
Abstract
Primary hypertension is the most common type of hypertension, with a complex and not fully understood pathogenesis. Insulin resistance (IR) is a metabolic abnormality that has been shown to be quite prevalent among patients with hypertension in existing literature. The triglyceride-glucose (TyG) index is a reliable indicator for assessing insulin resistance (IR). This study aims to evaluate the relationship between the TyG index at admission and all-cause mortality (ACM) in patients with severe primary hypertension, and to explore its role in predicting the future all-cause mortality risk in primary hypertension patients. This study employs a retrospective design to categorize all patients into four quartiles based on the TyG index. The Kaplan–Meier (K-M) method was utilized to estimate the survival curves for each group and to compare the survival outcomes across different quartiles. To assess the nonlinear relationship between the TyG index and prognosis, Cox proportional hazards regression models and restricted cubic splines (RCS) were applied, adjusting for potential confounders. Additionally, subgroup analyses were performed to conduct stratified analyses and interaction tests. Kaplan–Meier survival curve analysis showed that patients with higher TyG index levels had higher all-cause mortality rates at 30 days, 60 days, and 90 days post-admission. This indicates that a higher TyG index is associated with an increased risk of death in the short term. Additionally, multivariate Cox proportional hazards regression analysis revealed that an increased TyG index was significantly associated with all-cause mortality at 30 days, 60 days, and 90 days. Meanwhile, RCS analysis indicates that as the TyG index level increases, the hazard ratio (HR) shows a significant upward trend, suggesting a gradual increase in the risk of all-cause mortality. In summary, among patients with primary hypertension in the intensive care unit, elevated TyG levels are associated with an increased risk of short-term mortality.
Similar content being viewed by others

Introduction
Hypertension is one of the most common and highly fatal chronic diseases worldwide. In recent years, with population aging and lifestyle changes, the incidence of hypertension has been steadily rising, making it a significant challenge in global public health1. Studies have shown that hypertension not only substantially increases the risk of cardiovascular events but is also closely linked to all-cause mortality. Particularly among younger populations, uncontrolled hypertension can lead to cardiovascular and systemic damage, thereby elevating all-cause mortality2. On September 19, 2023, the World Health Organization (WHO) released its first "Global Hypertension Report," indicating that nearly half of hypertensive patients are unaware of their condition, and about 80% have not received adequate treatment. If the global hypertension control rate were increased to 50%, 76 million deaths could be avoided between 2023 and 2050. Additionally, hypertensive patients in the Intensive Care Unit (ICU) often present with complex and variable conditions, frequently accompanied by multiple comorbidities3. Therefore, predicting the mortality of these patients is crucial for formulating effective treatment plans.
Insulin resistance (IR) is a metabolic condition characterized by reduced insulin effectiveness in target tissues. Early experiments have demonstrated that hyperinsulinemia and insulin resistance are prevalent among hypertensive patients4,5. Research indicates that insulin resistance is closely associated with vasoconstriction induced by systemic inflammation and oxidative stress, making it a significant risk factor for microvascular diseases6,7,8. The HOMA-IR index is currently the gold standard for assessing insulin resistance; however, its complexity and high cost limit its widespread clinical use9. In recent years, the triglyceride-glucose (TyG) index has gained attention as a simple alternative biomarker for insulin resistance. The TyG index, based on serum triglyceride and fasting blood glucose levels, is easy to measure and readily accessible in clinical settings10,11. Several studies have shown that the TyG index is closely related to the prognosis of cardiovascular diseases, including coronary artery disease, heart failure, myocardial infarction, stroke, and hypertension5. The TyG index is considered one of the effective tools for predicting cardiovascular risk. Although the application of the TyG index in predicting cardiovascular diseases has made some progress, research on the relationship between the TyG index and all-cause mortality in hypertensive patients in the ICU remains scarce. Given the complexity and high mortality of hypertensive patients in the ICU, this study will utilize the MIMIC-IV database to analyze the relationship between the TyG index and all-cause mortality in critically ill hypertensive patients. This study aims to explore the potential application of the TyG index in predicting all-cause mortality in hypertensive patients in the ICU, providing new perspectives and valuable predictive tools for clinical practice. The goal is to enable early identification of high-risk patients and implement appropriate interventions, thereby reducing ICU mortality and improving overall treatment outcomes.
