
Abstract
Neonatal jaundice is a physiological phenomenon that occurs in newborns. However, because excess bilirubin can cause cytotoxicity, abnormal hyperbilirubinemia can lead to bilirubin encephalopathy. In the evaluation of neonatal jaundice, serum bilirubin concentrations are indirectly assessed via a transcutaneous bilirubinometer. However, commercially available transcutaneous bilirubinometers are expensive, especially in developing countries. Therefore, many newborns still suffer from bilirubin encephalopathy worldwide. We previously developed a prototype wearable jaundice meter. In this study, we aimed to investigate further improvements in this device and evaluate its measurement accuracy at different measurement sites and at different pressures. The bilirubin values of forty-eight newborns were measured at different sites (middle of the forehead and upper eyebrows) and with different pressures (1 and 2 newtons). The transcutaneous bilirubin values measured by the wearable bilirubin meter were strongly correlated with the transcutaneous bilirubin values measured by a commercially available bilirubin meter (r > 0.9) and the actual serum bilirubin values (> 0.84), even under different conditions. This wearable jaundice meter is much cheaper and smaller than commercially available jaundice meters and is a novel medical device that could be useful for evaluating neonatal jaundice.
Similar content being viewed by others

Introduction
Neonatal jaundice is a physiological phenomenon that occurs in newborns and is one of the most common symptoms encountered in neonatal care. However, a sudden increase or abnormally high serum bilirubin concentrations can cause bilirubin encephalopathy. Bilirubin encephalopathy can cause long-term neurological sequelae, such as cerebral palsy, hearing impairment, intellectual disability, and developmental delay. In Japan, since the 1970s, regular monitoring of transcutaneous bilirubin (TcB) using a transcutaneous bilirubin meter, phototherapy, and blood exchange transfusions has been introduced to reduce the incidence of bilirubin encephalopathy. Consequently, the number of full-term infants suffering from severe sequelae of bilirubin encephalopathy has greatly decreased in Japan1.
However, in developing and emerging countries, treatment for neonatal jaundice may be delayed owing to factors, such as difficulty accessing medical institutions and the inability to purchase expensive over-the-counter transcutaneous jaundice meters. In addition, the inability to purchase phototherapy devices or a lack of electricity to power them can prevent appropriate treatment. Therefore, many newborns still suffer from bilirubin encephalopathy and its sequalae worldwide. In fact, in low- and middle-income countries, bilirubin encephalopathy is one of the main causes of neonatal death and brain damage, and it is a health care issue that needs to be addressed2,3,4,5. In 2010, at least 481,000 term or near-term infants worldwide developed severe hyperbilirubinemia. A total of 114,000 of these children were estimated to have died, and more than 63,000 survived with moderate or severe disabilities. At least 75% of these patients are infants in sub-Saharan Africa and South Asia6,7,8. To improve this situation, we believe that developing a low-cost, easy-to-use TcB measurement device that anyone in the world could operate is necessary.
Monitoring total serum bilirubin (TSB) concentrations is important for the early detection of neonatal jaundice, which requires treatment. Judging the presence or absence of skin jaundice via visual inspection or the use of a colorimeter is unreliable because it deviates from the actual TSB concentration. Although the reliability of monitoring TSB values via blood sampling is high, even if blood is sampled once a day, it is still invasive and impractical for children. Therefore, noninvasive transcutaneous jaundice meters have been developed and are becoming more widespread, enabling monitoring of TcB values with high reliability. The most commonly used transcutaneous bilirubinometer in Japan is the JM series (JM-105; Konica Minolta, Inc., Tokyo, Japan). The JM-105 calculates bilirubin concentrations by measuring the difference in absorbance of blue (center wavelength: 450 nm) and green light (center wavelength: 550 nm) to calculate bilirubin concentrations9. The correlation between the TcB and TSB values via the JM series is strong10,11,12. There are also other transcutaneous jaundice meters on the market that use xenon lamps or light-emitting diodes (LEDs), but all of these devices are heavy (approximately 200 g) and expensive (approximately 5,000–10,000 USD per unit).
