
Abstract
Significant sex disparities exist in the burden of atrial fibrillation and flutter. However, comprehensive and systematic analysis of its global trend by sex is scarce. The Global Burden of Disease Study 2021 was used as data source for analysis. Sex-specific prevalence, incidence, disability-adjusted life years (DALY), and mortality rates per 100,000 population from atrial fibrillation and flutter were estimated using the Bayesian meta-regression method. Temporal trends of average annual percent change (AAPC) of age-standardized and age-specific burdens across age bands were evaluated using the joinpoint model stratified by socio-demographic index (SDI). Sex differences in trends were tested using pairwise comparison. From 1990 to 2021, the global age-standardized DALY rate [from 109.93 (95% uncertainty interval, 88.5 to 134.72) to 112.05 (93.3 to 135.28), P < 0.001], age-standardized mortality rate [from 4.20 (3.65 to 4.59) to 4.44 (3.94 to 4.81), P < 0.001] for atrial fibrillation and flutter significantly increased in males, while the age-standardized incidence rate decreased from 58.0 (44.98 to 75.8) to 57.11 (46.19 to 72.14) in males (P < 0.001). Countries with low and low-middle SDI exhibited significant increases in age-standardized prevalence and incidence rates in both females and males (all P < 0.001), with a faster increase in females. Across all age bands, a faster increase in mortality was observed among males, while females under age bands of 50 years showed a higher increase in prevalence and incidence on a global scale compared to males. High systolic blood pressure was the predominant risk factor contributing to atrial fibrillation and flutter-related DALY. Notably, the impact of high body-mass index on DALY of atrial fibrillation and flutter was increasing fast over last three decades, especially in males. Although the global burden of atrial fibrillation and flutter has substantially increased, disparities exist across different sexes, age bands, and countries with different socio-demographic status.
Similar content being viewed by others


Introduction
Atrial fibrillation is a major global health concern with well-documented sex disparities in its epidemiology1. The Framingham Heart Study reported an age-adjusted prevalence of atrial fibrillation nearly twice as high in men (96.2 per 1,000 person-years) compared to women (49.4 per 1,000 person-years) over a 50-year observation period2. Similar disparities have been observed in European and Asian populations3,4. While men generally show a higher incidence of atrial fibrillation, women with the condition often face higher rates of complications, such as stroke, heart failure, and mortality5,6.
The mechanisms underlying these sex disparities are complex, involving a web of risk factors at individual, familial, community, and societal levels. Behavioral and metabolic risk factors play crucial roles7,8, alongside differences in healthcare access and quality9,10. Despite the critical importance of understanding sex disparities in atrial fibrillation epidemiology and associated risk factors, there is a notable lack of studies offering a global perspective on this issue, with most published studies conducted in specific countries or regions2,3,4. While the Global Burden of Disease Study 2021 provides an updated and comprehensive dataset on AF11, existing analyses have primarily focused on overall trends without exploring sex-specific differences in detail.
Our research aims to fill this gap by leveraging the Global Burden of Disease Study 2021 database, which provides standardized methods for quantifying the burden of diseases and risk factors across populations. By evaluating the global burden and attributable risk factors for atrial fibrillation and flutter with a focus on sex differences, we aim to provide comprehensive insights that can inform public health policies and clinical practices worldwide.
Methods
Data source
The Global Burden of Disease Study 2021 project produced estimates of prevalence, incidence, mortality, years of life lost (YLL), years lived with disability (YLD) and disability-adjusted life years (DALY) for 371 diseases and injuries across 204 countries and territories from 1990 to 202112,13. Additionally, 88 risk factors and their risk-outcome pairs were included to estimate the risk attributable burdens14. This project adheres to the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER) recommendations, and its analytic procedures have been detailed in previous reports12,13,14. Briefly, Global Burden of Disease Study 2021 gathered extensive data from various sources, including surveys, censuses, vital statistics, and other health-related data, which were standardized for disease burden estimation.
Estimation of global burden of atrial fibrillation and flutter
The data were processed under the Bayesian meta-regression model framework, using DisMod-MR 2.1 modelling tool, to estimate the non-fatal burden of atrial fibrillation and flutter. A detailed description of the Bayesian meta-regression model and its prior assumptions can be found in the supplementary materials. Hospital and outpatient administrative data from certain geographies were excluded if they were implausibly low.
-
YLD estimation: The unadjusted YLD were equal to the prevalence estimated from the DisMod-MR model multiplied by the disability weights for each atrial fibrillation and flutter-related sequela. Additionally, a micro-simulation adjusting for comorbidities was performed to generate the final estimate of comorbidity-adjusted YLD.