Materials and methods
Data source
The study employs a retrospective analysis method to evaluate the association between the TyG index and all-cause mortality in hypertensive patients in the ICU. By collecting and analyzing historical data, retrospective analysis offers extensive insights and is instrumental in identifying key clinical correlations. The data for this study were sourced from a large public critical care database—Medical Information Mart for Intensive Care IV (MIMIC-IV, version 2.2). The MIMIC-IV database was developed in collaboration between the Massachusetts Institute of Technology (MIT) Computer Science and Artificial Intelligence Laboratory (CSAIL) and the Beth Israel Deaconess Medical Center (BIDMC) in Boston. The database includes detailed clinical data from over 190,000 patients and 450,000 hospital admissions between 2008 and 2019. This database provides a rich resource of clinical data for researchers worldwide and is widely used in critical care medicine. The MIMIC-IV database encompasses comprehensive patient information, including but not limited to demographic data (such as age, gender, race), laboratory test results (such as blood glucose, lipids, liver, and kidney function), medication usage (such as antihypertensive drugs, antibiotics), vital signs (such as blood pressure, heart rate, temperature), surgical information, disease diagnoses, medication management, and follow-up survival status. These data provide researchers with a solid foundation for in-depth analysis of patient conditions and disease progression trends, particularly suited for studying the multifactorial impact of complex diseases. To ensure ethical and legal compliance in data usage, researchers must complete a training course on the protection of human research participants provided by the National Institutes of Health (NIH) and pass the Collaborative Institutional Training Initiative (CITI) program test before accessing the MIMIC-IV database. All patient information in the database is anonymized, containing no protected personal information, and therefore, informed consent from patients is not required for this study. This data access protocol ensures compliance with ethical standards while safeguarding patient privacy.
Study design and population
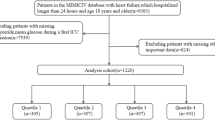
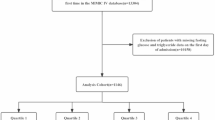
Patients who were hospitalized for the first time, stayed in the ICU for more than 3 h, and were over 18 years of age, were included in this study. A total of 50,769 patients were enrolled. The study further included a total of 28,742 patients with primary hypertension. Hypertensive patients in the study were classified and diagnosed using the International Classification of Diseases, Ninth Revision (ICD-9), and Tenth Revision (ICD-10) codes. The ICD-9 codes for hypertension in this study include 4010 for malignant essential hypertension, 4011 for benign essential hypertension, and 4019 for unspecified essential hypertension. The ICD-10 code for hypertension is I10 for primary hypertension. The exclusion criteria were as follows: (1) missing data (triglycerides, glucose); (2) patients with malignant tumors, severe liver disease, or AIDS. The final study cohort included 3,859 patients, who were divided into four groups based on the quartiles of their TyG index (Fig. 1).

Flowchart of the selection of patients.
Data extraction
Data extraction was performed using Navicat Premium 16 and PostgreSQL software (version 13.7.2), applying Structured Query Language (SQL) to retrieve ICU data, including demographic information (age, gender, and ethnic background); laboratory data (triglycerides [Tg], bicarbonate, chloride, sodium, creatinine, glucose, potassium, hemoglobin concentration [Hb], platelet count [PLT], red blood cell count [RBC], high-density lipoprotein [HDL], low-density lipoprotein [LDL], partial pressure of carbon dioxide [Pco2], partial pressure of oxygen [Po2]); vital signs data (Systolic Blood Pressure [SBP], Diastolic Blood Pressure[DBP]); existing comorbidities (primary hypertension, myocardial infarction [MI], congestive heart failure [CHF], peripheral vascular disease [PVD], cerebrovascular disease [CVD], dementia, chronic obstructive pulmonary disease [COPD], peptic ulcer disease [PUD], mild liver disease, paraplegia, metastatic solid tumor [MST], malignant neoplasm [MC], systemic inflammatory response syndrome [SIRS], Sequential Organ Failure Assessment [SOFA] score, Simplified Acute Physiology Score II [SAP II], and SAP II-PROB). The TyG was calculated as follows: Ln [(TG (mg/dL) × FBG (mg/dL)]/2. The values and scores were collected within 24 h before and after ICU admission. To mitigate the impact of missing data, variables with more than 20% missing data were excluded, and those with less than 20% missing data were imputed using the median.
