
Abstract
Gait analysis systems are essential for rehabilitation but are often time-consuming and less accessible in low- and middle-income countries. GAITWell was developed to address these challenges with its portable and modular design for automated gait data collection and analysis. This study evaluates its methodological properties. GAITWell uses discrete binary sensors on interconnected plates to capture gait data, analyzed using the DBSCAN (Density-Based Spatial Clustering of Applications with Noise) algorithm, which identifies key reference points like foot contact and toe-off. DBSCAN detects clusters of arbitrary shapes and sizes, separates noise from data, and identifies natural patterns within the data space without prior group knowledge. Each plate measures 44 cm × 37 cm and has an 11 × 7 sensor array with 4 cm spacing. Test–retest reliability was evaluated using the intraclass correlation coefficient (ICC), standard error of the mean (SEM), and Bland–Altman plots. Concurrent validity was assessed by comparing GAITWell measurements to those from the Qualisys Pro-Reflex system. Results: 38 healthy adults participated (average age 33.2 years, SD 13.0). Correlations between GAITWell and Qualisys ranged from moderate (right step length) to very high (gait speed, cycle time, right and left step time, left step length, stance time, swing time, right and left cadence, and base of support). Moderate to good agreement was found for gait speed, cycle time, stride length, right and left step length, right and left step time, and stance and swing time, but poor agreement was observed for double support times, right and left cadence, and base of support. Preliminary analysis suggests that increasing sensor resolution could reduce measurement error by 70%. Conclusions: GAITWell is a promising tool, with future research focusing on enhancing sensor accuracy for improved reliability.
Similar content being viewed by others

Introduction
Gait analysis plays a fundamental role in both scientific research and clinical practice, serving as a compelling method for comprehensively understanding motor disorders and meticulously monitoring the progression of treatments1,2,3,4. The identification of abnormal locomotion patterns paves the way for personalized treatments that meet the specific needs of each patient, thus improving prognoses and reducing associated costs, especially in the context of rehabilitation5. Recent research underscores a significant increase in clinical gait analysis, with the number of references rising from only eight in 1973 to approximately 10.200 by 20206. This substantial growth highlights the expanding role of gait analysis in clinical diagnosis, rehabilitation, and biomechanical research. As a vital tool, gait analysis should be widely available and accessible to healthcare professionals across diverse settings to ensure all patients receive the highest standard of care tailored to their unique needs.
In clinical practice, simpler methods such as visual observation and functional mobility tests, including the Timed Up and Go (TUG)7and the 10-Meter Walk Test (10MWT)8, are commonly used due to their accessibility and ease of implementation. While these methods provide valuable insights into mobility and functional status, they lack the precision and objectivity offered by advanced gait analysis technologies. This gap underscores the need for solutions that balance accuracy and accessibility, particularly in resource-constrained settings.
Gait kinematic variables such as gait speed, step length, cadence, and other spatiotemporal parameters are crucial in both clinical and research settings for several reasons. Gait speed, for instance, serves as a fundamental indicator of overall mobility and functional status, making it a vital measure in assessing changes due to aging, neurological conditions, or rehabilitation interventions9,10. Step length provides insights into stride dynamics and can reveal asymmetries or compensatory mechanisms in gait patterns, aiding in the diagnosis and treatment planning for musculoskeletal disorders or post-surgical recovery11,12. Cadence, the number of steps per minute, correlates with energy expenditure and efficiency, influencing recommendations for physical activity and rehabilitation protocols13. These gait variables collectively offer quantitative metrics that enhance the precision of assessments, inform therapeutic strategies, and facilitate objective monitoring of treatment outcomes over time. By comprehensively analyzing these parameters, clinicians and researchers can tailor interventions more effectively, promote functional independence, and improve the quality of life for individuals with mobility impairments.
Despite the rapid increase in movement analysis facilities worldwide over the past 50 years6and the variety of gait analysis systems available—from portable solutions like the GAITRite system14and wearable sensors15,16to sophisticated laboratory-based optoelectronic setups17,18—access to clinical gait assessment remains limited. Significant barriers to widespread adoption include cost, the time-consuming nature of data collection, processing, and analysis, and the need for specialized personnel. Additionally, in the event of technical issues, the equipment often has to be sent to another country for repairs, which is particularly challenging for low- and middle-income countries that could greatly benefit from these technologies5,6. For example, sophisticated laboratory-based optoelectronic systems like Vicon19and Qualisys20,21, utilize multiple cameras and reflective markers to capture high-precision kinematic data. While these setups are considered the gold standard for gait analysis due to their accuracy and detailed motion capture capabilities, they require significant investment in equipment and infrastructure, as well as specialized personnel and time-consuming processes5. Wearable sensors, including inertial measurement units (IMUs) and accelerometers22,23,24, allow for continuous monitoring of gait patterns in real-world environments, giving valuable insights into daily movement and activity levels25,26,27. However, despite being simple to use and lower in cost compared to more sophisticated laboratory-based systems, they often require extensive and advanced programming for data analysis28. Similarly, insoles, equipped with pressure sensors and often integrated with machine learning algorithms, enable detailed analysis of gait parameters such as plantar pressure distribution and center of mass trajectory29,30. While these insoles are cost-effective, portable, and versatile, they may struggle with fine detail accuracy and durability issues under adverse conditions. Regular calibration and maintenance are essential to ensure optimal performance, and external factors like weather and surface unevenness can impact data accuracy31.
Among these systems, pressure mat systems are highly valued in both clinical and research settings for their ability to provide detailed gait analysis without requiring extensive personnel training, markers, or complex calibration procedures14,32,33,34. However, their implementation in low- and middle-income countries faces challenges such as the lack of technical support and infrastructure required for maintenance and calibration. Additionally, environmental factors such as high humidity, temperature variations, and limited access to stable power sources can impact the durability and accuracy of pressure mats. These barriers highlight the need for a more robust, adaptable, and user-friendly mat system that can perform reliably in diverse and resource-constrained settings.
Recognizing the critical need to enhance accessibility to gait analysis, an interdisciplinary team of professionals at the Bioengineering Laboratory of the Federal University of Minas Gerais (lab.bio), Brazil, has pioneered the development of a portable and modular system named GAITWell. This innovative system offers comprehensive hardware and software solutions for the automated extraction, processing, and analysis of human gait data. The present study evaluated the methodological properties of the GAITWell system in spatial and temporal gait analysis. Reliability was assessed by examining the system’s consistency in measuring gait parameters on two separate occasions, while concurrent validity was evaluated by comparing the results of the GAITWell system with those obtained from the gold-standard Qualisys system. The GAITWell system seeks to broaden access to precise gait analysis across diverse healthcare settings, which is particularly significant for Brazil, where innovative solutions are needed to enhance the availability and effectiveness of gait analysis technologies.