We have developed a lightweight and inexpensive wearable transcutaneous jaundice meter that can measure TcB concentrations and vital signs (Fig. 1)13. This device calculates TcB values on the basis of Lambert–Beer’s law from the difference in absorbance of blue and green light emitted from a small LED. In the clinical measurements of 50 neonates via this wearable transcutaneous jaundice meter, the correlation coefficient with the TcB value of the JM-105 was 0.81. The developed jaundice meter is highly reliable and inexpensive and is expected to be widely used in developing and emerging countries. However, there has been no detailed study of the ideal installation conditions for the measurement of TcB values via a wearable jaundice meter or the variation in values associated with these conditions. The investigation of these conditions should contribute to the accuracy of measurements of TcB values via jaundice meters, including wearable jaundice meters, and ultimately to the treatment of neonatal jaundice.

Overview of the developed device. (a) Internal structure of the device. (b) Appearance of the fabricated device. (c) Principle of measurement. (d) LED drive voltage and photodiode (PD) output voltage after signal processing.
In this study, we investigated installation conditions to improve the measurement accuracy of wearable jaundice meters. Specifically, we measured TcB values at different pressures on the skin and at different measurement sites on the head by installing a pressure sensor inside a wearable jaundice meter to reduce unevenness in measurements. By verifying the reliability of this system, we also evaluated its safety and clarified the conditions under which stable jaundice measurements can be made.
Methods
Study design, settings, and participants
This study was designed to improve our previously developed wearable transcutaneous jaundice meter13. We measured TcB values with this improved device at different measurement sites (middle of the forehead and upper eyebrows) and at different pressures and compared them with TcB values from a commercially available jaundice meter and actual serum bilirubin values. This multicenter, collaborative study was performed at Yokohama City University Hospital, Yokohama City University Medical Center, National Hospital Organization Yokohama Medical Center, and Yokohama Rosai Hospital. The study protocol was approved by the Yokohama City University ethics committee for Research on Life Sciences and Medicine (Approval No. B190200011) and was also approved by the ethics committee of each institution. This study was performed in accordance with relevant guidelines and regulations. Informed consent was obtained from all the participants’ legal guardians.
The neonates who participated in the study were born at the four abovementioned facilities between April and December 2021. Eligible patients were neonates who were born by at least 35 weeks of gestation, had a birth weight of at least 2,000 g, showed normal weight gain after birth, and whose mothers were able to admit them in the same room. Neonates who received medical treatment, such as cholestasis, oxygen administration, ventilator management, or infusion management, were excluded.
Measurement instruments
The basic principle of our wearable transcutaneous jaundice meter we developed is described in a previously published paper13. Briefly, the TcB values were calculated from the difference in the absorbances of blue and green light emitted from a small blue LED (KPTD-1608QBC-D, Kingblight electronic Co. Ltd., New Taipei, Taiwan) and a small green LED (KPTD-1608CGCK, Kingblight electronic Co. Ltd., New Taipei, Taiwan) on the basis of Lambert–Beer’s law. The blue light emitted by the small LED was at 460 nm, the wavelength at which bilirubin was most absorbent. The green light has a wavelength of 570 nm, which results in a low absorbance of bilirubin and a high absorbance of substances other than bilirubin, to eliminate the influence of substances other than bilirubin, such as melanin and hemoglobin oxide, in the skin. The formula for calculating the TcB value is shown below.
where C is the TcB value and IGreen and IBlue are the reflected light intensities of blue and green light, respectively. The constants α, D, and E depend on the emission intensity of the LED and the distance between the LED and the photodiode. Since this varies from device to device, they are calibration constants to be determined by performing calibration. Using the Bland-Altman Method as the criterion for calibration, the constants α, D, and E were determined when the mean error (ME) and the standard deviation (SD) of the difference between the developed device and commercial device were minimum and the correlation coefficient R was maximum. The actual procedure was performed in the following order. First, the constant α was set for the maximum R. Next, the constant D was set to minimize SD. Finally, the constant E was set so that ME would be zero. This device can also measure hyperbilirubinemia due to hemolysis.
