
Abstract
Analyzing the trend and identifying the factors influencing the utilization of modern contraceptives is essential for designing effective measures to improve reproductive health and economic development to ensure universal access to family planning services. This study aimed to investigate the trends in modern contraceptive use among women of reproductive age in Ethiopia and the factors influencing these trends. Data from the 2014 to 2019 Performance Monitoring and Accountability/Action Survey datasets were analyzed, with 4422 women in 2014, 5113 in 2015, 5071 in 2016, 4927 in 2017, 4981 in 2018, and 6117 in 2019 included. Data analysis was conducted using Stata version 16.0 statistical software. Given the sample disproportionality, survey design considerations were taken into account by applying probability weights. The sample weight was utilized with weighting factors provided in the PMA data to address the complex survey design. The ‘svy’ Stata command was applied to consider the clustering effect before descriptive statistical analysis. The trend was examined based on selected characteristics, with the primary statistical parameter being the trend of modern contraceptive utilization. The trends of modern contraceptive utilization for each year from 2014 to 2019 were calculated. Then, logit-based decomposition analysis was used to identify the factors driving changes in modern contraceptive utilization. Statistical significance was determined at a P value of less than 0.05, and results were presented as decomposition coefficients and percentages. Additionally, we conducted data smoothing to predict the future trend of modern contraceptive utilization and did not visually observe a distinct trend. We explored different time-series models such as linear, quadratic, exponential, and exponential smoothing. The results showed that the exponential smoothing trend model provided the most accurate fit, with the lowest standard error of estimate, sum square error, and highest adjusted R2 value. The modern contraceptive utilization trend increased from 32.5% in 2014 to 37% in 2019, with 5.94% and 94.06% attributed to changes in composition and behavior, respectively. Changes in composition were influenced by factors such as women’s age, marital status, education level, community lifestyle, and number of children. Meanwhile, changes in behavior among educated women, those aged 35–49, with a certain number of children, and living an agrarian lifestyle contributed to the change in modern contraceptive use. The most significant increase in modern contraceptive methods mix during this timeframe was noted in the adoption of implants. The future trend in modern contraceptive use can be described by the formula: modern contraceptive utilization = 32.5 + 1.3 (coded year) − 0.099 (squared coded year), with an adjusted R2 value of 0.99 and a P value of 0.027. It suggests that the exponential smoothing trend can explain nearly 99% of the variation in modern contraceptive utilization. Over the past 6 years, population composition and behavior changes have driven a noticeable increase in modern contraceptive utilization. In Ethiopia, it is essential to target interventions toward advancing-age women, those women with no children, and women belonging to pastoralist communities to enhance contraceptive utilization rates further. Further, focusing on behavioral interventions and education to increase modern contraceptive use rather than solely targeting demographic changes is imperative.
Similar content being viewed by others


Introduction
As emphasized in the 2030 agenda for sustainable development, the effective utilization of contraceptive methods plays a vital role in attaining broad reproductive health advantages1. Contraception enables individuals and couples to exercise their right to make informed decisions about the number and spacing of their children2. The increasing utilization of contraceptives has led to positive health outcomes, including lower rates of unintended pregnancies and maternal and infant mortality, as well as improvements in education and economic opportunities, particularly for women and girls3. Access to contraceptives is not only linked to women’s reproductive rights and reducing unintended pregnancies but also contributes to the improved health and nutrition of children by promoting longer birth intervals and reducing maternal mortality rates1.
There is a global effort to promote the use of contraceptives to enhance sexual and reproductive health for women, with support from various international organizations, governments, NGOs, and community-based groups4. Despite significant investments in contraceptive services, millions of women worldwide express a desire to use contraceptives but face barriers to accessing them5. According to world population projections, significant shifts in sexual and reproductive practices have occurred over the past 50 years. There has been a notable decrease in family size and a substantial rise in the use of modern contraceptives, particularly in developing nations. From 1950–1955 to 2005–2010, the global average family size has halved from around 5–2.5 children and is projected to decrease further to 2.1 by 20506. However, developing countries still have a higher average number of children per woman than developed nations, with sub-Saharan Africa showing exceptionally high fertility rates among developing regions7.
Globally, there is a noticeable rise in contraceptive prevalence rates and a decline in unmet family planning needs. The increasing use of contraception has enabled many couples to plan the timing and desired size of their families efficiently. From 1990 to 2021, the global adoption of modern contraceptives has increased from 35% to approximately 45%5. However, the rate of change varied across regions8,9. In Ethiopia, the history of family planning started with the establishment of the Family Guidance Association of Ethiopia (FGAE) in 1966 in one clinic in Addis Ababa10. Following the transitional government’s adoption of the population policy in 1993, numerous local and international family planning organizations have partnered with the government to improve family planning programs and services. The Ethiopian Ministry of Health released Guidelines for Family Planning Services in 1996 to guide healthcare providers and administrators and expand and maintain high-quality family planning services nationwide11. Additionally, by working with the Ethiopian Ministry of Health, various parties have united their efforts to improve the availability of family planning services and assist in furthering the government’s dedication to the Family Planning 2020 program. This initiative strives to improve the population’s health outcomes and fulfill the nation’s developmental goals12.
The yearly rate of modern contraceptive utilization has steadily risen3. In 1990, only 3.9% of women of reproductive age in Ethiopia were using contraceptives13. However, by 2016, this rate had significantly increased to 36%. Even though there have been advancements, the use of modern contraceptives in Ethiopia remains low, indicating a significant unmet need for family planning at 22%14. Despite efforts to improve women’s sexual and reproductive health through initiatives like Family Planning 2020, progress in this area has been limited15. The high maternal mortality rate of 353 per 100,000 live births, of which 30% of deaths were attributed to abortion-related complications, demonstrates the high unmet need for FP in Ethiopia in addition to the early pregnancy among teenagers and high fertility rates that increase the risk of maternal and neonatal mortality16.
