
Abstract
Facial fractures significantly impair functions related to respiration, vision, and speech, while also posing long-term cosmetic and psychological challenges. Regional disparities in the burden of facial fractures reflect variations in risk factors, healthcare accessibility, and preventive measures. This study investigates recent causes, trends, and the burden of facial fractures in China and the United States. Utilizing the Global Burden of Disease 2021 dataset, the study analyzed epidemiological data on facial fractures in China and the United States, focusing on age-standardized incidence rates and years lived with disability from 2010 to 2021. Estimated annual percentage changes (EAPC) were calculated to assess trends, while age- and sex-specific analyses provided further insights into population-specific patterns. Additionally, the primary etiologies of facial fractures in both countries were examined. Between 2010 and 2021, the incidence of facial fractures increased in both China and the United States, with a more pronounced rise in China (EAPC: 1.56%) compared to the United States (EAPC: 0.38%). In 2021, the highest incidence in China was observed among males aged 30–34 years, while in the United States, it was among males aged 20–24 years. Males consistently exhibited higher rates than females in both countries. Falls and road injuries were the leading causes of facial fractures in China, whereas falls and mechanical forces were predominant in the United States. The rising incidence of facial fractures in China and the United States highlights the need for targeted preventive strategies tailored to each country’s specific risk factors and demographic patterns. These findings underscore the importance of addressing facial fractures as a global public health priority, with implications for policy-making and resource allocation to reduce the burden of these injuries worldwide.
Similar content being viewed by others

Introduction
Facial fractures, including fractures of the craniofacial bones, jaws, and associated structures, account for nearly one-seventh of all fractures globally, impacting approximately 1.5 million individuals in 20191. According to the International Classification of Diseases, Tenth Revision (ICD-10), facial fractures are categorized under specific codes: S02.2 (nasal bone fracture), S02.3 (orbital floor fracture), S02.4 (mandibular fracture), S02.5 (maxillary fracture), and S02.6–S02.7 (other facial bone fractures, including zygomatic and complex fractures)1. Representing a substantial global public health concern, facial fractures can lead to vision and hearing impairments, airway obstruction, significant hemorrhage, and, in severe cases, pose life-threatening risks2. These injuries also profoundly impact facial aesthetics, resulting in asymmetry, deformities, and psychosocial challenges3. Prompt diagnosis and effective treatment are therefore critical to restoring both function and appearance.
The etiology of facial fractures is multifactorial, with causes ranging from traffic accidents and falls to sports injuries and violent incidents4. Studies indicate that traffic accidents are a predominant cause, accounting for approximately 40–50% of facial fractures, particularly among young men5. Fall is a significant cause of facial fractures, particularly among the elderly and children, due to factors such as osteoporosis, balance issues, and high-energy injuries during outdoor activities. In elderly populations, falls account for approximately 20–30% of facial fractures, predominantly involving the nasal and zygomatic bones, while in children, they contribute to 15–20% of cases, often occurring in home or school environments6,7. In China, the incidence of facial fractures has increased in parallel with socioeconomic development and population mobility, factors closely linked to traffic regulation enforcement and growing public safety awareness5,8. These data underscore the need for prevention and treatment strategies tailored to different socioeconomic contexts to mitigate the impact of facial fractures on patients’ quality of life.
Despite extensive research on the epidemiology of facial fractures, there remains a significant gap in comparative studies between countries with differing Social Demographic Index (SDI) classifications, particularly in terms of etiology, trends, and disease burden9. China and the United States, representing medium and high SDI categories respectively, are the world’s most populous nations10. In China, the total hospitalization cost for traumatic fractures in tertiary public hospitals surpassed $5.5 billion in 202011, while in the United States, annual emergency room visits for facial fractures exceed 400,000 cases, with costs surpassing $1 million12. In China, traffic accidents are identified as the primary cause of maxillofacial fractures, comprising 56.3% of cases, predominantly affecting young and middle-aged males13. In contrast, the proportion of elderly patients with maxillofacial fractures is higher in the United States, and with the growing elderly population, fall-related facial fractures among older adults are increasingly common14. Additionally, studies show that female patients with maxillofacial fractures in the U.S. have a lower economic burden compared to males, but it remains significant15. By comparing the etiology and burden of facial fractures in these two nations, this study aims to inform tailored prevention and treatment strategies for countries at different stages of economic development.
