
Abstract
This study aimed to compare three different loops (T loop, Cherry loop, and Open helical loop) and optimal tip back angle (10°, 15°, 20°) for protraction of mandibular second molar using Finite Element Model (FEM). A CBCT scan of a 20-year-old patient was recorded. It was converted into a CAD file and then into a FEM. A FEM model developed was used to find out the efficacy of the loops and optimal tip-back angles. Displacement of the molar was measured at four reference points: the mesio-buccal cusp, distobuccal cusp, mesial root, and the distal root of the first molar. No significant difference was seen in the displacement for all three loops. At a 10° angle, there was more mesial tipping (5.9°) and molar extrusion. At a 15° angle, there was less mesial tipping (2.9-3°) and no changes in the vertical plane. At a 20° angle, there was bodily movement and intrusion of molars. All three loops are equally effective in the protraction of mandibular molar. A 15° tip back angle was most effective in protracting the mandibular molar as only a negligible amount of mesial tipping of the molar was seen, and there was no extrusion or intrusion of the molar, thus maintaining the occlusal plane. Loop mechanics are preferred over the use of power chains as this helps maintain better control over the molar position during protraction. Loops are very effective at avoiding mesial tipping and extrusion of molars during mesialization to close spaces.
Similar content being viewed by others

Introduction
The mandibular first molar is the most commonly extracted tooth due to caries1. Loss of the first molar causes mesial tipping of the second molar in the extraction space; thus, inadequate space is left for prosthetic replacement of the first molar. Previously, prosthetic replacement of the first molar was the only treatment option considered. Protraction of the second molar in the first molar space was not undertaken as it is one of the most challenging orthodontic tooth movements due to increased anchorage demands. With the advent of temporary anchorage devices, the protraction of molar has become less challenging. According to Zachrisson2, orthodontic tooth movement is an excellent way to regenerate new alveolar bone and soft tissue. However, if a prosthetic implant is considered a choice of treatment, there will be a need for autogenous or allogenic grafts in cases of atrophic alveolar ridge. Other situations where molar protraction is required are in cases of Angle’s class II malocclusion, where mesializing the molar will correct the distocclusion, and in cases of high mandibular plane angle, like skeletal open bite cases where protracting the molars will close the bite due to ‘wedge effect’1.
Molar protraction in the mandible is more complicated than in maxilla3 due to dense cortical bone, and roots of the mandibular molar are wider buccolingually than mesiodistally. Protraction of molar is challenging, adults typically require more treatment period than children, as children have fewer periodontal and root resorption problems during molar protraction. Moreover, alveolar height and width reduction is seen in long-standing edentulous sites, which limits the mesial movement of molar. Initially, the threshold for mandibular molar’s mesial movement was considered 7 mm buccolingually and 6 mm for mesiodistally4. Later, molar protraction in the edentulous ridge was found to lead to bone regeneration.
Protraction of molar can be done by friction or frictionless mechanics. The advantage of frictionless mechanics is that it does not have to overcome the frictional resistance to tooth movement. The side effects that occur during molar protraction are mesial tipping and mesio-lingual rotation of the molar. These side effects can be avoided by understanding the biomechanical variables affecting molar protraction by applying appropriate tip-back and toe-in angles in the loop design.
There is abundant literature available for loops used in retraction, but there is limited literature regarding loops used for protraction; thus, this study was undertaken. The present study uses the finite element (FE) method to find out the efficacy of three different loops i.e. T loop, Cherry loop, and Open helical loop, and the optimal tip back angles among 10°, 15°, and 20° for all three loops, that can be used clinically to bodily protract mandibular second molar in the space of first molar without any undesirable movements. The Null hypothesis assumed that the effect of all three loops on molar movement will be different.
Materials and methods
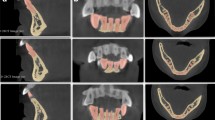
A full-face CBCT model of a 20-year-old female patient was taken from the Department of Oral Medicine and Radiology at Karnavati School of Dentistry. Written informed consent was obtained from the patient for use of their records for academic and research purposes. Ethical approval was applied for and obtained from the ethics committee at Karnavati School of Dentistry with the ethical number: KSDEC/21–22/Apr/012.