The LED and photodiode (VBPW34S, Vishay Intertechnology, Inc., Pennsylvania, USA) were covered with a black silicone rubber material to prevent the LED light from mean errordirectly entering the photodetector (Fig. 1a, b). The black silicone rubber material was prepared by mixing polydimethylsiloxane (PDMS: SYLGARD 184Silicpne Elastomer, Dow Corning Corp., Michigan, USA) and Ecoflex (Ecoflex00-50, Smooth-On Inc., Pennsylvania, USA) at a ratio of 1:1 and was colored black. The light from the blue and green LEDs entered through the skin and was reflected by the skull. The reflected light was detected by a photodetector (Fig. 1c). The system of the fabricated device is operated by a Bluetooth low energy module (BLE module: EYSHCNZWZ, KAGA FEI Co., Ltd., Kanagawa, Japan). This BLE module also has the function of a microcontrol unit (MCU). This BLE module controls the measurement cycle and light emission timing of the two-color LEDs. The time interval of the measurement cycle was 500 ms, and the green and blue LEDs emitted light once every 4 ms. Figure 1d shows the LED drive current and the signal detected by the photodiode. The light transmitted through the skin was read by the photodetector and converted into a current, which was further amplified by an operational amplifier (AMP: NJM2732RB-TE1, New Japan Radio Co., Ltd., Tokyo, Japan), and the voltage data were read by the MCU and transmitted via Bluetooth to a smartphone (Fig. 2). All the materials were mounted on a foldable flexible substrate (PF-10R-A4, Sunhayato Corp., Tokyo, Japan) (Fig. 3). The processing system and display were on a smartphone or personal computer, which avoided a large device. This setup allowed the device to be wearable.

Schematic of our device. The PD detects the light intensity of two LEDs reflected from the skin. Signal processing is performed, and numerical values are displayed on a display device such as a smartphone.

Expanded view of our device. Each electronic element is mounted on a flexible substrate, and a flexible material is used for the interface. The flexible material is colored black to block light leakage and stabilize the LEDs.
In this study, improvements were made in the setup of the wearable jaundice meter (pressure and location) to improve the accuracy of this device. A force sensor (FSR404, Interlink Electronics Inc., California, USA) was actually mounted on a circuit board to enable the detection of applied pressure during measurement. The resistance of the force sensor decreases with applied pressure, and when a voltage is applied to one terminal, it can be measured from the other terminal as a voltage value corresponding to the applied pressure. A jig was also fabricated to detect applied pressure (Fig. 4a). By applying pressure to the apex of this jig, force is transmitted to the force sensor, which returns a corresponding voltage value. The voltage value was read by the MCU, which turned on a green LED from 0.5 to 1.5 N, a blue LED from 1.5 to 2 N, and a red LED > 2 N, and the read voltage value was transmitted to a smartphone via Bluetooth. The read voltage values were transmitted to the smartphone via Bluetooth (Fig. 4).

Installation and function of the developed device in a newborn. (a) Diagram of assembly of the device. (b) Measurement at 1 N of applied pressure on the center of the forehead. The pressure indicator LED on the device glows green. (c) Measurement at the top of the eyebrow on one side. (d) Applied pressure of 2 N. The pressure indicator LED on the device glows blue. (e) Applied pressure of ≥2 N. The pressure indicator LED on the device glows red.
Measurement methods
The wearable transcutaneous jaundice meter was turned on. The blinking of blue and green LEDs was confirmed. Next, we activated a web app for bilirubin measurement on our smartphones and connected the wearable jaundice meter to our smartphones via Bluetooth. Bluetooth is at the level of a normally used cell phone signal and has no adverse effect on newborns. We measured the TcB value by pressing the jaundice meter against the center of the neonate’s forehead and above the left or right eyebrow for 30 s (Fig. 4b, c). At each measurement site, the TcB values were measured at 1 N (N/m2) and 2 newtons of pressure. After the measurement, the device is turned off, and the data are saved on the web application. The measurement data were saved as a Comma-Separated Values file. Simultaneously, the TcB value was measured at the center of the forehead via a JM-105 transcutaneous jaundice meter (Konica Minolta). Five days after birth, or when TcB values measured with the JM-105 were close to or exceeded the criteria for indication for phototherapy, blood was collected to measure serum TSB concentrations to assess the indication for phototherapy.
TcB concentrations were measured once a day during hospitalization, and measurements were completed when the patient was discharged or required phototherapy for neonatal jaundice. Neonates whose parents provided consent early after birth were measured multiple times during hospitalization. The measurement site above the eyebrow was not specified as left or right. The presence or absence of skin damage such as skin redness was assessed after measurement with a wearable transcutaneous jaundice meter. In Japan, healthy newborns are usually discharged from the hospital at 5–7 days of age after birth.