In Ethiopia, a considerable proportion of women express a desire for contraceptives but do not currently utilize them. The utilization of modern contraceptive methods remains limited, resulting in challenges such as unintended pregnancies, unsafe abortions, elevated fertility rates, and the spread of STIs and HIV/AIDS. It is essential to thoroughly evaluate and cater to the prevailing contraceptive requirements to combat these significant reproductive health concerns effectively17,18. Addressing the unmet need could reduce unintended pregnancies by 90%, lowering unplanned births from 1.2 million to 128,000 and miscarriages from 571,000 to 59,000 annually. Additionally, improving access to modern contraceptives and care for pregnant women and newborns could decrease maternal deaths by 81% (from 12,000 to 2000) and newborn deaths by 85% (from 92,000 to 13,000) each year19.
Given the high rates of unintended pregnancies, unsafe abortions, and high fertility rates that could be reduced through contraception, alongside the considerable unmet need for family planning and low modern contraceptive utilization in Ethiopia, complemented by such a lack of evidence about the changes or trends and factors affecting contraceptive utilization in Ethiopia, there is a critical need for a thorough investigation to analyze the trends over time and pinpoint crucial predictors.
The examination of the trends in modern contraceptive methods use in Ethiopia is vital for monitoring advancements, pinpointing influential factors, and assessing progress at a national scale. The intention behind this analysis is to provide insightful information to inform policymaking aimed at enhancing the acceptance of modern contraceptives among women of childbearing age in the country.
The key research questions are: (1) How has the utilization of modern contraceptives changed in Ethiopia over 6 years? (2) What factors affect the utilization of modern contraceptives in Ethiopia over 6 years? Answering these questions has its advantages in evaluating Ethiopia’s family planning program. Further, identifying the factors that affect modern contraceptive utilization would help tackle them and put better programs for better achievement. The hypothesis for these research questions is that there has been a notable change in the utilization of modern contraception among women of reproductive age. The increase in modern contraceptive use in Ethiopia from 2014 to 2019 may be attributed to behavioral factors, as well as changes in the characteristics of women within the study group, including factors such as age, marital status, education level, place of residence, community lifestyle, region, and wealth index.
Methods and materials
Study design and settings
The study used population-based cross-sectional survey data from PMA2020 Ethiopia 2014, 2015, 2016, 2017 and 2018. In addition, it has used data from the PMA-Ethiopia 2019 survey. Ethiopia is located in Eastern Africa in the southern Red Sea region. It borders the west with Sudan, on the north by Eritrea and Djibouti, Somalia on the east, and Kenya on the south. The country’s total area is 1,127,127 square kilometers20. Ethiopia has ten states: Afar, Amhara, Benishangul-Gumuz, Gambela, Harari, Oromia, Somali, SNNP, Tigray, and Sidama21. As of the Ethiopian Health Sector Transformation Plan report, Ethiopia has 16,440 health posts, 3547 health centers, and 311 hospitals, and it is indicated that the country has successfully implemented its strategy of expanding and rehabilitating primary healthcare facilities22. The Ethiopian overall UHC service coverage for 2015 was about 34.3%, ranging from 52.2% in Addis Ababa to 10% in the Afar region. The national RMNCH service coverage was 37.5%. Access to essential medicine was 50.8%, and only 13% of the population had access to hospital admission services23.
Study population
All women aged 15–49 years included in the PMA2020R1-6 and PMA-Ethiopia 2019 surveys across the country were considered the study population.
Sampling technique and sample size
PMA2020 started in 2014 (rounds 1 and 2), then one round every year, and the PMA 2019 was round 7. PMA2020 Ethiopia rounds 1–6 (2014–2018) were collected through a cross-sectional study design, and it generated nationally representative data on family planning (and more on other issues) that have been collected over different times from individual reproductive-age women, health facilities, and spatial and geographic factors. The PMA-Ethiopia 2019 survey implemented both cross-sectional and cohort studies that measure key indicators of reproductive, maternal, and newborn health (RMNH), including family planning. In each round of cross-sectional data collection, the data were collected over a 1-month by the PMA Ethiopia under the Ethiopian Ministry of Health and Addis Ababa University School of Public Health. Data collectors (female resident enumerators) supported by supervisors, regional coordinators, and PMA-Ethiopia central staff collected the data on individual reproductive-age women24.
Data source for the trends in modern contraceptive utilization
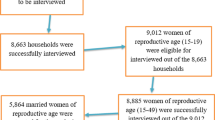
The current study used secondary data from the Ethiopia Performance Monitoring and Accountability Survey (PMA2020ET) and Performance Monitoring for Action Survey (PMAET) surveys, collected through nationally representative cross-sectional surveys conducted in 2014, 2015, 2016, 2017, 2018 and 2019 rounds and accessed from the PMA program official database https://www.pmadata.org/countries/ethiopia. The PMAET collected demographic, socio-economic, and health data from a representative sample of 6514 women in 2014, 7628 women in 2015, 7537 women in 2016, 7460 women in 2017, 7542 women in 2018, and 8928 women in 2019. Ethiopia has been stratified into eleven geopolitical provinces. Each province is made up of enumeration areas (EAs), which comprise the sampling frame. Respondents included in the PMAET were selected using a two-stage sampling strategy. The first stage involved selecting clusters, which were the primary sampling units; sampling was done with a probability proportional to the size, and the second stage involved a systematic sampling of households from the clusters that had been selected. In the current study, the analysis was focused on sexually active women who, at the time of the survey, had had sexual intercourse before. Our sample sizes for the trends in modern contraceptive use from the six PMAET were 4422 women in 2014, 5113 women in 2015, 5071 women in 2016, 4927 women in 2017, 4981 women in 2018, and 6117 women in 2019 (Fig. 1). All those who reported being pregnant or not sexually active or sub/infecund were excluded from the study.

The selection process for including women in the analysis of trends in modern contraceptive utilization data from the 2014 to 2018 Performance Monitoring and Accountability Ethiopia (PMAET2020) surveys and the 2019 Performance Monitoring for Action Ethiopia survey.
Study variables
The study focused on the utilization trends of modern contraceptives as the dependent variable. The independent variables included socio-demographic and maternal characteristics, with specific classifications for each. These independent variables and their respective categories were as follows: (Table 1)
Outcome variables
The outcomes variable for this objective was the Trends of modern contraceptive utilizations.
