
Abstract
Suicide causes over 700,000 deaths annually worldwide. Mental disorders are closely linked to suicidal ideation, but predicting suicide remains complex due to the multifaceted nature of contributing factors. Traditional assessment tools often fail to capture the interactions that drive suicidal thoughts, underscoring the need for more sophisticated predictive approaches. This study aimed to predict suicidal and self-harm ideation among university students using machine learning models without relying on suicidal behavior related predictors. The goal was to uncover less obvious risk factors and provide deeper insights into the complex relationships between psychiatric symptoms and suicidal ideation. Data from 924 university students seeking mental health services were analyzed using seven machine learning algorithms. Suicidal ideation was assessed through the 9th item of the Patient Health Questionnaire-9. Three predictive models were developed, with the final model utilizing only subdomains from the DSM-5 Level 1 Self Rated Cross-Cutting Symptom Measure. Feature importance was assessed using SHAP and Integrated Gradients techniques. To ensure model generalizability, the best-performing model was externally validated on a separate dataset of 361 individuals. Machine learning models achieved strong predictive accuracy, with logistic regression and neural networks reaching AUC values of 0.80. The final model achieved an AUC of 0.80 on the training data and 0.79 on external validation data. Key predictors of suicidal ideation included personality functioning and depressed mood (both increasing the likelihood), while anxiety and repetitive thoughts were associated with a decreased likelihood. The use of non-suicidal predictors across datasets highlighted psychiatric dimensions relevant to early intervention. This study demonstrates the effectiveness of machine learning in predicting suicidal ideation without relying on suicide-specific inputs. The findings emphasize the critical roles of personality functioning, mood, and anxiety in shaping suicidal ideation. These insights can enhance early detection and personalized interventions, especially in individuals reluctant to disclose suicidal thoughts.
Similar content being viewed by others

Introduction
Suicide causes over 700,000 deaths annually, representing 1.3% of total deaths, with 58% occurring in individuals under 501. According to recent reports by the World Health Organization (WHO), suicide, which previously ranked as the second leading cause of death among individuals aged 15–29, has dropped to fourth place, following road traffic accidents, tuberculosis, and interpersonal violence. These reports also indicate a decrease of approximately 100,000 in the total number of suicide deaths1,2. This trend may be seen as a positive outcome of better access to psychiatric services; studies show that suicide-related deaths rise when access to mental health care decreases, while they decrease with improved access3,4. Similarly in terms of age group, among the 4061 suicide cases reported in Turkiye in 2023, the highest number of suicides occurred in the 20–29 age group, which accounted for 27% of total suicide deaths5, still underlining the importance of ongoing research to explain suicide.
Efforts to explain suicide began with Durkheim’s sociological approach (1897)6, yet no single explanation has prevailed7. Biological Suicide Theory emphasizes altered stress responses and serotonergic neurotransmission, whereas Hopelessness Theory links depression-induced hopelessness to suicide8,9. Klonsky and May’s (2015) Three-Step Theory suggests suicidal desire stems from pain and hopelessness, it increases when pain outweighs connectedness, and escalates to attempts with sufficient capability10. On the other hand, mental disorders strongly correlate with suicide11; 87% of suicide decedents has prior psychiatric diagnoses12, and some specific disorders significantly elevate suicide risk—psychotic disorders by 13.2-fold and mood disorders by 12.3-fold13. According to a recent review and meta-analysis study, depression, borderline personality disorder, and schizophrenia spectrum disorders represent the most substantial risk factors for suicide among all mental disorders14. However, mental disorders alone poorly predict attempts due to additional factors15. A psychological autopsy showed 37% of suicide cases lacked diagnosed mental disorders, underscoring subthreshold disorders and social influences16. Subthreshold eating disorders, psychosis, anxiety, post-traumatic stress disorder, and depression also significantly elevate suicidal ideation or attempt17,18,19,20,21. Further a comprehensive meta-analysis identified previous psychiatric hospitalization, prior suicide attempts, and past suicidal ideation as prominent risk factors7. Suicidal ideation involves thinking and planning of self-harm with intent to die22. Non-suicidal self-injury refers to self-harm without intent to die23. Suicidal ideation is a critical intervention point in preventing suicide attempt24. However, individuals may conceal suicidal thoughts due to factors like fear of stigmatization, hindering timely support25,26. Scale based screening tools help assess suicide risk27,28,29,30, but despite the established link between mental disorders and suicide11,12, existing tools like ASQ and C-SSRS27,28 offer only momentary assessments, failing to reveal underlying causes and these tools may provide only a snapshot of the current situation without elucidating underlying causes.
This study focuses on predicting suicidal ideation and self-harm ideation using symptoms of mental disorders from self-report scales and questionnaires, employing Machine Learning (ML) techniques. ML algorithms, particularly supervised learning with labeled data, enhance prediction accuracy in psychiatric studies and suicide prediction31,32. A meta-analysis found ML methods superior to traditional statistics in predicting suicide-related outcomes due to ML’s effective classification of large datasets, whereas statistical methods focus more on causal mechanisms33. A recent systematic review reported that 87% of studies achieved an AUC value of 70% or higher, with past suicide attempts and psychiatric diagnoses being the most predictive features34. However, many studies do not have an external validation sample, which is critical to evaluate the generalization performance of the ML model34,35,36.
In this study, routine psychometric and demographic data from graduate and undergraduate students who applied to Koç University Psychological Counseling and Therapy Center (KUPTEM) at two different intervals were used as ML model predictors. The primary goal was to identify psychiatric dimensions that most accurately explain suicidal ideation, without relying on data directly related to suicide (past attempts or thoughts). In most ML studies, past suicide attempts and thoughts are prominent predictors34, which avoids to explain the other psychiatric dimensions related to suicidal ideation25,26. The aim was to determine other dimensions predicting suicidal ideation hierarchically and directionally, using as few predictors as possible. Three ML models were created: the first with 32 predictors, the second reduced to 11, and the third using 13 variables directly related to psychiatric symptoms and disorders, utilizing only the subdomains of the DSM-5-TR Self-Rating Level 1 Cross-Cutting Symptom Scale (DSM-5 SRL1). Suicidal/self-harm ideation was assessed using the ninth question of the PHQ-9 questionnaire. Seven different classification algorithms capable of solving linear and non-linear relationships were employed. Models were trained on the first dataset and in order to address the previous gaps, externally validated machine learning models were developed for demonstrating reliability and generalizability. Using DSM-5 SRL1 subdomains, hierarchical importance and directional effects of psychiatric symptoms on suicidal ideation were identified.