Outcomes
The main outcome was the difference between the TcB values at the center of the forehead or at the area above the eyebrows measured via a wearable transcutaneous jaundice meter by applying a force of 1–2 N and the TcB values at the center of the forehead measured via the JM-105 or TSB values.
Statistical analysis
To evaluate the relationship between the TcB values measured via the wearable transcutaneous jaundice meter and the TcB values measured via the JM-105 or TSB values, scatter plots of each dataset were created, and correlation coefficients were calculated. The data were analyzed via simple correlation analysis via Excel software (Microsoft Co., Washington, USA). Bland–Altman analysis was performed to evaluate the error in the TcB values of the wearable transcutaneous jaundice meter and JM-105.

Correlations between the TcB values obtained via the wearable transcutaneous jaundice meter and those obtained via JM-105. (a) Center of the forehead with 1 N of applied pressure. (b) Center of the forehead with 2 N of applied pressure. (c) Upper eyebrow with 1 N of applied pressure. (d) Upper eyebrow with 2 N of applied pressure.

Measurement error of the TcB values between the wearable transcutaneous jaundice meter and JM-105. Average=JM-105+device/2. Difference=JM-105−device. (a) Center of the forehead with 1 N of applied pressure. (b) Center of the forehead with 2 N of applied pressure. (c) Upper eyebrow with 1 N of applied pressure. (d) Upper eyebrow with 2 N of applied pressure.

Correlations between the TcB values measured via the wearable transcutaneous jaundice meter and the serum bilirubin values. (a) Center of the forehead with 1 N of applied pressure. (b) Center of the forehead with 2 N of applied pressure. (c) Upper eyebrow with 1 N of applied pressure. (d) Upper eyebrow with 2 N of applied pressure. (e) Correlation between the TcB values measured by JM-105 and the serum bilirubin values.

Measurement error in the serum bilirubin concentration between the wearable transcutaneous jaundice meter and JM-105. Average=TSB+device/2. Difference=TSB−device. (a) Center of the forehead with 1 N of applied pressure. (b) Center of the forehead with 2 N of applied pressure. (c) Upper eyebrow with 1 N of applied pressure. (d) Upper eyebrow with 2 N of applied pressure.
Results
Patients’ background characteristics
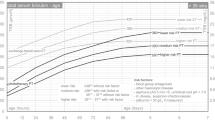
Forty-eight neonates, comprising 24 boys and 24 girls, were included in the study. The weeks of gestation at which neonates were born ranged from 37 to 41 weeks (median: 38.7 weeks), and the birth weights ranged from 2,288 to 4,000 g (median: 3,022 g). Measurements were taken on days 1–7 (median: day 4). The TcB values measured with JM-105 ranged from 35.91 µmol/L to 331.74 µmol/L (median: 218.88 µmol/L). The Japanese phototherapy criteria (Murata-Imura criteria) by birth weight and day of age are as follows. If the birth weight is greater than 2000 g, 171 µmol/L on day 1, 205.2 µmol/L on day 2, 239.4 µmol/L on day 3, 273.6 µmol/L on day 4, 290.7 µmol/L on day 5, 307.8 µmol/L on day 6 and 7; if the birth weight is greater than 2500 g, 205.2 µmol/L on day 1, 256.5 µmol/L on day 2, 290.7 µmol/L on day 3, 307.8 µmol/L on day 4, 324.9 µmol/L on day 5, 333.5 µmol/L on day 6, 342 µmol/L on day 7. A wearable transcutaneous jaundice meter was able to measure concentrations in the range of 47.40 µmol/L to 333.76 µmol/L.