The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments.
A finite element model was constructed for simulating orthodontic tooth movement. The following steps were followed for the construction of FE Model:
-
1.
3D slicer (slicer.org) was used to convert CBCT DICOM file into STL format5.
-
2.
FreeCAD software Current stable version: 0.20.2 was used for the construction of CAD model.
-
3.
ANSYS Student version 19.2 was used for FE analysis.
-
4.
Tecplot 360 was used for FE post-processing.
The CBCT scan of the patient was converted from a DICOM file to STL file. A CAD model was prepared, and it was edited such that the first molar was extracted from it to simulate molar protraction in the space. CAD models of T loop, Cherry loop and Open helical loop were made from 19 × 25 titanium molybdenum alloy wire. (Fig. 1) Dimensions of Cherry loop taken are 8 mm width and 8 mm height and 4 mm of distance between the loop ends6. For T loop, the height of vertical legs was 5 mm and the horizontal leg was 10 mm7. The open helical loop of 8 mm height and 3 mm size of the helix was considered8. The loop was positioned off-centre closer to the premolar to increase anterior anchorage and so that molar would not strike the loop while moving forward. CAD model was converted into a FEmodel. A complex structure was discretized into small elements. Tetrahedral elements were used in this model. The thickness of periodontal ligament was assumed to be uniform of 0.2 mm in dimension9. Brackets of 0.022 × 0.028-inch slot and buccal tube of 4 mm length were used. Whenever the procedure of molar protraction is carried out a segment of anteriors and premolars are consolidated to act as a single unit to enhance anchorage. Thus, teeth (anteriors and premolars), alveolar bone, and brackets were defined as rigid bodies. Frictional coefficient (µ = 0.15)9 was taken to simulate the interaction between buccal tube and wire. Three different tip back angles were given that are 10°, 15° and 20° were the anterior segment is kept constant and a constant toe in angle of 10° was given for all the cases as this angulation is considered to be optimal for bodily movement of molars during protraction9. A protraction force of 1.5 N was applied.

CAD file of all the three loops. (A) T loop, (B) Open helical loop, (C) Cherry loop.
The mechanical properties of tooth, bone, periodontal ligament, and Titanium molybdenum alloy (TMA) wire used are as follows10,11 (Table 1):
Grid Dependence test was performed in order to determine the final number of nodes and elements which were 36,463 and 100,656 respectively.
Simulation of tooth movement: In long-term tooth movement simulation, using an elastic support boundary condition in ANSYS was a justifiable choice, especially when combined with a steady-state simulation approach. An elastic support boundary condition was used assuming that the PDL can be modeled as a linear, elastic material that responds to mechanical loads in a predictable manner. This boundary condition accurately represents the elastic behavior of the PDL under physiologic loading conditions and is computationally efficient.
Tecplot 360 was used for postprocessing of the simulation to interpret the results. Linear displacement was calculated at the mesio-buccal cusp (MBC), distobuccal cusp (DBC), mesial root (MR) and distal root (DR) and angular deviation of the long axis of the molar tooth was measured post protraction compared to initial position of molar. Displacement was calculated in all three planes of space X, Y, Z axis. X axis represents transverse plane, Y axis represents sagittal plane and Z axis represents vertical plane. Positive value along X axis indicates movement towards the lingual side and negative value indicates movement towards buccal direction. Positive value along Y axis indicates distal movement and negative value indicates mesial movement. Positive value along Z axis indicates extrusive movement and negative value indicates intrusive movement.
Results
The results obtained for each loop (T loop, Cherry loop and open helical loop) at three tip back angles (10°, 15° and 20°) is explained as the displacement of mesio-buccal cusp, distobuccal cusp, mesial root and distal root in all three planes of space where X axis indicates transverse plane, Y axis represents sagittal plane and Z axis represents vertical plane and rotation (mesial or distal tipping) of molar along the X axis.