Results
Participated in the study 38 healthy adults, including 18 (47.4%) females, with a mean age of 33.2 years (SD 13.0) and BMI of 26.6 kg/m2 (SD 5.4). Of those, only 29 returned for the second visit, including 15 (50%) females, with a mean age of 33.0 years (SD 13.4) and BMI of 27.3 kg/m2 (SD 5.6).
Table 1 describes the mean and standard deviation of the gait variables obtained using the GAITWell and the Qualisys system during the first visit. Most of the correlations ranged from moderate to very high. Gait speed (r = 0.971, p < 0.001) and base of support (r = 0.914, p < 0.001) showed the strongest correlations. The only exception was stride length, which had a low but significant correlation with the Qualisys system (r = 0.360, p < 0.05).
The mean and standard deviations and the test–retest reliability results of the GAITWell system are described in Table 2. Reliability of the variables gait speed (ICC2,1 = 0.864, p < 0.001), stride length (ICC2,1 = 0.818, p = 0.001), cycle time (ICC2,1 = 0.847, p = 0.001), left step length (ICC2,1 = 0.764, p = 0.001), right step time (ICC2,1 = 0.821, p = 0.001), stance time (ICC2,1 = 0.837, p = 0.001) and swing time (ICC2,1 = 0.767, p = 0.001) achieved a good level of agreement. However, moderate reliability was observed for right step length (ICC2,1 = 0.650, p = 0.004) and left step time (ICC2,1 = 0.691, p = 0.001). Conversely, double support time (ICC2,1 = −0.344, p = 0.965), cadence of right (ICC2,1 = −0.528, p = 0.859) and left steps (ICC2,1 = −0.091, p = 0.588), and base of support (ICC2,1 = −0.639, p = 0.891) exhibited insufficient reliability, failing to attain statistical significance.
Figures 1 and 2 present Bland–Altman plots assessing the agreement between gait parameters measured using GAITWell and Qualisys Pro-Reflex systems obtained during visits 1 (V1) and 2 (V2). Descriptive data from the Qualisys system for V2 are not presented. In Fig. 1, for stride length, cycle time, and stance time, both systems demonstrated excellent agreement with minimal bias and narrow limits of agreement. The GAITWell exhibited slightly wider limits of agreement compared to Qualisys, but similar bias. In Fig. 2, for left step time, GAITWell also exhibited slightly wider limits of agreement compared to Qualisys, although the bias was similar between the two systems. Overall, both systems showed good agreement for the assessed gait parameters, with minimal bias and narrow limits of agreement for most parameters.

Bland–Altman analysis for gait speed, stride length, cycle time and stance time demonstrating reliability between visits 1 (V1) and 2 (V2) for the GAITWell system. Corresponding variables for the Qualisys system are included for visual comparison.

Bland–Altman analysis for swing time, right and left step length, and step time demonstrating reliability between visits 1 (V1) and 2 (V2) for the GAITWell system. Corresponding variables for the Qualisys system are included for visual comparison.
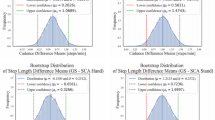
Figure 3 displays the Bland–Altman analysis for the GAITWell system and the Qualisys system, obtained during visits 1 (V1) and 2 (V2), focusing on variables that did not achieve reliability using the GAITWell system. Descriptive data from the Qualisys system for V2 is not presented. For the variables cadence and base of support, the GAITWell system was less consistent and reliable, showing greater variability compared to the Qualisys system, which demonstrated lower variability and more consistent measurements. For the variable double support time, the GAITWell system had similar bias compared to the Qualisys system but lower limits of agreement.

Bland–Altman analysis of the variables that did not achieve reliability (double support, right and left cadence and base of support) between visits 1 (V1) and 2 (V2) for the GAITWell system. Corresponding variables for the Qualisys system are included for visual comparison.
Discrepancies in sensor resolution
Further analysis was conducted due to the lack of reliability observed in some of the gait variables. This analysis explored the benefits of increasing the sensor resolution from 4 cm × 4 cm (Fig. 4a) to 1.2 cm × 1.2 cm (Fig. 4b) on the reliability of the GAITWell system. To quantify the potential reduction in error, we considered a scenario where the contact points of the heel and toe were positioned exactly in the middle between two sensors, thereby maximizing measurement error.

(a) Sensor resolution of 4 cm × 4 cm and (b) Sensor resolution of 1.2 cm × 1.2 cm, showing contact points of the heel and toe positioned exactly in the middle between two sensors.
Box 1 compares the 4 cm × 4 cm resolution with the proposed 1.2 cm × 1.2 cm resolution. The maximum systematic error occurs when the point of contact is halfway between two sensors; for a 4 cm × 4 cm grid, this distance is 2 cm. The spatial uncertainty, considering the distribution of sensors along the x and y axes, is calculated as 2.83 cm. With a sampling frequency of 1 kHz and an average speed of 0.72 m/s, for example, the temporal uncertainty, when converted to distance, is 0.72 cm. The quadratic combination of these uncertainties results in a total error of approximately 2.92 cm. With the adoption of a 1.2 cm resolution, the systematic error decreases to 0.6 cm, reducing the spatial uncertainty and total error, significantly enhancing measurement precision.
Figure 5 illustrates the impact of sensor resolution. Reducing the sensor resolution from 4 cm × 4 cm to 1.2 cm × 1.2 cm could potentially decrease the measurement error from 2 cm to 0.6 cm, representing a theoretical reduction of 70% in measurement error = [(2 − 0.6)/2] × 100 = 70%.

Comparison of Sensor Resolutions: (a) 4 cm × 4 cm and (b) 1.2 cm × 1.2 cm. The chart illustrates sensor area and maximum measurement error, highlighting a 70% error reduction with increased resolution.