Each subject’s observation period spanned from ICU admission to outcome events, including ICU mortality, hospital mortality, 30-day mortality, 60-day mortality, 90-day mortality, 1-year mortality, 5-year mortality, and 10-year mortality.
Statistical analysis
During data processing, all continuous variables were first subjected to a normality test to determine the type of data distribution. For continuous variables that followed a normal distribution, statistical analyses were performed using Student’s t-test and one-way analysis of variance (ANOVA), with results expressed as mean ± standard deviation (SD) to ensure accuracy and comparability. For continuous variables that did not follow a normal distribution, the Wilcoxon rank-sum test was used for analysis, and results were expressed as median and interquartile range (IQR) to accommodate the distribution characteristics of the data. For categorical variables, chi-square tests or Fisher’s exact tests were employed, with results expressed as absolute percentages to accurately assess the differences between groups.
To gain a deeper understanding of the relationship between the TyG index and patient outcomes, stratified analyses were conducted according to different levels of the TyG index. Kaplan–Meier (K-M) survival curves were used to evaluate the incidence of primary and secondary outcomes. This method estimates survival probabilities at different time points, visually displaying the survival status of different TyG index groups, which helps identify high-risk patient populations.
In the survival analysis, univariate Cox proportional hazards models were used to explore the relationship between the TyG index and mortality at different time points (including 30 days, 60 days, and 90 days). To control for potential confounders, multivariate Cox proportional hazards regression models were further employed, incorporating clinically relevant variables or those significantly associated with outcomes in univariate analysis. The variables included in the final model were carefully selected to ensure the reliability of the analysis results while avoiding overfitting. Through multilayered data processing and rigorous survival analysis, this study comprehensively evaluated the relationship between the TyG index and long-term mortality in hypertensive patients in the ICU, providing a robust statistical basis for assessing the impact of the TyG index on patients’ long-term prognosis.
Model 1 included only the TyG index, while Model 2 was adjusted for age, gender, and race. The fully adjusted Model 3 was controlled for age12, gender13, race14, PLT15, creatinine16, and SBP. These variables have been extensively studied and are directly or indirectly related to the pathogenesis of hypertension. Model 3 also includes comorbidities such as MI, CVD, dementia, COPD, MLD, and paraplegia. Additionally, we used the Schoenfeld residuals method to test the proportional hazards assumption for all variables included in Model 3 across different time points (30 days, 60 days, and 90 days). The results of the Schoenfeld residuals analysis are shown in Table S1. This method examines whether the residuals of each covariate change over time; a significant relationship (P < 0.05) indicates a violation of the proportional hazards assumption. In such cases, variables that violate the assumption are treated as time-dependent variables, modeling the covariates influence on risk as time-varying. This effectively controls confounding factors and enhances the model’s explanatory power for hypertension-related risks.
In all three models, the lowest quartile of the TyG index was used as a reference. The TyG index was also analyzed as a continuous variable using restricted cubic splines (RCS) to elucidate the dose–response relationship with the risk of primary and secondary outcome events. Additionally, stratified analyses were conducted by gender, age (< 65 years or ≥ 65 years), ethnicity/race (Asian, Black, White, others), MI, CVD, dementia, COPD, mild liver disease, and paraplegia. All statistical analyses were performed using R software (version 4.4.1, R Foundation for Statistical Computing, Austria), with P < 0.05 considered statistically significant.
