
Abstract
This study aimed to observe the effect of the location and severity of partial ureteral obstruction, based on ureteropelvic and ureterovesical junction strictures, on stone formation. Forty 8-week-old male rats were divided into five groups: control and mild/severe proximal or distal ureteral obstruction groups. A partial ureteral obstruction was created according to the type of obstruction by a surgical procedure. After 5 days of intraperitoneal glyoxylate injection, the urine, blood samples, and kidney tissues of the rats were examined. There were significant differences in urine citrate concentrations, pH values, and oxalate/creatinine, citrate/creatinine, and calcium/creatinine ratios between the groups (all p < 0.05). The mean citrate/creatinine ratio was 21.13 ± 0.44 in the control group, 17.31 ± 3.82 in the distal obstruction group, and 15.48 ± 1.87 in the proximal obstruction group. Regarding the degree of obstruction, urine citrate concentrations, pH values, and citrate/creatinine were lower, and the oxalate/creatinine ratio was higher in severe obstruction than in mild obstruction (p < 0.05). This study represents an initial attempt to evaluate a model of partial ureteral obstruction and urolithiasis. The findings indicate that obstruction alters urinary parameters, such as citrate and pH, indirectly increasing the risk of stone formation. Furthermore, stone formation in an obstructed urinary system appears to be a complex process. However, metabolic evaluation and treatment may help prevent stone formation in patients with ureteral obstruction.
Similar content being viewed by others

Introduction
Kidney stones occur in approximately 10% of adults, and their frequency is increasing1. The prevalence of kidney stones varies with age, sex, genetics, dietary habits, and geographical location2. If the factors that cause stone formation are not adequately addressed, kidney stones can recur at a rate of approximately 50% 10 years after the initial diagnosis3. Calcium oxalate stones are the most common stone composition in children and adults in developed countries4.
Many risk factors have been identified in the formation of urinary system stone disease. These risk factors include anatomical disorders, such as ureteropelvic and ureterovesical junction obstructions and ureteral strictures that cause urinary stasis. These congenital abnormalities are the most important cause of end-stage renal failure, especially in children5. Metabolically, urinary parameters such as hypocitraturia, hypercalciuria, and low or high urine pH encourage stone formation3,6.
Ureteral obstructions can occur at different levels and severities. Many surgical options are available for ureteral obstructions and kidney stones. However, applying the ideal treatment for urinary system stone disease, which can occur with ureteral obstruction, and making the decision to undergo simultaneous surgery are difficult7,8.
Unilateral ureteral obstruction has been widely studied in animals, and this model is a suitable research tool for evaluating renal damage because it can reliably induce tubular damage and interstitial fibrosis9. Animal studies have shown that daily intra-abdominal glyoxylate injections produce calcium oxalate nephrolithiasis, and renal crystal accumulation increases in the first week and then decreases and disappears on the 15th day10.
However, the relationship between the level and severity of the structure causing urinary stasis and stone formation is unknown. Therefore, this study aimed to determine the effects of anatomical disorders on kidney stone formation using a unilateral ureteral obstruction and nephrolithiasis rat model.
Materials and methods
This study was conducted by Sakarya University Animal Testing Local Ethics Committee approval in Sakarya University Experimental Research and Medical Centre. Forty Wistar Albino adult (8-week-old) male rats obtained from Sakarya University Experimental Research and Medical Center were used in this study. Each experimental group included eight rats. The rats were divided into the following five groups: controls (sham surgery; control group), mild partial obstruction in the unilateral distal ureter (mild distal obstruction group), severe partial obstruction in the unilateral distal ureter (severe distal obstruction group), mild partial obstruction in the unilateral proximal ureter (mild proximal obstruction group), and severe partial obstruction in the unilateral proximal ureter (severe proximal obstruction group).
Animal care and experimental procedure
The principles of 3Rs (Replacement, Reduction, and Refinement) were followed from the study design to the termination. In this context, the animals were housed in a standard polypropylene rat cage under standardized laboratory conditions (night/day: 12 h light/12 h dark, temperature 21 ± 2 ºC, humidity 55%) and fed with pellet feed and water. To prevent postoperative pain, paracetamol (2 mg/mL) was added to the drinking water until the 12th postoperative day when the study was terminated.
