
Abstract
With the climate changing and worsening rainfall patterns, dengue, and its vector, the Aedes spp. mosquito, are becoming an urgent matter both in Colombia and globally. The limited availability of vaccines for this arbovirus, combined with the risk of severe disease with each reinfection, means that dengue control primarily relies on targeted vector control tailored to specific areas. This study aims to analyze the social perceptions and environmental risk factors that affect mosquito presence and dengue acquisition in Restrepo, Meta, Colombia. A knowledge, attitudes and practices questionnaire, and focus groups were conducted in communities of Restrepo, and entomological indexes were calculated for the municipality. Quantitative and qualitative analysis were performed. Participants had good knowledge of arbovirus infections, but lacked specific knowledge about transmission and how best to protect themselves. Those knowledgeable of cleaning water tanks were 0.28 times as likely to have mosquitos trapped in their house than those who did not. By contrast, those that reported using bed nets were more likely to have mosquitoes in their house than those who did not, potentially due to an overestimated sense of protection or need to use a net because of their presence. There was little reported community organization to control Aedes mosquitos, and social stratum was determined to be a risk factor for mosquito presence. Participants were in favor of interventions by the Health Secretariat, especially insecticide spraying. Our findings identify areas of need for education and engagement initiatives: encouraging community responsibility and day-time bite prevention measures may empower residents to protect themselves better. This can help the Health Secretariat to guide promotion and prevention strategies by knowing the sociodemographic characteristics and popular knowledge of the inhabitants of the city of Restrepo.
Similar content being viewed by others

Introduction
In Colombia, Aedes aegypti mosquitos endemically transmit three arboviruses of significant concern: dengue, chikungunya, and Zika. Understanding the community’s perceptions of these diseases and their associated social and environmental risk factors is crucial for designing effective and sustainable vector control strategies. The Colombian Ministry of Health has identified arboviruses transmitted by Aedes aegypti or Aedes albopictus as a priority public health issue due to the frequency of outbreaks (approximately every three years), the simultaneous circulation of four serotypes of dengue, the presence of Ae. aegypti mosquitos in every region below 2,200 m of elevation, and the potential disability and loss of life due to infection1. All three arboviruses are notifiable diseases in Colombia and are tracked by public health departments2.
There are no arbovirus-specific vaccines or treatments available; although a dengue vaccine is available in some countries, this vaccine is not publicly available in Colombia3. Because of that, the primary focus of disease control programs is on controlling the spread of species of Aedes that are potential vectors of arboviruses. These mosquitos are home-dwellers and prefer oviposition sites like small, standing water containers such as discarded tires and flower pots4. Poor water management practices further encourage their breeding5. As they are primarily daytime biters, traditional bed nets are not effective in preventing bites6. Additionally, socio-economic factors of a household can prevent it from implementing effective mosquito control measures and bettering housing conditions7. Lack of knowledge about oviposition sites, transmission, and protection, can greatly impact the prevalence of dengue and mosquitos in a community, underscoring the need to understand community perspectives and barriers to intervention uptake8.
Multiple vector control methods have been employed by public health authorities in Colombia to control Ae. aegypti and Ae. albopictus, including insecticide spraying and educational campaigns. In response to the 2015 Zika virus outbreak, there was a major insecticide spraying campaign conducted in Villavicencio, the capital city of the department of Meta9. Since then, the Health Secretariat in Meta has focused primarily on educational campaigns for arbovirus control, including going door-to-door in at-risk communities, to teach about the importance of emptying and cleaning water tanks to prevent mosquito growth10. However, the success of any mosquito control program relies on high acceptability and compliance by the target community, especially when the intervention occurs within the home11. Research in communities where vector control programs are to be implemented can illuminate current practices and identify barriers to effective implementation. Discussion with community members may also provide insight into acceptability of proposed interventions and reveal any education that may be required for long-term sustainability of the proposed program. These kind of studies, therefore, provide an important link between studies of efficacy of new vector control strategies and the communities where they are to be implemented.
Here, we examine the perceptions of community members and the relationship between participants and the social and environmental risk factors that make them more susceptible to dengue and mosquito presence. By identifying these factors, the study aims to address critical gaps in the implementation of community-based mosquito control strategies, ensuring interventions are both acceptable and sustainable.
Methods
This study employed a convergent parallel mixed-methods design. Quantitative and qualitative data were collected in the same time frame and analyzed independently. The findings from both data types were synthesized to draw conclusions about community perceptions, social and environmental risk factors, and their relationship to mosquito presence and dengue risk.
Study area
Restrepo is a town of approximately 18,000 residents12. It is located approximately 15 km from Villavicencio, the capital city of Meta department and the main hub for health services in the region. It has an elevation of approximately 480 m (1,580 feet) above sea level and a Tropical monsoon climate, with consistently high temperatures and significant humidity throughout the year. Average high temperatures are around 29 °C, and average low temperatures are approximately 15 °C. Relative humidity varies throughout the year, with averages ranging from approximately 62% in February to 81% in May13.
Restrepo was chosen as a location for the project due to its historically high burden of arbovirus infection14. The rainy season lasts from approximately May to October, with a higher incidence of arbovirus infections typically reported at the start of the wet season during epidemic years15. For this study, Restrepo’s urban areas were divided into five zones: South Oriental, North Oriental, North Occidental, Occidental, and Downtown (Fig. 1).

Restrepo municipality with the zone division used for the study.
Questionnaire sample size estimation
The sample size estimation formula by proportions in a finite set was used to determine the number of participants needed for the questionnaires. The formula was:
where n = sample size; \(\:{Z}_{\frac{\alpha\:}{2}}\) = confidence level (95% or 1.96); p = disease prevalence (50% or 0.5); q = probability of no disease (1-p); N = population size; e = sampling error (5% or 0.05).
A target sample size of 369 people was calculated for recruitment across the municipality. These participants would take part in questionnaire surveys, and a subset of 100 would additionally have mosquitos sampled from their homes to determine mosquito indices. Non-probabilistic sampling was used, with participants chosen in each zone by investigators going door-to-door to recruit people. In addition, residents were invited to take part in focus group discussions (FGDs).