Results
Baseline characteristics
This study included 50,769 patients who were admitted to the ICU for more than 3 h and were over 18 years of age from the MIMIC-IV database. Of these, 3859 hypertensive patients met the inclusion criteria and were analyzed. Table 1 lists the baseline demographic and clinical attributes stratified by the TyG quartiles. The average age of patients enrolled in this study was 69 ± 11 years, with 54.7% being male. Among them, 63.5% were White, 2.6% were Asian, 10.0% were Black, and 23.9% belonged to other ethnic groups. The baseline characteristics of the study participants were analyzed according to the TyG index quartiles at the time of admission and are presented in Table 1. The TyG index quartiles were 6.550–8.580, 8.580–9.020, 9.020–9.570, and 9.570–13.690. Subjects in the highest TyG index group were younger and had higher prevalence rates of MI, COPD, and mild liver disease, with lower prevalence rates of CVD, dementia, and paraplegia. They also had lower levels of bicarbonate and higher levels of creatinine, glucose, potassium, platelet count, and white blood cells. Additionally, the all-cause mortality rates at 30 days (12.0% vs. 11.8% vs. 11.1% vs. 16.3%, P = 0.003), at 60 days (14.8% vs. 14.2% vs. 13.6% vs. 18.7%, P = 0.009), at 90 days (16.7% vs. 15.0% vs. 15.3% vs. 20.3%, P = 0.007), at 1 year (22.6% vs. 20.2% vs. 21.5% vs. 24.4%, P = 0.152), at 5 years (27.8% vs. 24.9% vs. 26.0% vs. 28.6%, P = 0.225), and at 10 years (29.6% vs. 26.3% vs. 27.5% vs. 30.5%, P = 0.153) were higher in the Q4 group compared to the other three groups, although the differences among Q2, Q3, and Q4 were not statistically significant.
Survival analysis
Kaplan–Meier curves indicated statistically significant differences in 30-day, 60-day, and 90-day mortality across the four TyG index quartiles, as depicted in Fig. 2. Patients with the highest TyG index had the highest all-cause mortality at 30 days, 60 days, and 90 days (30-day log-rank P = 0.003, 60-day log-rank P = 0.008, 90-day log-rank P = 0.006), while no significant differences were observed in 1-year, 5-year, and 10-year mortality (Figure S2).

Kaplan–Meier survival analysis curves for (A) 30 days, (B) 60 days, and (C) 90 days ACM. ACM, all-cause mortality.
TyG and outcomes
To investigate the independent impact of the TyG index on mortality, three Cox proportional hazards models were used to assess the relationship between TyG and all-cause mortality (ACM) at different time points (30 days, 60 days, and 90 days). As shown in Table 2, when analyzing TyG as a continuous variable, the adjusted hazard ratios (HRs) and 95% confidence intervals (CIs) for 30-day all-cause mortality in the initial adjustment Model 1 and the comprehensive adjustment Model 2 were (HR: 1.13, 95% CI 1.02–1.26, P-value: = 0.018; HR: 1.47, 95% CI 1.32–1.64, P-value: < 0.001); for 60-day all-cause mortality, they were (HR: 1.11, 95% CI 1.01–1.22, P-value: = 0.032; HR: 1.47, 95% CI 1.33–1.63, P-value: < 0.001); and for 90-day all-cause mortality, they were (HR: 1.10, 95% CI 1.00–1.21, P-value: = 0.042; HR: 1.45, 95% CI 1.32–1.60, P-value: < 0.001). When the TyG index was categorized from lowest to highest as an ordinal variable (Q1: 6.550–8.580, Q2: 8.580–9.020, Q3: 9.020–9.570, Q4: 9.570–13.690), the risk of 30-day, 60-day, and 90-day ACM significantly increased in the highest quartile in the Cox proportional hazards models: in the initial adjustment Model 2, the adjusted HRs and 95% CIs for all-cause mortality were (HR: 2.24, 95% CI 1.74–2.89, P-value: < 0.001; HR: 2.17, 95% CI 1.73–2.74, P-value: < 0.001; HR: 2.09, 95% CI 1.68–2.61, P-value: < 0.001). In the fully adjusted Model 3, hazard ratios (HRs) and 95% confidence intervals (CIs) were (HR: 3.30, 95% CI 1.84–5.90, P-value: < 0.001; HR: 2.94, 95% CI 1.72–5.02, P-value: < 0.001; HR: 2.53, 95% CI 1.55–4.14, P-value: < 0.001).