Method
Participants
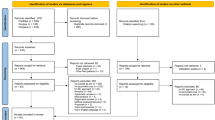
This study involved data from participants who had applied to the Koç University Psychological Counseling and Psychotherapy Center (KUPTEM), which is a comprehensive mental health clinic that provides various clinical services including individual psychotherapy, psychiatric consultation and treatment. It is not a regular counseling center, but more of a mental health clinic. When students initially contact KUPTEM either by email or by visiting the office, they are scheduled for an intake appointment by a clinical psychologist. Before the interview, a series of routine screening questions that help to determine the severity and immediacy of students’ concerns are used for a comprehensive evaluation to collaboratively determine the best management options for students. KUPTEM is committed to delivering culturally competent services that are responsive to the needs, strengths, and identities of Koç University’s diverse community of students. The services are free of charge. The psychopathology of the students that apply, may vary from mild adjustment disorder symptoms to borderline personality disorder with severe suicidal behavior and to schizophrenia. All students give an informed consent for the use of the anonymized scale data for academic purposes before filling the surveys. All applicants who were older than 18 years of age and who filled all the survey data fully and reliably were included in the analysis (Fig. 1). For the building of the machine learning model, a first group of participants’ data was collected from 924 students who applied between September 2019 and October 2022 ( Mean age: 23.54 ± 3.4. age range: 18–40, 66% women). Data from another group of participants composed of 361 students (Mean age: 22.25 ± 3.56, age range: 18–44, 61.5% women) who applied to KUPTEM between January 2023 and January 2024 was used as an external validation sample to use for Methods Sect. 2.8. The primary study and use of the validation sample study was approved by Koç University ethics committee (2022.478.IRB2.075). All procedures have been in accordance with the Declaration of Helsinki.

Flowchart of study representing data collection at two time points.
Suicidal ideation/self-harm definition
Suicidal ideation/self-harm was monitored with the answer to question 9 of the PHQ-9 scale. (“Thoughts that you would be better off dead, or of hurting yourself in some way?“). This question has answers in the range of 0 to 3. Responses other than 0 were accepted as 1 regardless of their severity and the target variable was converted into binary37. The dataset was naturally well-balanced, with 45% of participants reporting suicidal ideation/self-harm in the first dataset and 51.8% in the external validation dataset. Given this relatively balanced distribution between the classes, no additional balancing techniques (such as oversampling or undersampling) were required for the machine learning analysis. This natural balance in the data helps ensure that the models’ performance metrics are not biased by class imbalance issues, as research has shown that class imbalance only becomes problematic when the minority class represents less than approximately 20–25% of the majority class38.
While both the PHQ-9 and DSM-5 SRL1 assess suicidal/self-harm thoughts, question 9 of PHQ-9 was chosen to use as target variable for several reasons. The PHQ-9 question asks about ‘Thoughts that you would be better off dead, or of hurting yourself in some way,’ while the DSM-5 SRL1 item specifically asks about ‘Thoughts of actually hurting yourself.’ Despite their slightly different wording - the DSM-5 SRL1 focuses on active self-harm, while the PHQ-9 captures both thoughts of death and self-harm thought. On the other hand, the two items showed a strong correlation (Spearman’s ρ = 0.68, p < 0.001), which was computed with the scipy library39. Using the same binarization approach as question 9 of PHQ-9, the DSM-5 SRL1 item 11 responses showed 339 positive (presence of self harm ideation) and 585 negative (absence of self harm ideation) cases, which was also used for the further analysis to validate the model.
Psychometric scales and measures used in the study
DSM-5 self-rated level 1 cross-cutting symptom measure
This 23-item assessment tool evaluates major domains of psychopathology40. It covers thirteen domains including depression, anger, mania, anxiety, somatization, self-harm, psychosis, sleep disturbances, memory, repetitive thoughts, dissociation, personality functioning and substance use. The anhedonia (item 1) and mood (item 2) components of depression were used separately, and a total of 13 subdomains were used, excluding the self-harm subdomain (item 11). Turkish validation study was conducted by Çökmüş et al.41.
Patient health questionnaire (PHQ-9)
A nine-item instrument for screening and measuring depression severity29, with Turkish validity established in 201642.
Other assessment tools
Additional validated measures included the Mood Disorder Questionnaire43,44, SCOFF (Sick-Control-One-Fat-Food) Questionnaire for eating disorders45,46, Adult ADHD Self-Report Scale47,48, CAGE (Cut, Annoyed, Guilty, and Eye) Questionnaire for alcohol dependence49,50, General Anxiety Disorder-7 (GAD-7) scale for anxiety51,52, and Short Dissociative Experiences Scale for dissociative measures53,54,55. Scale details are summarized in Table 1.
Data preparation and preprocessing
Prior to model training, the predictors underwent a preprocessing step where they were scaled using a Min-Max Scaler to ensure that all variables were on the same scale, thus facilitating better performance across all machine learning algorithms. This step is critical, especially for models that are sensitive to the scale of input features, such as K-Nearest Neighbors (KNN) and Support Vector Machines (SVM).
Machine learning algorithms
Seven different ML algorithms were used in the study: KNN, Naive Bayes, Logistic Regression, Decision Trees, SVM, Random Forest, and Artificial Neural Networks (Fig. 2). First of all, the algorithms were used in the Python programming language with default hyperparameters in the scikit-learn library56. In order to reach the optimum performance of ML models, the hyperparameters were optimized by the Bayesian optimization method, due to its ability to efficiently find the optimum parameters in a high-dimensional and complex search space57. The MATLAB Classification Learner Toolbox was used to perform the optimization of algorithms other than logistic regression, as it is efficient with its parallel computation capability58. Logistic regression was optimized using the 0.10.1 version of the skopt, which integrates well with scikit-learn, due to the limitations of MATLAB’s optimization capabilities. In all machine learning models, the mean Receiver Operating Characteristic (ROC) Area Under the Curve (AUC) values were evaluated using a 5-fold cross-validation approach, both with default hyperparameters and during hyperparameter optimization. Additionally, a neural network with Multi-Layer Perceptron (MLP) architecture was developed for the prediction task using Keras deep learning framework59. The results of the machine learning models were visualized using the matplotlib library60.

