
Abstract
Water is vital for the human body. Due to concerns over tap water, preference for taste, and convenience, there has been increased consumption of reverse osmosis (RO) water. Various metal ions (e.g., magnesium, calcium, sodium) are essential for human growth and function. Evaluate and compare serum calcium, magnesium, phosphate, alkaline phosphatase, and vitamin D levels in children consuming RO, non-RO, and high-fluoride drinking water. This comparative study included children aged 9–13. Participants were divided into three groups: RO water drinkers, non-RO water drinkers, and those consuming high-fluoride water. A questionnaire gathered socio-demographic, medical, sunlight exposure, and including a validated food frequency questionnaire (FFQ) for nutrient intake. Water samples were analyzed per APHA guidelines for calcium, magnesium, phosphorous, fluoride, and TDS. Urine samples assessed calcium and creatinine, while automated chemistry analyzers measured calcium, phosphorous, and alkaline phosphatase. Vitamin D levels were analyzed using immunoassay. Participants across all age groups were evenly distributed among the three water type groups. Drinking water type significantly correlated with serum and ionic calcium, magnesium, alkaline phosphatase, and serum phosphate levels. Higher 24-h urine calcium and creatinine were found in the high-fluoride group. Regression analysis showed significant associations between drinking water calcium, magnesium, phosphate, TDS, and serum levels after adjusting for age, gender, socioeconomic status, and dietary intake. (serum calcium = β = 0.006, p < 0.001, serum magnesium = β = 0.002, p < 0.001,serum phosphate = β = − 1.260, p = 0.016). Drinking water type impacts serum calcium, magnesium, phosphate, and alkaline phosphatase levels in children.
Similar content being viewed by others

Introduction
Water is an essential element for the human body. The relationship between water, health, and the ecosystem is very important to avoid the consequences for mankind. The main sources of drinking water come from ground and surface water sources.1,2 Due to the ostensible risks of tap water, the favoured taste, and the convenience, there has been an increase in the consumption of reverse osmosis (RO) water. Traditional methods of water purification like boiling, distillation, and filtration have been replaced by advanced methods such as nanofiltration, ultrafiltration, absorption, ion exchange, chemical and ultraviolet disinfection, and reverse osmosis. RO water purification technology has spread worldwide in recent years3.
Fluoride is ubiquitous in our environment and is the most electronegative and reactive of all elements. Various metal ions, such as magnesium, calcium, and sodium, are important for the proper growth, development, and functioning of the human body as they comprise the material for bones, regulate the water-electrolyte balance, and affect the course of metabolic processes4.
The popularity of RO water has been steadily increasing since it was first introduced as a home water purification system in the 1970s. RO system membranes provide a form of hyper-filtration by restricting the passage of many substances; membrane processes can remove a broad spectrum of minerals. The WHO 1980 report recommended that the minimum total dissolved solids (TDS) in drinking water should be 100 mg/L5.
However, calcium serves multiple crucial physiologic functions beyond bone mineralization. The body employs a sophisticated regulatory system involving various tissues to oversee both bone formation and resorption along with the absorption of calcium in the intestines. This complex regulatory system is necessary to keep serum calcium concentrations within a narrow range3.
Researchers are still uncertain whether fluoride is essential to human health. Many believe that small amounts of fluoride in the diet can help prevent dental caries and strengthen bones. On the other hand, chronic ingestion of high doses of fluoride has a number of adverse effects on human health, including dental fluorosis and skeletal fluorosis, increased bone fractures, decreased birth rates, increased rates of urolithiasis, impaired thyroid function, and lower intelligence in children. Before the endemic fluorosis occurs, early indicators of bone dam age such as serum calcium, magnesium, phosphate, and alkaline phosphatase levels and bone mineral density change. Therefore, it is important to determine the thresholds for these bone indicators to assess early fluoride impact to human health.7 Based on our literature search, there are very limited studies relating to the effects of low mineral content drinking water on young children. So, we hypothesize that there is a difference in bone metabolism indicators like serum and ionic calcium, magnesium, vitamin D, serum phosphate, and alkaline phosphatase levels among 9 to 13-year-old children. Thus, the objective of the present study was to evaluate and compare serum calcium, magnesium, phosphate, alkaline phosphatase, and vitamin D levels in children consuming Reverse Osmosis (RO), non-RO, and high fluoride drinking water.