Nonlinear relationship detection
Restricted cubic splines (RCS) were applied to Model 3 with full multivariable adjustment to detect nonlinear relationships between the TyG index and 30-day, 60-day, and 90-day all-cause mortality. We found that the TyG index has a monotonically increasing relationship with 30-day, 60-day, and 90-day all-cause mortality. (P for nonlinearity = 0.5142, P for nonlinearity = 0.3935, P for nonlinearity = 0.1978), However, in the Restricted cubic spline curve for 90 days, when TyG < 8.236203, the HR shows a slight decline but generally remains stable, as illustrated in Fig. 3. When the TyG was 9.026, the HR was 1.003. The mortality risk increased non-linearly as the TyG index exceeded 9.04. In the range of 9.570 to 13.690, for every unit increase, the 30-day, 60-day, and 90-day mortality risks increased by 230%, 194%, and 153%, respectively (HR: 3.30 95% CI 1.84–5.90, P-value: < 0.001; HR: 2.94, 95% CI 1.72–5.02, P-value: < 0.001; HR: 2.53, 95% CI 1.55–4.14, P-value: < 0.001). Moreover, RCS regression analysis indicated a nonlinear increase at 1, 5 and 10 years mortality risk with rising TyG values (non-linear P = 0.2720, non-linear P = 0.1763, non-linear P = 0.2137, respectively; Figure S3).

Restricted cubic spline curve for (A) 30 days, (B) 60 days, and (C) 90 days, ACM. HR, hazard ratio; CI, confidence interval; TyG index, triglyceride-glucose index; ACM, all-cause mortality.
Subgroup analysis
To further investigate whether the relationship between the TyG index and 30-day, 60-day, and 90-day all-cause mortality persisted under different conditions, subgroup analyses were performed based on gender, age (< 65 years or ≥ 65 years), ethnicity/race (Asian, Black, White, others), MI, CVD, dementia, COPD, MLD, and paraplegia.
TyG is an important predictor of increased 30-day mortality risk within subgroups, particularly in individuals under 65 years old and those aged 65 and older (HR: 1.26, 95% CI 1.11–1.44; HR: 1.41, 95% CI 1.17–1.69), individuals with myocardial infarction (MI) (HR: 1.48, 95% CI 1.21–1.82), individuals with and without cardiovascular disease (CVD) (HR: 1.24, 95% CI 1.05–1.45; HR: 1.18, 95% CI 1.02–1.36), individuals with dementia (HR: 1.16, 95% CI 1.04–1.29), individuals without chronic obstructive pulmonary disease (COPD) (HR: 1.29, 95% CI 1.06–1.56), individuals without mild liver disease (MLD) (HR: 1.15, 95% CI 1.02–1.29), and individuals without paraplegia (HR: 1.21, 95% CI 1.08–1.36; Fig. 4A).

Forest plots of stratified analyses of TyG index for (A) 30-days, (B) 60-days, (C) 90-days all-cause mortality. MI, myocardial infarction; CVD, cardiovascular disease; COPD, chronic obstructive pulmonary disease.
Similarly, for 60-day mortality, a significant association with TyG was observed in individuals under 65 years old and those aged 65 and older (HR: 1.25, 95% CI 1.11–1.41; HR: 1.40, 95% CI 1.18–1.66), individuals with MI (HR: 1.41, 95% CI 1.17–1.70), individuals with and without CVD (HR: 1.20, 95% CI 1.03–1.39; HR: 1.15, 95% CI 1.01–1.31), individuals with dementia (HR: 1.13, 95% CI 1.02–1.25), individuals without COPD (HR: 1.28, 95% CI 1.08–1.52), individuals without MLD (HR: 1.14, 95% CI 1.02–1.26), and individuals without paraplegia (HR: 1.13, 95% CI 1.02–1.26; Fig. 4B). Notably, a significant association was also observed in male individuals (HR: 1.15, 95% CI 1.01–1.32; Fig. 4B).
For 90-day mortality, a significant association with TyG was observed in individuals under 65 years old and those aged 65 and older (HR: 1.24, 95% CI 1.10–1.39; HR: 1.37, 95% CI 1.16–1.61), individuals with MI (HR: 1.34, 95% CI 1.12–1.60), individuals with CVD (HR: 1.20, 95% CI 1.04–1.39), individuals with dementia (HR: 1.12, 95% CI 1.02–1.24), individuals without COPD (HR: 1.21, 95% CI 1.02–1.43), individuals without MLD (HR: 1.13, 95% CI 1.02–1.24), and individuals without paraplegia (HR: 1.14, 95% CI 1.03–1.27; Fig. 4C).