Results obtained for the T loop
At a 10° tip back angle: The mesiobuccal cusp showed 1.7 mm of mesial movement and 0.1 mm of intrusive movement. The distobuccal cusp showed 1.6 mm of mesial movement and 0.4 mm of extrusive movement. The mesial root showed 0.1 mm of distal movement and 0.2 mm of extrusive movement. The distal root showed 0.072 mm of distal movement and 0.5 mm of extrusive movement. Rotation of molar along X axis was by 5.9°. Thus, there was mesial tipping of molar along with extrusion (Fig. 2) (Tables 2 and 3).

Molar protraction obtained with T loop. (A) T loop with 10° tip back angle with occlusal view, (B) T loop with 15° tip back angle with occlusal view, (C) T loop with 20° tip back angle with occlusal view.
At a 15° tip back angle: The mesiobuccal cusp showed 1.5 mm mesial movement and 0.09 mm of intrusive movement. The distobuccal cusp showed 1.5 mm of mesial movement and 0.19 mm of extrusive movement. The mesial root showed 0.7 mm of mesial movement and no extrusive or intrusive movement. The distal root showed 0.7 mm of mesial movement and 0.1 mm of extrusive movement. Rotation of molar along X axis was by 2.9°. This indicates there was minimal amount of tipping of molar with no changes in vertical plane (Fig. 2; Tables 2 and 3).
At a 20° tip back angle: The mesiobuccal cusp showed 1.3 mm of mesial movement and 0.07 mm of intrusive movement. The distobuccal cusp showed 1.3 mm of mesial movement and 0.06 mm of intrusive movement. The mesial root showed 1.4 mm of mesial movement and 0.14 mm of intrusive movement. The distal root showed 1.4 mm of mesial movement and 0.2 mm of intrusive movement. Rotation of molar along X axis by 0°. This indicated that there was bodily translation of molar with intrusion of molar. (Fig. 2; Table 2 and& 3)
Results obtained for the Cherry loop
At a 10° tip back angle the mesiobuccal cusp showed 1.7 mm mesial movement and 0.06 mm of intrusive movement. The distobuccal cusp showed 1.7 mm mesial movement and 0.5 mm of extrusive movement. The mesial root showed 0.09 mm of distal movement and 0.2 mm of extrusive movement. The distal root showed 0.07 mm of distal movement and 0.18 mm of extrusive movement. Molar rotation along X axis was 5.9°. Thus, there was mesial tipping of molar along with extrusion (Fig. 3; Tables 2 and 3).

Molar protraction obtained with cherry loop. (A) Cherry loop with 10° tip back angle with occlusal view, (B) Cherry loop with 15° tip back angle with occlusal view, (C) Cherry loop with 20° tip back angle with occlusal view.
At a 15° tip back angle the mesiobuccal cusp showed 1.5 mm mesial movement and 0.06 mm intrusive movement. The distobuccal cusp showed 1.5 mm of mesial movement and 0.2 mm extrusive movement. The mesial root showed 0.6 mm of mesial movement and 0.05 mm of extrusive movement. The distal root showed 0.6 mm of mesial movement and 0.18 mm of extrusive movement. Molar rotation along X axis was 3°. This indicates there was minimal amount of tipping of molar with no changes in vertical plane (Fig. 3; Tables 2 and 3).
At a 20° tip back angle the mesiobuccal cusp showed 1.3 mm mesial movement and 0.06 mm of intrusive movement. The distobuccal cusp showed 1.3 mm of mesial movement and 0.04 mm intrusive movement. The mesial root showed 1.4 mm mesial movement and 0.12 mm intrusive movement. The distal root showed 1.4 mm mesial movement and 0.17 mm of intrusive movement. Molar rotation along X axis was 0°. This indicated that there was bodily translation of molar with intrusion of molar (Fig. 3; Tables 2 and 3).
Results obtained for the open helical loop
At a 10° tip back angle the mesiobuccal cusp showed 1.7 mm mesial movement and 0.09 mm of intrusive movement. The distobuccal cusp showed 1.7 mm mesial movement and 0.49 mm of extrusive movement. The mesial root showed 0.05 mm distal movement and 0.2 mm extrusive movement. The distal root showed 0.02 mm distal movement and 0.5 mm extrusive movement. At 10° tip back bend the molar rotated along X axis by 5.9°. Thus, there was mesial tipping of molar along with extrusion. (Fig. 4) (Tables 2 and 3).