Sample size determination
The determination of group size was based on previous studies using a partial ureteral obstruction in an animal model, which included an a priori power analysis. The study conducted by Cimen et al., which utilized the partial ureteral obstruction model, was taken as a reference in determining the sample size11. The a priori power analysis of our study was conducted using the G*Power (version 3.1.9.6, Franz Faul, Universitat, Kiel, Germany). In our study, for a power of 0.95, an alpha value of 0.05 and an effect size of 0.73, the number of animals required was 8 per group. Therefore, the sample size was determined as 40 rats for 5 groups.
Procedures
Surgical procedure (day 0)
Eight-week-old male rats were prepared for the surgical procedure and administered 40 mg/kg of 10% ketamine hydrochloride (Ketalar; Pfizer, Istanbul, Turkey) and 8 mg/kg xylazine (Rompun; Bayer, Istanbul, Turkey) intraperitoneally, and anaesthesia was achieved. The abdominal skin of the rats was shaved before surgery, and laparotomy was performed with a midline incision under sterile conditions. The skin of the control group was closed with 4/0 nylon sutures without any intervention. In the mild distal obstruction group, after the right ureter was released from the distal level, unilateral mild partial ureteral obstruction was created by ligating it with 4/0 nylon suture over a 0.6-mm diameter steel wire. In the severe distal obstruction group, after the right ureter was released from the distal level, unilateral severe partial ureteral obstruction was created by ligating it with 4/0 nylon suture over a 0.3-mm diameter steel wire (Fig. 1). In the mild proximal obstruction group, after the proximal right ureter (from the ureteropelvic junction) was released, unilateral mild partial ureteral obstruction was created by tying it with 4/0 nylon suture over a 0.6-mm diameter steel wire. In the severe proximal obstruction group, after the proximal right ureter (from the ureteropelvic junction) was released, unilateral severe partial ureteral obstruction was created by tying it with 4/0 nylon suture over a 0.3-mm diameter steel wire. After these procedures, the subcutaneous area and skin were closed with a 4/0 monofilament absorbable suture (Fig. 2).

Surgical procedures performed on the groups of rats with obstruction at the distal level (mild distal obstruction and severe distal obstruction groups): (a) Dissection of the distal ureter; (b) Knotting of the ureter using steel wire; (c) Appearance after removing the wire and cutting the suture.

Surgical procedures performed on the groups of rats with obstruction at the proximal level (mild proximal obstruction and severe proximal obstruction groups): (a) Dissection of the ureteropelvic junction; (b) Knotting of the ureter using steel wire; (c) Cutting the suture after removing the wire.
Glyoxylate injection (day 7)
After 7 days, intraperitoneal administration of glyoxylic acid solution (glyoxylic acid solution, Sigma-Aldrich, Germany) at a dose of 120 mg/kg/day was initiated in all groups. The rats were injected with glyoxylic acid for 5 days.
Performing bilateral nephrectomy (day 12)
The rats were anaesthetised by intraperitoneal administration of 40 mg/kg of 10% ketamine hydrochloride (Ketalar; Pfizer) and 8 mg/kg of xylazine (Rompun; Bayer). The abdominal skin of the rats was shaved. Laparotomy was performed with a midline incision under sterile conditions. During surgery, intracardiac blood samples were collected, and the rats were sacrificed using the exsanguination method. The right kidney was identified, and the renal artery and renal vein were cut. The ureter was also cut at the proximal level. The same procedure was applied to the left kidney, and the specimens were treated separately with 10% formaldehyde solution as the right kidney and left kidney. Urine was collected from the bladder of each rat using a syringe.
Histopathological examination
The size of the rat kidneys was measured before histopathological evaluation. After the kidney tissues were sectioned, haematoxylin and eosin staining was performed. The degree of hydronephrosis was assessed and the EGTI (Endothelial, Glomerular, Tubular, and Intersitisyel) scoring system, which scores tubular damage, endothelial damage, glomerular damage, and tubulointerstitial damage, was used to determine renal damage12.
To evaluate calcium oxalate crystal accumulation, sections stained with haematoxylin and eosin were classified into four grades. According to the Pizzolato classification, five areas were examined at ×100 magnification, and 0.1-mm crystals were counted and the average crystal count of the five areas was calculated. This system is graded as follows: Grade 0, 0 crystals/field; Grade 1, < 5 crystals/field; Grade 2, 5–10 crystals/field; and Grade 3, > 10 crystals/field13 (Fig. 3).