Discussion
This study aimed to evaluate the methodological properties of the GAITWell system, a portable and modular technology designed to measure gait spatiotemporal parameters in healthy young adults. During testing, the hardware demonstrated remarkable durability, withstanding transport in a cargo vehicle under varying conditions, including paved roads, sidewalks, and temperatures ranging from 27 °C to 34 °C. Its robust design and protective features ensured reliable performance without any functional or structural issues, highlighting its suitability for field applications. The GAITWell system also combines portability and simplicity by utilizing hardware modules with binary logic sensors, eliminating the need for calibration even after extended transport or storage.
The GAITWell system demonstrated validity when compared with the gold standard Qualisys Pro-Reflex system, as well as excellent reliability, as evidenced by the Bland–Altman analyses presented in Figs. 1 and 2. For stride length, cycle time, and stance time, both systems exhibited excellent agreement, with minimal bias and narrow limits of agreement. Similarly, for gait speed and left step time, the bias was minimal, although GAITWell displayed slightly wider limits of agreement compared to Qualisys. These results indicate that GAITWell can reliably capture specific gait parameters, highlighting its potential utility in clinical and research settings where accurate assessment of stride length, cycle time, and stance time is essential. However, some limitations in reliability were observed for double support time, cadence, and base of support. Given the cyclic nature of gait, consistent measurement across all parameters is crucial for comprehensive gait analysis. The observed unreliability in these key variables undermines the system’s ability to accurately assess stability, balance, and symmetry35. To fully leverage the GAITWell system’s potential for clinical and research applications, it is essential to improve the reliability of these measurements. Enhancing the system’s capability to provide consistent and accurate data across all gait parameters will be crucial for effectively evaluating mobility and monitoring rehabilitation progress.
Preliminary results suggest that the lack of reliability may be attributed to the low resolution of the sensors used in the GAITWell system. Increasing the sensor resolution to 1.2 cm × 1.2 cm is projected to reduce the error in detecting heel contact and toe-off events by approximately 70% (Fig. 5). This improvement is vital for capturing subtle variations in gait dynamics, which are essential for accurate spatiotemporal parameter assessment. Unlike continuous measurement technologies used in pressure and force sensors, the GAITWell employs discrete sensors that operate at binary levels (0 and 1). The current spatial resolution of its 4 cm × 4 cm sensor array may not sufficiently capture fine movement variations in peripheral areas of the foot. This limitation can impact the accuracy of gait metrics such as double support time, as subtle variations in foot movement may be missed. The resolution of the sensor array affects data acquisition, classification, and processing, thereby influencing the precision of gait measurements.
Despite these improvements, our findings indicate that achieving high reliability remains a challenge even for gold standard systems. Bland–Altman plots (Fig. 3) showed that the GAITWell system generally exhibited minimal bias for double support time, and base of support, suggesting that these measurements are reasonably aligned with reference values. However, discrepancies were noted when comparing this to data from visit 2 with the Qualisys system (not reported here). Specifically, the Qualisys system displayed higher bias and wider limits of agreement for double support time compared to the GAITWell system. This observation indicates that measurement variability is a broader issue in gait analysis and is not confined to the GAITWell system alone. Nevertheless, enhancing the reliability of the GAITWell system remains a primary concern. Improving sensor resolution and addressing the system’s limitations are crucial for ensuring consistent and accurate measurements across all gait parameters. This will be essential for the system’s effectiveness in evaluating mobility and monitoring rehabilitation progress.
Our study aligns with prior research on mat-based gait analysis systems, including evaluations of the GAITRite system. For instance, Menz et al.14 reported high ICC values (0.83 to 0.94) for most gait parameters but identified challenges with base of support and toe-in/toe-out angles, which had higher 95% limits of agreement. The authors attributed this discrepancy to the GAITRite system’s spatial resolution (1.27 cm), which impacts the accuracy of calculating the toe-in/out angle due to its reliance on identifying three reference points from two different footprints. Cutlip et al.36 highlighted both strengths and limitations of the GAITRite system in comparison to a video-based motion analysis system. Temporal parameters such as stride time and stance duration showed excellent reliability across both systems (ICCs > 0.94). However, spatial parameters like step length and stride velocity exhibited discrepancies, with the GAITRite underestimating step length by 5.4 cm at higher gait speeds. These differences were attributed to the GAITRite system’s use of pressure transducers that detect initial contact, regardless of foot position, unlike the visual estimation method in the video-based system. Bilney et al.37 reported a low ICC (0.44) for double support time when comparing the GAITRite system with a foot insole, explaining this discrepancy as due to the insole’s correction factor, which adjusts contact times in the gait cycle. This may lengthen the double support percentage or reflect less sensitivity to toe-off compared to the GAITRite system. Vallabjajosula et al.34observed significantly greater stride width on the GAITRite compared to the Zeno Walkway. The ICC values for healthy older adults walking at a comfortable pace ranged from 0.449 to 0.918, with differences attributed to surface textures, footfall processing software, and walkway dimensions. These findings suggest moderate concurrent validity for most temporal parameters in healthy older adults walking at a comfortable pace. Together, these studies highlight the challenges in achieving reliable and accurate gait measurements across different systems and emphasize the need for rigorous testing and continual refinement during the early stages of system development.
The low correlation observed in stride length (r = 0.360, p < 0.05) between the GAITWell and Qualisys systems can be attributed to differences in their methodologies for detecting foot contact and toe-off events. The GAITWell system utilizes the DBSCAN clustering algorithm, which effectively extracts information and filters out noise, but it may be affected by sensor resolution issues, as observed in this study, potentially leading to inaccuracies in stride length calculation. In contrast, the Qualisys system captures ground reaction forces (GRF) from the force plates, resulting in more accurate measurements. Thus, discrepancies in stride length measurements may arise from differences in the identification and timing of heel contact and toe-off events. Despite these discrepancies, our study found strong correlations in step lengths: right step length (r = 0.672, p < 0.001) and left step length (r = 0.803, p < 0.001) were consistently measured by both systems. This indicates that while discrete-sensor-based systems like GAITWell offer a viable alternative, systems utilizing GRF generally provide more reliable measurements for spatial variables such as stride length and base of support.
Two limitations in our study merit discussion. Firstly, while we assessed the validity of the GAITWell system against the Qualisys Pro-Reflex, an established motion track system, it would have been ideal to also evaluate its validity against other widely recognized carpet-based systems such as GAITRite34or the Zeno Walkway33. Comparative assessments with these systems could provide a more comprehensive understanding of the GAITWell’s performance across different measurement systems. Secondly, our study focused exclusively on a cohort of healthy young adults. Therefore, generalizability to broader populations, including individuals with disabilities or different age groups, remains uncertain. Future research efforts should prioritize expanding the participant pool to encompass diverse demographic and clinical profiles, thus ensuring the applicability and relevance of the GAITWell system across a wider spectrum of users.