Molar protraction obtained with Open Helical loop. (A) Open helical loop with 10° tip back angle with occlusal view, (B) Open helical loop with 15° tip back angle with occlusal view, (C) Open helical loop with 20° tip back angle with occlusal view.
At a 15° tip back angle the mesiobuccal cusp showed 1.5 mm mesial movement and 0.09 mm intrusive movement. The distobuccal cusp showed 1.5 mm mesial movement and 0.19 mm extrusive movement. The mesial root showed 0.7 mm mesial movement and no intrusive or extrusive movement. The distal root showed 0.7 mm mesial movement and 0.12 mm extrusive movement. At 15° tip back bend the molar rotated along X axis by 2.9°. This indicates there was minimal amount of tipping of molar with no changes in vertical plane (Fig. 4; Tables 2 and 3).
At a 20° tip back angle the mesiobuccal cusp showed 1.3 mm mesial movement and 0.10 mm of intrusive movement. The distobuccal cusp showed 1.3 mm of mesial movement and 0.10 mm intrusive movement. The mesial root showed 1.4 mm mesial movement and 0.16 mm intrusive movement. The distal root showed 1.5 mm mesial movement and 0.22 mm of intrusive movement. At 20° tip back bend the molar rotated along X axis by 0°. This indicated that there was bodily translation of molar with intrusion of molar (Fig. 4; Tables 2 and 3).
Discussion
The most common scenarios where molar protraction is performed3 is correction of Angle’s class II malocclusion, open bite cases and replacing the extraction space of first molar by mesialization of second and third molars. Molar protraction is now considered as an alternative treatment plan instead of a prosthesis in missing first molar space. When this edentulous space of missing first molar is closed entirely by protraction of second molar the common side effects that occur while protracting the molar over a long edentulous space are mesial tipping and mesiolingual rotation of the second molar crown. Thus, it is necessary to incorporate tip back and toe in bends in the loop design used for protracting the molar. There is limited literature available for molar protraction using loops thus the present study was undertaken to find out the most efficient loop and appropriate tip back angle.
In this study as we increase the tip back Angle from 10°, to 15° to 20° the mesial tipping of molar reduces in all the loops. The mesial tipping of 5.9° was seen at 10° tip back angle, mesial tipping of about 3° was seen at 15° tip back angle and molar translated forward at a tip back angle of 20°. This occurs because as we increase the amount of vertical bend, there is an increase in the M/F ratio which leads to more amount of root movement12. These results are similar to the study by Abhay Chaudhari13, which stated the effect of increasing the number of gable bends in a T loop. He found that greater gable bend produced higher moment to force ratio required for tooth translation. Similar results were seen in the study done by Paiboon et al.14, they found that adding a vertical bend in T loop increased the M/F ratio enough to produce root movement.
At 10°, tip-back angle mesial crown and distal root movement with extrusion of distobuccal cusp and intrusion of mesiobuccal cusp was seen. If the molar tips mesially while protracting there are greater chances of relapse as the roots are tipped distally. Due to mesial tipping of molar during protraction molar extrusion may occur which affects the vertical dimension of the face as it causes clockwise rotation of the mandible. In low angle cases, molar extrusion is helpful as it helps in opening of the deep bite. However, in high angle cases or in cases of skeletal open bite, extrusion of molar has to be controlled by using appropriate treatment mechanics3.
At 15° tip back angle there was slight amount of mesial tipping of 3° but crown and root both showed movement in mesial direction. Changes in vertical plane were minimal at 15° tip back angle. Thus, it can be used in cases where the occlusal plane of the patient has to be maintained. The mesial movement achieved was more at 15° tip back angle than at 20°. Ryu et al.8 performed a FEM study to find out the appropriate bending angles for mandibular molar protraction using a running loop. He found out that a tip back angle of 11.5° and toe in Angle of 9.9° helps in achieving bodily protraction of molar. Kim and Park15 also suggested that the optimal tip back angle should be 11° using a running loop for mesial translation of mandibular molar using indirect anchorage.