Method
The present cross sectional study was conducted among children aged 9 to 13 years old. Based on the need and requirements of the study, schools were randomly selected for the selection of the children. In the present study, school children were categorized based on type of drinking water consumed continuously for last 3 years : the first group who drank RO water, the second group non-RO water, and the third group who drank water high in fluoride which has more than 1.5 ppm. In each group 60 samples were selected. The entire study was conducted between March 2022 to October 2023 in and around Mysore district, India.
At the beginning of the study, the source and type of drinking water were noted by enquiring with the school children and their parents. Children were categorized into 3 groups according to the type of drinking water, as mentioned above. Consent from the parents and the assent of the children were taken from participants willing to be part of this study.
Inclusion criteria
-
Those who gave informed consent.
-
Children who drank the same form of water continuously for 3 years.
Exclusion criteria
-
Malnutrition (defined as a weight/height ratio < 5th percentile).
-
Presence of chronic systemic diseases (such as tuberculosis, diabetes, endocrine disorders, primitive and inflammatory bowel diseases).
-
Use of nutritional supplements in medicated form and systemic steroids.
Interview
At the time of recruitment, participants received a questionnaire including socio-demographic information, medical history, sunshine exposure, lifestyle factors, and use of supplements. The questionnaire included a validated food frequency questionnaire (FFQ) to calculate the intake of calcium, magnesium, vitamin D, and fluoride.7 Food frequency questionnaire details were elicited from the children in the presence of their parents. The food frequency questionnaire was designed to assess the frequency of consumption, over the previous month, of foods that are reported as good sources of minerals. After the interview, the body mass index of the children (BMI) was calculated.
Nutrient analysis was performed using the NSR (Nutrition Support Resource) Nutrical 5.1, developed by NSR Nutriedu Tech Solutions (P) Ltd. This tool is designed to improve the efficiency and productivity of dietary calculations and assessments. The software operates within a Google Sheets interface, which allows for easy creation and formatting of spreadsheets for nutrition assessment.
Method
Each ingredient or recipe is entered in the food item column, and a database (IFCT 2017, USDA 2019) is selected for evaluation. The appropriate weight in grams is entered after measuring each ingredient according to the cup size (A, B, C, D, E) indicated by the child while completing the food frequency questionnaire. This data is then cross-checked with the 24-h food intake questionnaire. Macronutrients such as kcal, carbohydrates, protein, and fat are selected from a dropdown menu, while micronutrients like vitamin D, calcium, magnesium, phosphorus, and potassium are also selected from the dropdown.
Each time an ingredient is added and the NSR button is pressed, the tool generates approximate values with their respective denominations. Once all ingredients are added, the total row displays the combined values for each respective column. The rows with the resulting values are then transferred to an Excel sheet for further evaluation.
Before the commencement of the study, ethical approval was obtained from the institutional ethical committee (JSSDCH IEC Research Protocol No: 11/2020 dated 30/04/2020). Informed consent was obtained from all subjects and/or their legal guardian(s) and the study conducted in accordance with the Declaration of Helsinki."
The sampling method
The sample size was calculated based on 95% confidence interval and 80% power and assuming the the mean difference of 1 mg/dl in serum calcium content between non RO water and RO water and the standard deviation of 1.78. The sample size obtained was 50 in each group. To overcome loss to follow up and due to any other reasons the sample size will be increased to 60 in each group. So the total sample size for the present study will be 180 (Hypothesis testing for two means equal variance- N-master sample size calculation software).
Drinking water analysis
Study participants were asked to provide water samples from their homes to determine the mineral content in their drinking water. The calcium, magnesium, phosphorous, fluoride, and TDS (total dissolved solids) levels were measured according to American Public Health Association (APHA) guidelines using standardized instruments.