Histological evaluation of representative rat kidney cortex sections according to the Pizzolato classification ((a) Grade 0; (b) Grade 1; (c) Grade 2; (d) Grade 3). Arrows show crystals in sections of renal cortex (haematoxylin and eosin staining, x100 magnification.
Biochemical examination
Urea(mg/dl) and creatinine (mg/dl) concentrations were measured in the blood collected on the day that the glyoxylic acid injection started (day 7) and on the day that the study ended (day 12). On the day that the study ended (day 12), concentrations of oxalate (mmol/l), calcium (mg/dl), citrate (g/ml), magnesium (mg/dl), phosphate (mg/dl), and creatinine (mg/dl) and the pH were examined in urine collected from the bladder using a syringe. We calculated the oxalate/creatinine, citrate/creatinine, and calcium/creatinine ratios.
Statistical analysis
Statistical analyses were conducted using SPSS (version 26, Chicago, IL, USA). Differences between groups were evaluated using the Kruskal–Wallis test for non-parametric data and one-way analysis of variance for parametric data. Chi-square test or Fisher’s exact test was used to test the relationships between categorical data. The Spearman correlation test was used to determine relationships. A p value < 0.05 was considered statistically significant.
Results
Biochemical findings
Serum creatinine levels were compared between the groups on the seventh day and at the end of the study. The first serum creatinine mean was 0.20 ± 0.02 in the control group and 0.27 ± 0.07 in the obstruction group. The final serum creatinine mean was 0.50 ± 0.18 in the control group and 0.62 ± 0.16 in the obstruction group. We found that the first serum creatinine value was significantly higher in the obstruction group compared to the control group (p < 0.001), and there was no difference in the final serum creatinine value (p = 0.115).
Urinary parameters were examined according to the level and degree of obstruction. For the mild obstruction groups, the mild distal and mild proximal obstruction subgroups were combined. Similarly, for the severe obstruction groups, the severe distal and severe proximal obstruction subgroups were combined. Additionally, within the distal obstruction groups, the mild and severe distal obstruction subgroups were grouped together, while for the severe obstruction groups, the severe distal and severe proximal obstruction subgroups were also combined.
We found that the citrate/creatinine ratio was significantly lower in the distal obstruction groups (mild distal obstruction group and severe distal obstruction group) and proximal obstruction groups (mild proximal obstruction group and severe proximal obstruction group) compared to the control group (p < 0.001). There were differences between the degree of obstruction and citrate concentrations, pH, and citrate/creatinine and oxalate/creatinine ratios. In mild obstruction groups (mild distal obstruction group and mild proximal obstruction group), citrate values were significantly higher than in the control group and severe obstruction groups(severe distal obstruction group and severe proximal obstruction group) (p = 0.002). In severe obstruction groups, urine pH was significantly lower than in the control group and mild obstruction groups (p < 0.001). In mild and severe obstruction groups, citrate/creatinine ratio was significantly lower than in the control group (p < 0.001). In mild obstruction groups, oxalate/creatinine ratio was significantly lower than in the control group (p = 0.041). (Tables 1 and 2).
When urine parameters were evaluated using the Pizzolato crystal score, we found that groups with crystal scores of 1 and 2 had significantly higher oxalate concentrations and oxalate/creatinine ratio than those with crystal scores of 0 (Table 3).
Right renal pelvis diameter, EGTI score and urinary parameters were examined. We found that magnesium, phosphate, and creatinine values were positively correlated (p = 0.002, p = 0.014, p = 0.002, respectively), and the citrate/creatinine ratio was negatively correlated (p = 0.025) with the pelvic diameter. However, no correlation was found when the right renal EGTI score and urine parameters were examined (Table 4).
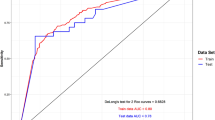
Acidic or basic urine pH was not related to the right kidney crystal score (p = 0.502) (Fig. 4).
Mean ± SD is shown in the table.

Evaluation of the right renal crystal score according to the pH (\(\:{X}^{2}\) = 3.031, p < 0.502)
Histopathological findings
The parenchymal thickness and pelvic diameter were significantly different between the groups (p = 0.005 and p = 0.001, respectively). There was no difference in the EGTI renal damage score or Pizzolato crystal score between the groups (Tables 5 and 6).
Discussion
It has been reported in studies that ureteropelvic junction obstruction and stone disease are seen together at a rate of 20%8. However, studies indicating the incidence between ureterovesical junction stricture and stone formation are limited.
