
Abstract
Autism Spectrum Disorder (ASD) is a neurodevelopmental condition that requires public understanding to foster acceptance and reduce stigma. This study aimed to evaluate ASD knowledge and stigma among the Lebanese population and the factors influencing them. An online cross-sectional study was conducted between February and July 2022 among Lebanese adults. Participants completed a self-administered structured questionnaire that comprised a sociodemographic section and two validated scales serving the study’s purpose (The Autism Stigma and Knowledge Questionnaire (ASK-Q) and The Autism Social Distance Scale). A total of 949 participants filled out the questionnaire. More than half of them had adequate knowledge of autism diagnosis and symptoms (57.9%), while only 6.6% and 9.6% showed adequate knowledge of its etiology and treatment, respectively. Additionally, 83.4% of the participants did not endorse stigma toward autism. The multivariate analysis taking the knowledge total score and subscales as the dependent variables showed that declaring prior knowledge of autism was significantly associated with better knowledge (Beta = 1.38) and higher stigma (Beta = 0.26). Furthermore, a higher knowledge score (Beta = − 0.06) and a declared prior knowledge of autism (Beta = − 0.62) were significantly associated with lower autism social distance. These findings highlight the need for targeted awareness campaigns to address knowledge gaps and further reduce stigma in Lebanon.
Similar content being viewed by others

Introduction
Autism Spectrum Disorder (ASD) is a complex neurodevelopmental condition characterized by persistent difficulties in social interaction and communication and the presence of repetitive or restricted behavioral patterns1,2. ASD affects individuals across various cultural, ethnic, and socio-economic backgrounds3. Its severity varies widely, from mild to severe cases that demand substantial support4,5. With a global prevalence rate estimated by the World Health Organization (WHO) to be around 1 in 100 children, ASD has become a significant public health concern6. Additionally, the Centers for Disease Control and Prevention (CDC) report that 1 in 36 children in the U.S. is diagnosed with ASD, with boys being nearly four times more likely to be diagnosed than girls7,8. Lebanon, like many other countries, has also witnessed an increase in the prevalence of ASD in recent years, estimated to affect 1 in 66 children across all Lebanese regions9.
The impact of ASD extends beyond the individuals diagnosed with the disorder, affecting their families, communities, and societies at large10. Early diagnosis and intervention are critical to improving long-term outcomes, yet diagnosing ASD remains challenging due to the absence of definitive medical tests or biomarkers as well as a lack of adequate knowledge and awareness about the disease11. Diagnosis relies primarily on behavioral observation, and while signs of ASD can often be identified by the age of 18 months, many children are not diagnosed until much later12. This delay in diagnosis can result in individuals with ASD not receiving the early assistance and support that is crucial for their well-being13. Indeed, previous studies have demonstrated that early interventions in ASD significantly improve cognition, language, and adaptive behavior14,15.
While efforts have been made to raise awareness and enhance support for individuals with ASD, significant gaps still exist in public knowledge and perceptions of this disorder. It is noteworthy to mention that misconceptions about ASD are widespread in many Arab countries, influenced by cultural beliefs, misinformation, and a lack of public awareness16. In these societies, parents often seek alternative explanations for their child’s diagnosis, such as attributing ASD to the “evil eye”. Studies have shown that in Saudi Arabia, families frequently turn to religious healers for spiritual healing instead of evidence-based interventions, delaying diagnosis and appropriate care17. Additionally, misconceptions linking vaccines to ASD persist despite scientific evidence disproving any such association18,19. Numerous studies have examined the level of understanding regarding ASD, with a predominant focus on healthcare professionals, university students, and families, while paying comparatively less attention to the broader general population20,21,22,23,24. It was revealed that ASD knowledge levels differed significantly across the general population25. For instance, parents and professionals in Indonesia had adequate knowledge of ASD26. Moreover, a high prevalence of adequate knowledge was found among university students in the USA27. On the other hand, a recent study that examined ASD knowledge, beliefs, and sources of information in a sample of Lebanese general population showed that the participants’ understanding of ASD was low, with many respondents unable to identify key diagnostic features or evidence-based interventions28. Likewise, Alyami and colleagues reported insufficient knowledge about ASD among the general population in Saudi Arabia, particularly regarding diagnostic criteria and etiology29. Comparable findings were observed in Turkey, where a general lack of awareness was noted, leading to delays in diagnosis and intervention30.
On another note, a major obstacle to improving the lives of individuals with ASD is the pervasive stigma associated with the disorder, which often stems from a lack of accurate information and a host of misunderstandings and misconceptions about the condition31,32. Social distancing is a key aspect of stigma and a widely used historical method for measuring stigma in research33. It refers to the degree to which an individual is willing to engage in social intimacy with someone from the studied group, such as those distinguished by race, social class, mental health issues, or medical conditions34. As a consequence of this false belief, individuals with ASD encounter negative experiences in their everyday lives. This stigma can lead to social isolation, discrimination, and barriers to accessing necessary resources such as education and healthcare31,35. Individuals with ASD may also face challenges in finding employment, making friends, and forming meaningful relationships due to the negative attitudes and beliefs associated with their condition31,36,37. Moreover, parents of children with ASD may also face societal judgment, compounding the challenges they already encounter38.
Recent studies highlighted the detrimental impact of stigma on individuals with ASD and their families. For instance, Kinnear et al. found that parents of children with ASD experience significant social rejection, leading to isolation and increased caregiver stress39. Similarly, the majority of parents of children with ASD in Nigeria internalized stigma and recounted negative experiences of stigma40. Also, public stigma and negative societal attitudes toward ASD contributed to heightened stress, anxiety, and depression in both individuals with ASD and their families31,41. In the Middle East, stigma often leads families to conceal an ASD diagnosis, further isolating individuals and impeding support networks42.