Measurements
Data quality control
Supervisors and regional coordinators conducted regular supervision and follow-up activities to guarantee data quality. Additionally, the completeness and consistency of the data were checked daily by supervisors and the data management team from the central staff of PMA-Ethiopia. The questionnaire was translated into Tigrigna, Amharic, and Afan-Oromo and then back-translated into English for data analysis. A reliable and valid tool relevant to the PMA-Ethiopia context was utilized. A pilot test and pre-test of the tool were conducted in an area with similar characteristics to the study population in various enumeration areas (EA) across the country. The pre-test was carried out 2 weeks before actual data collection to ensure the questions’ clarity, wording, logical sequence, and relevance. Furthermore, data collection was done using a smart mobile-based application (ODK) that facilitated skip patterns and immediate quality checks on the server, eliminated paper costs, and was user-friendly for data collectors. A data management team was assigned at the Addis Ababa PMA-Ethiopia central team and the JHU School of Public Health to oversee the daily data collection process24.
Data processing and analysis
The data retrieved from the official PMA database was exported and analyzed using the Stata 16.0 statistical software. Initial exploratory data analysis was conducted to identify outliers and missing data and ensure data consistency. Given the sample disproportionality, survey design considerations were taken into account by applying probability weights. The sample weight (SW) was utilized with weighting factors provided in the PMA data to address the complex survey design incorporating sample weighting, clustering, and stratification through the ‘svy’ analysis on Stata to adjust for varying population sizes. The ‘svy’ Stata command managed the clustering effect of complex sampling by applying it before statistical analysis.
The trend was examined based on selected characteristics, with the primary statistical parameter being the trend of modern contraceptive utilization and its associated factors. The trends of modern contraceptive utilization for each year from 2014 to 2019 were calculated using the Microsoft Excel for windows trend analysis. A line graph was generated to illustrate the trend over different years. Despite no clear trend observed in the initial line graph with actual data, exponential smoothing was employed to mitigate random and cyclical effects using a smoothing coefficient of 0.25 (Eq. 1). Even after smoothing the data, the trend remained indiscernible, prompting the use of exponential smoothing for short-term future value forecasting.
Three other time series models (linear, quadratic, exponential), including the exponential smoothing, were tested to determine the most suitable model explaining the trend based on criteria like lowest standard error of estimate, sum square error (SSE), and highest adjusted R2 value25. The exponential smoothing trend model emerged as the best fit, followed by the quadratic model, while the linear model exhibited the weakest fit, and the exponential model followed suit. Consequently, the exponential smoothing trend model was selected to characterize the trend. The exponential smoothing trend model was therefore used to describe the trend.
Exponential smoothing formula
where “W” represents the smoothing number, we chose the smallest smoothing number (W) of 0.25 in this case. The “current value” indicates the value or prevalence of modern contraceptive utilization in each survey year.
Finally, the datasets were merged using the Stata ‘append’ command, and multivariate decomposition analysis was conducted to examine changes in modern contraceptive utilization and its contributing factors.
To address the research questions, a multivariate decomposition analysis was employed to examine changes in modern contraceptive use. This analysis involved a regression decomposition of the differences in modern contraceptive use across six PMA-Ethiopia surveys, aiming to identify the sources of changes in utilization over the past 6 years (2014–2019). This method is commonly used in demography because it helps to elucidate how changes in population composition and behavior relate to modern contraceptive use. The current analysis investigates explicitly how variations in women’s characteristics influence modern contraceptive use and how these factors contribute to differences observed across PMA surveys conducted at different times. For linear relationships, the dependent variable is modeled as a function of a linear combination of predictors and regression coefficients. The logistic regression model output facilitated decomposing observed differences in modern contraceptive utilization into two components: population composition changes across surveys and population behavior variations. Consequently, the observed differences in modern contraceptive use between various surveys are decomposed into two components: one reflecting characteristic (or endowments) and the other reflecting coefficients (or effects of factors).
Ethics approval
This study did not require ethical approval since we have used publicly available PMA-Ethiopia datasets. The data were accessed from https://www.pmadata.org/countries/ethiopia after the purpose of the study with respect to the data-sharing policy was explained. The accessed data were used for the purpose of a registered research paper only. Confidentiality of the data was maintained, and no effort was made to identify any household or individual respondents interviewed in the survey. The data were not passed on to other researchers without the written consent of PMA-Ethiopia.
Results and discussion
Characteristics of the study population
Table 2 shows the distribution of the sampled reproductive-age women. Among the respondents, more than five out of ten in all the six PMA-ET survey periods were in the age category of 34–49. Among the respondents, around 50% of the respondents in the six surveys had a never-educated educational status. The proportion with primary education rose slightly from 30.45% in 2014 to 34.2% in 2019. Across the six survey periods, more than eight of ten women’s marital status was married or living with a partner.
Concerning residence, in all the survey periods, the respondents resided in more than 75% of rural areas, except in the 2019 survey period, where 31.6% lived in urban areas and 68.4% resided in rural areas. The number of parties in each category remained more or less similar across all six survey periods. Regarding the women’s wealth index quintile, more or less the share of the proportion in each category was 20%.
In all six surveys, only a small proportion of women reported being visited by a health extension worker who talked about FP. Moreover, the percentage decreased from 25% in 2014 to 11.2% in 2019. Similarly, the proportion of women who spoke about FP during facility visits with staff decreased from 33.8% in 2014 to 24.2% in 2019 (Table 2).
Trends in modern contraceptive utilization by background characteristics
The trend period was segmented into five phases to analyze the variations in the increment over time based on women’s background characteristics. The most significant increase in modern contraceptive utilization was seen in 2014–2015 in the age group of 15–19 women, with 9.33 percentage points compared with a decrement of 3.35 percentage points in 2017–2018. An overall increment of 15.36 percentage points was seen among the age group 15–19 women in 2014–2019.
The Oromia, Benishangul-Gumuz, Gambella, Dire-Dawa, SNNP, Addis Ababa, and Tigray regions showed an increment in modern contraceptive use between 2014 and 2019. In contrast, the Afar, Somali, Amhara, and Harari regions experienced the most significant decrease in modern contraceptive utilization between 2014 and 2019. Overall, the highest modern contraceptive utilization was in SNNP (46.09%), Amhara (50.03%), Gambella (50.87), Dire-Dawa (49.57), Addis Ababa (45.37%), while the lowest utilization of modern contraceptive was in Somali (0.98%) and Afar (2.13%).
