompensated liver cirrhosis. Z. Gastroenterol. 49, 331–334 (2011).
Hu, H. et al. Diabetes is associated with poor short-term prognosis in patients with hepatitis B virus-related acute-on-chronic liver failure. Hep. Intl. 15(5), 1093–1102. https://doi.org/10.1007/s12072-021-10243-1 (2021).
Ruan, Y., Tan, G. D., Lumb, A. & Rea, R. D. Importance of inpatient hypoglycaemia: impact, prediction and prevention. Diabet. Med. 36, 434–443 (2019).
Wen, X., Tong, J., Yao, M., Hu, J. & Lu, F. Prognostic value of HDL-related biomarkers in patients with HBV-related ACLF. J. Hepatol. 75(1), 243–245. https://doi.org/10.1016/j.jhep.2021.02.019 (2021).
Zhang, Y., Chen, P., Zhang, Y., Nie, Y. & Zhu, X. Low high-density lipoprotein cholesterol levels predicting poor outcomes in patients with hepatitis B virus-related acute-on-chronic liver failure. Front. Med. 9, 1001411. https://doi.org/10.3389/fmed.2022.1001411 (2022).
Trieb, M. et al. HDL-related biomarkers are robust predictors of survival in patients with chronic liver failure. J. Hepatol. 73(1), 113–120. https://doi.org/10.1016/j.jhep.2020.01.026 (2020).
Tandon, P. & Garcia-Tsao, G. Bacterial infections, sepsis, and multiorgan failure in cirrhosis. Semin. Liver Dis. 28, 26–42 (2008).
Gustot, T., Durand, F., Lebrec, D., Vincent, J. L. & Moreau, R. Severe sepsis in cirrhosis. Hepatology 50, 2022–2033 (2009).
Iqbal, A. J. et al. Acute exposure to Apolipoprotein A1 inhibits macrophage chemotaxis in vitro and monocyte recruitment in vivo. Elife 5, 586. https://doi.org/10.7554/eLife.15190 (2016).
Levine, D. M., Parker, T. S., Donnelly, T. M., Walsh, A. & Rubin, A. L. In vivo protection against endotoxin by plasma high density lipoprotein. Proc. Natl. Acad. Sci. U S A 90, 12040–12044 (1993).
Hubsch, A. P., Casas, A. T. & Doran, J. E. Protective effects of reconstituted highdensity lipoprotein in rabbit gram-negative bacteremia models. J. Lab. Clin. Med. 126, 548–558 (1995).
McDonald, M. C. et al. Reconstituted high-density lipoprotein attenuates organ injury and adhesion molecule expression in a rodent model of endotoxic shock. Shock 20, 551–557 (2003).
Xiao, L. et al. The 90-Day survival threshold: a pivotal determinant of long-term prognosis in HBV-ACLF patients—insights from a prospective longitudinal cohort study. Adv. Sci. (Weinheim, Baden-Wurttemberg, Germany) 11(16), e2304381. https://doi.org/10.1002/advs.202304381 (2024).
Funding
The study was supported by the Health Commission of Jiangxi Province, China (202310025), and Jiangxi Provincial Administration of Traditional Chinese Medicine, China (2022B927).
Author information
Authors and Affiliations
Contributions
Wentao Zhu conceived the idea for the study and was a major contributor in writing the manuscript. Songsong Yuan managed the logistics for the study. Juan Liu and Wenfeng Zhang managed the logistics for this study and was a major contributor in revising the manuscript. Ying Zhu supervised the study. Qinglang Xu was a major contributor in revising the manuscript. Tianxin Xiang supervised the study. Xiaoping Wu conceived the idea for the study, designed and supervised the study, and provided all final approvals for all stages of the study. All authors read, reviewed, and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study was carried out according to the Declaration of Helsinki and was approved by the medical ethics committee of the First Affiliated Hospital of Nanchang University in China (no. IIT-2022-096). All patients provided written informed consent to participate in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yuan, S., Taozhu, W., Liu, J. et al. High glycosylated serum protein to high density lipoprotein cholesterol ratios are predictive of worse acute on chronic liver failure prognoses. Sci Rep 15, 14288 (2025). https://doi.org/10.1038/s41598-025-91779-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-91779-2