To our knowledge, no prior comparative analysis has been conducted between China and the United States on this subject. The Global Burden of Disease Study (GBD) provides the most extensive measure of injury and disease burden trends globally, offering valuable insights for public health policy formulation16,17. Notably, the GBD 2021 update incorporates a more comprehensive dataset and improved estimation methodology compared to GBD 2019, enhancing its utility for such comparative analyses by incorporating expanded data sources and refined modeling techniques. These advancements enable more accurate estimations of disease burden and injury trends, offering critical insights for health systems planning and evaluation.
This study aims to analyze and compare the epidemiology of facial fractures in China and the United States using GBD 2021 data, focusing on trends in incidence rates and years lived with disability (YLDs). Understanding the burden of facial fractures in these two nations will ultimately support the development of targeted prevention and treatment strategies.
Materials and methods
Data source
Data on the disease burden of facial fractures were sourced from the Global Burden of Disease (GBD 2021) database, under the auspices of the World Health Organization (WHO) and coordinated by the Institute for Health Metrics and Evaluation, with generous support from the Bill and Melinda Gates Foundation18. The GBD database integrates data from national health surveys, hospital records, and administrative datasets to estimate disease burden19. Its reliability has been widely recognized due to robust modeling techniques. These comprehensive data sources make GBD a valuable tool for comparative health analyses.
GBD defines fractures as a type of injury rather than a disease cause. Facial fractures in GBD are classified based on the International Classification of Diseases (ICD). Specifically, they align with ICD-9 code 802 and ICD-10 codes S02.2, S02.3, S02.4, S02.5, S02.6, and S02.7, encompassing nasal, orbital, mandibular, maxillary, and other facial bone fractures1. This study extracted data specific to China and the United States, focusing on causes such as “Animal contact”, “Conflict and terrorism”, “Drowning”, “Environmental heat and cold exposure”, “Exposure to forces of nature”, “Exposure to mechanical forces”, “Falls”, “Fire, heat, and hot substances”, “Foreign body”, “Interpersonal violence”, “Other transport injuries”, “Poisonings”, “Police conflict and executions”, “Road injuries”, “Self-harm”, and “All causes”. The detailed ICD codes used to identify causes of injury are described in the supplementary table S1. The primary metrics were “incidence” and “YLDs,” each reported with a 95% uncertainty interval (95% UI). Age-related patterns in incidence and YLDs were examined across 20 distinct age groups: < 5, 5–9, 10–14, 15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59, 60–64, 65–69, 70–74, 75–79, 80–84, 85–89, 90–94, and 95 + years. Comprehensive descriptions of the general methodologies employed in GBD 2021 are accessible on the official research site (https://ghdx.healthdata.org/gbd-2021).
Statistical analysis
Annual incidence and years lived with disability (YLDs) rates for facial fractures were obtained from the GBD 2021 dataset, disaggregated by sex, age, and country for the period from 2010 to 2021. To evaluate the burden of facial fractures, the age-standardized rate (ASR) was calculated using the WHO standard population, and the estimated average percentage change (EAPC) was also calculated.
In this formula, \({a}_{i}\) represents the age-specific rate for the \(i\) th age group, \(w\) denotes the population or weight of the \(i\) th age group based on the reference standard population, and \(A\) indicates the total number of age groups. The EAPC was calculated using the approach described by Liu et al., applying the equation y = a + bx + e, where y is the natural logarithm of the age-standardized rate ln (ASR), and x represents the calendar year. EAPC was then calculated as 100 × (exp(b) −1), with a 95% confidence interval (CI) derived from the linear regression model. An EAPC greater than zero indicates an increasing trend in the age-standardized rate, while an EAPC less than zero signifies a decreasing trend; an EAPC of zero reflects stability in the indicator. Data analyses were conducted using Excel 2019, R software (version 4.2.0, Free Software Foundation), and Prism (Version 10.1.1 (270), November 21, 2023).