Given these limitations, it is crucial to contextualize the current development stage of the GAITWell system. The system is currently classified at Technology Readiness Level (TRL) 5, indicating that it has progressed beyond initial conceptualization and prototyping. At this stage, the system has undergone validation testing in controlled environments and has demonstrated functionality and reliability. However, further validation, particularly in clinical settings and with diverse populations, is necessary to advance the system toward higher TRL stages, such as clinical deployment or commercial application. This provides a clearer understanding of the GAITWell system’s potential, while also highlighting the work required to optimize its design for broader use.
In conclusion, while the GAITWell system shows considerable promise for advancing gait analysis in research and clinical practice by capturing a broad range of spatiotemporal gait variables, the system failed to demonstrate consistent reliability across key variables such as double support, cadence, and base of support. Preliminary findings suggest that enhancing sensor resolution could address these issues and improve measurement accuracy. Despite these shortcomings, one key advantage of the GAITWell system is its user-friendly design, which significantly reduces the time required for data collection and analysis. The modular structure and software interface, designed for ease of use, allow for quick setup and minimal user training, making it an accessible tool for healthcare professionals across various settings. The automated gait analysis process eliminates the need for complex data processing, providing immediate results that can support timely clinical decision-making.
Moreover, the system’s portable and modular design further underscores its potential as a valuable tool for gait analysis in low- and middle-income countries. It is particularly well-suited for use in rehabilitation clinics, senior care homes, and health institutions with limited space and resources. Future studies will focus on collecting specific data to further validate these time-saving and ease-of-use benefits. Additionally, ongoing work will concentrate on upgrading the sensors and refining the system to fully realize its potential in improving patient care and advancing research in gait analysis. We are committed to these enhancements to ensure the continued growth and effectiveness of the GAITWell system in the field.
Materials and methods
Study design
This methodological study evaluated the reliability and validity of the GAITWell system. Reliability refers to the consistency and accuracy of the data obtained and how effectively a measuring tool minimizes random error38,39. Test–retest reliability was assessed on two visits one week apart. Validity examines how accurately a measurement reflects the concept it is intended to measure. Concurrent validity assesses how well a system’s measurements compare to those of a gold standard system38,39. In this study, the spatiotemporal gait parameters measured with the GAITWell system were compared to those measured by the gold standard Qualisys Pro-Reflex MCU240 systems (QUALISYS MEDICAL AB, 411 12 Gothenburg, Sweden). This approach allowed us to examine the consistency and reproducibility of gait parameter measurements over time.
Participants
Healthy young adult participants, aged 18 and older, without any orthopedic or neurological problems, lower limb deformities, or heart disease that would prevent walking several times on the electronic walkway were invited to take part in the study. Participants were recruited from the university community through flyers, posters, and word of mouth. This study was approved by the Research Ethics Committee of the Federal University of Minas Gerais, Brazil (CAAE – 95186518.0.0000.5149). All experiments were performed in accordance with the relevant guidelines and regulations. Written informed consent was obtained from the individual(s) for participation.
Measurement instrument
GAITWell gait analysis system
The GAITWell system employs modular hardware and C# software, featuring a user-friendly interface designed for ease of use and adaptability to individual needs, while building on concepts from previous systems. Although we have not yet tested the interface with clients, we have adapted it based on existing systems. In the future, we plan to further customize the interface to better meet user needs. It employs discrete sensors that operate at a binary level (activated or deactivated) rather than relying on pressure sensors or retroreflective markers, offering a straightforward and precise method for gait pattern analysis.
The hardware consists of interconnected plates that form the electronic walkway, as depicted in Fig. 6a. The GAITWell system has a total length of 3.08 m, with a minimum of 1.76 m required to capture a complete gait cycle. It features a configuration of 7 × 2 plates along its length and 1 × 2 plates across its width, collectively covering the entire gait cycle. Each plate measures 44 cm × 37 cm and contains a set of discrete sensors arranged in an 11 × 7 grid, with a center-to-center spacing of 4 cm. The electronic structure of each plate consists of five layers and two enclosures, as illustrated in Fig. 6b. This structure features a rubber surface (1) in contact with the ground, a plate housing the electronic circuit (2), a perforated protection plate (3) to shield the sensors, and a transparent plate (4) to prevent particle or dust infiltration. Additionally, a carpet (5) and two enclosures (6) cover the electronic communication block and connectors. The electronic circuit layer (2) includes microcontrollers, the sensor array, connectors for external power supply and interconnection, as well as a module for communication and data transmission via Bluetooth and USB. The hardware’s durability was tested by transporting it in a 95 cm × 43 cm vehicle cargo compartment, housed in protective boxes to prevent damage. The modules withstood paved road and sidewalk transport in temperatures ranging from 27 °C to 34 °C without any functional or structural issues upon inspection. While not designed for prolonged exposure to extreme conditions, such as high humidity or very high temperatures, the system’s modular architecture and mechanical protections provide resistance to moderate environmental variations during transport and operation. Additionally, the GAITWell system is powered by a 5-V source compatible with standard chargers, ensuring stable operation in resource-constrained settings. Its low-current design optimizes energy efficiency and enhances reliability for field applications.

In (a), an image of the electronic device. In (b), the five layers forming the modular hardware structure are shown. The image was created by the author using SolidWorks software, version 2018 (Dassault Systèmes, Vélizy-Villacoublay – France).
In addition, the GAITWell system software is organized into three main modules: the user interface (GUI), the data acquisition module, and the processing module. The software starts with an authentication screen, which grants access to the GAITWell Graphical User Interface (GUI), allowing for data management, device connection setup, and result visualization.
The GUI is essential for configuring hardware interfaces, verifying the integrity of connected devices, and performing scans of the electronic walkway and integrated sensors. These scans collect data at a frequency of 1 kHz, with each cycle completing in 1 ms, ensuring high precision in monitoring. After connecting the hardware to the software via serial communication and confirming the system’s integrity, real-time gait data collection can be initiated. During the collection, data from individuals are recorded as vectors, including timestamps and corresponding states, which are then transmitted to the backend system. In the backend, the data are stored and prepared for subsequent processing.