Efforts to reduce stigma have shown promising results. For example, Harrison et al. developed the Autism Stigma and Knowledge Questionnaire (ASK-Q) to assess public perceptions and guide targeted awareness campaigns25. Similarly, Gillespie-Lynch et al. demonstrated that brief educational interventions significantly improved knowledge and reduced stigma among college students43. These findings emphasize the importance of public education initiatives in dispelling myths and fostering inclusivity.
In Lebanon, stigma toward ASD remains prevalent, influenced by cultural norms and limited public understanding16,44. Families may avoid seeking diagnostic services due to fear of judgment, exacerbating delays in receiving essential interventions26. Therefore, understanding the level of knowledge and the prevailing stigma toward ASD among the Lebanese population is crucial to developing effective interventions and support systems that provide the unique needs of individuals with ASD and their families, as well as, creating a more inclusive and empathetic society for individuals with the disease. Accordingly, the current study was conducted to assess the Lebanese public ASD knowledge in the areas of diagnosis and symptoms, etiology, and treatment, assess their stigma and social distancing towards ASD. It also aimed to examine the factors that affect their knowledge, stigma, and social distancing.
Methods
Study design
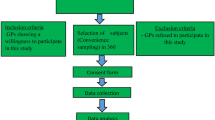
A cross-sectional questionnaire-based study was conducted that included participants from all over Lebanon. The sample was purposefully selected from the five governorates of Lebanon (Beirut, Beqaa, Mount Lebanon, South, and North) through a snowball technique (80%); additional conveniently selected participants were added to reach the total sample size (20%). The study was carried out between February 2nd and July 8th, 2022 using an online questionnaire created on Google Forms.
Ethical aspect
The Lebanese International University School of Pharmacy Research and Ethics committee approved the study protocol (2021RC-024-LIUSOP). The study carried no harmful risks as it was observational, and the anonymity of all participants was warranted as personal identifiers weren’t traced during data collection and analysis. Written consent was obtained from each person at the beginning of the questionnaire.
Sample size
Using the Epi-info software and considering an expected frequency of 43.1% of participants’ understanding of autism spectrum disorder among a sample of the Lebanese population based on a previous study28. With a confidence level of 95%, a margin of error of 4%, and a design effect of 1, the minimal sample size needed was 588. We have included in the current study 949 participants.
Procedure and data collection
The structured questionnaire was developed by the research team based on a literature review to cover the primary key points of knowledge and stigma related to ASD under the title of: “A National Survey Assessing Knowledge and Awareness of Autism Spectrum Disorder among the Lebanese Population”25,45,46,47. Initially created in English, the questionnaire was translated into Arabic through a rigorous back-translation process involving two experts in English and special education. Differences between the original and back-translated versions were resolved to ensure alignment with spoken Lebanese Arabic while preserving the original meaning, and education professionals validated the final Arabic version for accuracy and clarity. A pilot test with 10 participants assessed the questionnaire’s clarity, readability, and flow, resulting in minor revisions to the Arabic version to improve wording and structure. The average completion time was 7–10 min. The finalized questionnaire was converted into an online survey using Google Forms and distributed via social media platforms such as Facebook, Instagram, and WhatsApp. Participants were encouraged to share the link, employing a snowball sampling technique to expand the reach. Eligibility criteria included individuals residing in Lebanon aged 18 years or older, while non-residents and those under 18 were excluded. The study’s scope and purpose were explained at the beginning of the survey, and participants were informed of the voluntary nature of the study. Anonymity and confidentiality were ensured by not collecting personally identifiable information (e.g., names, email addresses, or IP addresses), and all data were stored securely in a password-protected system accessible only to the research team.
Measurement tools
The structured questionnaire consisted of questions that covered several areas divided into three sections. The first section addressed the participants’ sociodemographic data: age, gender, nationality, region of residence, marital status, number of children, educational level, working status, smoking status, monthly family income, and health insurance coverage. Furthermore, participants were asked about their experience with ASD (e.g., whether or not they have participated in ASD training, or interacted with an individual with ASD, or attended a lecture about ASD). In the second and third sections, two validated scales that served the purpose of the study in measuring the participants’ knowledge and stigma toward ASD were included as follows:
The autism stigma and knowledge questionnaire (ASK-Q)
The ASK-Q is a recently developed tool designed to address many of the measurement challenges found in earlier ASD knowledge assessments. The ASK-Q was created to have cross-cultural utility, and initial data indicates that it has strong psychometric properties25,48,49. It is a 49-item questionnaire designed to evaluate ASD knowledge in the categories of diagnosis/symptoms (D/S, 17 items), etiology (ET, 15), and treatment (TR, 13), as well as the endorsement of stigma (ST, 3). In addition, the statement “I have prior knowledge about autism” was used as a screening question in the demographic section since it was not designed to be part of the diagnostic analyses.
The Diagnosis/Symptoms subsection included 17 statements that describe symptoms of ASD, some based on the DSM-V definition and others pertaining to common misconceptions. This subsection was used to assess participants’ understanding of the characteristics of autism. Some statements included in this section are: “Children with autism do not enjoy the presence of others,” “Many children with autism show the need for routines and sameness,” and “Many children with autism have difficulty using everyday language to communicate their needs.”
The Etiology subsection included 15 statements that describe the source of ASD, some scientifically based and some misconceptions. Items in this subsection included, for example: “Vaccines cause autism,” “Autism occurs more commonly among higher socioeconomic and educational levels,” and “Autism affects people of all races and ethnicities.”
The Treatment subsection included 13 items; some described evidence-based treatment, while others addressed non-evidence-based treatments. Items in this subsection included, for instance: “Children with autism are never too old to benefit from treatment,” “Behavior therapy is an intervention most likely to be effective for children with autism,” and “Children with autism can grow up to live independently.”25.