Discussion
In this study, we preliminarily explored the correlation between TyG levels and all-cause mortality in critically ill patients with primary hypertension from a large public ICU database cohort. The study revealed a J-shaped nonlinear relationship between the TyG index and 30-day, 60-day, and 90-day all-cause mortality in patients with primary hypertension in the ICU. This indicates that when the TyG index is elevated, the risk of mortality significantly increases. Even after adjusting for potential confounding factors, the TyG index remained closely associated with short-term all-cause mortality (ACM), highlighting its importance in evaluating the short-term prognosis of patients with primary hypertension within a specific range. The findings suggest that the TyG index can serve as a valuable tool for clinical decision-making and as an independent risk factor for critically ill patients with primary hypertension. By incorporating the TyG index into clinical decisions, physicians can better identify high-risk patients and develop more precise interventions to reduce mortality in these patients. Moreover, the use of the TyG index can provide new guidance for the formulation of clinical guidelines, particularly in the ICU setting, to direct the treatment and management of critically ill hypertensive patients.
Insulin resistance (IR) is a key factor in the pathogenesis of hypertension. IR induces vasoconstriction by enhancing tissue angiotensin II (AngII) and aldosterone activity17, increasing sympathetic nervous system activity, and promoting oxidative stress18,19, leading to elevated blood pressure and associated target organ damage. This includes damage via membrane ion exchange, inhibition of atrial natriuretic peptide activity, sodium retention, and plasma volume expansion, resulting in chronic kidney disease, left ventricular hypertrophy, and atherosclerosis. These damages further exacerbate the condition of hypertensive patients, significantly increasing their mortality risk. Furthermore, research indicates that the TyG index, as a surrogate marker for IR, plays a crucial role in managing hypertensive patients. Existing studies have demonstrated the significant role of the TyG index in assessing cardiovascular and cerebrovascular disease risks. Previous research has extensively explored the relationship between IR surrogates and hypertension outcomes. For example, XinMing Huang and colleagues studied the relationship between TyG-BMI and hypertension in Japanese normoglycemic subjects19. Yahui Liu et al. investigated the use of the TyG index in predicting adverse cardiovascular outcomes in coronary heart disease patients with hypertension20. Veronica Maria Tagi et al. examined the mechanisms and treatment of hypertension in children with insulin resistance, indicating that IR contributes to the development of hypertension and atherosclerotic cardiovascular disease17. However, research specifically focused on primary hypertensive patients in the ICU is still limited. This study addresses this gap by systematically evaluating the relationship between the TyG index and mortality in critically ill hypertensive patients, confirming that a high TyG index is a significant independent predictor of increased mortality risk, providing a new perspective for risk assessment in ICU patients.
The hyper insulinemic-euglycemic clamp (HEC) is the most accurate method for diagnosing insulin resistance, but due to its complexity, high cost, time consumption, and reproducibility challenges, it is rarely used extensively in clinical practice21. Currently, the Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) and the TyG index are widely considered simple surrogate biomarkers for IR10. The TyG index is a composite measurement derived from TG and FBG levels and has been recognized as a feasible biomarker for metabolic syndrome, atherosclerosis, and cardiovascular pathology21. In certain cases, the TyG index outperforms the individual measurement of glucose or TG, making it a reliable indicator of the cardiovascular disease spectrum and other disorders associated with metabolic dysfunction22.
The required indicators for the TyG index are easily obtainable in clinical settings and can be widely applied, making it a common tool in clinical research for assessing IR in high-risk individuals. Our further studies demonstrate the predictive value of the TyG index for outcomes in ICU patients with primary hypertension, particularly in the short term, where the TyG index’s role as a prognostic marker is especially pronounced. This provides new guidance for clinicians in managing and making decisions for patients. Additionally, our research emphasizes the importance of the TyG index as a comprehensive marker for risk stratification, offering a detailed tool for accurately describing high-risk individuals. While there are few studies confirming the relationship between the TyG index and long-term outcomes in ICU patients with primary hypertension, and it is uncertain whether short-term results can predict long-term outcomes, the predictive power of the TyG index for long-term mortality in critically ill primary hypertensive individuals should not be overlooked.