When serum creatinine levels were examined in the control and obstruction group, the first serum creatinine value was higher in the obstruction group, while no difference was observed in the final serum creatinine value. In previous studies, it was shown that the increase in serum creatinine value on day 10 in the partial obstruction model was not significant14. Furthermore, no correlation was found between histologically EGTI score and urine parameters. The results in our study may be due to the physiological response of the kidney and the injection of glyoxylic acid administered to all rats.
In this study, we performed spot urine analysis. Twenty-four-hour urine collection creates difficulties in daily practice compared with spot urine analysis. Many studies have compared a 24-hour urine analysis with a spot urine analysis, showing that a spot urine analysis can be used to analyse urine metabolites15,16,17.
In the present study, we found that the oxalate value and oxalate/creatinine ratio are significantly higher in rats with crystal scores of 1 and 2 than in rats with crystal scores of 0. Moreover in one rat, the right kidney crystal score was evaluated as 3. Our findings showed that the oxalate/creatinine ratio is important in crystal formation, but this ratio decreases in the presence of mild obstruction. We recommend that the oxalate/creatinine ratio can be used in the management of patients with urinary stasis because it indicates the onset of stone formation.
Twenty-four-hour urine analysis shows that low citrate concentrations, high urine pH, high calcium concentrations, and the presence of oxalate are risk factors for calcium oxalate stone formation18. In the present study, we found that oxalate concentrations and the oxalate/creatinine ratio were related in crystal formation, and there were no relationships between citrate, pH, and calcium values and calcium oxalate crystals.
Alelign and Petros showed that a urine pH between 5.0 and 6.5 is a risk factor for calcium oxalate stone formation19. In contrast, in the present study, no relationship was found between pH ≤ 6.5 and crystal formation. However, a significant relationship was found between the severity of obstruction and pH ≤ 6.5. All rats (n = 8) with pH ≤ 6.5 were observed to have severe obstruction. Our findings suggest that severe obstruction is a risk factor for stone formation in some types of stones by decreasing the pH level.
It is known that epithelial injury and progressive inflammation is caused by CaOx crystals, rather than CaOx crystals forming secondary to renal damage20. In our study, no difference was found in right kidney EGTI renal damage score between the groups. The level and degree of obstruction did not have a statistically significant impact on renal injury. The intraperitoneal glyoxylic acid injection administered to all groups may have caused this outcome.
To the best of our knowledge, no studies have performed a urine analysis in patients with uterovesical junction obstruction. In the present study in which urine parameters of the control group and the groups with uterovesical junction obstruction were evaluated, we found that the citrate/creatinine ratio was lower in the groups with uterovesical junction obstruction than in the control group.
Wang et al. showed that there was no difference in the recurrence of stones between patients with and those without urinary system anomalies. In addition, they highlighted that parameters such as urine volume, calcium, citrate, and phosphate play a significant role in the recurrence of kidney stones21. Our study showed that ureteral obstruction did not directly cause crystal formation, but urinary metabolites played a role in crystal formation, and the results of our study are consistent with with those of the meta-analysis by Wang et al.
Medical treatment is used in the prophylaxis of urinary system stone disease. Potassium citrate has been demonstrated to reduce stone recurrence in patients with calcium oxalate stones by lowering urinary calcium levels and increasing urinary citrate concentration22. Furthermore, the ILLUMINATE-B study, which evaluated the efficacy and safety of Lumasiran in patients with hyperoxaluria type 1, it was shown that oxalate and oxalate/creatinine ratio decreased with treatment and nephrocalcinosis decreased at 12-month follow-up23.
It is clinically difficult to apply the ideal treatment for urinary system stone disease that can be seen together with ureteral obstruction and to decide on simultaneous surgical intervention. Moaveni et al. reported in a study of 76 patients with unilateral ureteropelvic junction obstruction that 2 (8%) of 26 patients with supranormal differential renal function required pyeloplasty at 9-month follow-up. This study recommends an individualized management plan for ureteropelvic junction obstruction in the decision of conservative follow-up or pyeloplasty24.
Previous studies have demonstrated that animal models of ureteropelvic junction obstruction closely replicate human pathology5. As a result of our study, we believe that a personalized treatment or follow-up plan should be established after metabolic evaluation such as spot urine or 24-hour urine analysis in patients with urinary tract stones with ureteral obstruction. Regulation of abnormal oxalate level, oxalate/creatinine ratio and urine pH detected in urine analysis can prevent patients with urinary stasis from unnecessary surgical interventions.