Overview of the machine learning algorithms used in the study. Illustrations of: (A) KNN algorithm assigns a new data point to a group based on the proximity of its surrounding points. The green point is classified by identifying the predominant group among its closest neighboring points, shown within the circled area, (B) Naive bayes is a classification technique grounded in probabilistic principles, relying on the assumption that each attribute is independent of others. Each feature (Feature 1, Feature 2, Feature 3) contributes to determining the overall category of the observation, (C) Logistic regression especially binary logistic regression is a useful predictive approach for situations with two possible outcomes. The curve models how the attributes influence the likelihood of belonging to one of the two categories. It uses a logistic curve to express these probabilities. (D) Decision Tree is a hierarchical structure where the initial node splits the data into branches based on attribute values, eventually leading to final categories at the leaf nodes. Each split along the path is a decision made to classify data step-by-step, (E) SVM seeks to draw a dividing boundary that best separates different categories within the data. The boundary is drawn in such a way that it maximizes the margin between the nearest points of different categories, depicted by the dotted lines, (F) Random Forest is an ensemble technique that creates numerous decision trees. During classification, it collects the results from each tree and determines the final output by majority voting, capturing collective knowledge across trees, (G) Artificial Neural Network is a computational model organized in layers. Input data is processed through weighted connections in the network, where neurons in hidden layers transform the input, ultimately leading to a prediction at the output layer.
Machine learning prediction models
In the first model of the study, suicidal/self-harm ideation was tried to be predicted by using 32 features belonging to 924 individuals. The initial machine learning model was developed using a comprehensive set of predictors which encompassed a range of demographic, psychometric, and clinical variables thought to be relevant to suicidal ideation.
In the second model, it was aimed to simplify the predictive model by reducing the number of predictors. Specifically, the DSM-5 SRL1 scale items were replaced by the DSM-5 Self-Rating Level-1 scale total score, which reduced the number of predictors from 32 to 11.
Finally, the third model was developed using subdomains of the DSM-5 SRL1. These subdomains represent different psychiatric symptoms and disorders. The subdomains were derived from the original scale by summing the scores of relevant items and included anhedonia (item 1), depressed mood (item 2), anger (item 3), mania (item 4 + item 5), anxiety (item 6 + item 7 + item 8), somatization (item 9 + item 10), psychosis (item 12 + item 13), sleep (item 14), memory (item 15), repetitive thoughts (item 16 + item 17), dissociation (item 18), personality functioning (item 19 + item 20), and substance use (item 21 + item 22 + item 23)40. This model focused on understanding the contribution of specific psychiatric symptoms and disorders to suicidal ideation. Table 2 summarizes the predictors used across the models.
Neural network analysis
For the model using DSM-5 SRL1 subdomains, it was decided to build a more qualified neural network algorithm because, after adjusting the hyper-parameters of the algorithms, the neural networks showed the best performance in the third model. This neural network model with MLP architecture consisted of an input layer with the number of neurons corresponding to the number of features in the dataset (DSM-5 SRL1 subdomains) and two hidden layers with 64 and 32 neurons, respectively. The neural network was trained with the first data set of 924 participants. Non-linearity was ensured by using the Relu activation function between layers61. For binary classification, a sigmoid activation function was used in the output layer consisting of only one neuron62. The model was compiled using the Adam optimizer, which is highly capable in adaptive learning rate optimization, and the binary cross-entropy loss function63. The early stopping method was used to prevent overfitting64. If no increase in the validation AUC was observed for 10 epochs, training was stopped.
Two different methods were used to observe the hierarchical and directional contributions of the 13 subdomains of DSM-5 SRL1 to suicidal ideation. These methods are SHapley Additive exPlanations (SHAP) and Integrated Gradients, respectively. The SHAP method assigns feature importance values (SHAP values) based on game theory by comparing model predictions with and without each feature65. Integrated Gradients was also used to validate the SHAP results by accumulating gradients from a baseline to the actual inputs, providing a complementary and reliable assessment of feature importance66.
External validation of the neural network model
This model was validated using data from a second group of 361 individuals. This second group included 361 students who applied between January 2023 and January 2024. Mean age: 22.25 ± 3.56, age range: 18–44, 61.5% women. Applying weights and biases obtained from the training of initial dataset to a separate external validation dataset tested the model’s generalizability and accuracy in predicting suicidal ideation across diverse cohorts. Data underwent Min-Max scaling, with model performance evaluated by AUC.
Additionally, the final MLP model was assessed for further predicting the DSM-5 SRL1 item 11 responses using the same methodology.
Results
Machine learning models results
In the analysis for the first model, results indicated that logistic regression reached the highest mean AUC value of 0.78, while random forest followed closely behind with a mean score of 0.77. In contrast, the decision tree model had the lowest mean AUC value of 0.64. Other models such as neural networks and SVM exhibited mean AUC performances of 0.72 and 0.76, respectively (Fig. 3A). Post-tuning, all models showed significant improvements in terms of mean AUC value: KNN attained 0.76, logistic regression improved to 0.79, neural networks also hit 0.79, SVMs achieved 0.80, decision tree increased to 0.71, Ensemble method improved to 0.79, and Naive Bayes scored 0.75.
In the second model results revealed that logistic regression reached an AUC value of 0.80, neural networks and SVM showed mean AUC values of 0.78 and 0.77, respectively. In contrast, the decision tree model recorded the lowest mean AUC value at 0.64 (Fig. 3B). The mean AUC values obtained after optimization of the hyperparameters are as follows: KNN 0.75, logistic regression 0.80, neural networks 0.80, SVM 0.80, decision tree 0.75, ensemble methods 0.79 and naive bayes 0.75.
In the third (last) model logistic regression reached a mean AUC value of 0.75, followed by random forest and naive bayes with mean AUC values of 0.74. Decision tree model recorded the lowest mean AUC value of 0.553 (Fig. 3C). After hyperparameter optimization in the last model, the neural networks reached 0.76 mean AUC value. Table 3 shows the AUC values of the algorithms across the models after hyperparameter optimization. The optimized parameters are presented in Supplementary Table 1.