This study employed a cohort study design to ensure systematic follow-up of the study subjects and accurate data collection. To mitigate the potential impact of imbalance and confounding bias on the results, multivariate Cox regression analysis was used. This method allows for the simultaneous inclusion of multiple relevant variables in the model, enhancing the robustness of the study’s findings. Through rigorous statistical analysis, the study was able to more precisely assess the association between the TyG index and patient mortality.
The main strength of this study lies in the fact that while existing research has shown the TyG index to be crucial in assessing the risk of cardiovascular and cerebrovascular diseases, studies focusing on primary hypertensive patients, especially in critical care settings, remain limited. This study is the first to systematically evaluate the relationship between the TyG index and short-term all-cause mortality in ICU patients with primary hypertension, demonstrating the clinical value of the TyG index as an independent risk predictor. This provides clinicians with a new decision-making tool, helping to identify high-risk patients early and take appropriate interventions. Furthermore, the results of this study also point to directions for future research, particularly in exploring the application value of the TyG index in different hypertensive patient populations and its interaction with other clinical indicators. However, this study also has some limitations that cannot be ignored. Firstly, as a retrospective study, its conclusions are constrained by data availability and quality. For example, since the data are derived from previous records, there is the possibility of residual confounding factors that may not have been fully controlled, and thus the residual confounding effects cannot be entirely excluded. Despite the use of multivariate adjustments and subgroup analyses, the possibility of residual confounding remains. For instance, certain variables that could influence mortality and specific causes of death were not included in the study. Secondly, this study only assessed the TyG index at baseline and did not track its dynamic changes during the patient’s hospitalization. This limitation might affect the comprehensive understanding of the relationship between the TyG index and mortality. The impact of changes in the TyG index over time on patient prognosis still requires further investigation. Moreover, converting the TyG index into categorical variables and conducting segmented stratified analyses, while providing more detailed results, may reduce the sample size, thereby affecting test efficiency. Future studies could expand the sample size or focus on a specific subgroup for separate analysis to further validate the application value of the TyG index in different hypertensive patient populations and explore its interaction with other clinical indicators.
Conclusion
In summary, TyG is significantly associated with ACM in ICU patients with primary hypertension. This correlation highlights the importance of TyG as a simple and practical metabolic syndrome indicator, demonstrating its crucial predictive value in assessing mortality risk in critically ill primary hypertensive patients. The clinical application of TyG can aid in the stratification of critically ill hypertensive patients, enhancing treatment decisions and disease management. We recommend incorporating the TyG index into routine prognostic evaluation tools in clinical practice to optimize the management strategies of critically ill patients and improve overall prognostic outcomes.
Data availability
The datasets used and/or analysed during the current study available from us on reasonable request.
References
NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 398, 957–980 (2021).
Robitaille, C. et al. Diagnosed hypertension in Canada: Incidence, prevalence and associated mortality. CMAJ Can. Med. Assoc. J. = journal de l’Association medicale canadienne 184, E49-56 (2012).
Jackson, D. L., Proudfoot, C. W., Cann, K. F. & Walsh, T. A systematic review of the impact of sedation practice in the ICU on resource use, costs and patient safety. Crit. Care 14, 59 (2010).
Relationship between the triglyceride-glucose index and risk of cardiovascular diseases and mortality in the general population: a systematic review and meta-analysis—PubMed. https://pubmed.ncbi.nlm.nih.gov/35778731/.
Dang, K. et al. The association between triglyceride-glucose index and its combination with obesity indicators and cardiovascular disease: NHANES 2003–2018. Cardiovasc. Diabetol. 23, 8 (2024).
Brownlee, M. The pathobiology of diabetic complications: A unifying mechanism. Diabetes 54, 1615–1625 (2005).
Mancusi, C. et al. Insulin resistance the hinge between hypertension and type 2 diabetes. High Blood Press. Cardiovasc. Prev. 27, 515–526 (2020).