The ASK-Q examines the endorsement of autism stigma through a fourth subscale that assesses participants’ endorsement of misinformation about autism. The stigma-related questions are integrated into the other three subscales as a secondary construct25. For instance, the question “Autism is preventable” evaluates both participants’ understanding of etiology and their endorsement of stigma. Similarly, other items assessing stigma endorsement, such as “All children with autism usually have problems with aggression” and “Most children with autism are extremely impaired and cannot live independently as adults,” also simultaneously evaluate participants’ knowledge of autism diagnosis/symptoms and treatment, respectively.
For each item, participants were asked to respond by signifying “agree” if the statement does describe ASD or individuals with ASD, “disagree” if the statement does not describe ASD or an individual with ASD, or “don’t know.” Items were scored as either correct or incorrect. Given the need for dichotomous answer choices in our method of analysis, the “don’t know” answer choice on the ASK-Q was coded as incorrect (whether the correct answer was “agree” or “disagree). The reason was that if participants selected “don’t know,” it was an indirect way of assessing that they did not know the correct answer.
Cutoff scores were determined for each knowledge subscale distinguishing between adequate and inadequate knowledge, and ranges were as follows: in the D/S subdomain, 0–10 (inadequate) and 11–17 (adequate); for ET, 0–10 (inadequate) and 11–15 (adequate); for TR, 0–9 (inadequate) and 10–13 (adequate). Regarding the ST subdomain, 0–2 indicated that the participant endorsed stigma, while those scoring 3–7 were categorized as not endorsing stigma25,46,47,50. The Cronbach’s alpha for the ASK-Q in this study was 0.818.
The autism social distance scale
The third section of the questionnaire included the Autism Social Distance Scale, adapted by Gillespie-Lynch and colleagues from the Bogardus Social Distance Scale, which was initially used to examine the social distance from non-clinical outgroups, such as racial minorities51.
Participants were asked to read six questions and rate how likely they would be to engage in certain activities with individuals with autism. The questions included scenarios such as “How willing would you be to move next door to someone with autism?” and “How willing would you be to marry or date a person with autism?” Each statement was rated on a 4-point Likert scale, reflecting varying degrees of willingness toward the social distance items. Scoring was as follows: 4 (definitely unwilling), 3 (somewhat unwilling), 2 (somewhat willing), 1 (definitely willing). Hence, total scores spanned 6 to 24, with higher scores indicating greater social distance and, by extension, increased stigma. In this study, the Cronbach’s alpha value was 0.771.
Statistical analysis
All analyses were performed using IBM’s Statistical Package for the Social Sciences (SPSS) version 26.0 (IBM, Inc., Chicago, IL). Cronbach’s alpha was calculated for the reliability analysis of all scales.
A descriptive analysis was performed using absolute frequencies and percentages for categorical variables and means and standard deviations (SD) for quantitative measures. The sample was normally distributed, as checked by visual inspection of the histogram, and skewness and kurtosis were below |1.96|. The multicollinearity was checked by using the Variance Inflation Factor (VIF). VIF < 5: The variable has low multicollinearity (no significant issue).
In order to answer the objective of the study, the ASK-Q total scale, and subscales included in the stigma scale were considered as dependent variables. In addition, to reply to the secondary objective we have considered the autism social distance scale as a dependent variable. The sociodemographic variables were considered as independent variables.
Student’s t-test or ANOVA F tests were used for the associations of ASK-Q total score, subscales, and autism social distance scale (continuous variables) with categorical ones. Person correlation was used to test the association between ASK-Q total score, subscales, and autism social distance scale.
Bonferroni correction was applied for multiple tests; the corrected p-value was obtained by dividing 0.05 by the number of variables to be tested (= 20), yielding a p = 0.0025 in the bivariate analysis. All p-values less than 0.0025 were considered as significant.
A multivariate analysis of covariance (MANCOVA) was carried out, taking the Autism Stigma and Knowledge Questionnaire as the dependent variable. MANCOVA was used to assess the effect of independent variables (sociodemographic and other characteristics) on multiple dependent variables (ASK-Q total score and subscales) simultaneously. It takes into account the relationships among the dependent variables, providing a multivariate perspective.
Also, a hierarchical linear regression analyses were performed using the enter method and taking the autism social distance scale as the dependent variable. In the first step, the sociodemographic variables were considered as the independent variables. In the second step, the following variables were added to the model: training for interacting with individuals with autism, prior knowledge and experience with individuals with Autism. In the third step, the Autism Stigma and Knowledge Questionnaire total scores were added to the model. The unstandardized Beta was used to measure the effect of the factors on the dependent variable.
The variables that showed a p-value < 0.1 in the bivariate analysis were considered independent variables and were included in all models to avoid potential confounders. A p-value < 0.05 was considered significant.
Results
Participants’ characteristics and baseline demographics
A total of 949 Lebanese respondents filled out the questionnaire. The mean age of the participants was 32.74 ± 10.93 years. The percentage of males was 49.9% (n = 473), while females represented 50.1% (n = 476). The analyzed sample included participants from all Lebanese districts, with the highest proportion being from the Beqaa area (43.4%, n = 412). Moreover, the majority of respondents were married (65.6%, n = 623), non-smokers (65.4%, n = 621), did not consume alcohol (97.4%, n = 929), and 291 (30.7%) of the participants did not have children. Only 20.7% (n = 196) had a university education level, and 9.8% (n = 93) were employed in a health-related field. A minority of participants declared not having prior knowledge of autism (41.1%, n = 370), while most (66.7%, n = 633) did not have any experience with individuals with ASD, 80.2% (n = 761) did not attend any lecture or seminar about autism, and 94.3% (n = 895) did not undergo training for interacting with autistic members. Supplementary Table S1 provides the detailed sociodemographic characteristics of the participants.