Comparison of TcB values obtained by a wearable transcutaneous jaundice meter with those obtained by the JM-105
We obtained 73 measurements taken at the center of the forehead and 75 taken at the top of the eyebrows. The correlation coefficient between the TcB values of the wearable transcutaneous jaundice meter and those of JM-105 was 0.920 for the 1 N (N) measurement at the center of the forehead and 0.907 for the 2 N measurement at the center of the forehead. Similarly, the correlation coefficient for the measurement of 1 N above the eyebrow was 0.918, and that for the measurement of 2 N above the eyebrow was 0.907 (Fig. 5). The Bland–Altman analysis confirmed the agreement between the two instruments over the full range of TcB values. The abscissa represents the mean value of JM-105 and the wearable transcutaneous jaundice meter, and the ordinate represents the difference between JM-105 and the wearable transcutaneous jaundice meter. The limits of agreement are shown as dots (Fig. 6). The standard deviation (SD) of the error between TcB values of the wearable transcutaneous jaundice meter and those of JM-105 was 1.28 for 1 N at the center of the forehead and 1.37 for 2 N at the center of the forehead. Similarly, the SD of the error was 1.36 for 1 N above the eyebrow and 1.43 for 2 N above the eyebrow (see Supplementary Table S1 online).
Comparison of TcB and TSB values using a wearable transcutaneous jaundice meter
Forty data points measured at the center of the forehead and 41 data points measured at the top of one of the eyebrows were obtained via a wearable transcutaneous jaundice meter. The correlation coefficient between the TcB values and TSB values determined via the wearable transcutaneous jaundice meter was 0.856 for the 1 N pressure measurement at the center of the forehead and 0.840 for the 2 N measurement at the center of the forehead. The correlation coefficient between the TcB values and TSB values obtained via the wearable transcutaneous jaundice meter for the 1 N pressure measurement above the eyebrow was 0.871, and that for the 2 N pressure measurement above the eyebrow was 0.884 (Fig. 7). The correlation coefficient between TcB and TSB values obtained via the JM-105 was 0.90 (Fig. 7e).
Bland‒Altman analysis confirmed the agreement between the TcB and TSB values when the wearable transcutaneous jaundice meter was used. The abscissa represents the mean TSB values and TcB values obtained via the wearable transcutaneous jaundice meter, and the ordinate represents the difference between the TSB values and TcB values obtained via the wearable transcutaneous jaundice meter. The limits of agreement are shown as dots (Fig. 8). The SD of the error between the TcB and TSB values obtained via the wearable transcutaneous jaundice meter was 1.92 for 1 N at the center of the forehead and 2.02 for 2 N at the center of the forehead. Similarly, the SD was 1.90 for 1 N above the eyebrow and 1.80 for 2 N above the eyebrow (see Supplementary Table S2 online).
Discussion
In healthy neonates, the TcB values measured with our wearable transcutaneous jaundice meter strongly correlated with the TcB values measured with JM-105, and the TcB values also correlated with the TSB values. The SD of the error for the TcB values between our wearable transcutaneous jaundice meter and JM-105 was small, ranging from 1.28 to 1.43. This finding suggests that our jaundice meter can measure TcB values with almost the same accuracy as the commercially available JM-105. Differences in applied pressure during measurement are thought to have little effect on the measured values. Therefore, creating a compact device without a pressure sensor is possible. In the future, we plan to create a device that can be used for low-birth-weight infants.
In this study, the measurement time was as short as 30 s in healthy newborns. However, if a miniaturized wearable transcutaneous jaundice meter could be continuously fixed to the forehead, measurement over a longer period of time would be possible. Long-term continuous measurement enables the detection of hyperbilirubinemia without delay and can lead to early therapeutic intervention. Although this study revealed that there was no difference in measurement accuracy in any part of the forehead, further creative efforts are necessary to ensure continuous and stable placement of the wearable transcutaneous jaundice meter. Newborns’ body movements are not voluntary. Therefore, developing a cap that can hold the device stably even during large body movements and an adhesive that is less invasive to the skin of newborns may be necessary. Furthermore, regarding the battery operation time, our device can measure a maximum charge continuously for only 40 min. Therefore, installing a new battery or using a wired device is needed.
The world’s first transcutaneous jaundice meter was developed in Japan in 1980 (Jaundice Meter, JM-101; Minolta Camera, Ltd., Tokyo, Japan). BiliChek™ (SpectRx, Inc., Norcross, Georgia, USA)12,14, BiliMed™ (Nufer Medical, Guemligen/Berne, Switzerland)15, BiliTest™ (Bertocchi SRL Elettromedicali, Cremona, Italy)12,16, BiliCare™ (Mennen Medical, Ltd., Rehovot, Israel)17,18, KJ-8000™ (Xuzhou Kejian Hi-tech Co., Ltd., Xuzhou, Jiangsu, China)19, and many others were subseqeuntly developed. The JM series has improved over time, and JM-105 is currently widely used (Konica Minolta, Inc.).