-
Mortality estimation: Vital registration data were analyzed using the Cause of Death Ensemble modelling (CODEm) model to estimate the atrial fibrillation and flutter-related mortality identified by the corresponding International Classification of Disease codes (details in supplementary materials). An estimation model that integrated longitudinal prevalence and excess mortality data, combining DisMod-MR model and CODEm, was employed to mitigate the impact of changing death certification patterns13. This approach aimed to produce more accurate mortality estimates by adjusting for covariates (details in supplementary materials).
-
YLL calculation: Calculated by multiplying the number of estimated atrial fibrillation and flutter-related deaths by the predicted life expectancy by age, sex, location and year.
-
DALY estimation: Computed by adding YLL and YLD for each age, sex and location.
Estimation of risk factor attributable DALY rate of atrial fibrillation and flutter
A causal web of hierarchically organized risk factors based comparative risk assessment framework was reported in a previous study14, and the definitions of risk exposures are listed in supplementary materials. Six risk factors from three categories of risk exposures, as discussed and determined by the Global Burden of Disease Study Scientific Council, were analyzed for their attributable DALY rate on atrial fibrillation and flutter:14.
-
Environmental/occupational risks: Lead exposure.
-
Behavioral risks: Smoking, high alcohol use and diet high in sodium.
-
Metabolic risks: High systolic blood pressure and high body-mass index.
The attributable DALY rate of a given risk factor refers to the potential reduction in outcome-related DALY if past population exposure had shifted to an ideal level of that risk factor. The estimation of risk attributable DALY—for risk-outcome pairs was calculated by multiplying the total DALY by the population attributable fraction. Population attributable fraction represents the proportion of risk that would be reduced in a given year if past exposure to a certain risk factor was reduced to the theoretical minimum risk exposure level.
Statistical analysis
Given that the data sources are derived from scientific studies reported with uncertainty, all estimates were generated by predicting 1,000 draws based on the variance-covariance matrix13. Results were presented as the mean of these draws, with 95% uncertainty intervals (UI, the 2.5th and 97.5th percentiles).
-
Age-standardization: Prevalence, incidence, DALY, and mortality rates were calculated using the Global Burden of Disease Study reference population13. All rates were reported per 100,000 population.
-
The sex-specific burden analysis: Evaluated by analyzing the male to female ratio of age standardized rates in terms of prevalence, incidence, DALY and mortality associated with atrial fibrillation and flutter.
The temporal trend in age-standardized burdens for atrial fibrillation and flutter and its attributable risk factors were analyzed using the Joinpoint regression models. The Joinpoint Regression Program software (version 4.9.1.0, National Cancer Institute, USA) was employed for this purpose, evaluating time trends by assessing the average annual percent change (AAPC) of the age-standardized rates. Initially, the joinpoint model established the minimum number of joinpoints, typically at zero, representing a straight line. The model then tests whether additional joinpoints should be added, up to a predetermined maximum, based on statistical significance. The 95% confidence intervals (CI) of AAPC were estimated using the Parametric method. This helped ascertain if perceived shifts in trends were statistically meaningful. Each trend between joinpoints was tested using Monte Carlo methods, with the significance level adjusted through a Bonferroni correction15. Trends were classified as increasing or decreasing based on whether the AAPC was positive or negative. The sex differences in the trends of disease burdens were compared by analyzing the differences in the AAPC between females and males using pairwise comparison16.
The comparison of atrial fibrillation and flutter burden and its risk factors attributable burden between females and males was conducted across:
-
Various age bands (in five-year intervals).
-
Five socio-demographic index (SDI) regions.
-
Seven world regions, and at the global level.
Additionally, Spearman’s rank correlation (Spearman’s ρ) was performed to evaluate the association of SDI with age-standardized burdens of atrial fibrillation and flutter, as well as the risk factors attributable DALY rates. The introduction and methods for calculating SDI are detailed in supplementary materials. The proportional burden of each risk factor was calculated by dividing the attributable burden of that factor by the total burden for atrial fibrillation and flutter.
R software (version 4.3.2) was used for the statistical analyses. A two-sided P value of less than 0.05 was considered statistically significant.
Results
In 2021, the age-standardized prevalence rate, age-standardized incidence rate, age-standardized DALY rate, and age-standardized mortality rate per 100,000 population of atrial fibrillation and flutter in females were 529.12 (95% UI, 430.79 to 663.14), 47.26 (95% UI, 37.38 to 60.87), 92.24 (95% UI, 76.84 to 111.24), and 4.29 (95% UI, 3.53 to 4.80), respectively. For males, these rates were 728.88 (95% UI, 601.91 to 895.81), 57.11 (95% UI, 46.19 to 72.14), 112.05 (95% UI, 93.30 to 135.28), and 4.44 (95% UI, 3.94 to 4.81), respectively (supplementary Table 1).