Results
Changes in the worldwide ranking of ASIR and ASYR in China and the United States from 2010 to 2021
The age-standardized incidence rate (ASIR) trends from 2010 to 2021 across 204 countries and regions reveal a gradual rise in the ASIR ranking of facial fractures for both China and the United States. From 2010 to 2021, China’s ranking improved, rising from being ahead of over 14.22% of countries and regions in 2010 to being ahead of over 28.92% in 2021 (a 14.7% increase). During the same period, the United States also increased in its ranking, going from being ahead of over 54.41% of countries and regions in 2010 to being ahead of over 60.78% in 2021 (a 6.37% increase) (Fig. 1A).

Global ranking of ASIR and ASYR for facial fractures in China and the United States, 2010–2021. (A) ASIR in China and the United States. (B) ASYR in China and the United States. Abbreviations: ASIR, age-standardized incidence rate; ASYR, age-standardized years lived with disability rate. The x-axis represents 204 countries and regions worldwide for each year. This percentage represents country’s position in the ASIR ranking of all countries in the world out of 204 countries and regions. Abbreviations: ASIR, age-standardized incidence rates; ASYR, age-standardized years lived with disability rates.
For the age-standardized years lived with disability rate (ASYR), global rankings indicate that China and the United States exceeded 28.43% and 61.27% of countries worldwide in 2021, with increases of 11.27% and 6.86%, respectively (Fig. 1B). Notably, the United States consistently showed higher ASIR and ASYR values than China throughout the study period.
Burden and trends of facial fractures from 2010 to 2021
In China, approximately 1,194,145 (95% UI: 909,426–1,571,247) new facial fracture cases were reported in 2021, with an ASIR of 90.501 (95% UI: 69.814–118.789) per 100,000. Of these, about 372,161 (95% UI: 265,162–503,880) cases involved females (31.17%), with an ASIR of 57.864 (95% UI: 42.306–78.637) per 100,000, while males (68.83%) accounted for 821,984 (95% UI: 639,705–1,059,019) cases and an ASIR of 120.363 (95% UI: 94.501–153.172) per 100,000. Between 2010 and 2021, the total number of new cases increased by 16.93%, and the ASIR rose by 17.74%, with an EAPC of 1.564 (95% CI: 1.294–1.835) (Table 1). Over the same period, YLDs rose by 29.04%, and ASYR increased by 15.62%, with an EAPC of 1.367 (95% CI: 1.138–1.598) (Table 2).
In the United States, the total number of new facial fracture cases reached 492,670 (95% UI: 378,858–640,022) in 2021, with an ASIR of 151.122 (95% UI: 116.607–195.929) per 100,000. From 2010 to 2021, new cases rose by 8.85%, while the ASIR showed a modest increase of 1.35%, with an EAPC of 0.382 (95% CI: 0.074–0.690) (Table 1). Between 2010 and 2021, YLDs increased by 15.73%, while ASYR rose by 1.63%, with an EAPC of 0.351 (95% CI: 0.108–0.595) (Table 2).
Changes in the burden and trends of facial fractures by age and sex in 2021
In 2021, the age-specific incidence of facial fractures was analyzed (Fig. 2), showing that new cases in China consistently outnumbered those in the United States across all age groups. Peak incidence was observed among individuals aged 30–34 (10.7% in total population) in China and 20–24 (10.5% in total population) in the United States (Fig. 2A). Among females, peak incidences occurred in the 30–34 age group in China and 55–59 age group in the U.S. (Fig. 2B), while for males, peak incidences aligned with the overall trends (Fig. 2C).

New cases of facial fractures by age group in China and the United States, 2021. (A) New cases in females and males. (B) New cases in females. (C) New cases in males.
The incidence rates by age subgroup were further examined (Fig. 3). Except for those aged over 90, the United States showed higher incidence rates than China across all age groups. The highest incidence rates for both countries were recorded in the 20–24 age range (Fig. 3A). Notably, female incidence rates began rising significantly from age 70 in China, with a peak in the 50–64 age group in the United States (Fig. 3B). For males, peak rates occurred in the 15–34 age range in both countries (Fig. 3C).

Incidence of facial fractures by age group in China and the United States, 2021. (A) Incidence in females and males. (B) Incidence in females. (C) Incidence in males.