ASK-Q results
Overall, the sample was knowledgeable about the diagnosis and symptoms of ASD, with more than half of the participants (57.9%, n = 549) demonstrating adequate knowledge, with scores falling in the range of 11–17. For the etiology subdomain, 93.4%(n = 887) had inadequate knowledge. Regarding the treatment subdomain, participants exhibited a lack of knowledge, where 90.4% (n = 858) scored 0–9. Additionally, 83.4% (n = 792) did not endorse stigma, with scores spanning 3–7. Table 1 presents the scoring details.
Autism social distance scale results
The mean autism social distance total score was 13.73 ± 3.56 with a median of 14 and a range between 6 and 24. Six questions constitute the scale rated on a 4-point Likert scale with a minimum of 1 and maximum 4. The item about Marry/date oneself had the highest score with a mean of 3.15 ± 0.99 and the lowest item was for spend an evening socializing 1.80 ± 0.73 (Supplementary table S2).
Bivariate analysis
Supplementary table S3 presents the bivariate analysis, taking the Autism Social Distance Scale and the Autism Stigma and Knowledge Questionnaire (ASK-Q scale) as the dependent variables. When considering the ASK-Q scale total score as the dependent variable, the results showed a significantly higher mean knowledge score among males, those working in a health-related job, having a high-income level, having previously attended any lecture or seminar about autism, having an experience with individuals with autism, having a friend or acquaintance with autism, and declaring no prior knowledge of autism. In addition, a significantly older age was related to poor knowledge, while a higher number of children was associated with better knowledge. Almost the same results were found in the knowledge subscales.
Regarding the autism social distance scale, significantly higher mean scale scores were found among non-single participants, those with an intermediate income, those who did not attend any lecture or seminar about autism, and those who declared no prior knowledge of autism. In addition, older age and number of children were associated with significantly higher social distance scores.
All ASK-Q scale subscores were intercorrelated and correlated with the total ASK-Q scale. The correlation coefficients varied between moderate correlation r = 0.481, p < 0.001 (for the stigma total score and the diagnosis/symptom total score) and strong correlation r = 0.877, p < 0.001 (for the ASK-Q total score and the diagnosis/symptom subscore). Moreover, a significant positive moderate to strong correlation was found between ASK-Q total score and subscores (p < 0.001 for all). As for the correlation between social distance and the ASK-Q total score and subscores, a negative weak correlation was found except for the etiology subscore where a positive weak correlation was found (r = 0.004, p = 0.044) (Table S4).
Multivariable analysis
A multivariate analysis (MANCOVA) was conducted, taking the ASK-Q total score and subscales as the dependent variables. When considering the ASK-Q total score and subscales (etiology and treatment) and the stigma scale as the dependent variables, the results showed that having prior knowledge of autism (Beta = 1.386, 95% Confidence interval (CI) 0.30–2.46, partial η2 = 2.46) was significantly associated with better knowledge (higher knowledge scale and higher etiology and treatment subscales) and higher stigma. Considering the diagnosis subscale as the dependent variable, the results showed that having an experience with individuals with ASD (Beta = 0.89, 95% CI 0.10–1.67, partial η2 = 0.007), having a family/friend relationship with autistic people (Beta = 1.36, 95% CI 0.49–2.24, partial η2 = 0.013) were significantly associated with better knowledge of diagnosis (Table S5).
However, the female gender and older age were significantly associated with lower knowledge and stigma. A detailed association of the independent variables with the dependent variables is shown in Table 2.
When considering the autism social distance scale as the dependent variable, the results showed that a high number of children (Beta = 0.41) and a low family income (Beta = − 1.03) were significantly associated with high social distance (Table 3, Model 1).
When adding the variables related to the experience and prior knowledge with someone with autism the results showed that being a smoker (Beta = 0.50), high number of children (Beta = 0.36) and having an experience with individuals with autism (Beta = 0.87) were significantly associated with high social distance. However, a high family income (Beta = − 0.89) and prior knowledge (Beta = − 0.72) were significantly associated with low social distance (Table 3, Model 2).
By adding the ASK-Q total score in the third model the results showed that a high knowledge (Beta = − 0.06) was significantly associated with lower social distance (Table 3, Model 3).
Discussion
This study offers a comprehensive description of public knowledge and stigma toward ASD, providing an overview of its current state among the Lebanese population. The main findings revealed adequate public knowledge of ASD diagnosis and symptoms, limited knowledge of its etiology and treatment, and a low stigma toward ASD among most participants.
ASD knowledge and socio-demographics
The study found that only 20% of the participants had a university education, with half being unemployed. In rural areas of Lebanon, access to higher education, employment, and family income opportunities is limited. Given that 43% of the sample was from the Beqaa, a rural area in Lebanon, with limited services for conditions like ASD, low education, unemployment, and low income were expected factors. All these conditions may explain the inadequate knowledge of ASD’s etiology and treatment, as public understanding of ASD varies significantly across different populations and regions52. A similar pattern was observed in another study, where ASD treatment options varied according to parent’s income, education, and location53.
Older age was linked to lower ASD knowledge across all categories (general knowledge, diagnosis, and etiology), consistent with recent findings54. Females in our study had lower autism knowledge, contrasting with findings from another study where women demonstrated higher levels of knowledge55. Cultural norms, societal expectations, educational disparities, and varying access to information may explain gender differences in ASD knowledge29,55. While females in our study showed lower general ASD knowledge, including diagnosis and etiology, no gender difference was found in treatment knowledge. Future research should further explore these factors to better understand gender-specific knowledge gaps.
Contrary to existing literature, lack of health insurance was linked to higher ASD knowledge. This unusual finding may be due to other factors, such as community outreach or educational programs targeting lower socioeconomic groups56,57,58. Further research is needed to explore this relationship.
ASD knowledge findings compared to previous studies
In this study, more than half of the participants had adequate knowledge of ASD diagnosis and symptoms, but few had an understanding of its etiology and treatment, similar to findings in studies from various regions, including Australia, Africa, and Saudi Arabia55,59,60. In fact, ASD is a complex condition, and understanding its causes and treatment is still evolving. Limited media coverage, misinformation, and a focus on diagnosis over causes or treatment contribute to knowledge gaps. Therefore, participants’ knowledge reflects scientific uncertainty on ASD, not a lack of awareness.