Machine learning models’ results with default hyperparameters. This figure presents the AUC values for seven different machine learning algorithms, evaluated on three different models with default hyperparameters. Illustrations of: (A) Logistic Regression reached the highest mean AUC value of 0.78, followed by Random Forest at 0.77. Neural Network and SVM scored 0.72 and 0.76 respectively. Decision Tree recorded the lowest score at 0.64 in the first model, (B) Logistic Regression again reached the highest mean AUC value of 0.80. Random Forest and SVM scores of 0.78 and 0.77, respectively. Decision Tree again recorded the lowest score at 0.64 in the second model, (C) Logistic Regression maintained the highest performance with a mean AUC value of 0.75. Random Forest and Naive Bayes followed closely at 0.74. Decision Tree performance declined to the lowest score of 0.55 in the last model.
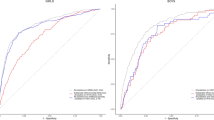
In the MLP based neural network model created with keras with the predictors used in the third model, the training AUC increased from around 0.450 to 0.850, while also the validation AUC increased with significant improvements, stabilizing around 0.800. This MLP model was evaluated on the external validation dataset. The model achieved an AUC value of 0.79 on the external validation data. Figure 4 illustrates the change in the loss and AUC performances of the MLP model built with Keras according to the epochs and external validation data set ROC curve respectively. Furthermore, when this MLP model was applied to predict DSM-5 SRL1 item 11 responses using the same binarization methodology as before, it achieved an AUC of 0.78.(Supplementary Fig. 1).

Performance evaluation of the neural network model built with keras. Illustrations of: (A) This plot shows the loss values over 30 epochs for both training and validation datasets. The training loss (blue line) and validation loss (orange line) decrease steadily, indicating improvement in model performance, (B) this plot depicts the AUC values over 30 epochs for both training and validation datasets. The training AUC (blue line) increases consistently, while the validation AUC (orange line) also improves, stabilizing around 0.800, (C) the ROC curve shows the true positive rate against the false positive rate for the external validation dataset. The model achieved an AUC value of 0.79, indicating similar performance on unseen data. The curve (blue line) demonstrates the trade-off between sensitivity and specificity, with the diagonal line (dashed) representing the performance of a random classifier.
Feature contribution analysis results
In the SHAP summary plot for the first dataset used to train the MLP model several features stand out as significant contributors to the model’s predictions of suicidal ideation (Fig. 5A). Personality functioning showed major positive impact, with higher values increasing predicted suicidal ideation. Anxiety exhibited strong negative influence, as increased SHAP values corresponded with decreased suicidal ideation probability. Similar to personality functioning, an increase in depressed mood score had an effect on increasing the probability of the model predicting suicidal ideation. The increase in repetitive thoughts decreased the model’s prediction probability of suicidal ideation.
In external validation (Fig. 5B), anxiety maintained its negative contribution to suicidal ideation probability. Personality functioning remained a robust positive predictor consistent with the first dataset. Notably, anger emerged as an influential feature in the external dataset. Depressed mood and repetitive thoughts maintained their respective positive and negative relationships with suicidal ideation probability across both datasets.

SHAP summary plots for MLP model predictions. Illustrations of: (A) First dataset used to train the MLP model, (B) external validation dataset, the plots display the impact of DSM5-SRL1 subdomains on model output. Each point represents an individual sample, with color indicating feature value (blue for low, red for high). Features are arranged vertically by their overall importance. The horizontal position of each point shows the SHAP value, representing the feature’s impact on the model prediction for that sample. Positive SHAP values (right of center) indicate an increase in the model’s output, while negative values (left of center) indicate a decrease. This reflects differences in feature impact magnitudes between the datasets. Key observations include the significant influence of Personality Functioning and Anxiety across both datasets, with notable differences in the relative importance of other features such as Depressed Mood and Anger between the training and validation data.
The Integrated Gradients analysis of the datasets revealed the relative contributions of the DSM-5 SRL1 subdomains to suicidal ideation prediction. Anxiety, anhedonia, depressed mood, repetitive thoughts, and personality functioning were among the top six predictors for both datasets. Anxiety and repetitive thoughts again showed negative contributions, while depressed mood, personality functioning, and anhedonia demonstrated positive contributions to the model’s predictions (Supplementary Table 2). Supplementary Fig. 2 and Supplementary Fig. 3 show the results of this analysis for the first and external dataset respectively.
Discussion
This study demonstrated that suicidal/self-harm ideation can be predicted by various ML algorithms without relying on suicide-specific predictors like past attempts or explicit thoughts. It is one of the first to predict suicidal ideation in a large university student sample using machine learning (ML) without depending on such predictors. Predicting suicidal ideation through routine psychometric assessments offers a discreet yet powerful tool for early intervention. Clinicians could integrate ML-based screening tools from models like this study into routine evaluations to identify high-risk students earlier, facilitating preventive interventions. These tools enable mental health professionals to focus on students who may not openly report suicidal ideation due to stigma or fear of consequences25. Furthermore, the results demonstrate potential for personalized mental health care. University services could tailor interventions based on specific psychiatric dimensions contributing most to suicidal ideation, such as depressive mood and personality functioning.
An ML model’s performance is considered moderate with accuracy of 0.70–0.79, good at 0.80–0.89, and excellent above 0.9067. In the three models created for this study with varying predictors, both linear and non-linear algorithms achieved good AUC value, especially after hyperparameter tuning. Logistic regression performed consistently well, and algorithms like SVM, neural networks, and random forest, which capture complex relationships, were also successful. This suggests suicidal ideation has both linear and intricate relationships with input features. These algorithms achieved above 0.90 AUC value in an adolescent suicide risk study68. However, their use of oversampling to address data imbalance may not generalize to real-world data. In another college study, an AUC of 0.80 was obtained using random forest, with 12-month suicidal ideation as the most important variable69. Similarly, a UK Biobank study achieved an AUC around 0.90, with past suicide attempt as a key feature70. It was emphasized that suicide-specific characteristics could significantly improve prediction accuracy but were excluded in this study as they may overshadow other contributing factors.
Notably, despite fewer predictors in the second model, the AUC value increased to 80%, in line with the aim of the study. In model 3, predicting suicidal ideation using only DSM-5 SRL1 subdomains was most successful with logistic regression, achieving an AUC of 0.755 using default parameters. Although initially underperforming, neural network performance improved after hyperparameter optimization, leading to a sophisticated MLP architecture that achieved an AUC of 0.80 on 924 participants and 0.79 on an external validation set of 361 participants. The model’s ability to predict outcomes on an independent dataset collected at a different time—without exposure during training—with similar accuracy underscores its reliability and generalizability35. Additionally, using the trained model to predict item 11 of the DSM-5 SRL1 (self-harm ideation), which was previously excluded during training, an AUC of 0.78 was obtained, further confirming its generalization capacity.