Liu, X. Z., Fan, J. & Pan, S. J. METS-IR, a novel simple insulin resistance indexes, is associated with hypertension in normal-weight Chinese adults. J. Clin. Hypertens. 21, 1075–1081 (2019).
Unger, G., Benozzi, S. F., Perruzza, F. & Pennacchiotti, G. L. Triglycerides and glucose index: A useful indicator of insulin resistance. Endocrinol. Nutr. 61, 533–540 (2014).
Ramdas Nayak, V. K., Satheesh, P., Shenoy, M. T. & Kalra, S. Triglyceride Glucose (TyG) Index: A surrogate biomarker of insulin resistance. JPMA J. Pak. Med. Assoc. 72, 986–988 (2022).
Chen, N. et al. Effects of triglyceride glucose (TyG) and TyG-body mass index on sex-based differences in the early-onset heart failure of ST-elevation myocardial infarction. Nutr. Metab. Cardiovasc. Dis. 34, 590–597 (2024).
Lakatta, E. G., Cohen, J. D., Fleg, J. L., Frohlich, E. D. & Gradman, A. H. Hypertension in the elderly: Age- and disease-related complications and therapeutic implications. Cardiovasc. Drugs Ther. 7, 643–653 (1993).
Connelly, P. J., Currie, G. & Delles, C. Sex differences in the prevalence, outcomes and management of hypertension. Curr. Hypertens. Rep. 24, 185–192 (2022).
Deere, B. P. & Ferdinand, K. C. Hypertension and race/ethnicity. Curr. Opin. Cardiol. 35, 342–350 (2020).
He, Z. et al. Effects of platelet count on blood pressure: Evidence from observational and genetic investigations. Genes 14, 2233 (2023).
Falkner, B. et al. Pediatric primary hypertension: An underrecognized condition: A scientific statement from the American Heart Association. Hypertension 80, e101–e111 (2023).
Tagi, V. M., Mainieri, F. & Chiarelli, F. Hypertension in patients with insulin resistance: Etiopathogenesis and management in children. Int. J. Mol. Sci. 23, 5814 (2022).
Steinberg, H. O. et al. Obesity/insulin resistance is associated with endothelial dysfunction. Implications for the syndrome of insulin resistance. J. Clin. Investig. 97, 2601–2610 (1996).
Huang, X. et al. TyG-BMI and hypertension in Normoglycemia subjects in Japan: A cross-sectional study. Diab. Vasc. Dis. Res. 20, 14791641231173616 (2023).
Liu, Y. et al. Triglyceride-glucose index as a marker of adverse cardiovascular prognosis in patients with coronary heart disease and hypertension. Cardiovasc. Diabetol. 22, 133 (2023).
Zhang, R. et al. Independent effects of the triglyceride-glucose index on all-cause mortality in critically ill patients with coronary heart disease: Analysis of the MIMIC-III database. Cardiovasc. Diabetol. 22, 10 (2023).
Huang, Y., Li, Z. & Yin, X. Triglyceride-glucose index: A novel evaluation tool for all-cause mortality in critically ill hemorrhagic stroke patients-a retrospective analysis of the MIMIC-IV database. Cardiovasc. Diabetol. 23, 100 (2024).
Author information
Authors and Affiliations
Contributions
J.D. completed the entire manuscript writing and data analysis, J.L. completed the data extraction and processing, X.C. and K.L. contributed to parts of the manuscript writing and revisions, K.Z. prepared the figures, and S.Y. prepared the tables. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent
This study was conducted in accordance to the Declaration of Helsinki, and the MIMIC-IV database has also been approved by the Massachusetts Institute of Technology and the Beth Israel Deaconess Medical Center. Copies of these data can be found in the MIMIC database. Therefore, this trial does not require ethical approval or informed consent. Written informed consent was obtained from all patients.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ding, J., Li, J., Cai, X. et al. The relationship between the triglyceride-glucose (TyG) index and all-cause mortality in ICU patients with primary hypertension: a retrospective study. Sci Rep 15, 12071 (2025). https://doi.org/10.1038/s41598-025-96202-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-96202-4