At 20° tip back angle along with bodily translation of molar a slight amount of intrusion is seen on the molar. This is helpful in cases of vertical growth pattern. As the tip back Angle increases, the intrusive component of force increases thus these results are obtained. This finding was analogous with findings of Burstone and Koeing16, they explained that when the loop is placed closer to the anterior segment there is an extrusive force at the segment where shorter arm of the loop is engaged whereas at the posterior segment a vertical intrusive force is seen. Proffit17 also explained this with the help of V bend principle, the loop position acts like an off centered V bend.
Wu et al.18 also suggested that a tip back angle of 20 to 30° and a toe in Angle of 15° were given while protracted the mandibular molar using a L loop. Similar amount of tip back bend was suggested by Chae and Kim19 et al. that is 20 to 30° while using a running loop for protraction of mandibular molar. Saga et al.20 also suggested that a 20° tip back bend should be given while mesializing mandibular molar using a helical loop. Narmada et al.21 in their case report applied a tip back angle on 20–30° but this caused the slight distal tipping of molar at the end of treatment.
Thus, the amount of tip back bend to be given during mandibular molar protraction should be between 15° to 20°. Tip back bends have the benefit of a wide activation range and constant moment application22.
There were no differences seen in movement of molar in the three loops thus the null hypothesis was rejected. The changes seen were mainly due to the change in tip back Angle. This finding can be explained as the length of wire incorporated in all three loops is equivalent, so the length of the wire incorporated in loop design has an effect on the moment to force ratio produced by the loop. Chen et al.23 suggested that if we increase the vertical or horizontal dimension of the loop there is reduction in the load deflection rate. Reducing the dimension of the loop increased the load deflection rate and the stress in the loop and reduces the moment to force ratio dramatically.
Future recommendations
The study can be further extended by performing clinical trials to evaluate the efficiency of T loop, Cherry loop and Open helical loop and the effect of tip back angles on molar protraction as well as the effect of patient related factors like age, periodontal health and occlusal forces that effect tooth movement.
Conclusion
The conclusion can be drawn as follows:
-
1.
All the three loops are equally effective in protraction of mandibular molar.
-
2.
15° tip back angle was most effective in protracting the mandibular molar as there was only negligible amount of mesial tipping of molar and there was no extrusion or intrusion of molar thus maintaining the occlusal plane.
-
3.
At 10° tip back angle there was more amount of tipping movement of molar and extrusion of molar in relation to occlusal plane.
-
4.
At 20° tip back angle there was bodily translation of molar along with intrusion of molar, thus can be used case specific.
Data availability
All data related to the study can be provided on reasonable request from the corresponding author.
References
Goje, S. & Jain, R. Evaluation of changes in the vertical dimension following mesialization of mandibular molars between average and hyperdivergent facial type: A retrospective cephalometric study. J. Posit. School Psychol. 6 (5), 6980–6988 (2022).
Zachrisson, B. U. Implant site development by horizontal tooth development. World J. Orthod. 4, 266–272 (2003).
Asok et al. Molar Protraction – A review. IP Indian J. Orthod. Dentofac. Res. 6 (4), 229–235231 (2020).
Barney, M., Hom, P. K. & Turley The effects of space closure of the mandibular first molar area in adults. Am. J. Orthod. 85 (Issue 6), 457–469 (1984).
Fedorov, A. et al. Kikinis R. 3D slicer as an image computing platform for the quantitative imaging network. Magn. Reson. Imaging. 30 (9), 1323–1341 (2012).
Peretta, R. & Segù, M. Cherry loop: a new loop to move the mandibular molar mesially. Prog Orthod. 2 (1), 24–29 (2001).
Hoenigl, K. D., Freudenthaler, J., Marcotte, M. R. & Hans-Peter, B. The centered T-loop—A new way of preactivation. Am. J. Orthod. Dentofac. Orthop. 108 (2), 149–153 (1995).
Faulkner Use of vertical loops in Retraction systems. Am. J. Orthod. Dentofac. Orthop. 99 (4), 328–336 (1991).