Questionnaire
A structured household questionnaire was used to collect data on sociodemographic variables (stratum, zone, people living at home, use of property, garbage collection, sewage, tap water, water tanks at home), disease variables (whom at the family have had any arbovirus, were they diagnosed by a doctor), and knowledge, attitudes and practices about arboviruses variables that may influence mosquito presence and dengue acquisition by member of a community. The questionnaire was developed specifically for use in this study, and was validated by iterative testing with subject matter experts (authors GIJR and RTJ). Questionnaire face-to-face interviews were conducted in Spanish after written and verbal consent were obtained. The data collectors were trained prior to the interview. The questionnaire was conducted using Google Surveys connected to Google Sheets, with answers recorded on a phone. One member of each household was interviewed, and the information collected belongs to the entire household (group-level). The subsequent analysis is aligned with this unit of observation.
Questionnaire analysis
After collection, the data was checked for accuracy. Missing values were dropped and the “I do not know” answers were recharacterized as missing for questions about past disease acquisition. Responses to ‘yes’ and ‘no’ questions were recoded to be binary. Variables with multiple choice answers were also made binary with the creation of dummy variables. Categorical variables were kept the same. The analysis investigated the various independent variables (social and environmental risk factors) that affect both mosquito presence and dengue acquisition. The two dependent variables were both binary and correlated individually against the different independent variables as both have similar risk factors. All the independent variables were either binary or categorical.
The data was exported into Stata (StataCorp LLC, College Station, TX, 2019, version 16) to understand the distributions among the variables. Missing data and data sparsity were dealt with according to the rule of 10; hence, if a variable had less than 10 responses were excluded from regression analysis. No parameter restrictions were applied due to varying outcome numbers across individual variables. Descriptive analysis was conducted to observe patterns and summarize the variables. Univariate analysis was performed for stratified variables such as zone and stratum of the participants. Bonferroni corrections for multiple tests were applied (for example alpha of 0.05 was lowered to 0.0167 when correcting for 3 tests)16.
Logistic regression analysis was chosen because dependent variables were binary and independent variables were categorical, binary, or originally string data converted into dummy binary variables. Since no data on potential confounders like age or education were collected, no a priori adjustments were made. Multiple-choice questions, such as those regarding mosquito bite protection, were transformed into dummy variables for regression analysis to isolate the effect of individual practices while controlling for other factors. Those variables with fewer than 10 categories were dropped, such as social stratum (only 4 categories) and use of property (1 category). Similarly, missing values were dropped and the “I don´t know” answers were recharacterized as missing for questions about past disease acquisition. Some variables were excluded from analysis by Stata due to collinearity. This program doesn’t return results on which variables were eliminated.
Mosquito data collection
For the first 100 participants, mosquitos were collected from the property of the resident by the Health Secretariat of the Meta department using a mosquito aspirator. The collected mosquitos were sent into the office of the Health Secretariat for identification by an entomologist. Data collected included demographic information on the department (Meta), municipality (Restrepo), neighborhood, block (if applicable), and the address of the property where the collection took place. When mosquitos were collected, they were identified to species (Ae. aegpyti, Ae. albopictus, and Culex spp.) and sex was recorded. The data were used to calculate the House Index (HI) for Ae. aegpyti.
Focus group discussions
Focus group discussions were conducted with residents over 18 years old of Restrepo. A discussion guide was written and a semi-structured interview setup was followed to ensure consistency between groups (Supplementary Materials). Participants were asked to sign written consent forms. Participants were also asked to complete a short questionnaire with demographic information. Each discussion lasted for approximately one hour. FGDs were conducted with four to twelve participants per session. A total of eight focus group discussions were completed. FGDs were conducted until the responses reached saturation; that is, until the responses became similar between groups. Seven of the eight FGDs were conducted in-person in community locations (meeting rooms, schools), and one session was held online due to the availability of the participants. The in-person nature of the discussions allowed for more natural and informal conversation between participants. Participants were recruited in order to ensure that each zone of the municipality was equally represented.
FGD data collection
Audio recordings of the FGDs were taken and immediately uploaded to a drive. Audio files were processed and transcribed by Descript software (Descript, San Francisco, CA). The software did not capture some important moments and nuances in the discussions, so the transcription files were manually edited.
FGD data analysis
The transcripts were analysed in the original Spanish, although the coding and thematic analysis was completed in English. Each transcript was coded using NVivo (QSR International, Burlington, MA, 2018, version 18). A primarily inductive approach was employed, where codes were generated based on the data itself. Prior to coding, some codes were derived from the focus group discussion guide, while additional codes emerged from unanticipated discussions among participants. Following this, a thematic analysis approach was used to develop themes from the codes identified in the data analysis process17. A triangulation was performed on the qualitative data. SB and EF/GIJR independently reviewed the interview responses to develop themes.
Ethics approval and consent to participate
The project was approved by the Research Committee of the Universidad Cooperativa de Colombia (minute number 005 - May 18th 2021) and the Ethics Committee of Universidad Cooperativa de Colombia (No. BIO190, minute number 002 – June 10th 2021). Additionally, a favorable opinion was provided by the London School of Hygiene & Tropical Medicine MSc Research Ethics Committee: reference numbers 29,051 and 28,862. The study was conducted in accordance with the principles of the Declaration of Helsinki, with the wellbeing and rights of participants being the first consideration. Additionally, the handling of information and its confidentiality, adhered to the provisions outlined under Colombian law Resolution 8430 of 1993. No vulnerable group was involved in the research. Written informed consent was obtained from all participants, ensuring voluntary participation and confidentiality.
Results
A total of 149 participants were recruited for the questionnaire survey, and of these 100 also had their properties inspected for mosquitos. The number of participants varied by zone. Many of the participants used their property for residential purposes and 67 of the 100 houses checked were positive for mosquito presence. Public goods like sewage, garbage, and portable water were used by more than 90% of the participants. In terms of people’s knowledge, 110 (73.8%) participants knew that the bite of a mosquito spreads dengue, chikungunya, or Zika; 57 (38.3%) participants said that mosquitos bit them all hours of the day. Out of the 149 participants, 35 (23.5%) said that they or someone in their family had previously contracted dengue.