Our results align with previous studies, showing a higher autism knowledge among healthcare workers61, those who attended autism-related lectures62, interacted with individuals with autism63,64,65, or had prior knowledge of the condition66,67. Additionally, parents with more children tended to have greater autism knowledge, likely due to increased concern about health issues affecting their children’s well-being26.
Not drinking alcohol was associated with higher ASD diagnosis knowledge in our sample. This may relate to a study showing autistic individuals are less likely to consume alcohol excessively68, suggesting that those with better ASD knowledge may also recognize alcohol’s harmful effects69. It should be noted that only 3% of our sample consumed alcohol, with its use less common in some regions of Lebanon such as Bekaa, South, and North due to cultural and religious factors. This regional disparity may bias our results, necessitating further investigation for broader generalizability.
Unexpectedly, working in a non-health-related setting was linked to higher ASD treatment knowledge, possibly due to sample bias, as half of the participants were unemployed and only 9% worked in healthcare. Health professionals typically have better ASD knowledge61.
ASD stigma results compared to previous studies
This study found a low prevalence of stigma toward ASD, with most participants (83.4%) showing no stigma, in contrast to a previous survey where only 43.4% had no stigma toward ASD54. The low stigma in our study may reflect increased awareness and acceptance of neurodiversity, driven by advocacy efforts, media representation, and shifting public attitudes. However, stigma varies across cultures and subgroups, and our sample may not fully capture these differences.
On the other hand, being a female was associated with a lower stigma toward autism, which is coherent with previous findings, where females had less stigmatized views about autism43,64,70, and higher levels of acceptance with a more positive attitude towards autistic people70. Moreover, the lack of knowledge about autism, being married, older age, having a higher number of children, and having a moderate income were associated with higher autism social distance and stigma, supporting the findings of a recent narrative review on stigma and ASD31. A conceptual framework such as the Health Belief Model can further help explain the dynamics of ASD sigma in our study by highlighting how individuals’ perceptions shape their attitudes toward ASD60,61.
Limitations and strengths of the study
This study has limitations, including the inability to make causal inferences due to its cross-sectional design, and potential sampling errors from snowball/convenient sampling, which may have caused over- or under-representation of certain groups based on socioeconomic, cultural, and regional factors. Thus, we acknowledge that the sample may not be fully representative of the broader Lebanese population, but we believe it still provides valuable insights into ASD knowledge and stigma assessment in Lebanon. Online surveys may have introduced selection bias and excluded certain demographic groups. Participants with connections to individuals with autism might have been over-represented. Additionally, limited access to reliable internet or insufficient digital literacy could have limited participation from some segments of the population. Moreover, some participants may have possibly renounced to participation in the survey due to a lack of knowledge about the topic. These factors could affect generalizability but do not impact the study’s associations. Furthermore, while the ASK-Q was designed for cross-cultural use, its validation in the specific Lebanese context was not formally conducted in this study. Future research should focus on validating the tool across diverse Lebanese subpopulations to ensure cultural appropriateness and accuracy. Despite these limitations, the study is the first in Lebanon to comprehensively assess public knowledge and stigma surrounding ASD, supported by a large sample size that enhances the reliability of the findings. Future research should use a more balanced and representative sample to improve generalizability and inform effective interventions.
Conclusion
The present study revealed that while the public has a reasonable understanding of the diagnosis and symptoms of ASD, knowledge about its etiology and treatment remains limited. Furthermore, most participants did not express stigma toward individuals with ASD, which suggests that, at least at a broad societal level, there is an openness and acceptance toward these individuals. These findings offer valuable insights that can guide the development of targeted social interventions, public awareness campaigns, and educational programs or national policies.
To address autism knowledge gaps and stigma in Lebanon, public awareness campaigns should focus on ASD etiology and treatment, especially in low-income and rural areas. Healthcare workers should receive specialized training, and schools should integrate ASD education into their curriculum and provide support to students affected by the condition and their families. Low-income families should advocate for policies promoting early screening and better healthcare.
To conclude, future research should build on this study’s findings and address gaps in ASD awareness and stigma among the Lebanese population by mainly focusing on exploring how cultural and regional factors influence stigma and awareness of this condition, particularly in diverse subgroups, to develop tailored interventions and support strategies.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Salari, N. et al. The global prevalence of autism spectrum disorder: A comprehensive systematic review and Meta-Analysis. Ital. J. Pediatr. 48, 112. https://doi.org/10.1186/s13052-022-01310-w (2022).
Hodges, H., Fealko, C. & Soares, N. Autism spectrum disorder: Definition, epidemiology, causes, and clinical evaluation. Transl Pediatr. 9, S55–S65. https://doi.org/10.21037/tp.2019.09.09 (2020).
Aylward, B. S., Gal-Szabo, D. E., Taraman, S. & Racial Ethnic, and sociodemographic disparities in diagnosis of children with autism spectrum disorder. J. Dev. Behav. Pediatr. 42, 682–689. https://doi.org/10.1097/DBP.0000000000000996 (2021).
Waizbard-Bartov, E., Fein, D., Lord, C. & Amaral, D. G. Autism severity and its relationship to disability. Autism Res. Off J. Int. Soc. Autism Res. 16, 685–696. https://doi.org/10.1002/aur.2898 (2023).
Wozniak, R. H., Leezenbaum, N. B., Northrup, J. B., West, K. L. & Iverson, J. M. The development of autism spectrum disorders: variability and causal complexity. Wiley Interdiscip Rev. Cogn. Sci. 8 https://doi.org/10.1002/wcs.1426 (2017).