All of these instruments are handheld instruments. Furthermore, the measured TcB values correlated with the TSB values. Handheld instruments have the advantage of being easy for anyone to use, but they are relatively large, weighing from 100 to 300 g. In addition, they are not maneuverable for a moving child. However, our wearable transcutaneous jaundice meter is much smaller and lighter, can be easily placed on a moving newborn’s forehead, and is easier to operate than other jaundice meters.
JM-105 is easy to perform, by simply pressing it against the forehead or anterior chest. Similarly, a wearable jaundice meter is easy to use because operators need only turn on the smartphone app and press the wearable jaundice meter against the forehead. The wearable transcutaneous jaundice meter is much smaller than the JM-105 and requires only 1 N of pressure on the forehead to take a measurement, which means that the physical burden on the newborn is small. BiliCam technology, which uses a smartphone application to estimate and measure TcB values, has been reported in the US20. BiliCam estimates and measures TcB values by simply taking a picture of a color calibration card placed on the chest and abdomen and the child’s skin on a single screen with a smartphone. The correlation coefficient between the BiliCam measurements and the TSB values is 0.91, which is a strong correlation.
While the selling price of the JM-105 is approximately 5,000 USD, the development cost of a wearable jaundice meter is considerably less expensive at approximately 100 USD. This price range is considered affordable in developing and emerging countries. Furthermore, since bilirubin, the causative agent of neonatal jaundice, can be measured automatically and over time, it eliminates the need for manual measurement by nurses and physicians, reducing physical and financial burdens. In summary, a wearable jaundice meter is expected to be widely used on the basis of the concept of a cheap, compact, and convenient device that is inexpensive, small, and easy for anyone to operate. BiliCam also has these features. However, BiliCam is an application used in home health care, such as making decisions about hospital visits, whereas the wearable jaundice meter is a small medical device used in medical facilities.
A limitation of this study is the small number of cases with TcB values below 171 µmol/L and higher than 342 µmol/L. In this study, 43 neonates had TcB values > 171 µmol/L and < 256.5 µmol/L, and 15 neonates had TcB values > 256.5 µmol/L and < 342 µmol/L measured by JM-105. These data represent 80% of the total subjects. In this study, a strong correlation was observed between the TcB values measured via the wearable jaundice meter and those measured via the JM-105. However, a discrepancy in TSB values has been reported to occur when the TcB values of JM-105 are ≥ 256.5 µmol/L21,22,23. Therefore, guaranteeing the accuracy of the wearable jaundice meter only by comparison with the JM-105 in cases of hyperbilirubinemia that require phototherapy may be difficult.
Another limitation is that the participants in this study were all Japanese because Japan is almost a monoethnic country. Maisels et al. compared TSB and TcB values in various ethnic groups via the JM-103 and reported a correlation in all ethnic groups but reported a slightly lower correlation in African Americans24. Several studies have compared TSB and TcB values in multiple ethnic groups and reported a high correlation in JM-103, independent of skin color25,26. Dam-Vervloet et al. reported that TcB values via the JM-105 are underestimated as skin pigmentation increases in an in vitro study27. There are many ethnic groups in developing and emerging countries that differ from the Japanese population. Therefore, data collected from multiple ethnic groups are preferable, and our results do not indicate that the correlation is as strong in other various ethnic groups as it is in Japanese individuals.
The wearable jaundice meter measures bilirubin and melanin on the basis of their different light absorption characteristics. Bilirubin absorbs blue light, whereas melanin and hemoglobin absorb blue and green light. The wearable jaundice meter calculates bilirubin concentrations from the ratio of blue and green light absorption. Although the amount of melanin in the skin varies by race, bilirubin can be accurately measured by a transcutaneous jaundice meter regardless of race, and we expect that a correlation will also be found in other ethnic groups25,28. The correlation between TSB and TcB values needs to be examined in races whose skin color differs from that of Japanese individuals.