Sex disparities in the burden of atrial fibrillation and flutter across regions in 2021
There is a regional disparity in the sex distribution of the atrial fibrillation and flutter burden. The largest difference between two sexes in age-standardized DALY rate for atrial fibrillation and flutter was in the United States, where the male-to-female ratio was 4.65. Conversely, the smallest ratio of 0.41 was observed in South Africa (Fig. 1). Male-to-female ratios across 204 countries and territories in age-standardized prevalence rate (supplementary Fig. 1), age-standardized incidence rate (supplementary Fig. 2), and age-standardized mortality rate (supplementary Fig. 3) are provided in the supplementary materials.

Age-standardized disability adjusted life years (DALY) rate and male-to-female ratio for DALY rate of atrial fibrillation and flutter in 204 countries and territories in 2021.
Sex disparities in the burden of atrial fibrillation and flutter across socio-demographic index in 2021
The age-standardized prevalence rate and DALY rate of atrial fibrillation and flutter varied across areas with different SDI. The highest prevalence and DALY rates were observed in countries with a high SDI for both females and males (supplementary Table 1). For instance, at the country level, the highest prevalence rates were found in Sweden, with 1211.57 (95% UI, 898.26 to 1562.27) in females and 1852 (95% UI, 1421.38 to 2340.23) in males (supplementary Fig. 5).
A significant positive correlation was observed between the SDI and the male-to-female ratio of age-standardized prevalence rate (Spearman’s ρ = 0.513, P < 0.001), age-standardized incidence rate (Spearman’s ρ = 0.373, P < 0.001), and age-standardized DALY rate (Spearman’s ρ = 0.273, P < 0.001), but not for age-standardized mortality rate (supplementary Fig. 6). Furthermore, the prevalence rate and DALY rate of atrial fibrillation and flutter were higher in older age bands for both females and males (supplementary Table 2).
Sex disparities in temporal trend of atrial fibrillation and flutter burdens by regions and socio-demographic index (1990–2021)
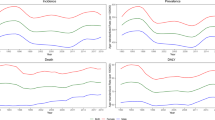
The global age-standardized prevalence rate of atrial fibrillation and flutter did not show an increasing trend. However, there were regional disparities. In countries with low and middle SDI, the age-standardized prevalence rate of atrial fibrillation and flutter increased significantly from 1990 to 2021. In contrast, countries with high and high-middle SDI presented a change in the age-standardized prevalence rate that aligned with the global trend (supplementary Table 1). Notably, despite both females and males experiencing a significant increase in the age-standardized incidence rate in low and low-middle SDI countries, the increment was larger in females compared to males (Fig. 2), with AAPC difference between females and males of 0.09 (95% CI, 0.06 to 0.12, P < 0.001) in low SDI countries and 0.05 (95% CI, 0.04 to 0.06, P < 0.001) in low-middle SDI countries.

Gender-specific average annual percent change (AAPC) in incidence rate of atrial fibrillation and flutter by age and socio-demographic index (SDI), from 1990 to 2021.
At the super-region level, an increasing trend in the age-standardized prevalence rate was observed in both females and males in Central Europe, Eastern Europe, and Central Asia, South Asia, Southeast Asia, East Asia, Oceania, and Sub-Saharan Africa. The increasing speed seemed faster in female population in South Asia and Sub-Saharan Africa, and in male population in the other super-regions (supplementary Table 1).
The global trend in the age-standardized DALY rate increased more significant in males rather than females (Fig. 3). However, similar increasing trends were observed in countries with low and low-middle SDI for both population (supplementary Table 1). At the super-regions level, both females and males in North Africa and the Middle East experienced an increasing trend in the age-standardized DALY rate of atrial fibrillation and flutter, with a higher rate observed in females (AAPC difference between females and males, 0.20; 95% CI, 0.03 to 0.37, P = 0.022). A similar trend was observed in age-standardized mortality rates in countries with low and low-middle SDI (supplementary Fig. 4).

Gender-specific average annual percent change (AAPC) in disability adjusted life years (DALY) rate of atrial fibrillation and flutter by age and socio-demographic index (SDI), from 1990 to 2021.
Sex disparities in age-specific trends of atrial fibrillation and flutter burden (1990–2021)
Regarding the age specific epidemic trend of prevalence and incidence rate of atrial fibrillation and flutter globally, higher increasing trend was observed in female population among age intervals under 50 years (supplementary Table 2). Conversely, a consistent decreasing trend of prevalence rate was found in both females and males among age bands over 75 years. Meanwhile, a faster increase in mortality was observed among male population across all age bands.