The distribution of YLDs by age subgroup in 2021 was also analyzed (Figure S1), revealing consistently higher YLDs in China compared to the United States across all age groups. The peak number of YLDs for China was found in the 50–54 (9.0% in total population) and U.S. in the 60–64 age groups (8.5% in total population) (Figure S1A), with females peaking at 55–59 and 65–69 (Figure S1B), and males peaking at 50–54 and 55–69 (Figure S1C). YLD rates by age subgroup (Figure S2) showed a progressive increase with age in both countries. The YLD rate in the United States remained higher than in China for all groups below age 90 (Figure S2A).
The ASIR ranks of causes for facial fractures ASIR in China and the United States from 2010 to 2021
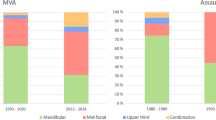
In China, falls were identified as the top cause of facial fractures, followed by road injuries, interpersonal violence, and exposure to mechanical forces (Fig. 4). Falls also showed the highest increase in ASIR, with an EAPC of 5.043, while foreign bodies demonstrated an upward trend (EAPC of 4.492). In contrast, road injuries exhibited a decline, with an EAPC of -1.62 (Table 3).

Annual ranking of causes for facial fractureASIR in China and the United States, 2010–2021. (A) Annual ranking of causes in China. (B) Annual ranking of causes in the United States. Abbreviations: ASIR, age-standardized incidence rates.
Similarly, in the United States, falls were the leading cause, followed by exposure to mechanical forces, road injuries, and interpersonal violence (Fig. 4). The ASIR for falls and mechanical forces increased, with EAPCs of 0.643 and 1.159, respectively, whereas conflict and terrorism showed the most pronounced decline (EAPC of -22.570).
Among both female (Figure S3) and male (Figure S4) populations in China and the United States, falls consistently ranked as the primary cause, with moderate variations in secondary causes between sexes.
Discussion
This study, spanning 2010 to 2021, revealed notable epidemiologic trends in facial fractures across China and the United States. Findings indicate that, while both ASIR and ASYR are lower in China than in the United States, each country has experienced a gradual rise in global rankings. This underscores the need to address disparities in facial fracture incidence between China and the United States, deepening insights into the underlying causes and informing targeted policy revisions in both nations. The observed trends align with the broader GBD goals of reducing health disparities by providing data-driven evidence to inform health policy.
Although the ASIR is higher in the United States, China records nearly double the new and YLD cases due to its larger population base—approximately 1.41 billion in China compared to 331 million in the United States as of 202120. Over the past decade, facial fracture rates and YLDs have trended upward in both countries. This may be attributed to economic and social development, as well as increased exposure to risk factors for facial fractures, such as traffic incidents, sports injuries, and evolving social lifestyles21. Furthermore, advancements in diagnostic techniques, including computed tomography (CT) and three-dimensional (3D) reconstruction, have enabled more precise and convenient detection of facial fractures, surpassing conventional X-ray capabilities22. Interestingly, only U.S. males showed a decrease in facial fracture rates from 2010 to 2021, potentially reflecting the impact of targeted injury prevention programs, heightened public awareness, and enhanced workplace safety standards.
Our findings indicate that the incidence of facial fractures is highest among young to middle-aged adults in both China and the United States, aligning with previous research1. Notable age-related differences were observed: in China, the highest incidence was among those aged 30–34, while in the United States, it was among individuals aged 20–24. In China, individuals aged 30–34 are often employed in high-risk sectors, such as manufacturing, construction, and driving, where facial injuries are more common2. Conversely, in the United States, peak incidences among 20–24-year-olds may be linked to higher participation in contact sports, risky driving behaviors under the influence, and other risk-taking activities among this demographic23,24. Furthermore, young adults in the U.S. may experience elevated rates of injuries associated with interpersonal violence25. The incidence rates decrease with age, likely due to reduced risk-exposure activities in older populations. However, facial fracture incidence in women increases after age 70, particularly in China, potentially due to postmenopausal osteoporosis, which predisposes older women to fractures26. Studies indicate that older women have lower bone density and a higher risk of osteoporosis and osteoarthritis compared to men of the same age, contributing to increased vulnerability27. YLDs, however, continue to rise progressively with age, potentially because declining bone density and muscle mass increase susceptibility to severe injuries and complications. Additionally, common comorbidities among older adults, such as osteoporosis and diabetes, may slow the healing process and prolong recovery.