A notable feature of the final model is its reliance on psychiatric symptom predictors. Interpretability analyses using SHAP consistently highlighted personality functioning, anxiety, depressed mood, and repetitive thoughts among the top predictors, with uniform directional effects across datasets. Integrated Gradients supported these findings, similarly identifying anxiety, depressed mood, personality functioning, anhedonia, and repetitive thoughts as leading predictors. While feature importance rankings differed slightly due to methodological variations65,66, the consistent directionality and overlap reinforce the significance of these symptoms as key drivers of model predictions. This application of interpretable machine learning techniques aligns with recent recommendations emphasizing explainable artificial intelligence in clinical mental health research71.
Personality functioning was consistently among the top contributors in both data sets. The DSM-5 SRL1 assesses this with two basic questions: the first deals with the individual’s inability to recognize who they are and to know what they want from life, and the second deals with the inability to form close and enjoyable relationships. These questions explore the person’s identity, sense of purpose, and relationships with others. Deficits in these areas, such as difficulty connecting with others and lacking purpose, correlate with increased suicide risk, while having life purpose is protective72. Furthermore, the personality functioning domain is significantly negatively associated with self-esteem in college populations, and low self-esteem has been shown to significantly predict suicidal ideation73,74. Further supporting its importance, Lear and Pepper75 found that self-concept clarity, closely related to identity, is significantly associated with non-suicidal self-injury in college students75, and similar identity and relationship disturbances characterize borderline personality disorder, frequently associated with suicidal behaviors76,77.
While anxiety has a significant positive relationship with suicidal ideation in many studies78,79, our results showed increased anxiety associated with decreased likelihood of suicidal/self-harm ideation. This unexpected inverse relationship aligns with de Klerk et al.‘s analysis, revealing that somatic anxiety symptoms might protect against self-harm and suicidal ideation when controlling for other variables, highlighting the importance of differentiating anxiety subtypes in risk assessment80. Capron et al. also found that elevated anxiety sensitivity related to physical concerns may be protective against suicide risk among individuals with higher cognitive anxiety concerns81. These findings suggest that rather than anxiety directly decreasing suicidal ideation, the neural network model may capture complex interactions integrating increased anxiety with decreased ideation in its predictions.
The repetitive thoughts domain assesses symptoms related to obsessive-compulsive disorder (OCD). SHAP and Integrated Gradients analyses both indicated that increased repetitive thoughts were associated with decreased likelihood of suicidal ideation. While counterintuitive, this aligns with some of the existing findings. Fernández de la Cruz et al. found that comorbid anxiety disorders acted as a protective factor against suicide in a large OCD cohort82. Pellegrini et al. also found that lifetime comorbid anxiety disorder had a protective effect against suicidal ideation in OCD patients83.
Another point is that our ML models’ accuracy did not exceed 0.80. The type of data affects accuracy; a recent review showed that models using administrative data achieved an average AUC of 0.91, while survey data averaged 0.8084. Since this study also uses survey-based data, it is noteworthy to achieve this average. The mental disorder-related predictors used may also explain this result. Although mental disorders are highly associated with suicidal behavior, other factors predict it. O’Connor and Nock (2014) review evidence showing that interpersonal stressors and adverse life events are prominent risk factors for suicidal ideation and behavior, with findings demonstrating this relationship can persist even after controlling for mental disorders85. That underscores the need for future research to examine factors beyond psychiatric diagnoses, including adverse life events, interpersonal stressors, coping mechanisms, and social factors, to develop a more comprehensive understanding of suicide risk prediction. Biological samples and neuroimaging data may be other predictors to increase accuracy. Neuroimaging studies have revealed structural differences in brain regions linked to suicidal tendencies86,87,88. Potential biomarkers include abnormalities in serotonin signaling and inflammatory markers like IL-1β and IL-6 levels89,90. These markers may enhance prediction accuracy when used alongside neuroimaging data. While suicide prediction offers important benefits, such as early intervention and personalised prevention strategies, it should be considered that it also raises ethical concerns, such as privacy issues and false positive or negative risk.
The clinical relevance of this work is significant given that the 20–29 age group, which comprises 27% of suicide deaths in Türkiye5. In university mental health settings, stigma may prevent students from openly discussing suicidal thoughts25,26, making indirect assessment methods clinically valuable. Our machine learning approach surpasses traditional assessments by identifying suicide risk through routine psychiatric evaluations without explicit suicide-related questions, facilitating standardized screening across large student populations, and pinpointing psychiatric domains requiring clinical attention. Rather than replacing clinical judgment, these models help clinicians prioritize high-risk cases and guide targeted interventions. To mitigate overfitting36, external validation and model simplification strategies were used and achieved consistent performance across datasets. Predicting DSM-5 SLR1 item 11 responses further validated the model’s generalizability. Table 4 summarizes 10 studies predicting suicidal ideation via machine learning; notably, most studies employed internal validation methods, and 8 included suicide-specific predictors.
Several limitations of this study should be noted. The cross-sectional nature of our data means that while our models can identify concurrent associations between psychiatric symptoms and suicidal ideation, they cannot predict future suicidal behavior. The term “prediction” is used here in the machine learning sense, referring to the models’ ability to classify cases based on learned patterns, rather than temporal prediction of future events. Furthermore, our data do not include information on actual suicide attempts or completed suicides; the analysis is based solely on self-reported suicidal/self-harm ideation, which may not always translate to suicidal behavior. Additionally, the study was conducted exclusively within a college population, limiting generalizability. The unique characteristics of college students may influence psychiatric symptoms and their relationship to suicidal ideation differently from the general population. Therefore, caution should be exercised when applying these results to broader populations, and further research is needed across diverse settings. Our models were defined based on previous theoretical knowledge about psychiatric dimensions. Dimensionality reduction by principal component analysis (PCA) was not preferred due to its tendency to compromise interpretability. While PCA effectively reduces dimensionality, it transforms variables into principal components, making it difficult to interpret each predictor’s contribution99. Given the importance of interpretability and preserving the direct influence of original variables, PCA was not appropriate. Additionally, one main goal is to identify a single scale that clinicians can use to predict suicide risk. The direct relationship between original variables and the outcome is critical, supporting the decision to avoid PCA.