Collection of blood
For each child, fasting venous blood samples (5 ml) from the Dorsal Hand Vein were collected by trained and experienced para-medical staff, as per protocol. The collected blood samples were transferred to pediatric vacutainer tubes, gently inverted, and labeled with the child’s name, age, medical record number, and date. The collected blood was preserved in clean plastic centrifuge tubes and immediately centrifuged for 10 min at 6000 rpm. Serum was quickly removed to other clean plastic tubes and stored in a refrigerator at − 40 °C until analysis.
24-h urine collection and assessment
To provide a 24-h urine sample, participants had to discard, for example, the 8:00 a.m. urine and then collect all urine samples through 8 o’clock the next morning in a special container provided and deliver it to the lab. After obtaining the sample, calcium, creatinine, and fluoride levels were assessed.
Laboratory investigations
Calcium, phosphorous, and alkaline phosphatase were analysed using a fully automated chemistry analyser, Toshiba TBA120 FR. Vitamin D was analysed using a fully automated immunoassay system, Roche-coba e601. Reproducibility was ensured by adhering to the external quality assessment scheme.
Statistical analysis
All collected data was entered into a Microsoft Excel sheet and analysed using SPSS. Frequencies, percentages, mean, standard deviation. median and interquartile range were used for descriptive statistics. Parametric tests like ANOVA and independent sample t-test were used for data following normal distribution, while the Kruskal–Wallis test and Mann–Whitney test was used for skewed data. Simple linear regression and multivariate regression were used to estimate the association between the type of drinking water consumed and variables such as calcium, magnesium, vitamin D, and alkaline phosphatase in children. A p-value < 0.05 was considered statistically significant. SPSS version 23 was used for statistical analysis.
Results
The mean age of the high fluoride group was 11.35yrs , the non-RO group was 11.20, and the RO group was 10.98. The mean age groups were almost similar and found to be statistically not significant. The participants were equally selected in all the 9 to 13-year-old age groups in the three comparison groups. In the high fluoride group and non-RO group, girls outnumbered boys, while in the RO group, boys were more than girls. Overall, girls were more in number than boys in all the groups, but the comparison was statistically not significant. In terms of socioeconomic status, the majority of the selected sample in the high fluoride and non-RO groups belonged to below the poverty line (BPL), while in the RO group, the majority were above the poverty line (APL). The overall comparison was found to be statistically highly significant (p < 0.001) (Table 1).
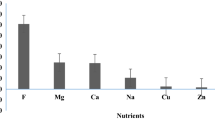
High fluoride drinking water contains higher mean levels of calcium, magnesium, fluoride, and total dissolved solids compared to non-RO and RO drinking water groups. Non-RO drinking water contains higher mean levels of calcium, magnesium, and TDS compared to RO drinking water. RO drinking water represented the least total dissolved solids (13.06units) and other elements. The comparison of all the groups was found to be statistically highly significant (p < 0.001) (Table 2).
RO group children consumed greater percentage of magnesium and phosphate, whereas in high fluoride group children, intake of calcium and vitamin D levels were higher when assessed through the food frequency questionnaire. The comparison of all the values was found to be statistically not significant.
In 24-h urine, calcium showed the highest mean in non-RO water-drinking children, with almost similar values obtained in high fluoride water and RO water-drinking children. The difference obtained was statistically not significant. In 24-h urine, creatinine levels were highest in RO water-drinking children and lowest in high fluoride water-drinking children. The difference obtained was statistically highly significant (p < 0.001). In 24-h urine, the calcium to creatinine ratio was higher in high fluoride water-drinking children, followed by non-RO water, and the least values were observed in RO water-drinking children. The observed difference was statistically highly significant (p < 0.001) (Table 2).
The mean serum calcium was found to be higher in the non-RO group, followed by the high fluoride group. The least mean serum calcium was found in the RO group. The comparison was found to be statistically highly significant (p < 0.001). The mean ionic calcium was found at higher levels in the high fluoride drinking water group, followed by the non-RO drinking group children. The least ionic calcium was recorded in RO drinking water children. Comparison of all the three groups found the value to be statistically highly significant (p < 0.001). The serum magnesium concentration was found to be higher in the high fluoride group, followed by the RO group, with the least concentration found in the non-RO group. The overall comparison was found to be statistically highly significant. In serum alkaline phosphatase, the least concentration was found in the high fluoride group, and the highest concentration was found in the non-RO group. Overall comparison was found to be statistically highly significant (Table 3).