Autism October Available online: (2023). https://www.who.int/news-room/fact-sheets/detail/autism-spectrum-disorders.
Maenner, M. J. Prevalence and characteristics of autism spectrum disorder among children aged 8 years—autism and developmental disabilities monitoring network, 11 sites, United States, 2020. MMWR Surveill Summ. 72 https://doi.org/10.15585/mmwr.ss7202a1 (2023).
Autism Spectrum Disorder (ASD). Available online: https://www.nimh.nih.gov/health/statistics/autism-spectrum-disorder-asd (2023).
Richa, S. et al. Estimating the prevalence of autism spectrum disorder in Lebanon. L’Encephale 46, 414–419. https://doi.org/10.1016/j.encep.2020.05.015 (2020).
Devenish, B. D. et al. A brief report: Community supportiveness may facilitate participation of children with autism spectrum disorder in their community and reduce feelings of isolation in their caregivers. Front. Psychol. 11 (2020).
May, T., Sciberras, E., Brignell, A. & Williams, K. Autism spectrum disorder: updated prevalence and comparison of two birth cohorts in a nationally representative Australian sample. BMJ Open. 7, e015549. https://doi.org/10.1136/bmjopen-2016-015549 (2017).
CDC Diagnostic Criteria | Autism Spectrum Disorder (ASD). | NCBDDD | CDC Available online: https://www.cdc.gov/ncbddd/autism/hcp-dsm.html (2023).
Ghanouni, P. & Seaker, L. What does receiving autism diagnosis in adulthood look like? Stakeholders’ experiences and inputs. Int. J. Ment Health Syst. 17 https://doi.org/10.1186/s13033-023-00587-6 (2023).
Elder, J. H., Kreider, C. M., Brasher, S. N. & Ansell, M. Clinical impact of early diagnosis of autism on the prognosis and parent-child relationships. Psychol. Res. Behav. Manag. 10, 283–292. https://doi.org/10.2147/PRBM.S117499 (2017).
Gabbay-Dizdar, N. et al. Early diagnosis of autism in the community is associated with marked improvement in social symptoms within 1–2 years. Autism 26, 1353–1363. https://doi.org/10.1177/13623613211049011 (2022).
Obeid, R. et al. A Cross-Cultural comparison of knowledge and stigma associated with autism spectrum disorder among college students in Lebanon and the united States. J. Autism Dev. Disord. 45 https://doi.org/10.1007/s10803-015-2499-1 (2015).
Alqahtani, M. Understanding autism in Saudi Arabia: A qualitative analysis of the community and cultural contextunderstanding autism in Saudi Arabia: A qualitative analysis of the community and cultural context. J. Pediatr. Neurol. 10, 15–22. https://doi.org/10.3233/JPN-2012-0527 (2012).
Asiri, W. M. A. et al. Assessment of parental knowledge, awareness, and perception about autism spectrum disorders in Aseer region, Southwestern Saudi Arabia. Int. J. Gen. Med. 16, 557–564. https://doi.org/10.2147/IJGM.S377521 (2023).
Goin-Kochel, R. P. et al. Beliefs about causes of autism and vaccine hesitancy among parents of children with autism spectrum disorder. Vaccine 38, 6327–6333. https://doi.org/10.1016/j.vaccine.2020.07.034 (2020).
Low, H. M. et al. S. A grassroots investigation of ASD knowledge and stigma among teachers in Luang Prabang, Lao PDR. Res. Autism Spectr. Disord. 80 https://doi.org/10.1016/j.rasd.2020.101694 (2021).
Al-Sharbati, M. M. et al. Awareness about autism among school teachers in Oman: A cross-sectional study. Autism Int. J. Res. Pract. 19, 6–13. https://doi.org/10.1177/1362361313508025 (2015).
Alobaid, A. S. & Almogbel, E. Awareness of autism spectrum disorder among pre-school teachers in Qassim region, Saudi Arabia. Health Psychol. Res. 10 https://doi.org/10.52965/001c.37676 (2022).
Chansa-Kabali, T., Nyoni, J. & Mwanza, H. Awareness and knowledge associated with autism spectrum disorders among university students in Zambia. J. Autism Dev. Disord. 49, 3571–3581. https://doi.org/10.1007/s10803-019-04044-7 (2019).
Anwar, M. S., Tahir, M., Nusrat, K., Khan, M. R. & Knowledge awareness, and perceptions regarding autism among parents in Karachi, Pakistan. Cureus 10, e3299. https://doi.org/10.7759/cureus.3299
Harrison, A. J., Bradshaw, L. P., Naqvi, N. C., Paff, M. L. & Campbell, J. M. Development and psychometric evaluation of the autism stigma and knowledge questionnaire (ASK-Q). J. Autism Dev. Disord. 47, 3281–3295. https://doi.org/10.1007/s10803-017-3242-x (2017).
Handayani, M. M. & Paramita, P. P. Stigma and knowledge about autism spectrum disorder among parents and professionals in Indonesia. In Proceedings of the Proceedings of the 3rd International Conference on Psychology in Health, Educational, Social, and Organizational Settings 97–100 (SCITEPRESS - Science and Technology Publications, Surabaya, Indonesia, 2018).
Reckard, S. Autism knowledge and stigma among college students at the University of Wisconsin—River Falls. Thesis (2021).
Rouphael, M. et al. Evaluation of the Lebanese adults’ knowledge regarding autism spectrum disorder. Int. J. Environ. Res. Public. Health 20, 4622. https://doi.org/10.3390/ijerph20054622 (2023).
Alyami, H. S., Naser, A. Y., Alyami, M. H., Alharethi, S. H. & Alyami, A. M. Knowledge and attitudes toward autism spectrum disorder in Saudi Arabia. Int. J. Environ. Res. Public. Health 19, 3648. https://doi.org/10.3390/ijerph19063648 (2022).