In conclusion, this study demonstrates that machine learning algorithms can effectively predict suicidal/self-harm ideation even without suicide-specific predictors such as past attempts or explicit suicidal thoughts. Findings emphasize the nuanced roles of cognitive and psychiatric factors, including personality functioning, depressed mood, anxiety, repetitive thoughts and anhedonia. Notably, inverse relationships between anxiety or repetitive thoughts and suicidal ideation challenge conventional assumptions, highlighting the complexity of these interactions. Limitations include reliance on survey-based data and restricted generalizability beyond university populations. Future research could incorporate biological markers like neuroimaging or inflammation biomarkers to enhance prediction accuracy. Overall, machine learning offers significant potential for improved early detection and targeted interventions in mental health care.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
World Health Organization. Suicide Worldwide in 2019: Global Health Estimates. (2021).
World Health Organization. Preventing Suicide: A Global Imperative (World Health Organization, 2014).
Hung, P., Busch, S. H., Shih, Y. W., McGregor, A. J. & Wang, S. Changes in community mental health services availability and suicide mortality in the US: A retrospective study. BMC Psychiatry. 20, 1–12 (2020).
Pirkola, S., Sund, R., Sailas, E. & Wahlbeck, K. Community mental-health services and suicide rate in Finland: A nationwide small-area analysis. Lancet 373, 147–153 (2009).
Türkiye İstatistik Kurumu (TÜİK). Ölüm ve Ölüm Nedeni İstatistikleri. (2024). Available at: https://data.tuik.gov.tr/Bulten/Index?p=Olum-ve-Olum-Nedeni-Istatistikleri–2024–53709
Durkheim, E. Suicide: A Study in Sociology (Routledge, 2005).
Franklin, J. C. et al. Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research. Psychol. Bull. 143, 187–232 (2017).
Oquendo, M. A. et al. Toward a biosignature for suicide. Am. J. Psychiatry. 171, 1259–1277 (2014).
Beck, A. T. Hopelessness as a predictor of eventual suicide. Ann. N Y Acad. Sci. 487, 90–96 (1986).
Klonsky, E. D. & May, A. M. The three-step theory (3ST): A new theory of suicide rooted in the ideation-to-action framework. Int. J. Cogn. Ther. 8, 114–129 (2015).
Ferrari, A. J. et al. The burden attributable to mental and substance use disorders as risk factors for suicide: findings from the global burden of disease study 2010. PLoS One. 9, e91936 (2014).
Arsenault-Lapierre, G., Kim, C. & Turecki, G. Psychiatric diagnoses in 3275 suicides: A meta-analysis. BMC Psychiatry. 4, 1–11 (2004).
Too, L. S. et al. The association between mental disorders and suicide: A systematic review and meta-analysis of record linkage studies. J. Affect. Disord. 259, 302–313 (2019).
Favril, L., Yu, R., Uyar, A., Sharpe, M. & Fazel, S. Risk factors for suicide in adults: systematic review and meta-analysis of psychological autopsy studies. BMJ Ment Health. 25, 148–155 (2022).
Nock, M. K. Why do people hurt themselves? New insights into the nature and functions of self-injury. Curr. Dir. Psychol. Sci. 18, 78–83 (2009).
Milner, A., Sveticic, J. & De Leo, D. Suicide in the absence of mental disorder? A review of psychological autopsy studies across countries. Int. J. Soc. Psychiatry. 59, 545–554 (2013).
Lipson, S. K. & Sonneville, K. R. Understanding suicide risk and eating disorders in college student populations: results from a National study. Int. J. Eat. Disord. 53, 229–238 (2020).
Yates, K. et al. Association of psychotic experiences with subsequent risk of suicidal ideation, suicide attempts, and suicide deaths: A systematic review and meta-analysis. JAMA Psychiatry. 76, 180–189 (2019).
Gilmour, H. Threshold and subthreshold generalized anxiety disorder (GAD) and suicide ideation. Stat. Can., 13–21 (2016).
Kim, H. Y. et al. Prevalence of lifetime psychiatric disorders and suicidality in adults with subthreshold posttraumatic stress disorder: A population-based nationwide study in Korea. Psychol. Trauma. (2021).
Balázs, J. et al. Adolescent subthreshold depression and anxiety: psychopathology, functional impairment and increased suicide risk. J. Child. Psychol. Psychiatry. 54, 670–677 (2013).
Centers for Disease Control and Prevention & Definitions Self-directed violence. Injury Prev. Control: Div. Violence Prev. (2015).
Crosby, A., Ortega, L. & Melanson, C. Self-directed violence surveillance: uniform definitions and recommended data elements. Centers Disease Control Prev. (2011).
Jobes, D. A. & Joiner, T. E. Reflections on suicidal ideation. Crisis 40, 227–230 (2019).
Hom, M. A., Stanley, I. H., Podlogar, M. C. & Joiner, T. E. Are you having thoughts of suicide? Examining experiences with disclosing and denying suicidal ideation. J. Clin. Psychol. 73, 1382–1392 (2017).
Hallford, D. J. et al. Disclosure of suicidal ideation and behaviours: A systematic review and meta-analysis of prevalence. Clin. Psychol. Rev. 101, 102272 (2023).
Horowitz, L. M. et al. Ask Suicide-Screening questions (ASQ): A brief instrument for the pediatric emergency department. Arch. Pediatr. Adolesc. Med. 166, 1170–1176 (2012).
Posner, K. et al. The Columbia–Suicide severity rating scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am. J. Psychiatry. 168, 1266–1277 (2011).
Kroenke, K., Spitzer, R. L. & Williams, J. B. The PHQ–9: validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613 (2001).
Osman, A. et al. The suicidal behaviors Questionnaire-Revised (SBQ-R): validation with clinical and nonclinical samples. Assessment 8, 443–454 (2001).
Chekroud, A. M. et al. The promise of machine learning in predicting treatment outcomes in psychiatry. World Psychiatry. 20, 154–170 (2021).
Grendas, L. N., Chiapella, L., Rodante, D. E. & Daray, F. M. Comparison of traditional model-based statistical methods with machine learning for the prediction of suicide behaviour. J. Psychiatr Res. 145, 85–91 (2022).
Schafer, K. M., Kennedy, G., Gallyer, A. & Resnik, P. A direct comparison of theory-driven and machine learning prediction of suicide: A meta-analysis. PLoS One. 16, e0249833 (2021).