Subsequently, this data proceeds to the next stage, referred to as ‘Processing’. In this step, the sensor triggers (events) are identified and transmitted to the computer through serial communication. They then undergo preprocessing and temporal analysis. During this process, the data is transformed into a list of instances of the ‘EventSensor’ class, each associated with a specific timestamp for subsequent analysis. Additionally, the processing involves the application of the Density-Based Spatial Clustering of Applications with Noise (DBSCAN) clustering algorithm to the Cartesian points derived from the sensor readings40,41. DBSCAN is crucial for identifying reference points such as foot contact and toe-off42. This method identifies clusters of arbitrary shapes and different sizes, separates noise from data, and detects ‘natural’ clusters and their arrangements within the data space, without any prior information about the groups43,44,45. DBSCAN was selected after testing K-means due to its popularity and simplicity. However, K-means had difficulty handling the variability and noise in gait data. While it performed reasonably well, it was not ideal for clusters with non-convex shapes, like human footprints, and was sensitive to noise, which affected the accuracy of gait measurements. Therefore, we opted to use DBSCAN instead.
For clustering purposes, DBSCAN distinguishes between three types of points: core points, border points, and noise points40,41. Core points are located within the densest area of a cluster and are characterized by having a minimum number of points within their Epsilon (Eps) neighborhood, equal to or greater than MinPts. MinPts represents the minimum quantity of points required within the Eps radius to establish a cluster40,41. Only core points form new clusters. Border points lie in the neighborhood of at least one core point41,45,46. Noise points are points that are neither core nor in the neighborhood of a core object. The DBSCAN estimates the density of points in a dataset by counting the number of points within a circle centered on the estimated points and with radius Epsilon (EPS)41. EPS is the maximum distance between two points for them to be considered neighbors in clustering algorithms41,45,46. A neighborhood is considered dense if the number of neighboring points is equal to or greater than the MinPts value41,46.
Thus, the method requires only one input parameter but supports determining an appropriate value for it42. For the initial choice of parameters Eps and MinPts, several gait readings were taken from volunteer participants who walked on the GAITWell electronic walkway. The effect of altering these parameters was observed to identify values that could correctly group the footprints41.
The number of footprints is equal to the number of clusters identified by the DBSCAN clustering algorithm. Furthermore, using the resulting vectors as a basis, the data from each cluster is separated into left and right footprints. This division considers account the direction of walking and the average position of two consecutive footprints in the perpendicular direction to the walking progression. Figure 7a and b illustrates this process, where the first identified footprint is classified as right if it is positioned further to the right when walking in the direction of increasing coordinates of the sensor line, or further to the left when walking in the opposite direction. Subsequent footprints alternate between right and left.

In (a) map of all footprints during the gait cycle test; (b) resulting clustering analysis after excluding the initial partial footprint; (c) schematic representation illustrating how GAITWell (3.08 m, 14 interconnected modules) determines step length relative to the (x, y) coordinate and the initial sensor activation on the device by heel strike, stride length and base of support.
Spatiotemporal variables are calculated from the clustered data (Fig. 7c). This includes parameters such as step length, stride length, gait speed, cadence, and gait cycle duration, providing a comprehensive understanding of the individual’s walking pattern. After processing, a detailed analysis of the spatiotemporal variables in the gait and visual representations of the cycle through images are displayed on the ‘Results Screen’ (Fig. 8). Additionally, the data, along with their respective date/time stamps, are stored in the database, serving as a customizable history of analyses, accessible through the ‘Management Screen’. Figure 5c illustrates the identification of heel contact and the calculation of step length, stride length, and base of support, while Fig. 6 shows the results on the GAITWell interface.

GAITWell interface shows the selected footprints and calculated spatiotemporal variables.
Simultaneous integration of GAITWell and Qualisys system for gait data collection
Spatial–temporal and kinematic gait parameters were simultaneously acquired using the GAITWell system and the Qualisys Pro-Reflex MCU240 (Qualisys MEDICAL AB, Gothenburg, Sweden). The Qualisys system, equipped with seven cameras and a 120 Hz sampling rate, was synchronized with two AMTI force plates embedded in a wooden platform. The force plates provide data for determining gait cycle events, such as foot contact on the first plate, toe-off, and subsequent contact on the second plate. Ground reaction force (GRF) data were recorded at 1 kHz and then resampled to 120 Hz. The Qualisys Track Manager 1.6.0.x-QTM software collected the data.
After calibrating the Qualisys system and the force plates, the GAITWell electronic walkway was placed on the wooden platform, as illustrated in Figs. 9a to 9d. To ensure participants stepped on both the force plates and the GAITWell plates simultaneously, the GAITWell walkway (1.76 m)—consisting of 4 rows and 2 columns of plates (each 44 cm × 37 cm)—was aligned directly over force plates 1 and 2 (each 51 cm × 51 cm), with an approximate 51 cm gap between them (Fig. 9b).

a to d. Panoramic view of the testing area, showing the camera setup and the GAITWell electronic walkway (1.76 m, 8 interconnected modules) positioned on a wooden platform with two embedded force plates. Figure 9d illustrates the capture of the gait cycle by the Qualisys cameras, with both feet in contact with the GAITWell hardware on the force plates. The 3D images were created by the author using SolidWorks software, version 2018 (Dassault Systèmes, Vélizy-Villacoublay – France).
The GAITWell system was then connected to a laptop via Bluetooth, and a pre-programmed calibration was conducted to ensure proper functionality. To prevent interference with the readings, the force plates were recalibrated (zeroed) after setting up the GAITWell system. The GAITWell system collected data at a frequency of 1 kHz, with a 1 ms interval between samples, providing high temporal resolution for gait analysis.
Only strides that included foot contact on the first force plate and subsequent contact on the second force plate were analyzed. These specific strides were visually inspected using the Qualisys system, which integrated camera footage and force plate signals. We specifically compared each individual stride containing force plate data with the corresponding stride data from the GAITWell system.
Experimental setup
Data was collected at the Laboratory of Movement Analysis of the School of Physical Education, Physical Therapy and Occupation Therapy at Federal University of Minas Gerais, Brazil. Participants were instructed to wear shorts and walk barefoot over the gait walkway. After the first visit, participants were invited to attend a second visit one week apart. This aspect of the experiment was designated for evaluating the test–retest reliability of the GAITWell.