Between 2014 and 2019, modern contraceptive utilization reduced by 13.01% in Harari, 7.09% in Afar, 3.63% in Amhara, and 3.02% in Somali but increased by 28.31 in Benishangul-Gumuz, 12.69% in Oromia, 9.7% in Gambella, 7.52% in Addis Ababa, 4.93% in SNNP and 4.59% in Diredawa. The lowest percentage point increment of 0.6 was seen in the Tigray region.
Between 2014 and 2019, there was an increase in modern contraceptive utilization among women based on their wealth index quintile. Specifically, the lowest quintile saw a rise of 8.55 percentage points, the lower quintile increased by 4.24 percentage points, the middle quintile increased by 8.85 percentage points, and the higher quintile increased by 1.79 percentage points. However, there was a decrease of 10.91 percentage points in modern contraceptive utilization for the highest quintile during this period.
Those married/living with partners and never-married women showed a more significant increment in modern contraceptive utilization during the 2014 and 2019 study periods compared to those separated/widow or divorced women. Women who reside in rural areas have a 4.9 percentage point Increment in modern contraceptive utilization. In contrast, there was only a 0.11 percentage point increment in modern contraceptive utilization among urban residents between 2014 and 2019. Among urban residents, the most significant increment in modern contraceptive utilization was seen during the 2014–2015 study period, at a 4.88 percentage point compared with a 4.42 percentage point decrease in 2016–2017 (Table 3).
The trend of modern contraceptive prevalence and method mix in Ethiopia
Between 2014 and 2019, just over one-third of women in Ethiopia utilized modern contraceptive methods. The prevalence of modern contraceptives among women of reproductive age showed significant growth from 32.5% in 2014 to 37% in 2019, showing an average yearly increase of 0.75 percentage points over the 6 years. Notably, modern contraceptive use experienced a notable rise of 4.5 percentage points from 2014 to 2015, followed by a smaller increase of 1.2 percentage points in 2016. However, there was a slight decline of 1 percentage point in 2017 before rebounding with a two percentage points increase in 2018. In 2019, there was a decrease of 2.2 percentage points in modern contraceptive use compared to the previous year. The most significant increase in modern contraceptive methods mix during this timeframe was noted in the adoption of implants (Figs. 2 and 3; Table 4).

Modern contraceptive use among women in Ethiopia for each year from 2014 to 2019.

Modern contraceptive method utilization mixes in each year from 2014 to 2019.
Time-series forecasting models for modern contraceptive utilization
The exponential smoothing trend model demonstrated the best fit, with the lowest standard error of estimate (0.024), the lowest sum of squared errors (0.0678), and the highest adjusted R2 value (0.99). As per the exponential smoothing trend time-series model, there was a statistically significant rise in modern contraceptive utilization. Over the reference period, modern contraceptive utilization showed an increasing trend, following the exponential smoothing equation, modern contraceptive utilization = 32.5 + 1.3 (coded year) − 0.099 (squared year code), with an R2 value of 0.99 and a P value of 0.027, indicating that approximately 99% of the variability in modern contraceptive utilization can be explained by the trend (Table 5).
Multivariate decomposition of modern contraceptive utilization from 2014 to 2019
The decomposition analysis model was utilized to consider the variations in characteristics (compositional factors) and the variations attributed to the impact of these characteristics (coefficients). About 5.94% of the overall change in modern contraceptive utilization was due to differences in characteristics and effects (explained/endowment component). Among the compositional factors, a significant contribution to change in modern contraceptive utilization among the reproductive age group was due to women’s age, marital status, educational status, number of living children/parity, and community way of life. The change in composition of women who were in the age group of 35–49 showed a significant contribution to increasing modern contraceptive utilization.
Furthermore, a substantial increase in modern contraceptive utilization was due to the change in the composition of women who were in primary, secondary, and more than secondary education. However, decrement in modern contraceptive utilization was observed in the composition of women who were divorced/separated/widowed and never married. The change in the composition of women who were agrarian as a community way of life has a significant contribution to decreasing modern contraceptive utilization. The change in the composition of women who had one and two to three children contributed to an increase in modern contraceptive utilization. However, the change in the composition of women who had four and above children contributed to a decrease in modern contraceptive utilization.
After controlling the effect of compositional factors, 94.06% of the change in modern contraceptive utilization was due to the differences in coefficient effects (unexplained/coefficient component). A significant change in modern contraceptive utilization was due to the age of women, educational status, parity, and community way of life. The change in the coefficients/effects of women aged 35–49 showed a significant contribution to the decrement of modern contraceptive utilization. The change in the coefficients/effects of women who were agrarian as a community way of life has also made a significant contribution to the decrement in modern contraceptive utilization.
Furthermore, women who had primary, secondary, and more than secondary educational status contributed to the decrement in modern contraceptive utilization. However, the change in the coefficients/effects of women who had one and above children contributed to increasing modern contraceptive utilization. Generally, the change in modern contraceptive utilization from 2014 to 2019 is more attributed to the changes in the coefficients/effect (behavioral changes) than the compositional factors (Table 6).
Discussion
The current study revealed an annual increase in modern contraceptive use in Ethiopia over the past 6 years (2014–2019). This trend aligns with findings from the DHS studies in Ethiopia, Ghana, and Zambia, indicating a rise in modern contraceptive usage over time14,26,27. The rise in the use of modern contraceptives can be credited to the comprehensive family planning initiatives undertaken by both governmental and non-governmental organizations. These efforts have been bolstered by healthcare infrastructure enhancements and health sector development strategies28. Additionally, Ethiopia’s Federal Ministry of Health (FMOH) has set ambitious goals to promote the provision of family planning services and counseling by frontline healthcare workers22.