Sex disparities in attributable risk factors for atrial fibrillation and flutter in 2021
Globally, metabolic risk factors contributed most to the DALY rate of atrial fibrillation and flutter, followed by behavioral risk factors (Fig. 4). High systolic blood pressure consistently ranked as the top risk factor for the DALY of atrial fibrillation and flutter, accounting for 29.1% (95% UI, 10.3 to 46.5) and 30.9% (95% UI, 11.1 to 48.6) of total atrial fibrillation and flutter DALYs in 2021 for all-age males and females, respectively.

Gender-specific proportion of all-age disability adjusted life years (DALY) rate of atrial fibrillation and flutter attributable to risk factors globally, from 1990 to 2021.
The second and third ranking risk factors are also observed globally by sex. In females, high body-mass index and high-sodium diet were the second and third ranking risks, whereas in males, smoking and high body-mass index occupied these positions. The influence of these risk factors on age-standardized DALY varies across countries with different SDI (supplementary Table 3). In high SDI countries, the top three risk factors in 2021 for both females and males were high systolic blood pressure, high body-mass index, and high alcohol use. Conversely, in low SDI countries, high systolic blood pressure remained the top risk factor for both females and males, followed by lead exposure, with the third risk factor changing into smoking in males and high body-mass index in females (supplementary Table 3).
Sex disparities in regional variations of risk factors for atrial fibrillation and flutter in 2021
Correlations between SDI and risk attributable age-standardized DALY rates of atrial fibrillation and flutter were moderate to strong with respect to smoking (Spearman’s ρ = 0.428, P < 0.001), high alcohol use (Spearman’s ρ = 0.619, P < 0.001), lead exposure (Spearman’s ρ=-0.531, P < 0.001), high systolic blood pressure (Spearman’s ρ = 0.500, P < 0.001), and high body-mass index (Spearman’s ρ = 0.647, P < 0.001) in males, while only a weak correlation between SDI and lead exposure (Spearman’s ρ = 0.143, P < 0.001) was found in females (supplementary Fig. 7).
Sex disparities in temporal trends of risk factors for atrial fibrillation and flutter (1990–2021)
From 1990 to 2021, the global age-standardized DALY rates of atrial fibrillation and flutter attributable to high systolic blood pressure and smoking decreased in both females and males. However, there were rising trends of high body-mass index and lead exposure attributable DALY rates in both females and males, and rising trends of high alcohol use and a high-sodium diet attributable DALY rates in males (Fig. 4 and supplementary Table 3).
Over the past three decades, temporal trends for risk factor attributable DALY rates varied between females and males across different SDI status and age groups. In countries with low and low-middle SDI, the age-standardized DALY rates of atrial fibrillation and flutter attributable to high systolic blood pressure, high body-mass index, and high alcohol use have significantly increased, especially in males (Fig. 5 and supplementary Table 3). For young females in the age intervals of 35 to 44 years, high systolic blood pressure and high body-mass index attributable DALY rate rose much faster compared to males (Fig. 6 and supplementary Table 4).

Gender-specific average annual percent change (AAPC) in proportion of age-standardized disability adjusted life years (DALY) rate of atrial fibrillation and flutter attributable to risk factors by socio-demographic index (SDI), from 1990 to 2021.

Gender-specific average annual percent change (AAPC) in proportion of age-standardized disability adjusted life years (DALY) rate of atrial fibrillation and flutter attributable to risk factors by age, from 1990 to 2021.
Discussion
Based on data from the Global Burden of Disease Study 2021, several key findings were identified (Table 1). The global burden of atrial fibrillation and flutter significantly increased from 1990 to 2021, particularly in countries with low and low-middle SDI. Over 30-year period, prevalence and incidence of atrial fibrillation and flutter decreased in older age intervals but increased in younger intervals, particularly females below 50 years old. The rising trends were faster among females in terms of prevalence and incidence rates, whereas males experienced higher increase in DALY and mortality rates. Among risk factors, metabolic risks contributed mostly to DALY rates for both sexes. The impact of metabolic and behavioral risks was notably correlated with socio-demographic status in males but not females. While burdens attributable to environmental and behavioral risks decreased, DALY rates attributed to metabolic risks increased. These findings highlight the growing burden of atrial fibrillation and flutter and underscore sex-specific disparities.
Increasing burdens of atrial fibrillation and flutter
Regional disparities in the age-standardized prevalence and incidence rates of atrial fibrillation and flutter from 1990 to 2021 were evident. Low-SDI countries experienced notable increases, consistent with previous findings that poor financial resources, such as unemployment17 and low household income18, are associated with higher incidence of atrial fibrillation. Conversely, high-SDI countries exhibited stable trends, exemplified by data from the US Centers for Medicare & Medicaid Services, which reported a consistent 9% prevalence among the US American Indian and Alaska Native population from 2015 to 201919.