Conclusion
This study suggests that the level and degree of ureteral obstruction do not directly cause kidney stones. Urinary stasis changes parameters such as citrate, pH, and the citrate/creatinine ratio in urine. Changes in urinary citrate and pH, along with a decreased citrate/creatinine ratio in patients with urinary stasis, these patients are indirectly at risk for stone formation. Treating kidney stones and ureteral obstruction simultaneously can involve major surgery for patients. Therefore, in patients with upper urinary tract obstruction, additional surgical procedures can be avoided by examining urinary parameters and providing medical treatment. Evaluating urinary parameters may also be useful in follow-up after stone surgery or unsuccessful ureteral stenosis surgery.
Data availability
The authors confirm that the data supporting the findings of this study are available within the article.
References
Singh, P., Harris, P. C., Sas, D. J. & Lieske, J. C. The genetics of kidney stone disease and nephrocalcinosis. Nat. Rev. Nephrol. 18 (4), 224–240. https://doi.org/10.1038/s41581-021-00513-4 (2022).
Dirie, N. I. et al. The prevalence of urolithiasis in subjects undergoing computer tomography in selected referral diagnostic centers in Mogadishu, Somalia. Front. Public. Health. 11, 1203640. https://doi.org/10.3389/fpubh.2023.1203640 (2023).
Song, L., Maalouf, N. M. & Nephrolithiasis [Updated 2020 Mar 9]. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. https://www.ncbi.nlm.nih.gov/books/NBK279069/ Accessed 8 December 2024.
Fontenelle, L. F. & Sarti, T. D. Kidney stones: treatment and prevention. Am. Family Phys. 99 (8), 490–496 (2019).
Klein, J. et al. Congenital ureteropelvic junction obstruction: human disease and animal models. Int. J. Exp. Pathol. 92 (3), 168–192. https://doi.org/10.1111/j.1365-2613.2010.00727.x (2011).
Reynolds, T. M. ACP best practice 181: chemical pathology clinical investigation and management of nephrolithiasis. J. Clin. Pathol. 58 (2), 134–140. https://doi.org/10.1136/jcp.2004.019588 (2005).
Krings, G. et al. Ureteropelvic junction obstruction and renal calculi: simultaneous treatment by robot-assisted laparoscopic pyeloplasty and transcutaneous retrograde flexible ureteroscopy. Technique description and early outcomes. Progres En urologie: journal de l’association Francaise d’urologie. Et De La. Societe Francaise D’urologie. 33 (5), 279–284. https://doi.org/10.1016/j.purol.2023.01.006 (2023).
Scarcella, S. et al. Combined treatment of ureteropelvic junction obstruction and renal calculi with robot-assisted laparoscopic pyeloplasty and laser lithotripsy in children: case report and non-systematic review of the literature. Int. J. Med. Rob. + Comput. Assist. Surgery: MRCAS. 17 (3), e2246. https://doi.org/10.1002/rcs.2246 (2021).
Takenaka, M. et al. Effect of Beraprost sodium (BPS) in a new rat partial unilateral ureteral obstruction model. Prostaglandins Leukot. Essent. Fat. Acids. 80 (5-6), 263–267. https://doi.org/10.1016/j.plefa.2009.03.002 (2009).
Okada, A. et al. Genome-wide analysis of genes related to kidney stone formation and elimination in the calcium oxalate nephrolithiasis model mouse: detection of stone-preventive factors and involvement of macrophage activity. J. Bone Mineral. Research: Official J. Am. Soc. Bone Mineral. Res. 24 (5), 908–924. https://doi.org/10.1359/jbmr.081245 (2009).
Çimen, S. et al. Protective effects of Ghrelin on kidney tissue in rats with partial ureteral obstruction. Turk. J. Med. Sci. 49 (2), 696–702. https://doi.org/10.3906/sag-1802-17 (2019).
Khalid, U. et al. Kidney ischaemia reperfusion injury in the rat: the EGTI scoring system as a valid and reliable tool for histological assessment. J. Histol. Histopathology. 3 (1), 1. https://doi.org/10.7243/2055-091X-3-1 (2016).
Pizzolato, P. Histochemical recognition of calcium oxalate. J. Histochem. Cytochemistry: Official J. Histochem. Soc. 12, 333–336. https://doi.org/10.1177/12.5.333 (1964).