The prevalence of modern contraceptive use among women of reproductive age has been on the rise, with rates increasing from 32.5% in 2014 to 37% in 2019, showing an annual increment of 0.75 percentage points. According to the DHS, Ethiopia saw an increase in modern contraceptive use rates to 35.2%, while Kenya and Rwanda had rates of 53.2% and 47.5%, respectively. The annual average increases in modern contraceptive prevalence among married women were 1.6 percentage points in Ethiopia from 2011 to 201914, 3.5 percentage points in Rwanda from 2008 to 201429, and 2.8 percentage points in Kenya from 2009 to 201430. In addition, it is less than the global modern contraceptive utilization, which is 2.1 percentage points31. Compared to Kenya and Rwanda, Ethiopia’s lower levels of modern contraceptive utilization could be attributed to the less availability of family planning services, insufficient health infrastructure and training for healthcare professionals, and cultural distinctions among the nations.
Additionally, the current study’s findings in 2019 showed a decrease in modern contraceptive use trends from the previous rounds of PMA data. This decline could be attributed to the changes in the health system may not meet the demands and needs of women seeking modern contraceptive services that discourage them from using modern contraceptive methods due to stock-outs of modern contraceptive commodities, a shortage of trained and qualified health workers to insert and remove implants and IUDs, insufficient equipment and supplies, and limited range and diversity of modern contraceptive methods32,33. The political instability in Ethiopia started in 2015/16 and later advanced to the armed struggle, which might have contributed later on to the trends in the utilization of modern contraception. This is supported by studies conducted in Tigray, Ethiopia, that indicated the decrease of modern contraceptive utilization post-war compared to prewar34. Further, a study conducted in Syria, where healthcare workers and health facilities were targeted during the war, has a direct effect on the declining provision of health services35. Moreover, the decrement might be associated to the US political administration called the Global Gag Rule (GGR), which imposes restrictions on programs in all countries, irrespective of the abortion laws in place. The GGR was indicated to have the potential to impede advancements in sexual and reproductive health and lead to a stagnation in modern contraceptive utilization in Ethiopia36.
The result indicates that while demographic changes play a role in the prevalence of modern contraceptives, the more significant driver of change is the behavioral change among individuals, which aligned with findings in Rwanda37. The decomposition analysis indicates that a small portion of the change in modern contraceptive prevalence can be attributed to differences in the characteristics of the population over time. In this case, only about 6% of the observed change in prevalence is due to changes in who makes up the population. This includes age, marital status, education levels, parity, and community lifestyle variables.
On the other hand, the substantial percentage suggests that the majority of the change in modern contraceptive prevalence (over 94%) is due to changes in behavior among individuals within the population. This could involve increases in contraceptive use due to factors such as age, educational status, parity, and community lifestyle. The key concept in this section is that a significant impact of the change in modern contraceptive utilization occurs when the population’s behavior changes in response to key variables. Hence, the insight from the decomposition analysis revealed a valuable result for policymakers and program planners as it indicates the importance of focusing on behavioral interventions and education to further increase modern contraceptive use rather than solely targeting demographic changes.
Changes in effects contributed to the majority of the change in modern contraceptive use. The change in the behavior of women aged 35–49 played a crucial role in the decline of modern contraceptive utilization. This observation aligns with studies from Bangladesh, which suggested that as women grow older, the likelihood of adopting modern contraceptive methods decreases38. This trend indicates that advancing-age women may face heightened chances of unintended pregnancies and shorter intervals between births, posing potential adverse outcomes. Connecting these findings to the decrement in the adoption of modern contraceptives in Ethiopia is essential for understanding and addressing the factors influencing contraceptive practices among different age groups of women.
The study found that the change in the coefficients/effects of women with one or more children played a role in increasing the use of modern contraceptives. This aligns with findings from a trend study in Ethiopia39,40. Evidence also indicates that disparities in family planning services based on parity are prevalent in many African regions. This discrimination often occurs when service providers hold negative views toward premarital sex or the use of contraceptives by women who have not given birth. Furthermore, there is societal pressure on women to conceive shortly after getting married, resulting in contraception being regarded as inappropriate until after their first delivery41,42. In addition, a higher likelihood of modern contraceptives among women with one or more children could be because of a greater understanding of the advantages and risks associated with various contraceptive options, enabling them to make informed choices. Having experienced parenthood and potentially achieved their desired family size, these women may possess more knowledge and expertise in contraceptive practices, resulting in improved information and behavior changes related to contraception.
An increase in the composition of education levels of women has been linked to a rise in the use of modern contraceptives as a contributing factor. This is aligned with other trend studies conducted elsewhere39,43,44. Educated mothers are more likely to have access to information and resources regarding contraception. Furthermore, education plays a crucial role in enhancing women’s independence and authority in making decisions within their households, which could facilitate discussions about contraceptive utilization with their partners. Consequently, with a higher proportion of educated women in society, there is a greater likelihood that more women will opt for modern contraceptives. This trend can potentially lead to a decrease in unintended pregnancies and mitigate the negative repercussions associated with fluctuations in fertility rates.
The change in the composition of women who were agrarian as a community lifestyle has also made a significant contribution to the increment in modern contraceptive utilization. This is similar to studies conducted in Ethiopia14,45. The trends of modern contraceptive methods utilization were indicated as low in the pastoralist communities of Afar and Somali regions. Women residing in the Afar and Somali regions of Ethiopia had the lowest increase in the trends of modern contraceptive utilization. This may be due to the pastoralist communities’ different social and cultural beliefs46. The Afar and Somali region populations are pastoralists and nomadic, less educated47, low wealth quintile48, which may limit their access to health facilities to get modern contraceptive methods easily. In addition, women residing in these regions are linked to less access to health facilities49. Further, The Afar and Somali women’s religion is primarily Muslim. Muslims found that there is significant evidence for a relationship between religious socialization and contraceptive behavior, and a study that examined religious group differences in fertility in 30 developing nations found that Muslim fertility is substantially higher than Christian fertility in many countries50. Lastly, the low coverage of family planning in the pastoralist communities could be due to the husband’s influence to have more children and religious and clan leaders.