Higher mean vitamin D levels were seen in the high fluoride drinking water group, followed by the non-RO drinking water group, and the least values were found in the RO drinking water group. All three comparisons were found to be statistically not significant. When vitamin D levels were categorized into deficiency (< 20 ng/ml), insufficiency (20–30 ng/ml), and sufficiency (> 30 ng/ml), altogether 83 (46.1%) belonged to the deficiency group and 75 (41.7%) belonged to the insufficiency group. The highest deficiency/insufficiency (90%) was seen in the high fluoride drinking water group, followed by the RO group (88.3%). A higher percentage of vitamin D sufficiency was found in the non-RO drinking water group. More children with deficiency percentage were found in the RO drinking water group (Table 3).
In serum phosphorus, a higher concentration was found in the non-RO group, followed by the high fluoride group, with the least concentration found in the RO group. Comparing all three groups, a statistically highly significant difference was seen. (Table 3).
Simple linear regression analysis and multivariate regression analysis adjusted with covariates are presented in Table 4. In simple and multivariate regression analysis, calcium, magnesium and phosphate present in drinking water and total dissolved solids were significantly associated with serum calcium, magnesium and phosphate after adjusting for variables such as age, gender, socioeconomic status, calcium, magnesium and phosphate in the diet (serum calcium = β = 0.006, p < 0.001, serum magnesium = β = 0.002, p < 0.001, serum phosphate = β = − 1.260, p = 0.016). (Table 4).
Discussion
The aim of this study was to explore whether drinking water mineral content and composition can play a major role in the biochemical constituents such as serum and ionic calcium, vitamin D, magnesium, phosphate, and alkaline phosphatase levels among children aged 9–13.
A study conducted in the Ethiopian Rift Valley found fluoride ion concentrations ranging from 0.65 mg/l to 11 mg/l and TDS concentrations from 284 to 725 mg/l. The study also reported a strong inverse correlation between depth and fluoride and TDS concentrations8.
RO water in the current study exhibited very low levels of calcium, magnesium, phosphorus, fluoride, and TDS, which are insufficient for human needs. As summarized in a 2019 table by Vannucci et al.9 over the past thirty years, numerous publications have explored the effectiveness of mineral water in maintaining adequate calcium intake. Drinking water, which is believed to compensate for mineral deficiencies, can provide a more consistent and stable supply of minerals, including calcium, compared to medicated calcium supplements.10,11 However, ensuring the safety of drinking water requires the use of direct drinking water systems (DDW), the installation of central water purifiers at the beginning of buildings or regional pipe networks, and reverse osmosis (RO) technology, which removes both minerals and contaminants12 and is often used in public places. Consequently, people have increasingly chosen bottled water, often purified water with very low mineral content, over tap water, resulting in a significant reduction in total mineral intake and posing a health risk to human development13.
Calcium is an essential nutrient for supporting growth spurts during childhood and adolescence. Adequate calcium intake during this period is critical for acquiring greater peak bone mass to prevent osteoporosis in later life. Few studies have compared the types of drinking water consumed and serum and ionic calcium levels in children. Previously, Huang et al. conducted a retrospective cohort study in children aged 10 to 13, divided into two groups: normal drinking water and very low mineral water. They concluded that consumption of very low mineral water might be associated with bone resorption activation, bone mineral reduction, and height retardation, attributing these effects to children not achieving recommended calcium intake1.
Calcium homeostasis depends on calcium absorption, excretion, and storage, mainly through hormonal systems such as parathyroid hormone and vitamin D, with dietary intake also affecting serum calcium levels. In the present study, vitamin D levels did not show a significant difference among the three different drinking water groups, likely due to the very low calcium levels in RO drinking water and dietary calcium intake. This likely contributed to the decrease in serum and ionic calcium levels in children from the RO group compared to those from the non-RO and high fluoride drinking water groups.