Woon- Kuk Ryu. Prediction of optimal bending angles of a running loop to achieve bodily Protraction of a molar using the finite element method. Korean J. Orthod. 48 (1), 3–10 (2018).
Chacko et al. Comparative assessment of the efficacy of closed helical and T loop for space closure in lingual orthodontics – a finite element study. Prog. Orthodont. ;19(1). (2018).
Vanessa et al. Comparative evaluation of compressive stresses on the periodontal ligament adjacent to two differently angulated Miniscrew implants (MSIs). Saudi J. Oral Dent. Res. 6 (6), 234–239 (2021).
Paiboon Techalertpaisarna. T-loop force system with and without vertical step using finite element analysis. Angle Orthod. 86 (3), 372–379 (2016).
Chaudhari, A. R. et al. T-Loop position and anchorage control: A finite element study. J. Ind. Orthod. Soc. 47 (4), 171–177 (2013).
Paiboon et al. Mechanical properties of opus closing loops, L-loops, and T-loops investigated with finite element analysis. Am. J. Orthod. Dentofac. Orthop. 143 (5), 675–683 (2013).
Kim et al. A finite element analysis of the optimal bending angles in a running loop for mesial translation of a mandibular molar using indirect skeletal anchorage. Orthod. Craniofac. Res. 21 (1), 63–70 (2018).
Burstone and Koeing. Optimizing anterior and canine Retraction. Am. J. Orthod. 70 (1), 1–19 (1976).
Proffit, W. R. The second stage of comprehensive treatment: correction of molar relationship and space closer. In (eds Proffit, W. R., Fields, H. W. Jr & Sarver, D. M.) Contemporary Orthodontics. 4th ed. St Louis: Mosby Elsevier; (2007).
Wu, J., Zheng, Y. & Dai, Y. Protraction of mandibular molars through a severely atrophic edentulous space in a case of juvenile periodontitis. Korean J. Orthod. 50 (2), 145–154 (2020).
Chae, J. & Kim, S. Running loop in unusual molar extraction treatment. Am. J. Orthod. Dentofac. Orthop. 132 (4), 528–539 (2007).
Saga et al. Orthodontic treatment with passive eruption and mesialization of semi-impacted mandibular third molar in an adult with multiple dental losses. Dent. Press. J. Orthod. 24(6), 36–47 (2019).
Narmada et al. Management of bimaxillary protrusion with missing molar using T-loop and couple force Dent. J. (Majalah Kedokteran Gigi). 56 (1), 17–22 (2023).
David Romeo. Tip back mechanics. Am. J. Orthod. Dentofac. Orthop. 72 (4), 414–421 (1977).
Chen, J., Isikbay, S. C. & Brizendine, E. J. Quantification of three-dimensional orthodontic force systems of T-loop archwires. Angle Orthod. 80 (4), 566–570 (2010).
Acknowledgements
The authors express their thanks and gratitude to AlMaarefa University, Riyadh, Saudi Arabia for the support to publish this article.
Author information
Authors and Affiliations
Contributions
A.D., A.S., A.P, B.J and K.S. wrote the main manuscript text and A.K. prepared figures. N.C. S.I. , M.F. and A.M. reviewed and edited the main manuscript and analyzed the data and helped with tabulation. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
Ethical approval was applied for and obtained from the ethics committee at Karnavati School of Dentistry with the ethical number: KSDEC/21–22/Apr/012. The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments.
Patient consent
Written informed consent was obtained from the patient for use of their records for academic and research purposes.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Mehta, A., Shah, A., Prasad, A. et al. Finite element study of the efficacy of three different loops for bodily protraction of the mandibular molar. Sci Rep 15, 13938 (2025). https://doi.org/10.1038/s41598-025-94627-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-94627-5
Keywords
This article is cited by
-
Orthodontic mesialization of third molars using a t-shaped palatal indirect anchorage device for posterior dentition rehabilitation: a case report and literature review
BMC Oral Health (2025)
-
Comparative study by FEM of different liners of a transfemoral amputated lower limb
Scientific Reports (2025)
-
Biomechanical evaluation of a lower-limb implant model under gait and stumbling conditions using finite element analysis
Scientific Reports (2025)