Rakap, S., Balikci, S., Kalkan, S. & Aydin, B. Knowledge of autism spectrum disorder among the general population in Turkey: Implications for public training and education. Int. J. Disabil. Dev. Educ. 69, 565–577. https://doi.org/10.1080/1034912X.2020.1719047 (2022).
Turnock, A., Langley, K. & Jones, C. R. G. Understanding stigma in autism: A narrative review and theoretical model. Autism Adulthood Chall. Manag. 4, 76–91. https://doi.org/10.1089/aut.2021.0005 (2022).
Dillenburger, K.; McKerr, L.; Jordan, J.A.; Devine, P.; Keenan, M. Creating an inclusive society. How close are we in relation to autism spectrum disorder? A general population survey. J. Appl. Res. Intellect. Disabil. JARID 28, 330–340. https://doi.org/10.1111/jar.12144. (2015)
Link, B. G., Yang, L. H., Phelan, J. C. & Collins, P. Y. Measuring mental illness stigma. Schizophr Bull. 30, 511–541. https://doi.org/10.1093/oxfordjournals.schbul.a007098 (2004).
Lauber, C., Nordt, C., Falcato, L. & Rössler, W. Factors influencing social distance toward people with mental illness. Commun. Ment Health J. 40, 265–274. https://doi.org/10.1023/b:comh.0000026999.87728.2d (2004).
Rivera, R. A. & Bennetto, L. Applications of identity-based theories to understand the impact of stigma and camouflaging on mental health outcomes for autistic people. Front. Psychiatry 14, 1243657. https://doi.org/10.3389/fpsyt.2023.1243657 (2023).
Lorenz, T., Frischling, C., Cuadros, R. & Heinitz, K. Autism and overcoming job barriers: Comparing job-related barriers and possible solutions in and outside of autism-specific employment. PLoS ONE 11, e0147040. https://doi.org/10.1371/journal.pone.0147040 (2016).
Huang, A. X. et al. Understanding the self in individuals with autism spectrum disorders (ASD): A review of literature. Front. Psychol. 8, 1422. https://doi.org/10.3389/fpsyg.2017.01422 (2017).
Hus, Y. & Segal, O. Challenges surrounding the diagnosis of autism in children. Neuropsychiatr Dis. Treat. 17, 3509–3529. https://doi.org/10.2147/NDT.S282569 (2021).
Kinnear, S. H., Link, B. G., Ballan, M. S. & Fischbach, R. L. Understanding the experience of stigma for parents of children with autism spectrum disorder and the role stigma plays in families’ lives. J. Autism Dev. Disord. 46, 942–953. https://doi.org/10.1007/s10803-015-2637-9 (2016).
Oduyemi, A. Y., Okafor, I. P., Eze, U. T., Akodu, B. A. & Roberts, A. A. Internalization of stigma among parents of children with autism spectrum disorder in Nigeria: A mixed method study. BMC Psychol. 9, 182. https://doi.org/10.1186/s40359-021-00687-3 (2021).
Gray, D. E. Ten years on: A longitudinal study of families of children with autism. J. Intellect. Dev. Disabil. 27, 215–222. https://doi.org/10.1080/1366825021000008639 (2002).
Alshaigi, K. et al. Stigmatization among parents of autism spectrum disorder children in Riyadh, Saudi Arabia. Int. J. Pediatr. Adolesc. Med. 7, 140–146. https://doi.org/10.1016/j.ijpam.2019.06.003 (2020).
Gillespie-Lynch, K. et al. Changing college students’ conceptions of autism: An online training to increase knowledge and decrease stigma. J. Autism Dev. Disord. 45, 2553–2566. https://doi.org/10.1007/s10803-015-2422-9 (2015).
Gillespie-Lynch, K. et al. Factors underlying cross-cultural differences in stigma toward autism among college students in Lebanon and the United States. Autism Int. J. Res. Pract. 23, 1993–2006. https://doi.org/10.1177/1362361318823550 (2019).
Yu, L., Stronach, S. & Harrison, A. J. Public knowledge and stigma of autism spectrum disorder: Comparing China with the United States. Autism Int. J. Res. Pract. 24, 1531–1545. https://doi.org/10.1177/1362361319900839 (2020).
Kitchin, J. & Karlin, N. Awareness and stigma of autism spectrum disorders in undergraduate students. Psychol. Rep. 125, 332941211014144. https://doi.org/10.1177/00332941211014144 (2021).
Harrison, A. J., Paff, M. L. & Kaff, M. S. Examining the psychometric properties of the autism stigma and knowledge questionnaire (ASK-Q) in multiple contexts. Res. Autism Spectr. Disord. 57, 28–34. https://doi.org/10.1016/j.rasd.2018.10.002 (2019).
Papadopoulos, A. et al. Evaluating the psychometric properties of the autism stigma and knowledge questionnaire (ASK-Q) among Greek mental health professionals: An exploratory study. Neurosci. Res. Notes 7. https://doi.org/10.31117/neuroscirn.v7i3.327 (2024).
Schultz, P. V. et al. Validation of autism stigma knowledge - questionnaire (ASK-Q) for Brazilian Portuguese. Explor. Res. Clin. Soc. Pharm. 15, 100495. https://doi.org/10.1016/j.rcsop.2024.100495 (2024).
Self, T., Batchelor, D., Parham, D. & Part, C. Early intervention providers’ knowledge of autism spectrum disorder prior to and following ASD-Specific training. Int. J. Cross-Discip. Subj. Educ. 12, 4386–4396. https://doi.org/10.20533/ijcdse.2042.6364.2021.0537 (2021).
Emory, S. & Bogardus A Social Distance Scale Available online: https://brocku.ca/MeadProject/Bogardus/Bogardus_1933.html (Accessed 7 August 2022).
Harrison, A. J. et al. Assessing autism knowledge across the global landscape using the ASK-Q. J. Autism Dev. Disord. https://doi.org/10.1007/s10803-023-05936-5 (2023).