Compared to previous studies, our analysis found that females in low to low-middle SDI regions experienced a higher increase in prevalence and incidence than males. The results from Atherosclerosis Risk in Communities study identified an education-sex interaction, where females with the lower education level had a higher risk of atrial fibrillation, an association not seen in males18. Similarly, females in higher-deprivation areas had a higher risk of atrial fibrillation hospitalization, a trend not observed in males20. These disparities warrant more active interventions. Improving socio-economic status, such as through education, may be effective in reducing atrial fibrillation risk among females21.
Atrial fibrillation, an age related disease, imposes a growing burden with population aging22. The Framingham Heart Study reported an almost three-fold increase in the prevalence of atrial fibrillation over the past five decades2. In Denmark, the lifetime risk of atrial fibrillation increased by 6.7% from 2000-2010 to 2011-202223. Our analysis revealed that while prevalence and incidence decreased among older-age population, it increased among younger-age population. Similar trends were observed in Norway, where cases rose significantly among those under 45 but remained stable in older adults24. These findings suggest a shift in atrial fibrillation onset towards younger individuals, with a notably higher growth rate in young females.
Atrial fibrillation is closely associated with stroke and heart failure, increasing severe disability risk25 and healthcare burden26. Our results showed an increasing DALY and mortality rate of atrial fibrillation and flutter in low and low-middle SDI countries, particularly among males. The discrepancy in prevalence and DALY rates between sexes highlight healthcare imbalance in developing countries. In these regions, females with established cardiovascular diseases may have better control over risk factors10, including high systolic blood pressure and smoking, which are important promotors of the progression of atrial fibrillation27. This shift also reflects changes in the disease spectrum with regional development28 and underscores the need for greater efforts to raise awareness of atrial fibrillation and implement effective interventions.
Metabolic risk factors contributed most to the disability adjusted life years (DALY) of atrial fibrillation and flutter
The attributable risk factors for atrial fibrillation and flutter have significantly changed over the past 30 years, with metabolic risks becoming dominant. High systolic blood pressure remains the top risk factor, while the DALY attributable to high body-mass index has increased globally. The Rotterdam Study found that cardiometabolic risks are strongly associated with the lifetime risk of atrial fibrillation, particularly in females and younger individuals29. Our analysis shows that, although behavioral and environmental risks attributable DALY have decreased in age bands under 60 years, the DALY attributable to metabolic risks has significantly increased. There is a notable sex difference in the 35 to 45 age band, where females have a higher rate of increase. This rise in metabolic risks among younger population partly explains the shift in atrial fibrillation onset from older to younger individuals, especially in females.
Metabolic risk factors are prevalent worldwide and exhibit sex-specific patterns. The global trend of obesity continues to rise, with projections indicating almost 18% of males and over 21% of females will be obese by 202530. According to data from the US National Health and Nutrition Examination Survey, the body-mass index increased more in females than males from 2001 to 201631. Notably, females experience a more rapid increase in blood pressure in their early life, despite a higher overall prevalence in males32, likely influenced by sex hormones33. In younger population, the association between hypertension and atrial fibrillation was stronger in females34. These sex differences in the prevalence of metabolic risk factors provide perspective on understanding sex-specific trends in the global burden of atrial fibrillation.
Regional differences are another important issue concerning the metabolic risks epidemic. Our analysis found that atrial fibrillation burden attributable to high systolic blood pressure decreased in high and high-middle SDI regions, but increased in low to middle SDI regions, particularly in males. On the other hand, although globally females had higher DALY rates attributable to high body-mass index in 2021, the increase was faster in males over the past 30 years, especially in those over 60 years old. Male population in high-SDI regions had greater high body-mass index attributable DALY rates, in line with previous study, which reported that the association between body-mass index and atrial fibrillation was more significant in males than in females7. This sex-specific trend aligns with findings from a global epidemiological survey on central obesity, which revealed a more rapid increase in males35. These findings underscore the need for region- and sex-specific public health strategies to address metabolic risks.
Effective strategies are essential to addressing the rising global burden of atrial fibrillation and its sex-specific disparities. Hypertension management remains a key priority, as elevated systolic blood pressure is the leading risk factor for atrial fibrillation and its associated DALYs. Individualized antihypertensive therapy and lifestyle modifications can improve blood pressure control, but sex-specific considerations are crucial. Males with high cardiovascular risk are less likely to receive or adhere to treatment, highlighting the need for targeted efforts to improve prescription and compliance10. In contrast, young females face a growing atrial fibrillation burden due to high body-mass index and lower rates of weight control, underscoring the importance of structured weight loss programs and lifestyle interventions36.