In response to the question about how to prevent dengue, chikungunya, or Zika, 89 (59.7%) participants knew that eliminating mosquito oviposition sites was important and 58 (38.9%) knew about fumigation. When asked about how to eliminate mosquito oviposition sites, 112 (75.2%) participants knew to eliminate standing and collected water, 60 (40.3%) suggested to fumigate, and 32 (21.8%) suggested to clean out the water tank. The most common “other” answer suggestion was using Clorox® disinfectant to clean. Just over half (78, 52.4%) of respondents knew that mosquitos lay eggs and develop in water but could not specify the type of water; approximately one third (52, 34.9%) thought that this happened in dirty standing water, and slightly fewer (47, 31.5%) thought of clean standing water. Since these were multiple choice answers, people could have picked more than one answer.
In terms of practice, 95 (63.8%) claimed to fumigate in their home to protect themselves from mosquito bites, 58 (38.9%) used bed nets and 58 (38.9%) eliminated breeding grounds. With regards to ideas about the entity responsible for eliminating mosquito oviposition and development sites, most of the people believed that every person and their family was responsible for their own elimination, 115 (77.2%).
We established two dependent variables for the analysis – mosquito presence in residence and dengue history of participant or someone in their household. In the 100 houses that were checked for mosquitos, 67 were deemed positive; 28.4% of them were in stratum one, the lowest stratum; 44.8% were in stratum two, 26.9% were in stratum three and 0% for stratum four. Based on a simple analysis without adjusting for confounders, being of stratum two and three could be a protective factor against the presence of mosquitoes in their houses in comparison with stratum one (Table 1).
None of the zones were as likely to have mosquitos than the Downtown houses; all their 95% CIs crossed 1 and none of their p-values were under 0.05.
Out of the 65 people that had mosquitos found in their house, 54 (83.1%) also had a water tank. However, participants with a tank were 0.32 times as likely (95% CI: 0.07–1.52; p-value: 0.151) to have mosquitos than those without a tank (Table 1).
In the 149 participants that were asked about dengue history in the past few years, only 35 (23.7%) participants said that they or someone in their family had contracted the disease. Out of those 35 households, 4 (11.4%) were in stratum one, 13 (37.1%) in stratum two, 16 (45.7%) in stratum three, and 2 (5.7%) in stratum four. For dengue, an increase in stratum was associated with an increase in the odds of dengue acquisition. Those in stratum three were 2.23 times as likely to have had dengue than those in stratum one. Out of the 35 participants, 26 (74.3%) had tanks and those with a tank were 0.90 as likely to acquire dengue than those without a tank. Six (17.1%) of the 35 houses were in the Downtown, 9 (25.7%) in the North Occidental, 7 (20.0%) in the Occidental, 8 (22.9%) in the North Oriental, and 5 (14.3%) in the South Oriental. With Downtown being the base, participants in other zones were generally less likely to have had dengue than participants in the Downtown. However, all these odds ratios had p-values over 0.05 and 95% CI crossing 1, so none of these were considered significant.
For mosquitos as the dependent, a logistic regression performed for association between mosquito presence and knowledge of disease (dengue, chikungunya, and Zika) prevention indicated that those that know about elimination of mosquito oviposition sites were 0.31 times as likely (95% CI: 0.09–1.10; p-value: 0.070) to have mosquitos than those that do not know about oviposition site elimination. Participants that thought destroying objects that collect water prevents dengue were 2.81 times more likely (95% CI: 0.78–10.15; p-value: 0.114) to have mosquitos than participants that did not think so.
As for information about elimination of oviposition sites, participants that knew of cleaning their water tank were 0.28 times as likely (95% CI: 0.09–0.85; p-value: 0.024) to have mosquitos than those who did not know this information. Those with knowledge of eliminating standing and collected water were 0.34 times (95% CI: 0.10– 1.08; p-value: 0.067) as likely to have mosquitos as participants who did not know this knowledge. Those that were aware of sweeping and disposing of trash were 9.86 times (95% CI: 1.54–63.27; p-value: 0.016) as likely to have mosquitos as those with no such information.
In terms of knowledge about where mosquitos reproduce, those that thought mosquitos lay eggs in clean standing water were 0.42 times as likely (95% CI: 0.11–1.60; p-value: 0.206) to have mosquitos as those that did not. Participants with knowledge of mosquitos laying eggs in dirty standing water were 1.45 times as likely (95% CI: 0.40–5.24; p-value: 0.572) to have mosquitos than those that did not. Regarding responsibility, those who believed that every person and family is responsible for eliminating mosquito oviposition sites were 0.66 times as likely (95% CI: 0.16–2.69; p-value: 0.564) to have mosquitos in their residence than those who did not. None of these results had p-values indicating statistical significance.
Lastly, participants that reported use of bed nets were 2.73 times as likely (95% CI: 0.98–7.63: p-value: 0.055) to have mosquitos than those who do not use the net. Participants that use screens on their doors and windows were 0.04 times less likely (95% CI: 0.002–0.88: p-value: 0.042) to have mosquitos that do not use the screens.
For dengue as the dependent, several logistic regressions were performed for association between dengue and various variables; however, due to the small number of individuals who reported having dengue in their family (only 35 participants), most results had wide confidence intervals and p-values above 0.05. The most notable variables from each question were: for knowledge about dengue prevention, those that knew of fumigation were 1.87 times as likely (95% CI: 0.77–4.59; p-value: 0.168) to have had dengue as those that did not. For knowledge of eliminating mosquito oviposition sites, those that knew of eliminating standing water were 0.37 as likely (95% CI: 0.13–4.71; p-value: 0.071) to have acquired dengue than those that did not.
Unlike mosquito presence, the only variable option with some statistical significance was that people that used bed nets to protect themselves from mosquito bites were 2.30 more likely (95% CI: 1.03–5.17; p-value: 0.043) to contract dengue than those who did not. However, this result was not statistically significant after adjusting for multiple testing (Table 2).
The odds ratios, p-values and confidence intervals for all the different options for both mosquito presence and dengue acquisition as dependent variables are present in Table 2; however, most of the responses have 95% CIs that cross 1 and/or are very wide due to the small sample size, and the p-values are much larger than 0.05. Lastly, using the number of mosquitos collected and the formula above, the general house index in Restrepo was calculated to be 67% for all mosquitos and 27% for Aedes aegpyti mosquitos.
Focus group analysis
There were 44 participants taking part in FGDs. There were approximately double the number of women interviewed as men and the mean age was 53.4 (± 16.4) years old. The majority of participants reported socio-economic stratum two and three. Approximately half of participants had experience with arbovirus infection (either themselves or a family member); 17 (39%) had experience with a dengue infection.