For the kinematic data obtained from the Qualisys system, anatomical markers were used to determine the coordinates of leg and foot. The markers were placed at the lateral and medial condyles, lateral and medial malleoli, heads of the first, second, and fifth metatarsals, and the distal end of the calcaneus44,45. In addition, a cluster consisting of a rigid plate attached to a neoprene girdle with four tracking markers were positioned in the medial third of both shanks44,45. Clusters of tracking markers were used to capture the motion of the lower limb segments. These markers are essential for accurately developing the biomechanical model, which serves as the foundation for analyzing gait. After attaching the passive markers and cluster, participants were asked to stand still using a comfortable stance for 5 s to record the static trial. The static trial is important to define each segment and teach the software the particular dimensions of the participant’s body part.
Next, the participants were instructed to walk over the GAITWell, which was positioned on top of the force plates, at their comfortable self-selected gait speed. A specific command was issued as follows: “Upon my command ‘go’, walk at a speed as close as possible to your normal gait speed." Participants were given a practice period to familiarize themselves with the procedures. Participants performed 10 trials. Trials in which the foot correctly contacted the force plate, and all the dynamic markers were visible were used for analysis. On average 5 trials were used for analysis. After each collection, the data were checked for quality and stored for analysis. The average length of stay of each participant was approximately 90 min.
Data reduction
Kinematic and kinetic data from the Qualisys system were processed using Visual 3D (HAS-Motion, Kingston, ON, Canada). Initially, a biomechanical model was constructed using the passive markers placed on anatomical landmarks described previously. The model was then applied to the dynamic files obtained with the tracking markers to interpret the kinematic data47. Heel strike and toe-off events were automatically detected using the vertical ground reaction force from the force plates with a 20 N threshold. These data were integrated to accurately define the gait cycle and generate both spatial and temporal gait parameters. A fourth-order Butterworth low-pass filter was applied to the data, with cut-off frequencies set at 6 Hz for kinematic data and 18 Hz for kinetic data, to reduce noise. Finally, the gait cycle was normalized to 101 data points to facilitate consistent analysis and comparison.
In the GAITWell system, the kinematic data was processed using the software developed by our group, which fully automates the data collection, processing, and visualization of the gait cycle. Data reduction in the GAITWell involves a post-clustering process, as described previously, aimed at deriving meaningful spatiotemporal variables characterizing an individual’s gait. The spatiotemporal parameters were calculated as detailed in Box 2.
Statistical analysis
The sample size was determined considering an acceptable level of reliability of 0.5, with a significance level of 0.05 and a beta of 0.2, which indicated that a minimum of 22 participants would be required48. Sample characteristics and spatiotemporal gait parameters were described using measures of central tendency and dispersion. Data from visit 1 was used to determine the concurrent validity of the GAITWell with the Qualisys system. Pearson’s correlation was conducted, and the correlations coefficients were interpreted as follows: negligible (0.0 to 0.30), low (0.30 to 0.50), moderate (0.50 to 0.70), high (0.70 to 0.90), and very high (0.90 to 1.0)49. It is hypothesized that there will be moderate-to-high positive correlations between the spatiotemporal variables obtained from the GAITWell and the Qualisys system.
To assess the test–retest reliability of the GAITWell system across two visits, the Intraclass Correlation Coefficient (ICC)2,1was employed with a two-way random effects model50. Interpretation of the ICC was as follows: poor (< 0.50), moderate (0.50 to 0.75), good (0.76 to 0.90), and excellent (> 0.90)50. It is hypothesized that the spatiotemporal variables will show good to excellent reliability.
The standard error of the mean (SEM)51 provides information about the repeatability of the measurement and was calculated using the pooled standard deviation between both visits and the ICC2,1, Eq. (1):
We also applied the Bland–Altman plots to visualize the agreement between visits for the variables that did not reach reliability52. Bland–Altman plots can be used to evaluate the amount of measurement bias, thus more reliable results will show an average bias closer to zero and narrower 95% limits of agreement52. Thus, if the measurement falls inside the limits of agreement, then it would suggest no bias in the measurement. All analyses were conducted at a significance level of 0.05, using statistical software SPSS Statistics for Windows version 29.0 (IBM Corp, Armonk, NY, USA).
Patents
The GAITWell technology has been patented under the number BR 202017028502–8, filed on 12/28/2017, and granted on 12/26/2023. The patent covers a device for quantifying the spatiotemporal parameters of human gait, as well as the processes of operating this device and quantifying these parameters using the device.
Data availability
The data supporting the findings of this manuscript are available upon request from the first author via email: wellingtaniadias.ufmg@gmail.com.
References
Auvinet, B., Touzard, C., Montestruc, F., Delafond, A. & Goeb, V. Gait disorders in the elderly and dual task gait analysis: A new approach for identifying motor phenotypes. J. Neuroeng. Rehabil. 14, 1–14. https://doi.org/10.1186/s12984-017-0218-1 (2017).
Curuk, E., Goyal, N. & Aruin, A. S. The effect of motor and cognitive tasks on gait in people with stroke. J. Stroke Cerebrovasc. Dis. 28, 11. https://doi.org/10.1016/j.jstrokecerebrovasdis.2019.104330 (2019).
Boekesteijn, R. J., van Gerven, J., Geurts, A. C. H. & Smulders, K. Objective gait assessment in individuals with knee osteoarthritis using inertial sensors: A systematic review and meta-analysis. Gait Posture 98, 109–120. https://doi.org/10.1016/j.gaitpost.2022.09.002 (2022).
Kirkwood, R. N. et al. Frontal plane motion of the pelvis and hip during gait stance discriminates children with diplegia levels I and II of the GMFCS. ISRN pediatrics https://doi.org/10.5402/2012/163039 (2012).
Simon, S. R. Quantification of human motion: Gait analysis—benefits and limitations to its application to clinical problems. J. biomech. 37, 1869–1880. https://doi.org/10.1016/j.jbiomech.2004.02.047 (2004).
Stebbins, J., Harrington, M. & Stewart, C. Clinical gait analysis 1973–2023: Evaluating progress to guide the future. J. biomech. https://doi.org/10.1016/j.jbiomech.2023.111827 (2023).
Podsiadlo, D. & Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 39, 142–148. https://doi.org/10.1111/j.1532-5415.1991.tb01616.x (1991).