Early detection through opportunistic screening in high-risk populations can enable timely intervention. Early rhythm control could reduce cardiovascular death and heart failure hospitalization37, while anticoagulation lowers stroke risk38. Notably, the widespread use of wearable electrocardiogram monitoring significantly increase atrial fibrillation detection, but it also raises challenges in determining who requires intervention39. Current evidence suggests that treatment decisions should be based on atrial fibrillation burden, symptoms, and stroke risk40,41. Integrating these strategies into public health policies is especially critical in low-SDI regions, where the atrial fibrillation burden is rapidly increasing.
Limitations
Several limitations of this study should be noted. Firstly, the estimation of atrial fibrillation burdens was constrained by the exclusion of non-literature-based data, apart from hospital and claims data. Additionally, reliance on modelling where data were unavailable and variations in measurement methods across data sources, and inherent biases could not be completely eradicated despite mitigation efforts. Secondly, the exclusion of hospital data in certain regions where data were implausibly low and outpatient administrative data with consistently zero prevalence may have restricted the accuracy of the estimations due to data adjustment constraints. Thirdly, the need for ECG confirmation of atrial fibrillation also required adjustments for alternative data sources, potentially introducing inaccuracies. Fourthly, differences in healthcare access and screening quality across countries may have led to underestimations in low-SDI regions, highlighting the importance of considering socioeconomic factors in the analysis. Moreover, the sensitivity of the trend changes assessed by AAPC may be limited by the study period length. Although we analyzed the sex differences in the trends of atrial fibrillation and flutter burdens over 1990–2021 to mitigate misinterpretations, subtle fluctuations may not achieve statistical significance and could be disregarded. Therefore, these findings should therefore be interpreted with caution.
Conclusion
The increasing burden of atrial fibrillation and flutter warrants urgent action, including improved healthcare access and quality in countries with low and low-middle SDI, with a specific emphasis on mitigating the impact of metabolic risks. Sex-specific tailored public health interventions, alongside efforts to curb the growing prevalence and incidence among young population, are crucial measures in alleviating the global burden of atrial fibrillation and flutter.
Data availability
The results from Global Burden of Disease Study 2021 are publicly available through the interactive platform of the Institute for Health Metrics and Evaluation (IHME). Global Burden of Disease Results. Seattle, WA: IHME, University of Washington, 2024. Available from https://vizhub.healthdata.org/gbd-results/ (Accessed May 17, 2024).
Change history
23 May 2025
A Correction to this paper has been published: https://doi.org/10.1038/s41598-025-01836-z
Abbreviations
- AAPC:
-
Average annual percent change
- DALY:
-
Disability-adjusted life years
- SDI:
-
Socio-demographic index
- YLD:
-
Years lived with disability
- YLL:
-
Years of life lost
References
Volgman, A. S. et al. Sex and race/ethnicity differences in atrial fibrillation. J. Am. Coll. Cardiol. 74, 2812–2815. https://doi.org/10.1016/j.jacc.2019.09.045 (2019).
Schnabel, R. B. et al. 50 Year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham heart study: A cohort study. Lancet 386, 154–162. https://doi.org/10.1016/s0140-6736(14)61774-8 (2015).
Wu, J. et al. Temporal trends and patterns in atrial fibrillation incidence: A population-based study of 3·4 million individuals. Lancet Reg. Health Eur. 17, 100386. https://doi.org/10.1016/j.lanepe.2022.100386 (2022).
Du, X. et al. Atrial fibrillation prevalence, awareness and management in a nationwide survey of adults in China. Heart 107, 535–541. https://doi.org/10.1136/heartjnl-2020-317915 (2021).
Emdin, C. A. et al. Atrial fibrillation as risk factor for cardiovascular disease and death in women compared with men: Systematic review and meta-analysis of cohort studies. Bmj 532, h7013. https://doi.org/10.1136/bmj.h7013 (2016).
Lip, G. Y. H. et al. Atrial fibrillation and stroke prevention: 25 years of research at EP Europace journal. Europace 25. https://doi.org/10.1093/europace/euad226 (2023).
Magnussen, C. et al. Sex differences and similarities in atrial fibrillation epidemiology, risk factors, and mortality in community cohorts: Results from the biomarcare consortium (Biomarker for cardiovascular risk assessment in Europe). Circulation 136, 1588–1597. https://doi.org/10.1161/circulationaha.117.028981 (2017).
Kloosterman, M. et al. Sex-related differences in risk factors, outcome, and quality of life in patients with permanent atrial fibrillation: Results from the RACE II study. Europace 22, 1619–1627. https://doi.org/10.1093/europace/euz300 (2020).