There are several limitations to this study. The number of subjects for which the TcB and TSB values obtained by the wearable jaundice meter were compared was small, and the correlation coefficient was relatively low. Therefore, a larger number of subjects is required to ensure the accuracy of the TcB and TSB values obtained by the wearable jaundice meter. In addition, a comparison between lower and higher total bilirubin values that could not be collected in this study is needed in the future. If the bilirubin value is even greater, the formula for determining the TcB value in the device may change and may need to be adjusted. The battery has a short operating time and should be replaced as needed. Owing to its large size for preterm infants, the current device size is limited to measurements for newborns over 2,000 g.
In conclusion, if our wearable jaundice meter is implemented, it may reduce brain damage due to hyperbilirubinemia in newborns in developing and emerging countries.
Data availability
The raw data were generated at Yokohama National University. The derived data supporting the findings of this study are available from the corresponding authors (S.I. and H.O.) upon request.
References
Nakamura, H., Morioka, I., Yonetani, M., Funato, M. & Arai, H. Current topics in the management of hyperbilirubinemia in the preterm infants less than 30 weeks of gestation. J. Japan Soc. Premature Newborn Med. 26, 57–66 (2014).
Olusanya, B. O. et al. Management of late-preterm and term infants with hyperbilirubinaemia in resource-constrained settings. BMC Pediatr. 15, 39. https://doi.org/10.1186/s12887-015-0358-z (2015).
Greco, C. et al. Neonatal jaundice in low- and middle-income countries: lessons and future directions from the 2015 don Ostrow Trieste yellow retreat. Neonatology 110, 172–180. https://doi.org/10.1159/000445708 (2016).
Slusher, T. M. et al. Burden of severe neonatal jaundice: a systematic review and meta-analysis. BMJ Paediatr. Open. 1, e000105. https://doi.org/10.1136/bmjpo-2017-000105 (2017).
Satrom, K. M., Farouk, Z. L. & Slusher, T. M. Management challenges in the treatment of severe hyperbilirubinemia in low- and middle-income countries: encouraging advancements, remaining gaps, and future opportunities. Front. Pediatr. 13 https://doi.org/10.3389/fped.2023.1001141 (2023).
Bhutani, V. K. et al. Neonatal hyperbilirubinemia and rhesus disease of the newborn: incidence and impairment estimates for 2010 at regional and global levels. Pediatr. Res. 74, 86–100. https://doi.org/10.1038/pr.2013.208 (2013).
GBD 2016 Causes of Death Collaborators. Global, regional, and National age-sex specific mortality for 264 causes death, 1980–2016: a systematic analysis for the global burden of disease study 2016. Lancet 390, 1151–1210. https://doi.org/10.1016/s0140-6736(17)32152-9 (2017).
Olusanya, B. O., Teeple, S. & Kassebaum, N. J. The contribution of neonatal jaundice to global child mortality: findings from the GBD 2016 study. Pediatrics.141, e20171471 ; (2018). https://doi.org/10.1542/peds.2017-1471
https://www.konicaminolta.jp/healthcare/attached/pdf/jm105.pdf (2019).
Lucanova, L. C., Zibolenova, J., Matasova, K., Docekalova, L. & Zibolen, M. Accuracy of enhanced transcutaneous bilirubinometry according to various measurement sites. Turk. Arch. Pediatr. 56, 15–21. https://doi.org/10.14744/turkpediatriars.2020.54514 (2021).
Mohamed, M. et al. Comparison between the transcutaneous and total serum bilirubin measurement in Malay neonates with neonatal jaundice. Malays J. Med. Sci. 29, 43–54. https://doi.org/10.21315/mjms2022.29.1.5 (2022).
Okwundu, C. I. et al. Transcutaneous bilirubinometry versus total serum bilirubin measurement for newborns. Cochrane Database Syst. Rev. 5 https://doi.org/10.1002/14651858.cd012660.pub2 (2023).
Inamori, G. et al. Neonatal wearable device for colorimetry-based real-time detection of jaundice with simultaneous sensing of vitals. Sci. Adv. 7, eabe3793. https://doi.org/10.1126/sciadv.abe3793 (2021).
Jones, D. F. et al. A prospective comparison of transcutaneous and serum bilirubin within brief time intervals. Clin. Pediatr. (Philia). 56, 1013–1017. https://doi.org/10.1177/0009922817701170 (2017).