Pigoni, A. et al. Machine learning and the prediction of suicide in psychiatric populations: A systematic review. Transl Psychiatry. 14, 140 (2024).
Ramspek, C. L. et al. Lessons learnt when accounting for competing events in the external validation of time-to-event prognostic models. Int. J. Epidemiol. 51, 615–625 (2022).
Dwyer, D. B., Falkai, P. & Koutsouleris, N. Machine learning approaches for clinical psychology and psychiatry. Annu. Rev. Clin. Psychol. 14, 91–118 (2018).
Jordan, P., Shedden-Mora, M. C. & Löwe, B. Predicting suicidal ideation in primary care: an approach to identify easily assessable key variables. Gen. Hosp. Psychiatry. 51, 106–111 (2018).
Silva, E. J. & Zanchettin, C. On the existence of a threshold in class imbalance problems. In 2015 IEEE international conference on systems, man, and cybernetics (pp. 2714–2719). IEEE. (2015), October.
Virtanen, P. et al. SciPy 1.0: fundamental algorithms for scientific computing in python. Nat. Methods. 17 (3), 261–272 (2020).
Narrow, W. E. et al. DSM–5 field trials in the united States and Canada, part III: development and reliability testing of a cross-cutting symptom assessment for DSM–5. Am. J. Psychiatry. 170, 71–82 (2013).
Çökmüş, F. P., Balıkçı, K. & Aydemir, Ö. Reliability and validity of Turkish form of DSM–5 Self-Rated level 1 Cross-Cutting symptom Scale-Adult version. Anadolu Psikiyatri Derg. 18, 5–13 (2017).
Sarı, Y. E. et al. Turkish reliability of the patient health Questionnaire–9. Biomed. Res. India. 27, S460–S462 (2016).
Hirschfeld, R. M. et al. Development and validation of a screening instrument for bipolar spectrum disorder: the mood disorder questionnaire. Am. J. Psychiatry. 157, 1873–1875 (2000).
Konuk, N. et al. Validation of the Turkish version of the mood disorder questionnaire for screening bipolar disorders. Turk. Psikiyatri Derg. 18, 147–154 (2007).
Morgan, J. F., Reid, F. & Lacey, J. H. The SCOFF questionnaire: assessment of a new screening tool for eating disorders. BMJ 319, 1467–1468 (1999).
Aydemir, Ö., Köksal, B., Sapmaz, S. Y. & Yüceyar, H. Kadın Üniversite öğrencilerinde REZZY Yeme Bozuklukları ölçeği Türkçe formunun Güvenilirlik ve geçerliliği. Anadolu Psikiyatri Derg. 16, 31–37 (2015).
Kessler, R. C. et al. The world health organization adult ADHD Self-Report scale (ASRS): A short screening scale for use in the general population. Psychol. Med. 35, 245–256 (2005).
Doğan, S., Öncü Çetinkaya, B., Saraçoğlu Varol, G. & Küçükgöncü, S. Erişkin Dikkat Eksikliği Hiperaktivite Bozukluğu Kendi bildirim ölçeği (ASRS-v1.1): Türkçe formunun geçerlilik ve güvenilirliği. Anadolu Psikiyatri Derg. 10, 77–87 (2009).
Mayfield, D., McLeod, G. & Hall, P. The CAGE questionnaire: validation of a new alcoholism screening instrument. Am. J. Psychiatry. 131, 1121–1123 (1974).
Arıkan, Z., Özdemir, Y. D., Candansayar, S. & Işık, E. SMAST ve CAGE tarama testlerinin alkolizmin tanısal önemi üzerine bir çalışma. In 27. Ulusal Psikiyatri Kongresi, Antalya (1991).
Spitzer, R. L., Kroenke, K., Williams, J. B. & Löwe, B. A brief measure for assessing generalized anxiety disorder: the GAD–7. Arch. Intern. Med. 166, 1092–1097 (2006).
Konkan, R., Şenormancı, Ö., Güçlü, O., Aydin, E. & Sungur, M. Z. Validity and reliability study for the Turkish adaptation of the generalized anxiety Disorder–7 (GAD–7) scale. Arch. Neuropsychiatry. 50, 53–58 (2013).
Dalenberg, C. & Carlson, E. Brief Dissociative Experiences Scale (DES-B) (2010).
Bernstein, E. M. & Putnam, F. W. Development, reliability, and validity of a dissociation scale. J. Nerv. Ment Dis. 174, 727–735 (1986).
Şar, V. et al. The reliability and validity of the Turkish version of the Dissociative Experiences Scale (DES-II). In Proceedings of the 33rd National Congress of Psychiatry, 55–64 (1997).
Pedregosa, F. et al. Scikit-learn: machine learning in python. J. Mach. Learn. Res. 12, 2825–2830 (2011).
Snoek, J., Larochelle, H. & Adams, R. P. Practical bayesian optimization of machine learning algorithms. Adv. Neural Inf. Process. Syst. 25, (2012).
The MathWorks Inc. MATLAB Version: 9.13.0 (R2022b) (The MathWorks Inc., 2022).
Chollet, F. Keras [Online Resource]. (2015).
Hunter, J. D. Matplotlib: A 2D graphics environment. Comput. Sci. Eng. 9 (03), 90–95 (2007).
Glorot, X. & Bengio, Y. Understanding the difficulty of training deep feedforward neural networks. In Proceedings of the Thirteenth International Conference on Artificial Intelligence and Statistics, 249–256 (2010).
Cybenko, G. Approximation by superpositions of a sigmoidal function. Math. Control Signals Syst. 2, 303–314 (1989).
Kingma, D. P., Ba, J. & Adam A method for stochastic optimization. ArXiv Preprint. arXiv, 14126980 (2014).
Prechelt, L. Early stopping—but when? In Neural Networks: Tricks of the Trade, 55–69 (Springer, (2002).
Scott, M. & Su-In, L. A unified approach to interpreting model predictions. Adv. Neural. Inf. Process. Syst. 30, 4765–4774 (2017).
Sundararajan, M., Taly, A. & Yan, Q. Axiomatic attribution for deep networks. In International Conference on Machine Learning, 3319–3328 (2017).
Šimundić, A. M. Measures of diagnostic accuracy: basic definitions. EJIFCC 19, 203–211 (2009).