Bhave, P. D., Lu, X., Girotra, S., Kamel, H. & Vaughan Sarrazin, M. S. Race- and sex-related differences in care for patients newly diagnosed with atrial fibrillation. Heart Rhythm. 12, 1406–1412. https://doi.org/10.1016/j.hrthm.2015.03.031 (2015).
Xia, S. et al. Sex differences in primary and secondary prevention of cardiovascular disease in China. Circulation 141, 530–539. https://doi.org/10.1161/circulationaha.119.043731 (2020).
Cheng, S. et al. Global burden of atrial fibrillation/atrial flutter and its attributable risk factors from 1990 to 2021. Europace 26. https://doi.org/10.1093/europace/euae195 (2024).
Ferrari, A. J. et al. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet (2024).
Naghavi, M. et al. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: A systematic analysis for the Global Burden of Disease Study 2021. Lancet (2024).
Brauer, M. et al. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990–2021: A systematic analysis for the global burden of disease study 2021. Lancet 403, 2162–2203. https://doi.org/10.1016/S0140-6736(24)00933-4 (2024).
Kim, H. J., Fay, M. P., Feuer, E. J. & Midthune, D. N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 19, 335–351 (2000).
Clegg, L. X., Hankey, B. F., Tiwari, R., Feuer, E. J. & Edwards, B. K. Estimating average annual per cent change in trend analysis. Stat. Med. 28, 3670–3682 (2009).
Soliman, E. Z., Zhang, Z. M., Judd, S., Howard, V. J. & Howard, G. Comparison of risk of atrial fibrillation among employed versus unemployed (from the reasons for geographic and Racial differences in stroke Study). Am. J. Cardiol. 120, 1298–1301. https://doi.org/10.1016/j.amjcard.2017.07.001 (2017).
Misialek, J. R. et al. Socioeconomic status and the incidence of atrial fibrillation in Whites and Blacks: The atherosclerosis risk in communities (ARIC) study. J. Am. Heart Assoc. 3. https://doi.org/10.1161/jaha.114.001159 (2014).
Eberly, L. A. et al. Cardiovascular disease burden and outcomes among American Indian and Alaska native medicare beneficiaries. JAMA Netw. Open 6, e2334923. https://doi.org/10.1001/jamanetworkopen.2023.34923 (2023).
Zöller, B., Li, X., Sundquist, J. & Sundquist, K. Neighbourhood deprivation and hospitalization for atrial fibrillation in Sweden. Europace 15, 1119–1127. https://doi.org/10.1093/europace/eut019 (2013).
Lunde, E. D. et al. Socioeconomic position and risk of atrial fibrillation: A nationwide Danish cohort study. J. Epidemiol. Community Health 74, 7–13. https://doi.org/10.1136/jech-2019-212720 (2020).
Vollset, S. E. et al. Fertility, mortality, migration, and population scenarios for 195 countries and territories from 2017 to 2100: A forecasting analysis for the global burden of disease study. Lancet 396, 1285–1306. https://doi.org/10.1016/s0140-6736(20)30677-2 (2020).
Vinter, N. et al. Temporal trends in lifetime risks of atrial fibrillation and its complications between 2000 and 2022: Danish, nationwide, population based cohort study. Bmj 385, e077209. https://doi.org/10.1136/bmj-2023-077209 (2024).
Kjerpeseth, L. J. et al. Prevalence and incidence rates of atrial fibrillation in Norway 2004–2014. Heart 107, 201–207. https://doi.org/10.1136/heartjnl-2020-316624 (2021).
McGrath, E. R. et al. Association of atrial fibrillation with mortality and disability after ischemic stroke. Neurology 81, 825–832. https://doi.org/10.1212/WNL.0b013e3182a2cc15 (2013).
Khazanie, P. et al. Outcomes of medicare beneficiaries with heart failure and atrial fibrillation. JACC Heart Fail. 2, 41–48 (2014).
Elliott, A. D., Middeldorp, M. E., Van Gelder, I. C., Albert, C. M. & Sanders, P. Epidemiology and modifiable risk factors for atrial fibrillation. Nat. Rev. Cardiol. 20, 404–417. https://doi.org/10.1038/s41569-022-00820-8 (2023).
NCD Countdown. Countdown 2030: Worldwide trends in non-communicable disease mortality and progress towards Sustainable Development Goal target 3.4. Lancet 392, 1072–1088 (2018).
Lu, Z. et al. Burden of cardiometabolic disorders and lifetime risk of new-onset atrial fibrillation among men and women: The Rotterdam study. Eur. J. Prev. Cardiol. https://doi.org/10.1093/eurjpc/zwae045 (2024).