In both countries, falls are the primary cause of facial fractures across age groups. Among young adults, falls frequently occur during recreational activities, sports, and accidental slips—often during bicycling, skateboarding, or contact sports—that result in facial trauma28. In older adults, physiological changes, including reduced muscle strength, bone density, balance, and reflexes, heighten fall risk and injury severity. Chronic conditions such as osteoporosis and arthritis further compromise bone integrity, increasing fracture risk29. Differences between the two countries show an EAPC in China eight times higher than that in the United States, potentially due to rapid urbanization and population aging30. Since 1999, China’s elderly population has steadily increased, reaching 158.31 million (11.4% of the total population) by 201731. In comparison, the aging population in the United States was 47 million as of 2015, according to the U.S. Census Bureau32.
Road injuries rank as the second leading cause of facial fractures in China and third in the United States. As the two largest global economies, economic expansion in both nations has led to increased motor vehicle ownership and traffic volume, thereby raising the incidence of road-related accidents and associated facial fractures33. Driving under the influence also contributes to road accidents34. However, the United States has implemented more advanced traffic management and road safety systems, with stringent legislation and enforcement of safety measures, such as mandatory seatbelt use and the promotion of child safety seats35. These regulations have effectively reduced facial injuries among vehicle occupants in traffic accidents. Nevertheless, the high vehicle usage rate and common practice of long-distance driving in the United States maintain traffic accidents as a significant source of facial fractures.
Among the top causes of facial fractures, interpersonal violence and mechanical force exposure also stand out. Interpersonal violence ranks high in China, possibly linked to social pressures, conflict resolution practices, and alcohol consumption habits36. Conversely, mechanical factors are more prominent in the United States, largely due to a greater prevalence of workers in high-risk industries and widespread mechanical automation.
To reduce the burden of facial fractures, countries should strengthen preventive measures such as traffic safety regulations, occupational safety standards, and sports injury prevention programs. Optimizing healthcare resources, particularly through improving primary care capabilities and promoting advanced diagnostic technologies, is essential for effective treatment. Public health education campaigns should focus on raising awareness of risk factors and promoting healthy lifestyles. Additionally, establishing national injury monitoring systems and supporting epidemiological research will provide valuable data to inform policy decisions and improve interventions.
Despite comprehensively analyzing the etiology, trends, and burden of facial fractures in China and the United States, several limitations exist in our study. First, the analysis relies on GBD 2021 data, which, although robust, may have inherent limitations related to data collection and reporting consistency across countries. Second, this study specifically addresses facial fractures without accounting for other concurrent injuries, potentially underestimating the overall trauma burden in these populations. Third, evolving factors such as traffic regulations, healthcare access, and social behaviors that may influence future trends were not within this analysis’s scope. Fourth, although this study provides valuable insights into the epidemiological characteristics of facial fractures, it is limited by the lack of data on mortality and survival rates. These indicators are crucial for understanding the full clinical impact and prognosis of facial fractures. Future research should prioritize incorporating these factors to offer a more comprehensive epidemiological assessment. Finally, while the findings reveal differences in facial fracture rates and burdens between China and the United States, the specific underlying causes and contributing factors are complex. Further research is essential to delve into these factors, including the role of socioeconomic status, healthcare infrastructure, and cultural factors in facial fracture prevention. Such research can contribute to more equitable health outcomes, aligning with the GBD’s mission to address health disparities through comprehensive epidemiological insights.
Conclusion
In summary, although China has lower ASIR and ASYR rates for facial fractures compared to the United States, the absolute number of cases is higher in China, with an upward trend observed in both countries. The age group most affected in China is 30–34 years, while in the United States, it is 20–24 years, with a notably higher incidence in males than females. In China, the leading causes of facial fractures are falls and road injuries, whereas in the United States, falls and exposure to mechanical forces predominate. These findings highlight the importance of establishing prevention and treatment strategies tailored to each country’s specific needs to improve the quality of life for those affected by facial fractures. Recommendations include strengthening road safety regulations and promoting fall-prevention initiatives, particularly for the elderly population in both countries. By offering evidence-based insights, this research underscores the value of injury prevention strategies in achieving better health outcomes and reducing the global burden of injuries.
Data availability
The datasets generated during this study are available from the corresponding author upon reasonable request.