Children in the RO group, who were above the poverty line (APL), exhibited lower serum and ionic calcium levels despite consuming a good diet rich in dairy products and nutritious foods. In contrast, children in the non-RO and high fluoride drinking water groups, mostly below the poverty line (BPL), showed increased serum and ionic calcium levels likely due to the consumption of mineral-rich drinking water and physical activity. Both APL and BPL children in the present study consumed 500–550 mg/day of calcium through their diet. Simple and multiple regression analyses indicated that calcium in drinking water and total dissolved solids play a major role in serum and ionic calcium levels in children aged 9 to 13.
In this study, children drinking high fluoride water exhibited lower alkaline phosphatase levels compared to those drinking non-RO and RO water. Long-term intake of excessive fluoride has adverse effects on health, including dental fluorosis, changes in bone metabolism indicators, and bone damage in animal studies.14,15,16,17,18,19 Alkaline phosphatase has been considered a marker of osteoblast activity. Fluoride can affect ALP activity by changing the enzyme’s structure or accumulating fluorine in bones to promote bone cell mitosis. The decrease in ALP levels in serum may result from fluoride interaction and enzyme structure changes. Higher ALP levels were observed in children drinking non-RO water, likely due to its higher mineral content, especially calcium and magnesium ions, stimulating bone metabolism and ALP regulation. Overall, higher mineral concentration in non-RO drinking water may enhance serum alkaline phosphatase levels20.
In this study, significant differences in serum magnesium levels were observed among the three different drinking water groups, with children drinking high fluoride water exhibiting higher magnesium levels compared to those drinking non-RO and RO water. However, the reason for this elevation in high fluoride water is unclear, warranting further molecular research and long-term studies. Previous studies have shown that supplying mineral-rich water increased serum magnesium and calcium levels and reduced hypertension. Additionally, recent meta-analyses have suggested that magnesium in drinking water may reduce the risk of coronary heart disease21,22.
The results also showed higher magnesium levels in the RO group compared to the non-RO group. Most children in the non-RO group belonged to the BPL group, while those in the RO group belonged to the APL group, with dietary practices and intake varying between the two groups. Low socioeconomic status children may have protein deficiency in their diet, which can affect magnesium uptake. Factors such as age and other food components in a meal can influence magnesium absorption. Higher protein and albumin intake can increase magnesium absorption. These factors may have contributed to the decreased serum magnesium levels in children from the non-RO group compared to those from the RO group.
RO drinking water children also exhibited a higher percentage of vitamin D deficiency/insufficiency compared to non-RO drinking water children. This may be due to lesser calcium and vitamin D supply through diet and drinking water, and decreased sunlight exposure, particularly in urban areas with higher air pollution23,24,25.
Children drinking high fluoride water exhibited slightly lower phosphate levels compared to those drinking non-RO water. This may be attributed to high phosphorous concentration in high fluoride water and its association with PTH and vitamin D, which may decrease serum phosphate levels compared to non-RO group children. Seasonal fluctuations were observed in some studies, though not recorded in the present study26,27.
The overall mean of calcium and creatinine ratio of the three groups was 0.16. RO drinking water children exhibited lower serum calcium and creatinine ratios compared to high fluoride drinking water children, with the highest ratios found in the latter group. Wide fluctuations were observed, likely due to several factors, including daily dietary calcium intake, serum 25OHD levels, serum magnesium, dietary magnesium, and phosphate levels, and intake through water28,29,30.
The strength of this study lies in the fact that, based on the literature review, it is the first of its kind to explore the association between bone metabolism markers, and different types of drinking water (Non-RO, RO, and high fluoride water) consumed by children. This study uniquely includes high fluoride drinking water among children and adolescents aged 9 to 13 years, and the selected indicators have the added advantage of being feasible for testing within community settings.
Study limitations
This cross-sectional study does not allow for the determination of causal influences of drinking water type on bone metabolism indicators like serum calcium, magnesium, vitamin D, and phosphate, nor can cause and effect relationships be assessed. However, children were recruited from government and private schools, as well as urban and rural locations, making the data representative of a wider range of social status, cultures, and dietary practices. Limitations include the reliance on parental/children reports for duration of drinking water type, physical activity, and food frequency questionnaire, which are subject to recall bias.