Collaboration, N. R. F. Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet 387, 1377 (2016).
Peters, S. A. E., Muntner, P. & Woodward, M. Sex differences in the prevalence of, and trends in, cardiovascular risk factors, treatment, and control in the united States, 2001 to 2016. Circulation 139, 1025–1035. https://doi.org/10.1161/circulationaha.118.035550 (2019).
Ji, H. et al. Sex differences in blood pressure trajectories over the life course. JAMA Cardiol. 5, 19–26. https://doi.org/10.1001/jamacardio.2019.5306 (2020).
Drury, E. R., Wu, J., Gigliotti, J. C. & Le, T. H. Sex differences in blood pressure regulation and hypertension: Renal, hemodynamic, and hormonal mechanisms. Physiol. Rev. 104, 199–251. https://doi.org/10.1152/physrev.00041.2022 (2024).
Kanazawa, S. et al. Sex differences in the association between hypertension and incident atrial fibrillation. J. Am. Heart Assoc. 12, e026240. https://doi.org/10.1161/jaha.122.026240 (2023).
Wong, M. C. S. et al. Global, regional and time-trend prevalence of central obesity: A systematic review and meta-analysis of 13.2 million subjects. Eur. J. Epidemiol. 35, 673–683. https://doi.org/10.1007/s10654-020-00650-3 (2020).
Cooper, A. J., Gupta, S. R., Moustafa, A. F. & Chao, A. M. Sex/gender differences in obesity prevalence, comorbidities, and treatment. Curr. Obes. Rep. 10, 458–466. https://doi.org/10.1007/s13679-021-00453-x (2021).
Kirchhof, P. et al. Early rhythm-control therapy in patients with atrial fibrillation. N. Engl. J. Med. 383, 1305–1316. https://doi.org/10.1056/NEJMoa2019422 (2020).
Svennberg, E. et al. Clinical outcomes in systematic screening for atrial fibrillation (STROKESTOP): A multicentre, parallel group, unmasked, randomised controlled trial. Lancet 398, 1498–1506. https://doi.org/10.1016/s0140-6736(21)01637-8 (2021).
Sanders, P. et al. Great debate: Device-detected subclinical atrial fibrillation should be treated like clinical atrial fibrillation. Eur. Heart J. 45, 2594–2603. https://doi.org/10.1093/eurheartj/ehae365 (2024).
Bucci, T. et al. Sex-related differences in presentation, treatment, and outcomes of Asian patients with atrial fibrillation: A report from the prospective APHRS-AF registry. Sci. Rep. 13, 18375. https://doi.org/10.1038/s41598-023-45345-3 (2023).
Yoshimura, H., Providencia, R., Finan, C., Schmidt, A. F. & Lip, G. Y. H. Refining the CHA2DS2VASc risk stratification scheme: Shall we drop the sex category criterion? Europace 26. https://doi.org/10.1093/europace/euae280 (2024).
Acknowledgements
We gratefully acknowledge all members of the Institute for Health Metrics and Evaluation (IHME), University of Washington, and all collaborators involved in the Global Burden of Disease Study 2021.
Funding
This work was supported by the National Key Research and Development Program of China (grant number 2022YFC3601300) and the National Natural Science Foundation of China (grant number 82103904, 82270316 and 82100326).
Author information
Authors and Affiliations
Contributions
X.P., J.W. and C.T. contributed equally to this work. X.P., J.W. and L.H. conceived the study. X.P. and C.T. collected and analyzed the data. L.H., J.L. and X.K. double checked the data and results. X.P., J.W. and C.T. drafted the manuscript. L.H., X.K. and C.M. supervised and coordinated the study. S.X., N.Z., X.D., D.L. and J.D. provided important comments on the manuscript. L.H., X.K. and C.M. revised the final version of the manuscript. L.H., X.K. and C.M. are guarantors for this study. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Corresponding authors
Ethics declarations
Competing interests
Dr Ma has received honoraria for presentations from AstraZeneca, Bayer Healthcare, Boehringer Ingelheim, Bristol-Myers Squibb, Johnson & Johnson, and Pfizer. Dr Dong has received honoraria for presentations from Johnson & Johnson. All other authors declare no competing interests.
Ethics approval and consent to participate
No human participants, human data, human tissue and animals were involved in this study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this Article was revised: In the original version of this Article, Xiaodong Peng was incorrectly identified as the corresponding author.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Peng, X., Wang, J., Tang, C. et al. Sex-specific trends in the global burden and risk factors of atrial fibrillation and flutter from 1990 to 2021. Sci Rep 15, 8092 (2025). https://doi.org/10.1038/s41598-025-93338-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-93338-1