After analysis, participants’ responses were evaluated and organized into key themes (Table 3). Theme generation followed Braun and Clarke’s six phases for thematic analysis18 A preliminary coding framework was established from the topic guide and some themes emerged as expected from this guide (for example, knowledge about arbovirus infection symptoms), while some emerged organically during discussions. Reflexivity was maintained throughout the analysis process, with the research team regularly discussing potential biases and interpretations. Themes were collaboratively refined to ensure consistency and alignment with the study’s objectives. The Health Belief Model (HBM) was used as a theoretical framework to understand participants’ beliefs about arbovirus infections, including perceived susceptibility, severity, benefits, and barriers to control measures19.
1. Technical knowledge and perception of arbovirus infection
Infection symptoms
In every FGD, at least one participant had personal experience of arbovirus infection. Dengue was the most common arbovirus infection discussed. Symptoms mentioned included fever, pain in the body, head, and stomach, and low platelet count. Some participants shared their experience of being hospitalized for treatment. Many participants described their symptoms as “duro” or “fuerte” (hard, strong). Some participants described a distinction between dengue fever and hemorrhagic dengue (more severe). Multiple participants had been hospitalized due to a sustained high fever or low platelet count.
Chikungunya was also described multiple times as having intense joint pain; for some participants, this pain and/or additional sequelae lasted for years after initial infection.
“Pain, a lot of pain. Personally, my joints [hurt] very strongly. I could not walk or even move my body.” (FGD1).
Participants of one FGD perceived chikungunya infection as more severe than dengue or Zika infection. This FGD included one person who had experienced a co-infection of dengue and chikungunya viruses; the health department became involved and conducted a spraying campaign around their house, perhaps adding to the perception of chikungunya as being very serious.
In general, knowledge about symptoms of arbovirus infection was widespread and accurate. Participants viewed the symptoms as difficult to endure and with potentially long-lasting effects. Some people had experienced infections more than once. Overall, there was a common thread that arbovirus control should be taken seriously due to the risks of infection. Participants in one FGD had knowledge of the dengue outbreak occurring at the time and the strain that it is causing in hospitals in the region, but most groups were unaware of the epidemic in Meta.
Transmission and prevention strategies
There was a spectrum of knowledge about arbovirus transmission that ranged from completely incorrect to a detailed understanding of the species of mosquito responsible for transmission. Two people believed that arboviruses are transmitted via having a conversation with or being near someone who is ill, although they were quickly corrected by other members of the FGD. Nevertheless, most participants knew that arboviruses are transmitted by mosquitos. A couple could identify the scientific name for Ae. aegypti and/or understood how to recognize Aedes by the black and white stripes on their legs.
One participant linked arbovirus transmission specifically to the cleanliness of their house and outdoor space. In every FGD, participants mentioned the presence of water as a contributing factor to arbovirus transmission in their communities. Some made an explicit connection between understanding that mosquitos are responsible for transmission and the presence of standing water:
“[Transmission] has to do, for example, with the sources of still water, stagnant water, which is where [the mosquitos] are… in stagnant but clean water in the tanks […]; the little mosquito larvae are there.” (FGD2).
“I know [that] in tanks of clean water, not in dirty water but in clean water, they reproduce in these waters.” (FGD6).
These specific connections were made by participants in FGDs with a higher average stratum, suggesting that those in a higher socioeconomic bracket may be more likely to have detailed knowledge about arbovirus transmission.
Even without the specific connection between mosquito larvae and standing water, most participants understood that water contributes to transmission. Some additionally made the clarification that it is standing and/or clean water that is the greatest risk. However, there was some confusion about other sources of water and whether they could also be responsible for transmission. There were multiple mentions of the “caños” (pipes) that surround communities in Restrepo. People were worried that mosquitos might congregate around those pipes. Some wished that the health authorities were more proactive about dealing with these sources of mosquitos. There was also a connection between the amount of rain and arbovirus transmission; people believed that in the rainy season, there are more mosquitos and more transmission.
Most participants were aware of the need to monitor water deposits as a method to prevent arbovirus transmission. For participants living in urban Restrepo, there was significant discussion about the need to keep water tanks clean. Municipal water access can be sporadic in Restrepo, so nearly every household collects rainwater in large tanks for periods of time when there is no piped municipal water available. Most FGD participants were aware that these tanks are a risk for arbovirus transmission. Most participants, when asked, said that one of the main things they do to prevent arbovirus transmission in their household was to clean water tanks. Chlorine tablets, boiling water, and keeping water tanks covered were mentioned as good options maintaining clean tanks. However, when talking about water as a source of transmission, there was very little discussion of other water sources as potential oviposition sites. The fact that Aedes larvae can hatch and develop in puddles as small as a discarded eggshell was met with surprise. One group requested that after the conclusion of the FGD, we take a quick walk outside to help identify such sites.
Most of the FGDs were conducted with participants who live in urban Restrepo. However, one FGD that was conducted with participants who live in rural neighborhoods near Restrepo, and revealed that these participants had a greater understanding of the many sites that can be used for egg laying by Aedes mosquitos.
“It is not that easy to control [mosquitos] in towns. Because if you have a tank […] it is easy to control –.
[The tanks] are smaller.
– but in the countryside, it is not easy. Water gets deposited easily around.” (FGD7).
The rural FGD participants discussed less the need to keep water tanks clean and more the need to find and eliminate ovisposition sites near their houses. There was occasionally some confusion between Aedes and Anopheles mosquitos and the difference between arboviruses and malaria parasites (malaria is also present in the department of Meta). Some participants had knowledge about mosquito-transmitted diseases in general, rather than the specifics of different infections and corresponding differences in control strategies. For example, some participants mentioned sleeping under mosquito nets as a method of arbovirus infection prevention; this is effective for malaria, but not arboviruses.
The two most commonly mentioned methods of arbovirus control were: (1) dealing with water sources (as a surrogate for eliminating oviposition sites), and (2) “fumigation” (insecticide spraying). Every FGD mentioned fumigation as a key method of arbovirus control. Some participants purchased insecticides from stores to spray in their houses; others had experiences with the health authorities coming to spray their houses for them. Fumigation was also seen as a good option to control other nuisance insects like flies.