Peters, D. M., Fritz, S. L. & Krotish, D. E. Assessing the reliability and validity of a shorter walk test compared with the 10-meter walk test for measurements of gait speed in healthy. Older Adults. J. Geriatr. Phys. Ther. 36, 24–30. https://doi.org/10.1519/JPT.0b013e318248e20d (2013).
Middleton, A., Fritz, S. L. & Lusardi, M. Walking speed: The functional vital sign. J. Aging Phys. Act. 23, 314. https://doi.org/10.1123/japa.2013-0236 (2015).
Kirkwood, R. R. et al. The slowing down phenomenon: What is the age of major gait velocity decline?. Maturitas 115, 31–36. https://doi.org/10.1016/j.maturitas.2018.06.005 (2018).
McAndrew Young, P. M. & Dingwell, J. B. Voluntary changes in step width and step length during human walking affect dynamic margins of stability. Gait Posture https://doi.org/10.1016/j.gaitpost.2012.02.020 (2012).
Padmanabhan, P. et al. Persons post-stroke improve step length symmetry by walking asymmetrically. J. Neuroeng. Rehabil. https://doi.org/10.1186/S12984-020-00732-Z (2020).
Slaght, J.; Sénéchal, M.; Hrubeniuk, T. J.; Mayo, A.; Bouchard, D. R. Walking Cadence to Exercise at Moderate Intensity for Adults: A Systematic Review. https://doi.org/10.1155/2017/4641203 (2017).
Menz, H. B., Latt, M. D., Tiedemann, A., Kwan, M. M. S. & Lord, S. R. Reliability of the GAITRite walkway system for the quantification of temporo-spatial parameters of gait in young and older people. Gait & Posture 20, 20–25. https://doi.org/10.1016/S0966-6362(03)00068-7 (2004).
Muro-de-la-Herran, A., García-Zapirain, B. & Méndez-Zorrilla, A. Gait analysis methods: An overview of wearable and non-wearable systems, highlighting clinical applications. Sensors 14(2), 3362–3394. https://doi.org/10.3390/s140203362 (2014).
MejiaCruz, Y. et al. Walking speed measurement technology: A review. Curr. Geriatr. Rep. 10(1), 32–41. https://doi.org/10.1007/s13670-020-00349-z (2021).
Richards, J. G. The measurement of human motion: A comparison of commercially available systems. Hum. Mov. Sci. 18, 589–602. https://doi.org/10.1016/S0167-9457(99)00023-8 (1999).
Kanko, R. M., Laende, E., Selbie, W. S. & Deluzio, K. J. Inter-Session Repeatability of Markerless Motion Capture Gait Kinematics. J. Biomech. https://doi.org/10.1016/j.jbiomech.2021.110422 (2021).
Windolf, M., Götzen, N. & Morlock, M. Systematic Accuracy and precision analysis of video motion capturing systems—Exemplified on the vicon-460 system. J. Biomech. 41, 2776–2780. https://doi.org/10.1016/J.JBIOMECH.2008.06.024 (2008).
Magalhães, C. M. B., Resende, R. A. & Kirkwood, R. N. Increased hip internal abduction moment and reduced speed are the gait strategies used by women with knee osteoarthritis. J. Electromyogr. Kinesiol. 23, 1243–1249. https://doi.org/10.1016/j.jelekin.2013.05.013 (2013).
Resende, R. A., Deluzio, K. J., Kirkwood, R. N., Hassan, E. A. & Fonseca, S. T. Increased unilateral foot pronation affects lower limbs and pelvic biomechanics during walking. Gait Posture https://doi.org/10.1016/j.gaitpost.2014.10.025 (2015).
Caldas, R. et al. A systematic review of gait analysis methods based on inertial sensors and adaptive algorithms. Gait Posture 57, 204–210. https://doi.org/10.1016/j.gaitpost.2017.06.019 (2017).
Díaz, S., Stephenson, J. B. & Labrador, M. A. Use of wearable sensor technology in gait, balance, and range of motion analysis. Appl. Sci. 10, 234. https://doi.org/10.3390/app10010234 (2020).
Chen, S., Lach, J., Lo, B. & Yang, G. Z. Toward pervasive gait analysis with wearable sensors: A systematic review. IEEE J. Biomed. health inf. 20(6), 1521–1537. https://doi.org/10.1109/JBHI.2016.2608720 (2016).
Beauchamp, M. et al. Monitoring mobility in older adults using a global positioning system (GPS) smartwatch and accelerometer: A validation study. PLoS One https://doi.org/10.1371/journal.pone.0296159 (2023).
de Bruin, E. D., Hartmann, A., Uebelhart, D., Murer, K. & Zijlstra, W. Wearable systems for monitoring mobility-related activities in older people: A systematic review. Clin. Rehabil. 22, 878–895. https://doi.org/10.1177/0269215508090675 (2008).
Twardzik, E. et al. What features of the built environment matter most for mobility? using wearable sensors to capture real-time outdoor environment demand on gait performance. Gait Posture 68, 437–442. https://doi.org/10.1016/j.gaitpost.2018.12.028 (2019).
Beyer, K. B. et al. NiMBaLWear analytics pipeline for wearable sensors: A modular, open-source platform for evaluating multiple domains of health and behaviour. BMC Digit. Health https://doi.org/10.1186/s44247-024-00062-3 (2024).
Nascimento, D. H. A. et al. Development of a human motion analysis system based on sensorized insoles and machine learning algorithms for gait evaluation. Invetions 7, 98. https://doi.org/10.3390/inventions7040098 (2022).
Jacobs, D. et al. Evaluation of the Validity and reliability of connected insoles to measure gait parameters in healthy adults. Sensors (Basel) 21, 6543. https://doi.org/10.3390/s21196543 (2021).
Taborri, J., Palermo, E., Rossi, S. & Cappa, P. Gait partitioning methods: A systematic review. Sensors 16, 66. https://doi.org/10.3390/s16010066 (2016).
McDonough, A. L., Batavia, M., Chen, F. C., Kwon, S. & Ziai, J. The validity and reliability of the GAITRite system’s measurements: A preliminary evaluation. Arch. Phys. Med. Rehabil. 82, 419–425. https://doi.org/10.1053/apmr.2001.19778 (2001).
Sabo, A., Gorodetsky, C., Fasano, A., Iaboni, A. & Taati, B. Concurrent validity of zeno instrumented walkway and video-based gait features in adults with parkinson’s disease. IEEE J. Transl. Eng. Health. Med. https://doi.org/10.1109/JTEHM.2022.3180231 (2022).