A decrease in the use of modern contraceptives was noted among the composition of unmarried women, including those who were divorced, separated, widowed, or never married, compared to women who were married or cohabiting. These findings align with previous evidence from elsewhere51,52,53. Various factors could explain this trend. Those women who are divorced, separated, widowed, or never married might experience societal stigma or judgment for using modern contraceptives. They may have limited access to accurate information about modern contraceptives compared to married women, which can result in misconceptions or fear of potential side effects. Cultural norms and beliefs may also discourage unmarried women from using modern contraceptives, as they could be viewed as contradicting traditional values or being promiscuous. Furthermore, unmarried women may fear criticism or disapproval from family members, partners, or society if they choose to use modern contraceptives, leading them to avoid seeking out these methods. Additionally, some unmarried women may be in relationships where their partners do not support contraceptive use, making it challenging for them to obtain and use modern contraceptives.
Modern contraceptive utilization showed a significant time-series forecasting trend, following the exponential smoothing equation, modern contraceptive utilization = 32.5 + 1.3 (coded year) − 0.099 (squared year code). This trend may provide insight into the short-term future of modern contraceptive utilization. However, the decline in modern contraceptive utilization observed in the results from 2018 and 2019 appears to have influenced the future modern contraceptive use trend, as the smoothing factors were impacted by the low prevalence of contraceptive use during those specific years.
Strengths and weakness
This research utilized large datasets and considered sample weighting in the analysis process. Using data from the Performance Monitoring for Action Ethiopia Survey, we made comprehensive conclusions about modern contraceptive usage with substantial sample size and statistical robustness. Furthermore, decomposition analysis allowed us to examine changes in population demographics and trends over time. However, the study focused on self-reported modern contraceptive utilization, which could be affected by recall bias. The other limitation is that the study could not establish causal conclusions due to its cross-sectional design, which simultaneously assesses exposure and outcome. As a result, no evidence typically indicates a temporal relationship between the two. It was also worth mentioning that the analysis incorporated specific variables consistently captured in all surveys, suggesting that these are not the only factors influencing the trend in modern contraceptive utilization.
Conclusions
Over the last 6 years, there has been a notable increase in the use of modern contraceptives among women of reproductive age in Ethiopia. This increase could be attributed to population composition and behavior changes. Factors such as women’s age, educational background, the number of children they have, and the community’s way of life all play significant roles in influencing the adoption of modern contraceptive methods. It is crucial to implement targeted interventions aimed at advancing age women, those women with no children, and women belonging to pastoralist communities to further enhance the utilization of modern contraceptives in Ethiopia. By addressing these specific groups, we can work towards increasing access to and acceptance of contraception, ultimately contributing to improved reproductive health outcomes in the region.
Data availability
We used a cross-sectional dataset from the Performance Monitoring for Action Ethiopia (PMA-ET) 2014 to 2019 survey which is publicly available and accessed after submitting our study’s abstract to PMA-Ethiopia at https://www.pmadata.org/countries/ethiopia. The terms and conditions of the PMA-Ethiopia data do not allow sharing the data with others (only used for the registered data). We didn’t receive any special privileges to access the data. Thus, any researcher can apply to access the data from the PMA-Ethiopia office at https://www.pmadata.org/countries/ethiopia.
Abbreviations
- DHS:
-
Demographic and Health Survey
- EA:
-
Enumeration area
- EDHS:
-
Ethiopian Demographic and Health Survey
- FGAE:
-
Family Guidance Association of Ethiopia
- FP:
-
Family planning
- FQ:
-
Female questionnaire
- GGR:
-
Global gag rule
- HEW:
-
Health extension workers
- HHQ:
-
House hold questionnaire
- JHBSPH:
-
John Hopkins Bloomberg School of Public Health
- JHU:
-
Johns Hopkins University
- LL:
-
Lower limit
- ODK:
-
Open data kit
- PMA2020:
-
Performance Monitoring and Accountability 2020
- PMA-Ethiopia:
-
Performance Monitoring for Action Ethiopia
- RE:
-
Resident enumerator
- SE:
-
Standard error
- SNNP:
-
South Nations Nationalities and People
- SSE:
-
Sum square error
- UL:
-
Upper limit
References
United Nations, Department of Economic and Social Affairs PD. Family Planning and the 2030 Agenda for Sustainable Development (Data Booklet). (ST/ESA/SER.A/429) [Internet] (New York, 2019). Available from: https://www.un.org/en/development/desa/population/publications/pdf/family/familyPlanning_DataBooklet_2019.pdf.
United Nations. Report of the International Conference on Population and Development [Internet] (New York, 1994). Available from: https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/files/documents/2020/Jan/un_1995_programme_of_action_adopted_at_the_international_conference_on_population_and_development_cairo_5-13_sept._1994.pdf.
United Nations Department of Economic and Social Affairs Population Division. World Fertility and Family Planning 2020 Highlights [Internet] (Department of Economic and Social Affairs Population Division, New York; 2020). Available from: https://www.un.org/en/development/desa/population/publications/pdf/family/World_Fertility_and_Family_Planning_2020_Highlights.pdf.
Fagbamigbe, A. F. & Afolabi, R. F. II. Demand and unmet needs of contraception among sexually active in-Union Women in Nigeria: Distribution, associated characteristics, barriers, and program implications. SAGE Open 8, 1–11 (2018).
United Nations, Department of Economic and Social Affairs PD. World Family Planning 2022, Meeting the Changing Needs for Family Planning: Contraceptive use by Age and Method [Internet] (United Nations, New York: United Nations, Department of Economic and Social Affairs, Population Division, 2022). Available from: https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/files/documents/2023/Feb/undesa_pd_2022_world-family-planning.pdf.
United Nations, Department of Economic and Social Affairs PD. World Population Prospects 2019: Highlights [Internet] (WPP, New York, 2019). Available from: https://www.ined.fr/fichier/s_rubrique/29368/wpp2019_10.key.findings_embargoed.version.en.pdf.
UN-DESA/POP/2022/TR/NO.3. World Population Prospects 2022 [Internet], 1–52 (United Nation, 2022). Available from: www.un.org/development/desa/pd/.
Alkema, L., Kantorova, V. & Menozzi, C. B. A. National, regional, and global rates and trends in contraceptive prevalence and unmet need for family planning between 1990 and 2015: A systematic and comprehensive analysis. Lancet 381(9878), 1642–1652. https://doi.org/10.1016/S0140-6736(12)62204-1 (2013).