Beyond eliminating oviposition sites and fumigation, participants reported using a variety of other methods to prevent arbovirus infection. Some reported wearing insect repellent during the day, some use electric rackets to kill mosquitos flying near them during the day, some keep their windows closed to prevent mosquitos from entering their homes. Others employ atypical methods, such as keeping egg cartons near the bed, having a smoky fire, employing a cat to eat mosquitos, eating a specific diet (spinach, lentils, onions, mineralized salt, and/or fat from animal skin), and spraying vinegar. Each of these home remedies was mentioned once. In general, most FGD participants did something to prevent arbovirus infection, and only a couple of participants did nothing for arbovirus infection control.
2. Perception of vector control programs
Issues with prevention strategies
Although participants reported widespread awareness of strategies for arbovirus infection control, some concerns were raised, mostly about fumigation. Some participants raised concerns about the toxicity of fumigation, both inside the house (to people), and to the environment if used outside the house. A major problem with continuous insecticide use is the establishment of insecticide-resistant mosquito populations. When prompted, a few participants were able to name “resistance” as an issue, although most had not thought of this issue before the discussion. One FGD mentioned resistance indirectly:
“But [insecticide spraying] didn’t do any good. That was sweet for [the mosquitos].
That’s the problem. With the secretary going around spraying….
It didn’t do any good.” (FGD6).
The cost of purchasing insecticides from grocery stores was high and was cited as a barrier to routine use. The cost of a bottle of insecticide was reported as ranging from $15,000 to $80,000 COP (approximately £3–15). The perceived barriers construct of the HBM was evident here, with participants feeling that access to fumigation is not sufficiently available or affordable Consequently, many participants wanted the health authorities to come to fumigate their homes and some described specifically requesting fumigation from health authorities.
“[The Health Secretariat] did not come back [to fumigate]?
No.
If we want [fumigation], we have to pay.
Exactly.” (FGD5).
Vector control programs
When asked what a vector control program is, none of the FGD participants were familiar with this term, but some of them could infer its purpose: to reduce the number of mosquitos, fumigation being the method most commonly mentioned. The perception was that these programs were always carried out by health authorities. Some participants linked these official vector control programs to specific times of year or specific outbreak scenarios:
“I know it’s a certain time of the year, I think in the time when summer ends and winter starts, that they start those campaigns, because that’s when they are going to see […] that mosquito proliferation.” (FGD4).
While there was acknowledgement that these programs are important, one participant expressed that they did not believe the programs are sustainable.
Responsibility for vector control programs
A major line of inquiry in our investigation was the question “Who do you think should be responsible for controlling vectors (mosquitos) in your community?” Broadly, there were three responses: the Health Secretariat and other government bodies, the community, and each individual person. However, there was overlap and interplay between these three responses. Many participants agreed that arbovirus and mosquito control begins at the household level, specifically with ensuring that water tanks are clean.
“I think that everyone [should be responsible].
Every family.
Every house.” (FGD7).
This highlights the HBM’s perceived susceptibility construct – the perceived susceptibility of the risk of arbovirus infection, as participants acknowledged the importance of preventing mosquito proliferation at the individual level. This is also a key factor influencing the perceived benefit of taking preventive actions.
The secretary of health was mentioned multiple times as an important player in mosquito and arbovirus control. Some believed that vector control is solely the responsibility of the Health Secretariat, while others said that it should be a shared effort:
“In general, it is the Health Secretariat’s responsibility, but it is the responsibility of each one of us to keep clean tanks and not to leave stored water [around]. [agreement from other participants]” (FGD5).
Multiple participants expressed a strong desire for the Health Secretariat to come to fumigate their houses. When participants had experienced campaigns by the health authorities, this was overwhelmingly seen as positive by those who described it and others listening in the discussion. In addition to fumigation campaigns, participants expressed a desire for educational materials to be provided by the Health Secretariat.
One FGD participant commented that they believe that the efforts of the Health Secretariat are not sufficient. Typically, when participants were told that the Health Secretariat is under significant pressure from the 2023 dengue outbreak and does not have time to conduct mass fumigation campaigns in areas that are not an epidemic priority, participants were disappointed. This frustration with the lack of government support aligns with the perceived barriers concept in HBM. However, some did see it as a call to action to work together as a community instead and were then more likely to agree that the responsibility for vector control should be at the community and individual levels.
When asked about whether there was any coordination for arbovirus control at the community level, most respondents reported none. Part of that was due to a perceived lack of support from authorities and experts. Nevertheless, many participants expressed a desire to work together to approach the problem of mosquito control. One barrier may be the lack of support from external sources; one participant expressed that their compound’s participation in our study was one way that they were working to improve arbovirus control in their community.
“The truth is that at the community level on this subject [vector control], there are no education programs. I would like [programs]. […] I would need to [work] with the universities.” (FGD2).
“We are on the same team because we are in the same environment.” (FGD3).
Concern about neighbors
Following the comments that each person should be responsible for their own house, concerns were raised about the adherence of neighbors to the same standard. This came up most frequently during discussions of taking care of water tanks.
“But there are people that have tanks that are green [with algae]. And they do not wash them.” (FGD3).
Participants recognized that without broader community engagement, their efforts might be undermined, thus enhancing their perceived susceptibility to arbovirus infection. A couple of questions were asked about how to approach this situation, and what to do if, for example, your neighbor goes away for a long period of time and leaves their water tank uncovered. Some participants also expressed that there were people in their community who simply did not understand or know the risks associated with mosquitos or the necessary prevention measures, highlighting the need for more community education. This connects to the perceived benefits of engaging in mosquito control efforts at a collective level. The concern straddles the line between individual and community responsibility; while participants believed that they had a duty to keep their property clean, they were aware that without greater community mobilization, they would still be at risk of infection.
3. Relationship to authorities
Treatment seeking
Multiple participants expressed that accessing medical care in Restrepo can be challenging. Although everyone who had a severe arbovirus infection had received medical and/or public health attention, there was still frustration with the medical establishment and general reluctance to go to the doctor. Participants referenced long wait times, frustrating bureaucracy, and the dangers of acquiring other infections in hospitals. One participant mentioned the “matrimonio” – a cocktail of drugs readily available without prescription in Colombian pharmacies. It can be incredibly dangerous if given to a patient with a dengue virus infection, as it can cause a sudden drop in platelet count20. The matrimonio is a common remedy sought by ill people when they want to avoid going to the doctor. Another participant said that they have some medical supplies at home and prefer to treat their family at home whenever possible. There was also some confusion about why doctors could only prescribe acetaminophen for arbovirus infections.