Alnemary, F. M., Aldhalaan, H. M., Simon-Cereijido, G. & Alnemary, F. M. Services for children with autism in the Kingdom of Saudi Arabia. Autism Int. J. Res. Pract. 21, 592–602. https://doi.org/10.1177/1362361316664868 (2017).
Rafiei, M., Nakhostin-Ansari, A., Meshkat, S., Khosravi, A. & Memari, A. H. Public awareness and stigma of autism spectrum disorder in Iran; an online survey. Res. Dev. Disabil. 134, 104441. https://doi.org/10.1016/j.ridd.2023.104441 (2023).
Abualhommos, A. K. et al. Community knowledge about autism spectrum disorder in the Kingdom of Saudi Arabia. Int. J. Environ. Res. Public. Health 19, 3438. https://doi.org/10.3390/ijerph19063438 (2022).
Cummings, J. R. et al. Health services utilization among children with and without autism spectrum disorders. J. Autism Dev. Disord. 46, 910–920. https://doi.org/10.1007/s10803-015-2634-z (2016).
Weiss, J. A. et al. Health concerns and health service utilization in a population cohort of young adults with autism spectrum disorder. J. Autism Dev. Disord. 48, 36–44. https://doi.org/10.1007/s10803-017-3292-0 (2018).
Matin, B. K. et al. Contributing factors to healthcare costs in individuals with autism spectrum disorder: A systematic review. BMC Health Serv. Res. 22, 604. https://doi.org/10.1186/s12913-022-07932-4 (2022).
Jones, S. C., Akram, M., Gordon, C. S., Murphy, N. & Sharkie, F. Autism in Australia: Community knowledge and autistic People’s experiences. J. Autism Dev. Disord. 51, 3677–3689. https://doi.org/10.1007/s10803-020-04819-3 (2021).
Wannenburg, N. & van Niekerk, R. Early diagnosis and intervention for autism spectrum disorder in Africa: Insights from a case study. Afr. Health Sci. 18, 137–146. https://doi.org/10.4314/ahs.v18i1.18 (2018).
Corden, K., Brewer, R. & Cage, E. A. Systematic review of healthcare professionals’ knowledge, self-efficacy and attitudes towards working with autistic people. Rev. J. Autism Dev. Disord. 9, 386–399. https://doi.org/10.1007/s40489-021-00263-w (2022).
Scheerer, N. E., Boucher, T. Q., Sasson, N. J. & Iarocci, G. Effects of an educational presentation about autism on high school students’ perceptions of autistic adults. Autism Adulthood Chall. Manag. 4, 203–213. https://doi.org/10.1089/aut.2021.0046 (2022).
Shand, A. J., Close, S. A. D. & Shah, P. Greater autism knowledge and contact with autistic people are independently associated with favourable attitudes towards autistic people. Exp. Results. 1, e46. https://doi.org/10.1017/exp.2020.46 (2020).
Kuzminski, R. et al. Linking knowledge and attitudes: Determining neurotypical knowledge about and attitudes towards autism. Plos One 14, e0220197. https://doi.org/10.1371/journal.pone.0220197 (2019).
Gillespie-Lynch, K., Kapp, S. K., Brooks, P. J., Pickens, J. & Schwartzman, B. Whose expertise is it? Evidence for autistic adults as critical autism experts. Front. Psychol. 8. https://doi.org/10.3389/fpsyg.2017.00438 (2017).
Liu, Y. et al. Attitudes, and perceptions of autism spectrum disorder in a stratified sampling of preschool teachers in China. BMC Psychiatry 16 https://doi.org/10.1186/s12888-016-0845-2 (2016).
Ma, A., Mm, A., Ra, S. & Mm, J. Public awareness of autism spectrum disorder. Neurosci. Riyadh Saudi Arab. 22 https://doi.org/10.17712/nsj.2017.3.20160525 (2017).
Weir, E., Allison, C. & Baron-Cohen, S. Understanding the substance use of autistic adolescents and adults: A mixed-methods approach. Lancet Psychiatry 8, 673–685. https://doi.org/10.1016/S2215-0366(21)00160-7 (2021).
Harmful use of alcohol. Available online https://www.who.int/health-topics/alcohol (Accessed 22 Jan 2024).
Kim, S. Y. The development and pilot-testing of the autism attitude acceptance scale: An instrument measuring autism acceptance. Autism Adulthood Chall. Manag. 2, 204–215. https://doi.org/10.1089/aut.2019.0066 (2020).
Acknowledgements
The authors would like to acknowledge all participants who responded to the study survey.
Author information
Authors and Affiliations
Contributions
SY conceptualized and designed the study. S.Y., N.M., C.H., D.S., and H.S. wrote the first draft of the manuscript; S.Y., S.M., N.H., Y.S., and S.B.M. acquired the data and designed the methodology; C.H., S.B.M., and P.S. carried out the analysis; C.H., D.S. and P.S. interpreted the results, P.S. and M.R. were responsible for project administration and supervision. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
All methods were performed in accordance with the Declaration of Helsinki and have been approved by the Ethics and Research Committee of the School of Pharmacy at the Lebanese International University (2021RC-024-LIUSOP). The study carried no harmful risks as it was observational, and the anonymity of all participants was warranted as personal identifiers weren’t traced during data collection and analysis. All participants agreed to participate and provided informed consent.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Younes, S., Mourad, N., Haddad, C. et al. A cross-sectional study of public knowledge and stigma towards autism spectrum disorder in Lebanon. Sci Rep 15, 11680 (2025). https://doi.org/10.1038/s41598-025-96858-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-96858-y
Keywords
This article is cited by
-
“More Than Just Taking Off Your Shoes”: A Mixed Methods Study of Cultural Adaptation Practices in the Autism Service System
Journal of Autism and Developmental Disorders (2025)