Zhu, W. et al. Establishment and observation of a new and ideal reversible model of PUUO. Ren. Fail. 39 (1), 222–228. https://doi.org/10.1080/0886022X.2016.1256318 (2017).
Williams, J. C., Gambaro, G., Rodgers, A., Asplin, J., Bonny, O., Costa-Bauzá, A.,Ferraro, P. M., Fogazzi, G., Fuster, D. G., Goldfarb, D. S., Grases, F., Heilberg,I. P., Kok, D., Letavernier, E., Lippi, G., Marangella, M., Nouvenne, A., Petrarulo,M., Siener, R., Robertson, W. G. Urine and stone analysis for the investigation of the renal stone former: a consensus conference. Urolithiasis, 49(1), 1–16. https://doi.org/10.1007/s00240-020-01217-3 (2021).
Rodriguez, A., Baccaro, R., Gambaro, G. & Ferraro, P. M. Urinary supersaturation on fractioned urine collections: which urine sample can explain better the variability observed on 24-h urine? A proof-of-concept study. Urolithiasis 48 (5), 403–408. https://doi.org/10.1007/s00240-020-01177-8 (2020).
Paccaud, Y. et al. Spot urine samples to estimate 24-hour urinary calcium excretion in school-age children. Eur. J. Pediatrics. 179 (11), 1673–1681. https://doi.org/10.1007/s00431-020-03662-z (2020).
Adomako, E. A., Li, X., Sakhaee, K., Moe, O. W. & Maalouf, N. M. Urine pH and citrate as predictors of calcium phosphate stone formation. Kidney360 4 (8), 1123–1129. https://doi.org/10.34067/KID.0000000000000184 (2023).
Alelign, T. & Petros, B. Kidney Stone Disease: An Update on Current Concepts. Adv. Urol. 2018, 3068365. https://doi.org/10.1155/2018/3068365 (2018).
Geraghty, R., Wood, K. & Sayer, J. A. Calcium oxalate crystal deposition in the kidney: identification, causes and consequences. Urolithiasis 48 (5), 377–384. https://doi.org/10.1007/s00240-020-01202-w (2020).
Wang, K. et al. Risk factors for kidney stone disease recurrence: a comprehensive meta-analysis. BMC Urol. 22 (1), 62. https://doi.org/10.1186/s12894-022-01017-4 (2022).
Solak, V., Gökce, M. İ. & Yaman, Ö. Potassium citrate vs. hydrochlorothiazide to reduce urinary calcium excretion in calcium oxalate stone patients with hypercalciuria: a prospective randomized study. Int. Urol. Nephrol. 53 (9), 1791–1796. https://doi.org/10.1007/s11255-021-02879-7 (2021).
Hayes, W. et al. Efficacy and safety of Lumasiran for infants and young children with primary hyperoxaluria type 1: 12-month analysis of the phase 3 ILLUMINATE-B trial. Pediatr. Nephrol. 38 (4), 1075–1086. https://doi.org/10.1007/s00467-022-05684-1 (2023).
Moaveni, A. K., Neishabouri, A., Paymani, Z., Haghighi, F. & Kajbafzadeh, A. M. Supranormal renal function in pediatric ureteropelvic junction obstruction: a multiparameter analysis to guide clinical management. Int. Urol. Nephrol. https://doi.org/10.1007/s11255-025-04369-6 (2025).
Funding
This work was supported by Sakarya University Scientific Research Projects Coordination Unit. (SAÜ, BAP, Project Number:2022-7-25-102)
Author information
Authors and Affiliations
Contributions
KD, HSS, EC: proposed research point and design, the biological experiments, the biochemical analysis, and its statistical analysis. KD, HSS, BE handled the methods, results, and statistical analysis of histopathological evaluations. KD, HSS, HIC wrote the manuscript and conducted an interpretation of the data. All authors have read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical standards
We confirm that this study is implemented in accordance with the Animal Research Reporting in Live Experiments (ARRIVE) guidelines.
Ethics approval
The questionnaire and methodology for this study was approved by the Sakarya University Animal Experiments Local Ethics Committee. (Ethics approval number:22, 06/04/2022). A scanned copy of the ethics review approval document has been uploaded to the submission website.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Demirhan, K., Saglam, H.S., Cimen, H.I. et al. Effect of the location and severity of partial ureteral obstruction on urinary system stone disease formation. Sci Rep 15, 11560 (2025). https://doi.org/10.1038/s41598-025-96879-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-96879-7