Prevention control programs
As an extension of the perception that the secretary of health should be at least partly responsible for arbovirus control, multiple participants expressed that they were unsatisfied with current government efforts. Requests to the Health Secretariat for fumigation that were denied were met with disappointment; multiple participants asked the study investigators whether the Health Secretariat would be coming to fumigate. Regardless of the perceived efficacy of the Health Secretariat’s programs (which ranged from good to unsustainable), participants still wanted the Health Secretariat to come and carry out vector control programs in their communities. There was high demand, especially for fumigation campaigns. More broadly, some participants perceived government programs for public health in general to be insufficient.
“The programs exist, but they exist on paper [only].” (FGD2).
“They spend their time putting out fires, this is how all administrations work, from the national, departmental and municipal levels, regardless of whether or not there is a regulation that obliges them to maintain a defined policy. Regarding specifically health issues, and other areas.” (FGD4).
An additional concern was insufficient numbers of full-time employees; the Health Secretariat typically employs workers on short-term contracts, so it can be difficult to maintain sustainable long-term programs.
4. Dangers of a lack of knowledge
“Desconocimiento,” or a lack of knowledge, was brought up multiple times as a barrier to effective vector control, and as danger to people. It affected health-seeking behaviour; some participants believed that in the current healthcare system, patients need to be able to advocate for themselves in order to receive adequate care.
“One as a patient can also teach the doctor ‘send this test’” (FGD1).
This concern highlights the perceived susceptibility to more severe health outcomes, with participants emphasizing the importance of being informed. If patients do not have enough knowledge about their condition, they cannot properly advocate for themselves, which can be very dangerous. A lack of knowledge was also seen as a barrier to community mosquito control. Participants discussed how their neighbors perhaps did not have enough knowledge about how to keep their properties clean, and how this can affect the community as a whole.
Discussion
Arbovirus infections are a growing public health problem in Colombia. It is crucial that new control methods are implemented thoughtfully and with consideration to the community’s needs. According to our results, low socioeconomic status proved to be the biggest risk factor of mosquito presence in a residence in Restrepo. Those in higher strata are expected to be able to afford better housing conditions and control measures, and evidence that the poorest communities have higher abundances of Aedes has been reported extensively in other settings21,22. Many results indicate that infestation levels for both Aedes species vary between neighborhoods of different socioeconomic levels, being higher in neighborhoods with a lower percentage of residents with a college degree and lower monthly family income23. However, there can be conflicting factors at play in both neighborhood-level and household-level determinants of Aedes presence. For example, neighborhoods with higher disease incidence may be targeted more frequently municipal control activities and so fewer mosquitos may be found in these settings at the time of sampling, and in some wealthier households, landscaping and vegetation that are absent in other areas could support higher Aedes populations24.
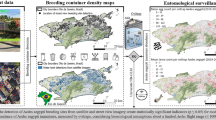
We did not find statistical support for one region of Restrepo having more mosquitoes than any other, but more extensive sampling may have allowed hotspots to be identified, and this would allow for targeted vector control activity and identification of predictors associated with Aedes densities. Various studies establish that seasonal climatic variation, vegetation height, human population and land cover determine the species of Aedes that remain in a given area23. Spatial mapping of disease cases also allows for the stratification of arbovirus transmission risk within urban areas, and can guide the implementation of surveillance and vector control. This can be combined with the creation of digital platforms that allow all the necessary data to be organized and gathered, making it available online as a geographic map of the data set25.
With regard to knowledge, participants that knew to eliminate mosquito oviposition sites to prevent dengue were less likely to have mosquitos than those that did not know such information. Similarly, those that knew of cleaning their tanks to eliminate these sites were less likely to have mosquitos than those who did not. Even though knowledge does not equate to practice, it is a prerequisite for taking appropriate actions to reduce the burden of mosquitoes in their domestic environment. Consequently, it is crucial to evaluate the municipality’s campaigns, communication strategies, and educational initiatives to ensure that the information provided is effectively translated into behavioral changes and leads to a reduction in these diseases26,27,28.
Unsatisfactory knowledge, attitudes, and practices at the population level are related to heightened risk of transmission. These issues can only be overcome with education and social mobilization tailored to local cultural and linguistic contexts, which are richly diverse in all countries in Latin America and have previously been identified as a potential challenge to effective community participation in Colombia29. In nearby Villavicencio, investigators found similar results to this study: over half of respondents understood that dengue is transmitted by a mosquito bite, but most could not name or identify Aedes aegypti, nor could they say the time of day at which they bite30,31. Also, consistent with our findings, the investigators found that a majority of respondents linked mosquito reproduction to standing water (80–90%); most also washed their water tanks at least once per week (73–87%). However, when asked if they participate in actions to prevent dengue in their neighborhood, 96% said that they do not30. Investigators also found a correlation between education level of the respondent and prevention activities, with those reporting little education more likely to have larvae present around their house31.
In Villanueva, in the department of Casanare, investigators also found that most respondents were aware of arbovirus infections and their associated symptoms32. When asked how to control Aedes species, respondents understood the importance of eliminating breeding sites and frequently mentioned fumigation. Similar to our findings, respondents also most commonly answered “fumigation” when asked what the Health Secretariat should be doing to control arboviruses. As with elsewhere in Latin America, our focus group participants stressed an important role of the state in protecting people from mosquitoes33,34,35. The communities have ignored this problem a little since they have normalized the presence of VBDs in their environment, which lowers the guard in the prevention measures that are specific to the populations and not to the Health Secretariat29.
There is limited evidence for the effectiveness of interventions against dengue36, but many studies have investigated the impact of interventions on mosquito counts or larval indices37. Screens on doors can prevent mosquitos from entering houses, while bed nets are not expected to have this effect; rather, they prevent mosquitos from biting people sleeping at night. Our finding that reported bed net usage increased the odds of mosquito presence inside the house suggests that some residents may opt for the use of a bed net rather than an intervention that prevents mosquito entry. This should be discouraged because of the daytime biting nature of Aedes. Indeed, there was a similar increase in the odds of being in a household with a previous dengue case when bed nets are used for protection (2.30 more likely to be in a dengue household than if bed nets are not used). However, it should be noted that these finding were not statistically significant.