Conclusion
Nevertheless, the data highlights a strong association between drinking water mineral content and serum levels of calcium, magnesium, and phosphate. Children consuming high fluoride water had better mineral profiles, whereas those consuming RO water exhibited deficiencies, despite adequate nutrition, underscoring the importance of mineral-rich drinking water for optimal growth and bone health in children.
Data availability
Data cannot be shared openly to protect study participants privacy. Data described in the manuscript, code book, and analytic code will be available with the first author ( Dr.Thippeswamy HM) and will be provided upon request, pending agreement.
References
Pampaloni, B. & Brandi, M. L. Mineral water as food for bone: An overview. Int. J. Bone Frag. 2, 48–55. https://doi.org/10.57582/IJBF.220202.048 (2022).
Saini, R. D. Health risks from long term consumption of reverse osmosis water. Int. J. Appl. Chem. 13(2), 293–301 (2017).
Kamalapriya, V., Mani, R., Venkatesh, V., Kunhikannan, S. & Ganesh, V. S. The role of low mineral water consumption in reducing the mineral density of bones and teeth: A narrative review. Cureus 15(11), e49119. https://doi.org/10.7759/cureus.49119 (2023).
AlNouri, D. M. The concentration of selected ions in bottled, commercial zamzam, and household water in Riyadh city and its effect on bone mineral content in growing rabbits. Progr. Nutr. 21(2), 458–466 (2019).
Singh, D. & Mulla, S. Chemical analysis of drinking water to compare reverse osmosis processed and unprocessed water quality. Environ. Dis. 5(3), 72–77. https://doi.org/10.4103/ed.ed_21_20 (2020).
Chen, S. et al. Change of urinary fluoride and bone metabolism indicators in the endemic fluorosis areas of southern china after supplying low fluoride public water. BMC Public Health 13, 156. https://doi.org/10.1186/1471-2458-13-156 (2013).
Rathi, R. S. et al. Development and validation of a food frequency questionnaire for assessing dietary intake in the Indian population. Public Health Nutr. 23(10), 1795–1803 (2020).
Abdurahman, S. G. & Zewdie, M. Fluoride ion and total dissolved solid distribution in Ethiopian Rift valley: The case of Hawassa city aquifer. J. Hydrol.: Reg. Stud. 19, 240–249 (2018).
Vannucci, L. et al. Calcium intake in bone health: a focus on calcium-rich mineral waters. Nutrients 10(12), 1930 (2018).
Vitoria, I. et al. The calcium concentration of public drinking waters and bottled mineral waters in Spain and its contribution to satisfying nutritional needs. Nutr. Hosp. 30(1), 188–199 (2014).
Pop, M. S. et al. Exploring the potential benefits of natural calcium-rich mineral waters for health and wellness: A systematic review. Nutrients 15(14), 3126 (2023).
Huang, Y. et al. A survey on the mineral contents and potential renal acid loads in primary and secondary school-supplied drinking water in Chongqing (Chinese Edition). Chin. J. Prev. Med 49(10), 930–932 (2015).
Huang, Y. et al. Consumption of very low mineral water is associated with lower bone mineral content in children. J. Nutr. 149(11), 1994–2000. https://doi.org/10.1093/jn/nxz161 (2019).
Chen, S. et al. Change of urinary fluoride and bone metabolism indicators in the endemic fluorosis areas of southern China after supplying low fluoride public water. BMC Public Health 20(13), 156. https://doi.org/10.1186/1471-2458-13-156 (2013).
Błaszczyk, I., Birkner, E., Gutowska, I., Romuk, E. & Chlubek, D. Influence of methionine and vitamin e on fluoride concentration in bones and teeth of rats exposed to sodium fluoride in drinking water. Biol. Trace Elem. Res. 146(3), 335–339 (2012).
Wu, C. X., Gu, X. L., Ge, Y. M., Zhang, J. H. & Wang, J. D. Effects of high fluoride and arsenic on brain biochemical indexes and learning-memory in rats. Fluoride 39, 274–279 (2006).