Vallabhajosula, S., Humphrey, S. K., Cook, A. J. & Freund, J. E. Concurrent validity of the zeno walkway for measuring spatiotemporal gait parameters in older adults. J. Geriatr. Phys. Ther. 42, E42–E50. https://doi.org/10.1519/JPT.0000000000000168 (2019).
Kirkwood, R. N., Brandon, S. C. E., de Moreira, B. & S., Deluzio, K. J.,. Searching for stability as we age: The PCA-biplot approach. Int. J. Stat. Med. Res. 2(4), 255–262. https://doi.org/10.6000/1929-6029.2013.02.04.2 (2013).
Cutlip, R. G., Mancinelli, C., Huber, F. & DiPasquale, J. Evaluation of an instrumented walkway for measurement of the kinematic parameters of gait. Gait Posture 12, 134–138. https://doi.org/10.1016/s0966-6362(00)00062-x (2000).
Bilney, B., Morris, M. & Webster, K. Concurrent related validity of the GAITRite walkway system for quantification of the spatial and temporal parameters of gait. Gait Posture 17, 68–74. https://doi.org/10.1016/s0966-6362(02)00053-x (2003).
Mokkink, L. B. et al. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: An international delphi study. Qual. Life Res. 19, 539–549. https://doi.org/10.1007/s11136-010-9606-8 (2010).
Mokkink, L. B., Prinsen, C. A. C., Bouter, L. M., de Vet, H. C. W. & Terwee, C. B. The consensus-based standards for the selection of health measurement instruments (COSMIN) and how to select an outcome measurement instrument. Braz. J. Phys. Ther. 20, 105–113. https://doi.org/10.1590/bjpt-rbf.2014.0143 (2016).
Ester, M., Kriegel, H., Sander, J. & Xu, X. A. Density-based algorithm for discovering clusters in large spatial databases with noise. Knowl. Discov. & Data Min. https://doi.org/10.5555/3001460.3001507 (1996).
Starczewski, A., Goetzen, P. & Er, M. J. A new method for automatic determining of the DBSCAN parameters. J. Artif. Intell. Soft Comput. Res. 10, 209–221. https://doi.org/10.2478/jaiscr-2020-0014 (2020).
Schubert, E., Sander, J., Ester, M., Kriegel, H. P. & Xu, X. DBSCAN revisited, revisited: Why and how you should (still) use DBSCAN. ACM Trans. Database Syst. 42, 1–2. https://doi.org/10.1145/3068335 (2017).
Ansari, M. Y., Ahmad, A., Khan, S. S., Bhushan, G. & Mainuddin.,. Spatiotemporal clustering: A review. Artif. Intell. Rev. 53(4), 2381–2423. https://doi.org/10.1007/s10462-019-09736-1 (2020).
Wang, C. et al. An improved DBSCAN method for liDAR data segmentation with automatic eps estimation. Sensors 19, 172. https://doi.org/10.3390/s19010172 (2019).
Tran, T. N., Drab, K. & Daszykowski, M. Revised DBSCAN algorithm to cluster data with dense adjacent clusters. Chemom. Intell. Lab. Syst. 120, 92–96. https://doi.org/10.1016/j.chemolab.2012.11.006 (2013).
Mahesh Kumar, K., Reddy, R. M. & A.,. A fast DBSCAN clustering algorithm by accelerating neighbor searching using groups method. Pattern Recognit. 58, 39–48. https://doi.org/10.1016/j.patcog.2016.03.008 (2016).
Kadaba, M. P., Ramakrishnan, H. K. & Wootten, M. E. Measurement of lower extremity kinematics during level walking. J. Orthop. Res. 8, 383–392. https://doi.org/10.1002/jor.1100080310 (1990).
Walter, S. D., Eliasziw, M. & Donner, A. Sample size and optimal designs for reliability studies. Stat. Med. 17, 101–110. https://doi.org/10.1002/(SICI)1097-0258(19980115)17:1%3c101::AID-SIM727%3e3.0.CO;2-e (1998).
Akoglu, H. User’s guide to correlation coefficients. Turkish J. Emerg. Med. 18, 91–93. https://doi.org/10.1016/j.tjem.2018.08.001 (2018).
Koo, T. K. & Li, M. Y. A Guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 15, 155–163. https://doi.org/10.1016/j.jcm.2016.02.012 (2016).
Weir, J. P. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J. Strength Cond. Res. 19, 231–240. https://doi.org/10.1519/15184.1 (2005).
Giavarina, D. Understanding Bland Altman analysis. Biochem. Med. 25(2), 141–151. https://doi.org/10.11613/BM.2015.015 (2015).
Acknowledgements
The authors would like to thank the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq)—Process number 142163/2018-0, for their support in this project. This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 001. The authors also acknowledge the support of the Pró-Reitoria de Pesquisa (PRPq) and the Pró-Reitoria de Pós-Graduação (PRPG) of the Universidade Federal de Minas Gerais (UFMG).
Funding
W.D.D was funded by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPQ)—Process number 142163/2018–0. All other authors have no financial disclosures to declare.
Author information
Authors and Affiliations
Contributions
W.D.D., I.C.B., I.O.C, and M. S., conceptualization; W.D.D., R.K., I.C.B., and I.O.C, formal analysis; W.D.D., R.K., I.C.B., and I.O.C., investigation; W.D.D. and R.K., methodology; W.D.D. and R.H, project administration; R.H., resources; W.D.D., 3D Modeling and Design; I.C.B. and I.O.C., software; W.D.D., R.K., I.C.B., and I.O.C, validation; W.D.D. and R.K., writing – original draft; W.D.D., R.K., M.S., F.C., C.B.S.V., and R.H., writing – review and editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Institutional review board
The study was conducted in accordance with the Ethics Committee of Brazil (COEP) under the number CAAE: 95186518.0.0000.5149. Approval number: 2.836.553, with approval granted on August 22, 2018, for studies involving human participants. All experiments were performed in accordance with the relevant guidelines and regulations.
Informed consent
Informed consent was obtained from all subjects involved in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Dias, W.D., Kirkwood, R., Brito, I.C. et al. Validity and reliability of GAITWell portable modular system for gait analysis. Sci Rep 15, 36130 (2025). https://doi.org/10.1038/s41598-025-92123-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-92123-4