Colombia’s politically verticalized and chemical-dependent model for vector control and needs to incorporate long-term strategies to abate socio-environmental vulnerability. As suggested by the Health Belief Model, understanding both the perceived susceptibility and barriers to engaging in vector control actions within the community is crucial for crafting effective interventions33. Unsatisfactory knowledge, attitudes, and practice at the population level are related to heightened risk of transmission and can only be overcome with education and social mobilization adapted to local cultural and linguistic contexts, which are richly diverse in all countries in Latin America.
Our study was limited by a relatively small sample size. Trapping for mosquitos in more houses may have allowed new associations to be identified or for others to have been supported with statistically significant results. Another limitation is that the inhabitants were not very receptive to the project and many did not want to participate, which meant that a lot of data was lost as we could not enter the houses. We note that the quantitative results are exploratory and that no information on confounding factors, which might influence the analyses, was collected.
Conclusion
For many years, control strategies have been established to reduce epidemic crises caused by vectors, especially in areas where temperatures and the environment predispose to an increase in the number of positive cases. Considering this, it is of great importance to understand the knowledge, perception, and practices of communities related to vector control to gain new perspectives and make modifications to the strategies currently in use, which do not seem to be showing positive results in terms of reducing both the vector and the diseases it transmits.
The use of the Health Belief Model as a framework for designing community interventions could assist in identifying and addressing the key barriers to participation in vector control programs. The Health Secretariat must change communication strategies with the community so that they feel they are not only part of the problem but also part of the solution, and that a large part of the success or failure of the control programs of these vectors is in them. The inclusive participation must be improved through and proper planning and implementation of novel educational interventions amongst populations.
Data availability
The datasets generated and/or analysed during the current study are not publicly available due to the recordings contain personal and sensitive information of the interviewees but are available from the corresponding author on reasonable request.
References
Instituto Nacional de Salud. Informe Técnico Entomológico de Arbovirus, Colombia 2018 [Internet]. Bogotá, Colombia: Instituto Nacional de Salud; 1–14. Available in: (2018). p https://www.ins.gov.co/BibliotecaDigital/informe-tecnico-entomologico-arbovirus-2018.pdf.
Instituto Nacional de Salud. Boletín Epidemiológico Semanal, semana epidemiológic 30, 21 al 27 de julio de 2019 [Internet]. Bogotá, Colombia: Instituto Nacional de Salud; 2019 [cited octobre 2023] pp. 1–30. Available in: https://www.ins.gov.co/BibliotecaDigital/Boletin-epidemiologico-semana-30-2019.pdf.
Thomas, S. J. & Yoon, I. K. A review of Dengvaxia®: development to deployment. Hum. Vaccines Immunother. 15 (10), 2295–2314 (2019).
Diéguez-Fernàndez, L. et al. Updating the breeding sites of Aedes aegypti (Diptera: Culicidae) in Camagüey, Cuba. Interam J. Med. Health [Internet] 24 de junio de 2024 [cited 25 octobre 2024];7. Available in: https://iajmh.com/iajmh/article/view/260.
Ferede, G. et al. Distribution and larval breeding habitats of Aedes mosquito species in residential areas of Northwest Ethiopia. Epidemiol. Health. 40, e2018015 (2018).
Buonomo, B. & Della Marca, R. Optimal bed net use for a dengue disease model with mosquito seasonal pattern. Math. Methods Appl. Sci. 41 (2), 573–592 (2018).
Zellweger, R. M. et al. Socioeconomic and environmental determinants of dengue transmission in an urban setting: An ecological study in Nouméa, New Caledonia. PLoS Negl. Trop. Dis. 11(4), e0005471 (2017).
Stewart Ibarra, A. M. et al. Dengue Vector Dynamics (Aedes aegypti) Influenced by Climate and Social Factors in Ecuador: Implications for Targeted Control. PLoS ONE. 8(11), e78263 (2013).
Garcia, C. Continua fumigación contra El Zika En Colombia. Assoc. Press. ;1. (2016).
Alcaldía de Villavicencio. Campaña de sensibilización del dengue realizó la Secretaría Local de Salud en el barrio Kirpas [Internet]. Sala de Prensa. 2019 [cited 25 octobre 2024]. Available in: https://historico.villavicencio.gov.co/NuestraAlcaldia/SalaDePrensa/Paginas/Campa%C3%B1a-de-sensibilizaci%C3%B3n-del-dengue-realiz%C3%B3-la-Secretar%C3%ADa-Local-de-Salud-en-el-barrio-Kirpas.aspx.
Montenegro-Quiñonez, C. A. et al. Interventions against Aedes/dengue at the household level: a systematic review and meta-analysis. eBioMedicine 93, 104660 (2023).
Censo Nacional de población y vivienda 2018-Colombia [Internet]. DANE & Bogotá Colombia: DANE; [cited 23 august 2023]. Available in: (2019). https://sitios.dane.gov.co/cnpv/#!/donde_estamos.
Restrepo climate summary [Internet]. [cited 10 January 2025]. Available in: https://weatherandclimate.com/colombia/meta/restrepo?utm_source=chatgpt.com.
Secretaría de Salud del Meta. Boletín epidemiológico, semana 29 [Internet]. Villavicencio, meta, Colombia: secretaría de Salud Del meta; 2023 [cited 5 June 2024]. Available in: https://devx.meta.gov.co/media/centrodocumentacion/2023/08/09/Boletin_Dengue_a_SE_29.pdf
Gutierrez-Barbosa, H., Medina-Moreno, S., Zapata, J. C. & Chua, J. V. Dengue infections in Colombia: epidemiological trends of a hyperendemic country. Trop. Med. Infect. Dis. 5 (4), 156 (2020).
Abdi, H. Bonferroni and Šidák corrections for multiple comparisons. En: Encyclopedia of Measurement and Statistics. Thousand Oaks: Sage; 103–107. (2007).
Maguire, M. & Delahunt, B. Doing a thematic analysis: A practical, step-by-step guide for learning and teaching scholars. AISHE-J 9 (3), 3351–33514 (2017).
Braun, V. & Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 3 (2), 77–101 (2006).
Rosenstock, I. M., Strecher, V. J. & Becker, M. H. Social learning theory and the health belief model. Health Educ. Q. 15 (2), 175–183 (1988).