Fiato, N. R. Family Planning in Sub-Saharan Africa: A Review of Interventions in Promotion of Long-Acting Reversible Contraception [Internet] (Univ Pittsburgh Comm, 2016). Available from: https://d-scholarship.pitt.edu/27371/1/fiatonr_etd_4_2016.pdf.
Federal Democratic Republic of Ethiopia Ministry of Health. National reproductive Health Strategy 2020–2016 [Internet] (Addis Ababa, 2016). Available from: https://www.prb.org/wp-content/uploads/2020/06/Ethiopia-National-Reproductive-Health-Strategy-2016-2020.pdf.
Federal Democratic Republic of Ethiopia Ministry Of Health. National Guideline for Family Planning [Internet] (Federal Democratic Republic of Ethiopia Ministry of Health, Addis Ababa, 2011). Available from: https://scorecard.prb.org/wp-content/uploads/2022/03/National-Guideline-for-Family-Planning-Services-In-Ethiopia-2020.pdf.
Brown, W. et al. Developing the “120 by 20” goal for the global FP2020 initiative. Stud Fam Plann. 45(1), 73–84 (2014).
Transitional Government of Ethiopia Central Statistical Authority Population Analysis and Studies Center. The 199O National Family and Fertility Survey Report [Internet] (Addis Ababa, Ethiopia, 1993). Available from: https://repository.uneca.org/bitstream/handle/10855/22310/Bib-28177.pdf?sequence=1.
Central Statistical Agency (CSA) [Ethiopia] and I. Ethiopia Demographic and Health Survey 2016 [Internet] (Addis Ababa, Ethiopia, and Rockville, Maryland, USA, 2016). Available from: https://dhsprogram.com/pubs/pdf/FR328/FR328.pdf.
Cahill, N., Sonneveldt, E., Stover, J., Weinberger, M. & Williamson, J. E. Modern contraceptive use, unmet need, and demand satisfied among women of reproductive age who are married or in a union in the focus countries of the family planning 2020 initiative: A systematic analysis using the family planning estimation tool. Lancet 391(10123), 870–882. https://doi.org/10.1016/S0140-6736(17)33104-5 (2018).
MoH. Ethiopia National Family Planning Communication Guideline, 2020 [Internet] (Federal Ministry of Health. Addis Ababa, Ethiopia, 2021). Available from: https://www.moh.gov.et/sites/default/files/2024-04/National-Family-Planning-Communication-Guideline.pdf.
Sundaram, A. et al. Benefits of meeting the contraceptive needs of Ethiopian women. In Brief [Internet] (Guttmacher Institute, New York, 2010). Available from: https://www.guttmacher.org/pubs/IB-Contraceptive-Needs-Ethiopia.pdf.
Singh, S., Darroch, J. E. & Ashford, L. S. Adding It Up: The Costs and Benefits of Investing in Sexual and Reproductive Health [Internet] (Guttmacher Institute and UNFPA, New York, 2014). Available from: https://www.guttmacher.org/report/adding-it-up-investing-in-sexual-reproductive-health-2019.
Guttmacher Institute. ADDING IT UP: Investing in Contraception and Maternal and Newborn Health for Adolescents in Ethiopia, 2018 [Internet] (New York, 2018). Available from: https://www.guttmacher.org/fact-sheet/adding-it-up-contraception-mnh-adolescents-ethiopia.
United States Library of Congress. Country Profile: Ethiopia [Internet] (2005). Available from: https://www.refworld.org/docid/46f913420.html.
Austrian Government DFAT. DFAT Country Information Report Ethiopia [Internet] (2020). Available from: https://www.dfat.gov.au/sites/default/files/country-information-report-ethiopia.pdf.
Federal Minister of Health (FMOH). Health Sector Transformation Plan [Internet] (2015). Available from: https://www.cmpethiopia.org/content/download/2268/9612/file/HSTP-Final-2015-10-19.pdf.
Eregata, G. T., Hailu, A., Memirie, S. & Norheim, O. F. Measuring progress towards universal health coverage: National and subnational analysis in Ethiopia. BMJ Glob. Heal. 4(6), 1–9 (2019).
Zimmerman, L. et al. Protocol for PMA-Ethiopia: A new data source for cross-sectional and longitudinal data of reproductive, maternal, and newborn health [version 1; peer review: 2 approved]. Gates Open Res. 4, 1–16 (2020).
Berenson, M., Levine, D., Szabat, K. A. & Krehbiel, T. C. Basic Business Statistics: Concepts and Applications [Internet], 510–25 (2012). Available from: https://www.amazon.com/Basic-Business-Statistics-Concepts-Applications/dp/0132168383.
Phiri, M. & Banda, C. Trends in Modern Contraceptive Use and Factors Associated with Current Use in Zambia: Evidence from DHS Data 1992–2014 [Internet] (2014). Available from: https://uaps2015.popconf.org/papers/150529.
Aviisah, P. A. et al. Modern contraceptive use among women of reproductive age in Ghana: Analysis of the 2003–2014 Ghana Demographic and Health Surveys. BMC Womens Health 18(141), 1–10. https://doi.org/10.1186/s12905-018-0634-9 (2018).
USAID/Africa Bureau, USAID/Population and Reproductive Health, Ethiopia Federal Ministry of Health, Malawi Ministry of Health RM of H. Three Successful Sub-Saharan Africa Family Planning Programs-Lessons for meeting the MDGs [Internet] (Washington, 2012). Available from: https://pdf.usaid.gov/pdf_docs/PA00HQSV.pdf.
National Institute of Statistics of Rwanda (NISR) [Rwanda], Ministry of Health (MOH) [Rwanda] and II. Rwanda Demographic and Health Survey 2014–2015 [Internet] (2015). Available from: https://dhsprogram.com/pubs/pdf/FR316/FR316.pdf.
Kenya National Bureau of Statistics (KNBS) and ICF International. Kenya Demographic and Health Survey [Internet], vol. 7 (2015). Available from: https://dhsprogram.com/pubs/pdf/fr308/fr308.pdf.
Kantorova, V., Wheldon, M. C. & DA Ueffing, P. Estimating progress towards meeting women’s contraceptive needs in 185 countries: A Bayesian hierarchical modelling study. PLoS Med. 17(2), 1–23 (2020).