Abbreviations
- GBD:
-
Global burden of disease
- EAPC:
-
Estimated average percentage change
- YLDs:
-
Years lived with disability
- ASIR:
-
Age-standardized incidence rate
- ASYR:
-
Age-standardized years lived with disability rate
References
Zhang, Z. X., Xie, L. & Li, Z. Global, regional, and national burdens of facial fractures: A systematic analysis of the global burden of Disease 2019. BMC Oral Health 24(1), 282 (2024).
Chen, Y., Weber, A. & Chen, C. Evidence-based medicine for midface/orbit/upper facial fracture repair. Facial Plast Surg 39(3), 253–265 (2023).
Lozada, K., Kadakia, S., Abraham, M. T. & Ducic, Y. Complications of midface fractures. Facial Plast Surg 33(6), 557–561 (2017).
de Lucena, A. L., da Silva Filho, G. F., de Almeida Pinto Sarmento, T. C., de Carvalho, S. H., Fonseca, F. R., de Santana Sarmento, D. J.: Epidemiological profile of facial fractures and their relationship with clinical-epidemiological variables. J. Craniofac. Surg. 2016; 27(2):345-349.
Zhou, H. H., Ongodia, D., Liu, Q., Yang, R. T. & Li, Z. B. Changing pattern in the characteristics of maxillofacial fractures. J Craniofac Surg 24(3), 929–933 (2013).
Diab, J., Flapper, W. J., Grave, B., Anderson, P. J. & Moore, M. H. Pediatric facial fractures in South Australia: Epidemiology, clinical characteristics, and outcomes. J Craniofac Surg 32(7), 2317–2321 (2021).
Hwang, K. & You, S. H. Analysis of facial bone fractures: An 11-year study of 2094 patients. Indian J Plast Surg 43(1), 42–48 (2010).
Chen, W. et al. National incidence of traumatic fractures in China: A retrospective survey of 512,187 individuals. Lancet Glob Health 5(8), e807–e817 (2017).
Yi, Y., He, X., Wu, Y. & Wang, D. Global, regional, and national burden of incidence, prevalence, and years lived with disability for facial fractures from 1990 to 2019: A systematic analysis for the Global Burden of Disease study 2019. BMC Oral Health 24(1), 435 (2024).
The global, regional, and national burden of benign prostatic hyperplasia in 204 countries and territories from 2000 to 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Healthy Longev. 2022, 3(11):e754–e776.
Huang, B. X. et al. Epidemiology and the economic burden of traumatic fractures in China: A population-based study. Front Endocrinol (Lausanne) 14, 1104202 (2023).
Allareddy, V., Allareddy, V. & Nalliah, R. P. Epidemiology of facial fracture injuries. J Oral Maxillofac Surg 69(10), 2613–2618 (2011).
Mao, J. et al. Epidemiology of maxillofacial fractures in northwest China: an 11-year retrospective study of 2240 patients. BMC Oral Health 23(1), 313 (2023).
Irgebay, Z., Kahan, E. H., Park, K. E., Choi, J. & Zellner, E. G. Characteristics and patterns of facial fractures in the elderly population in the United States based on trauma quality improvement project data. J Craniofac Surg 33(5), 1294–1298 (2022).
Peluso, H., Talemal, L., Moss, C., Araya, S., Kozorosky, E., Patel, S. A., Walchak, A.: Epidemiology and characteristics of women with facial fractures seeking emergency care in the United States: A retrospective cohort study. Craniomaxillofac. Trauma Reconstr. 2024:19433875241252194.
Global, regional, and national age-sex-specific mortality and life expectancy, 1950–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392(10159):1684–1735.
Liu, H., Yin, P., Qi, J. & Zhou, M. Burden of non-communicable diseases in China and its provinces, 1990–2021: Results from the Global Burden of Disease Study 2021. Chin Med J (Engl) 137(19), 2325–2333 (2024).
Murray, C. J. L. Findings from the global burden of disease study 2021. Lancet 403(10440), 2259–2262 (2024).
Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 2022, 9(2):137–150.
Scully, C. Drug effects on salivary glands: dry mouth. Oral Dis 9(4), 165–176 (2003).