Valarezo-Sevilla, D., Pazmiño-Martínez, A., Sarzosa-Terán, V. & Acuña-Santana, P. Dengue y Uso de Anti-inflamatorios no esteroideos: estudio observacional. Correo Científico Méd. 20(3), 531–538 (2016).
Whiteman, A. et al. Aedes mosquito infestation in socioeconomically contrasting neighborhoods of Panama City. EcoHealth 16 (2), 210–221 (2019).
Donnelly, M. A. P., Kluh, S., Snyder, R. E. & Barker, C. M. Quantifying sociodemographic heterogeneities in the distribution of Aedes aegypti among California households. PLoS Negl. Trop. Dis. 14(7), e0008408 (2020).
Myer, M. H. et al. Mapping Aedes aegypti (Diptera: Culicidae) and Aedes albopictus Vector Mosquito Distribution in Brownsville, TX. J. Med. Entomol. 57(1), 231–240 (2020).
Talbot, B. et al. Determinants of Aedes mosquito density as an indicator of arbovirus transmission risk in three sites affected by co-circulation of globally spreading arboviruses in Colombia, Ecuador and Argentina. Parasit. Vectors. 14 (1), 482 (2021).
Dzul-Manzanilla, F. et al. Identifying urban hotspots of dengue, Chikungunya, and Zika transmission in Mexico to support risk stratification efforts: a Spatial analysis. Lancet Planet. Health. 5 (5), e277–e285 (2021).
Jaramillo Ramírez, G. I. & Álvarez, L. S. B. Knowledge, attitudes and practices regarding dengue, Chikungunya, and Zika and their vector Aedes aegypti in Villavicencio, Colombia. Open. Public. Health J. 10 (1), 80–89 (2017).
Selvarajoo, S. et al. Knowledge, attitude and practice on dengue prevention and dengue Seroprevalence in a dengue hotspot in Malaysia: A cross-sectional study. Sci. Rep. 10 (1), 9534 (2020).
Soria, C., Almirón, W. R., Stewart-Ibarra, A. M. & Crocco, L. B. Systematic review of impacts of educational interventions to control breeding sites of Aedes aegypti and Aedes albopictus mosquitoes. Am. J. Trop. Med. Hyg. 110 (5), 979–988 (2024).
Jaramillo-Ramirez, G. I. et al. A qualitative analysis of the perceptions of stakeholders involved in vector control and vector-Borne disease research and surveillance in Orinoquia, Colombia. Trop. Med. Infect. Dis. 9 (2), 43 (2024).
Moreno-Giraldo, I. C. & Reyes-Cubillos, P. A. El dengue en las familias de los barrios de la comuna cuatro de Villavicencio, Colombia. Bol Semillero Investig En Fam [Internet]. 12 de enero de 2023 [cited 25 octobre 2024];4(2). Available in: https://revistas.unillanos.edu.co/index.php/bsif/article/view/820.
Hernández Cristancho, L. J. & Salamanca Ramos, E. Conocimientos, actitudes y prácticas Respecto al dengue En familias de La Comuna Uno, Villavicencio – Colombia. Rev. Colomb Cienc. Soc. 14 (1), 238–253 (2023).
Castañeda, O., Segura, O., Lara, E. & Manosalva-Sánchez, C. Conocimientos, actitudes y prácticas Frente al control Del vector Aedes aegypti, Villanueva- Casanare, Colombia, 2016. Rev. Médica Risaralda. 23 (1), 13–21 (2017).
Bancroft, D. et al. Vector control strategies in Brazil: a qualitative investigation into community knowledge, attitudes and perceptions following the 2015–2016 Zika virus epidemic. BMJ Open. 12 (1), e050991 (2022).
Sánchez-González, L. et al. Assessment of community support for Wolbachia-mediated population suppression as a control method for Aedes aegypti mosquitoes in a community cohort in Puerto Rico. PLoS Negl. Trop. Dis. 15(12), e0009966 (2021).
Pérez-Guerra, C. L. et al. Community perceptions on challenges and solutions to implement an Aedes aegypti control project in Ponce, Puerto Rico (USA). PLOS ONE. 18(4), e0284430 (2023).
Bowman, L. R., Donegan, S. & McCall, P. J. Is Dengue Vector Control Deficient in Effectiveness or Evidence? Systematic Review and Meta-analysis. PLoS Negl Trop Dis. 10(3), e0004551 (2016).
Manrique-Saide, P. et al. Protective effect of house screening against indoor Aedes aegypti in Mérida, Mexico: A cluster randomised controlled trial. Trop. Med. Int. Health. 26 (12), 1677–1688 (2021).
Acknowledgements
The authors thank the population of Restrepo for their willingness to carry out the project. Also to the Health Secretariat of Meta department for its accompaniment in the collection of information.
Funding
The project was supported by the Universidad Cooperativa de Colombia (INV3172). Students from the London School of Hygiene & Tropical Medicine were supported by the MSc Trust Fund Scholarship (student number 2203370).
Author information
Authors and Affiliations
Contributions
GIJR and GJPH conceptualized and conducted the study. Wrote original draft of the article. SB and EF were in charge of data collection and data analysis. LFCG and LASG were in charge of data collection. RTJ supported with methodology. Reviewed and edited the manuscript. All authors read, reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The project was approved by the Research Committee of the Universidad Cooperativa de Colombia (minute number 005 - May 18th 2021) and the Ethics Committee of Universidad Cooperativa de Colombia (No. BIO190, minute number 002 – June 10th 2021). Additionally, a favorable opinion was provided by the London School of Hygiene & Tropical Medicine MSc Research Ethics Committee: reference numbers 29051 and 28862. The study was conducted in accordance with the principles of the Declaration of Helsinki, with the wellbeing and rights of participants being the first consideration. Additionally, the handling of information and its confidentiality, adhered to the provisions outlined under Colombian law Resolution 8430 of 1993. No vulnerable group was involved in the research. Written informed consent was obtained from all participants, ensuring voluntary participation and confidentiality.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Jaramillo-Ramirez, G.I., Budhwar, S., Ford, E. et al. Social perception and environmental risk factors for dengue in an endemic municipality in eastern Colombia: a mixed method study. Sci Rep 15, 12736 (2025). https://doi.org/10.1038/s41598-025-96549-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-96549-8