Seyife, A., Fisseha, G., Yebyo, H., Gidey, G. & Gerensea, H. Utilization of modern contraceptives and predictors among women in Shimelba refugee campp, Northern Ethiopia. PLoS ONE 14(3), 1–11 (2019).
Ouma, L. et al. A cross-country qualitative study on contraceptive method mix : Contraceptive decision making among youth. Reprod. Health 18(105), 1–14. https://doi.org/10.1186/s12978-021-01160-5 (2021).
Tsadik, M. et al. Armed conflict and maternal health service utilization in Ethiopia’s Tigray Region: A community-based survey. BMC Public Health 24(1), 1–9 (2024).
Fouad, F. M. et al. Health workers and the weaponisation of health care in Syria: A preliminary inquiry for The Lancet-American University of Beirut Commission on Syria. Lancet 390(10111), 2516–2526. https://doi.org/10.1016/S0140-6736(17)30741-9 (2017).
Sully, E. A. et al. Impact of the global gag rule on women’s contraceptive use and reproductive health outcomes in Ethiopia: A pre-post and difference-in-difference analysis. BMJ Open 13(5), 1–10 (2023).
Muhoza, D. N., Rutayisire, P. C. & Umubyeyi, A. Measuring the Success of Family Planning in Rwanda: A Multivariate Decomposition Analysis in Rwanda [Internet] (DHS Program, 2013). Available from: https://dhsprogram.com/pubs/pdf/WP94/WP94.pdf.
Rana, S. et al. Exploration of modern contraceptive methods using patterns among later reproductive-aged women in Bangladesh. PLoS ONE 19(4), e0291100. https://doi.org/10.1371/journal.pone.0291100 (2024).
Kebede, N. et al. A multivariate decomposition analysis of modern contraceptive utilization among married women in the emerging region of Ethiopia (2000–2019). Sci. Rep. 13(1), 1–7. https://doi.org/10.1038/s41598-023-48176-4 (2023).
Hounton, S. et al. Patterns and trends of contraceptive use among sexually active adolescents in Burkina Faso, Ethiopia, and Nigeria: Evidence from cross-sectional studies. Glob. Health Act. 8(1), 29737 (2015).
Rivera, R., Mello, M. C. D., Johnson, S. L. & Chandra-Mouli, V. Contraception for adolescents: Social, clinical and service-delivery considerations. Int. J. Gynecol. Obstet. 75(2), 149–163 (2001).
Bankole, A. & Malarcher, S. Removing barriers to adolescents’ access to contraceptive information and services. Stud. Fam. Plann. 41(2), 117–124 (2010).
Emina, J. B. O., Chirwa, T. & Kandala, N.-B. Trend in the use of modern contraception in sub-Saharan Africa: Does women’s education matter?. Contraception 90(2), 154–161. https://doi.org/10.1016/j.contraception.2014.02.001 (2014).
Gordon, C., Sabates, R. & Bond, R. W. T. Women’s education and modern contraceptive use in Ethiopia. Int. J. Educ. 3(1), 9 (2011).
Alemayehu, M. et al. Family planning use and associated factors among pastoralist community of afar region, eastern Ethiopia. BMC Womens Health 16(1), 1–9. https://doi.org/10.1186/s12905-016-0321-7 (2016).
Srikanthan, A. & Reid, R. L. Religious and cultural influences on contraception. J. Obstet. Gynaecol. Can. 30(2), 129–137. https://doi.org/10.1016/S1701-2163(16)32736-0 (2008).
Ministry of Education of Ethiopia. Education Statistics Annual Abstract September 2019–March 2020 [Internet], 1–107 (2022). Available from: https://213.55.93.148/storage/Books/Education-Statistics-Annual-Abstract-March-2019-September-2020.
World Bank. Ethiopia Regional Poverty Report: Promoting Equitable Growth for All Regions [Internet] (Ethiopia Regional Poverty Report, 2020). Available from: https://documents1.worldbank.org/curated/en/627681605631546436/pdf/Ethiopia-Regional-Poverty-Report-Promoting-Equitable-Growth-for-All-Regions.pdf.
Tegegne, T. K. et al. Spatial variations and associated factors of modern contraceptive use in Ethiopia: A spatial and multilevel analysis. BMJ Open 10, 1–11 (2020).
Heaton, T. B. Does religion influence fertility in developing countries. Popul. Res. Policy Rev. 30, 449–465 (2011).
Beyene, K. M., Bekele, S. A. & Abu, M. Factors affecting utilization of modern contraceptive methods among women of reproductive age in Ethiopia. PLoS ONE 18(11), e0294444. https://doi.org/10.1371/journal.pone.0294444 (2023).
Zeleke, G. T. & Zemedu, T. G. Modern contraception utilization and associated factors among all women aged 15–49 in Ethiopia: Evidence from the 2019 Ethiopian Mini Demographic and Health Survey. BMC Womens Health 23(51), 1–7. https://doi.org/10.1186/s12905-023-02203-8 (2023).
Bizuneh, F. K., Bizuneh, T. K. & Masresha, S. A. Y. B. Individual and community level factors for modern contraceptives utilization among reproductive aged women in Amhara region, mixed effect multi-level modeling, data from mini-EDHS, 2019. Contracept. Reprod. Med. 8(1), 1–10 (2023).
Acknowledgements
We thank the Performance Monitoring for Action (PMA) program for allowing us to use this study’s Ethiopian Performance Monitoring and Accountability/Action (PMA-ET) data.
Data disclaimer
This manuscript’s depiction of the data is original and does not imply the expression of any opinion by Springer nature or any member of its group.
Author information
Authors and Affiliations
Contributions
HGG contributed to the initiation of the study, design, data collection, data analysis, and write-up. MA and GTD contributed to the initiation of the study, design, and write-up. HGG contributed to the interpretation of the findings and write-up of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Gebrekidan, H.G., Alemayehu, M. & Debelew, G.T. Trend and multivariate decomposition analysis of modern contraceptive utilization among women in Ethiopia. Sci Rep 15, 11503 (2025). https://doi.org/10.1038/s41598-025-96394-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-96394-9