Zhang, J. H., Liang, C., Ma, J. J., Zhou, B. H. & Wang, J. D. Changes in testis protein and metabolic enzyme activities in rats induced by sodium fluoride and sulfur dioxide. Fluoride 39, 179–184 (2006).
Zhan, X. A., Wang, M., Xu, Z. R., Li, W. F. & Li, J. X. Toxic effects of fluoride on kidney function and histological structure in young pigs. Fluoride 39, 22–26 (2006).
Zhan, X. A., Wang, M., Xu, Z. R., Li, W. F. & Li, J. X. Evaluation of caspase-dependent apoptosis during fluoride-induced liver lesion in pigs. Arch. Toxicol. 80, 74–80 (2006).
Zhang, Y. et al. Evaluation of the effect of reducing fluoride concentration in drinking water on dental fluorosis prevalence in a Chinese population. Environ. Health Perspect. 128(6), 067004 (2020).
Quattrini, S., Pampaloni, B. & Brandi, M. L. Natural mineral waters: chemical characteristics and health effects. Clin. Cases Miner. Bone Metab. 13(3), 173–180. https://doi.org/10.11138/ccmbm/2016.13.3.173 (2016).
Jiang, L. et al. Magnesium levels in drinking water and coronary heart disease mortality risk: A meta-analysis. Nutrients 8(1), 1–5 (2016).
Khadilkar, A. et al. Vitamin D status and determinants in Indian children and adolescents: A multicentre study. Sci. Rep. 12, 16790. https://doi.org/10.1038/s41598-022-21279-0 (2022).
Marwaha, R. K. et al. Vitamin D and bone mineral density status of healthy schoolchildren in northern India. Am. J. Clin. Nutr. 82(2), 477–482. https://doi.org/10.1093/ajcn.82.2.477 (2005).
Thippeswamy, H. M., Devananda, D., Nanditha Kumar, M., Wormald, M. M. & Prashanth, S. N. The association of fluoride in drinking water with serum calcium, vitamin D and parathyroid hormone in pregnant women and newborn infants. Eur. J. Clin. Nutr. 75(1), 151–159. https://doi.org/10.1038/s41430-020-00707-2 (2021).
Barbier, O., Arreola-Mendoza, L. & Razo, L. M. D. Molecular mechanisms of fluoride toxicity. Chem.-Biol. Interact. 188, 319–333 (2010).
Bailey, D. A., McKay, H. A., Mirwald, R. L., Crocker, P. R. & Faulkner, R. A. A six-year longitudinal study of the relationship of physical activity to bone mineral accrual in growing children: the university of Saskatchewan bone mineral accrual study. J Bone Miner Res. 14, 1672–1679 (1999).
Pekkinen, M., Viljakainen, H., Saarnio, E., Lamberg-Allardt, C. & Mäkitie, O. Vitamin D is a major determinant of bone mineral density at school age. PLoS One 7(7), e40090. https://doi.org/10.1371/journal.pone.0040090 (2012).
Grobler, S. R., Louw, A. J., Chikte, U. M. E., Rossouw, R. J. & Kotze, V. W. The relationships between two different drinking water fluoride levels, dental fluorosis and bone mineral density of children. Open Dent. J. 3, 48–54. https://doi.org/10.2174/1874210600903010048 (2009).
Zhang, Y. et al. Fluoride exposure and bone health: A systematic review and meta-analysis. Environ. Health Perspect. 128(6), 067004 (2020).
Funding
This research was funded by Indian Council of Medical Research(ICMR), India.
Author information
Authors and Affiliations
Contributions
T.H.M. -Project conception, development of overall research plan, and study oversight. R.S. - study oversight and data collection. N.K.M. - primary responsibility for final content, Wrote paper. P.S.N. - hands-on primary responsible for the final content. S.P. - hands-on conduct of the experiments and data collection.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Thippeswamy , H.M., Shanbhog, R., Kumar, M.N. et al. Comparison of serum calcium, magnesium, phosphate, alkaline phosphatase, and vitamin D levels in children consuming reverse osmosis, non reverse osmosis, and high fluoride drinking water. Sci Rep 15, 10689 (2025). https://doi.org/10.1038/s41598-025-94758-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-94758-9