Qi, M., Hu, X., Li, X., Wang, X. & Shi, X. Analysis of road traffic injuries and casualties in China: A ten-year nationwide longitudinal study. PeerJ 10, e14046 (2022).
Fox, L. A. et al. Diagnostic performance of CT, MPR and 3DCT imaging in maxillofacial trauma. Comput Med Imaging Graph 19(5), 385–395 (1995).
Ruslin, M., Boffano, P., ten Brincke, Y. J., Forouzanfar, T. & Brand, H. S. Sport-related maxillo-facial fractures. J Craniofac Surg 27(1), e91-94 (2016).
Greene, K. M., Murphy, S. T. & Rossheim, M. E. Context and culture: Reasons young adults drink and drive in rural America. Accid Anal Prev 121, 194–201 (2018).
Ganson, K. T., O’Connor, J., Benabou, S. E. & Nagata, J. M. Associations between interpersonal violence victimisation and concussions among US college students. Health Soc Care Community 30(1), 175–183 (2022).
Brown, J. P. Long-term treatment of postmenopausal osteoporosis. Endocrinol Metab (Seoul) 36(3), 544–552 (2021).
Hannan, M. T. et al. Risk factors for longitudinal bone loss in elderly men and women: The Framingham Osteoporosis Study. J Bone Miner Res 15(4), 710–720 (2000).
Viozzi, C. F. Maxillofacial and mandibular fractures in sports. Clin Sports Med 36(2), 355–368 (2017).
Chen, Y. S., Lian, W. S., Kuo, C. W., Ke, H. J., Wang, S. Y., Kuo, P. C., Jahr, H., Wang, F. S.: Epigenetic regulation of skeletal tissue integrity and osteoporosis development. Int. J. Mol. Sci. 2020, 21(14).
Beard, J. R. et al. The World report on ageing and health: A policy framework for healthy ageing. Lancet 387(10033), 2145–2154 (2016).
Wu, L., Huang, Z. & Pan, Z. The spatiality and driving forces of population ageing in China. PLoS One 16(1), e0243559 (2021).
Chiu, B. L. & Pinto, J. M. Aging in the United States: Opportunities and challenges for otolaryngology-head and neck surgery. Otolaryngol Clin North Am 51(4), 697–704 (2018).
Hyman, D. A. et al. Patterns of facial fractures and protective device use in motor vehicle collisions from 2007 to 2012. JAMA Facial Plast Surg 18(6), 455–461 (2016).
Jie-Ling, J. & Yuan-Chang, D. Analysis of drink-driving behavior: Considering the subjective and objective factors of drivers. Traffic Inj Prev 22(3), 183–188 (2021).
Zaloshnja, E., Miller, T. R. & Hendrie, D. Effectiveness of child safety seats vs safety belts for children aged 2 to 3 years. Arch Pediatr Adolesc Med 161(1), 65–68 (2007).
Zhou, X. et al. Global burden of self-harm and interpersonal violence and influencing factors study 1990–2019: Analysis of the global burden of disease study. BMC Public Health 24(1), 1035 (2024).
Acknowledgements
We acknowledge Bullet Edits Limited for its assistance with the linguistic editing and proofreading of this manuscript.
Funding
This study received no funding, and the authors declare no financial conflicts of interest.
Author information
Authors and Affiliations
Contributions
Hao Chen conducted the data analysis and study design. Zhi Jia, Xin He, and Xingyu Feng contributed to the review and editing of the study. Meng Wu prepared the initial draft of the manuscript, and Shuangyue Zhang participated in the design, review, and editing process. All authors have reviewed and approved the final manuscript for publication.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This article does not include any studies involving human participants or animals conducted by the authors.
Consent to publication
All authors have read and approved the content of this manuscript and take responsibility for its accuracy and integrity, in accordance with the criteria set by the International Committee of Medical Journal Editors (ICMJE).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Chen, H., Jia, Z., He, X. et al. Burden and trends of facial fractures in China and the United States based on GBD 2021 analysis. Sci Rep 15, 8328 (2025). https://doi.org/10.1038/s41598-025-92980-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-92980-z
Keywords
This article is cited by
-
Functional mechanism and clinical implications of lncRNA NEAT1 in traumatic fractures and their correlation with delayed healing
Journal of Orthopaedic Surgery and Research (2025)