Karen, T., Bucher, H. U. & Fauchère, J. C. Comparison of a new transcutaneous bilirubinometer (Bilimed) with serum bilirubin measurements in preterm and full-term infants. BMC Pediatr. 9, 70. https://doi.org/10.1186/1471-2431-9-70 (2009).
Bertini, G., Pratesi, S., Cosenza, E. & Dani, C. Transcutaneous bilirubin measurement: evaluation of bilitest. Neonatology 93, 101–105. https://doi.org/10.1159/000107351 (2008).
Yamana, K. et al. Evaluation of BiliCare™ transcutaneous bilirubin device in Japanese newborns. Pediatr. Int. 59, 1058–1063. https://doi.org/10.1111/ped.13364 (2017).
Chen, Y., Lake, S. & Scott, K. Accuracy and reproducibility of BiliCare™ transcutaneous bilirubin device. Clin. Lab. 69, (2023). https://doi.org/10.7754/clin.lab.2023.230117
Olivia, S., Edwards, P., Schmidt, P. & Birch, P. Evaluation of the Kejian KJ-8000 bilirubinometer in an Australian setting. J. Paediatr. Child. Health. 56, 283–288. https://doi.org/10.1111/jpc.14597 (2020).
Taylor, J. A. et al. Use of a smartphone app to assess neonatal jaundice. Pediatrics 140, e20170312. https://doi.org/10.1542/peds.2017-0312 (2017).
Kurokawa, D. & Morioka, I. Neonate with severe jaundice. Japanese J. Midwives. 70, 102–107 (2016).
Taylor, J. A. et al. Discrepancies between transcutaneous and serum bilirubin measurements. Pediatrics 135, 224–231. https://doi.org/10.1542/peds.2014-1919 (2015).
Ohishi, A., Kondo, M., Fujita, T., Baba, T. & Iijma, S. Accuracy of transcutaneous bilirubin level measured by JM-105 bilirubinometer. Pediatr. Neonatol 64, 32–37 ; https://doi.org/10.1016/j.pedneo.2022.05.012(2023).
Maisels, M. J. et al. Evaluation of a new transcutaneous bilirubinometer. Pediatrics 113, 1628–1635. https://doi.org/10.1542/peds.113.6.1628 (2004).
Raimondi, F. et al. Measuring transcutaneous bilirubin: a comparative analysis of three devices on a multiracial population. BMC Pediatr. 12, 70. https://doi.org/10.1186/1471-2431-12-70 (2012).
Afanetti, M., Trolli, S. E. D., Yousef, N., Jrad, I. & Mokhtari, M. Transcutaneous bilirubinometry is not influenced by term or skin color in neonates. Early Hum. Dev. 90, 417–420. https://doi.org/10.1016/j.earlhumdev.2014.05.009 (2014).
Dam-Vervloet, A. J. et al. Skin color influences transcutaneous bilirubin measurements: a systematic in vitro evaluation. Pediatr. Res. 17 https://doi.org/10.1038/s41390-024-03081-y (2024).
Bhutani, V. K. et al. Noninvasive measurement of total serum bilirubin in a multiracial predischarge newborn population to assess the risk of severe hyperbilirubinemia. Pediatrics 106, e17. https://doi.org/10.1542/peds.106.2.e17 (2000).
Acknowledgements
We thank Ellen Knapp, PhD, from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Funding
The research project titled “Development of a Smart Phototherapy Device for Optimization of Neonatal Jaundice Treatment” was funded by the Japan Agency for Medical Research and Development (AMED) (grant number: 21hm0102085h0002).
Author information
Authors and Affiliations
Contributions
H.O. and S.I. designed the study. I.O., M.S., and F.K. fabricated the devices. A.U., I.O., M.S., K.I., A.F., and H.H. collected the data. A.U., I.O., M.S., and Y.I. analyzed and interpreted the results and drafted the manuscript. S.I. supervised the project. A.U. wrote the manuscript with support from S.I. and H.O. All the authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Uozumi, A., Ohara, I., Shimamura, M. et al. Clinical evaluation of the installation conditions and accuracy of wearable neonatal jaundice meter. Sci Rep 15, 12909 (2025). https://doi.org/10.1038/s41598-025-93776-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-93776-x