Kim, K. W., Lim, J. S., Yang, C. M., Jang, S. H. & Lee, S. Y. Classification of adolescent psychiatric patients at high risk of suicide using the personality assessment inventory by machine learning. Psychiatry Investig. 18, 1137–1144 (2021).
Macalli, M. et al. A machine learning approach for predicting suicidal thoughts and behaviours among college students. Sci. Rep. 11, 11363 (2021).
Wang, J. et al. Prediction of suicidal behaviors in the middle-aged population: machine learning analyses of UK biobank. JMIR Public. Health Surveill. 9, e43419 (2023).
Hussain, S. Challenges and future research directions in automated detection of mental illness using machine learning. Acad. Bull. Mental Health. 2 (2), 56–60 (2024).
Li, W., Dorstyn, D. S. & Jarmon, E. Identifying suicide risk among college students: A systematic review. Death Stud. 44, 450–458 (2020).
Bravo, A. J., Villarosa-Hurlocker, M. C. & Pearson, M. R. College student mental health: an evaluation of the DSM–5 self-rated level 1 cross-cutting symptom measure. Psychol. Assess. 30, 1382–1389 (2018).
Wilburn, V. R. & Smith, D. E. Stress, self-esteem, and suicidal ideation in late adolescents. Adolescence 40, 33–45 (2005).
Lear, M. K. & Pepper, C. M. Self-concept clarity and emotion dysregulation in nonsuicidal self-injury. J. Pers. Disord. 30, 813–827 (2016).
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5 5th edn (American Psychiatric Association, 2013).
Pompili, M., Girardi, P., Ruberto, A. & Tatarelli, R. Suicide in borderline personality disorder: A meta-analysis. Nord J. Psychiatry. 59, 319–324 (2005).
Sareen, J. et al. Anxiety disorders and risk for suicidal ideation and suicide attempts: A population-based longitudinal study of adults. Arch. Gen. Psychiatry. 62, 1249–1257 (2005).
Choi, H. Y. et al. A study on correlation between anxiety symptoms and suicidal ideation. Psychiatry Investig. 8, 320–326 (2011).
de Klerk, S. et al. Prevalence and correlates of lifetime deliberate self-harm and suicidal ideation in naturalistic outpatients: the Leiden routine outcome monitoring study. J. Affect. Disord. 133, 257–264 (2011).
Capron, D. W., Cougle, J. R., Ribeiro, J. D., Joiner, T. E. & Schmidt, N. B. An interactive model of anxiety sensitivity relevant to suicide attempt history and future suicidal ideation. J. Psychiatr Res. 46, 174–180 (2012).
de la Fernández, L. et al. Suicide in obsessive–compulsive disorder: A population-based study of 36,788 Swedish patients. Mol. Psychiatry. 22, 1626–1632 (2017).
Pellegrini, L. et al. Suicide attempts and suicidal ideation in patients with obsessive-compulsive disorder: A systematic review and meta-analysis. J. Affect. Disord. 276, 1001–1021 (2020).
Somé, N. H., Noormohammadpour, P. & Lange, S. The use of machine learning on administrative and survey data to predict suicidal thoughts and behaviors: A systematic review. Front. Psychiatry. 15, 1291362 (2024).
O’Connor, R. C. & Nock, M. K. The psychology of suicidal behaviour. Lancet Psychiatry. 1 (1), 73–85 (2014).
Wagner, G. et al. Prefrontal cortical thickness in depressed patients with high-risk for suicidal behavior. J. Psychiatr Res. 46, 1449–1455 (2012).
Campos, A. I. et al. Brain correlates of suicide attempt in 18,925 participants across 18 international cohorts. Biol. Psychiatry. 90, 243–252 (2021).
Gifuni, A. J. et al. Brain cortical and subcortical morphology in adolescents with depression and a history of suicide attempt. J. Psychiatry Neurosci. 46, E347–E357 (2021).
Sullivan, G. M. et al. Positron emission tomography quantification of serotonin1A receptor binding in suicide attempters with major depressive disorder. JAMA Psychiatry. 72, 169–178 (2015).
Black, C. & Miller, B. J. Meta-analysis of cytokines and chemokines in suicidality: distinguishing suicidal versus nonsuicidal patients. Biol. Psychiatry. 78, 28–37 (2015).
Morales, S. et al. Acute mental discomfort associated with suicide behavior in a clinical sample of patients with affective disorders: ascertaining critical variables using artificial intelligence tools. Front. Psychiatry. 8, 7 (2017).
Jung, J. S. et al. Prediction models for high risk of suicide in Korean adolescents using machine learning techniques. PLoS One, 14(6), e0217639. (2019).
Ge, F., Jiang, J., Wang, Y., Yuan, C. & Zhang, W. Identifying suicidal ideation among Chinese patients with major depressive disorder: evidence from a real-world hospital-based study in China. Neuropsychiatr. Dis. Treat., 665–672. (2020).
Kim, S., Lee, H. K. & Lee, K. Detecting suicidal risk using MMPI–2 based on machine learning algorithm. Sci. Rep. 11 (1), 15310 (2021).
Song, S. I., Hong, H. T., Lee, C. & Lee, S. B. A machine learning approach for predicting suicidal ideation in post stroke patients. Sci. Rep. 12 (1), 15906 (2022).
Huang, Y. et al. Comparison of three machine learning models to predict suicidal ideation and depression among Chinese adolescents: A cross-sectional study. J. Affect. Disord. 319, 221–228 (2022).
Meda, N., Pardini, S., Rigobello, P., Visioli, F. & Novara, C. Frequency and machine learning predictors of severe depressive symptoms and suicidal ideation among university students. Epidemiol. Psychiatric Sci., 32, e42. (2023).
Sara, S. S., Rahman, M. A., Rahman, R. & Talukder, A. Prediction of suicidal ideation with associated risk factors among university students in the Southern part of Bangladesh: machine learning approach. J. Affect. Disord. 349, 502–508 (2024).
Kim, S. B. & Rattakorn, P. Unsupervised feature selection using weighted principal components. Expert Syst. Appl. 38 (5), 5704–5710 (2011).
Acknowledgements
We would like to thank all the clinical psychologists who worked at the KUPTEM service throughout the data collection periods.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
M.B. and H.Y.E.conducted the analysis and wrote the main manuscript body . All authors contributed to the design, conceptualization, and writing of the manuscript. All authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ballı, M., Dogan, A.E., Senol, S.H. et al. Machine learning based identification of suicidal ideation using non-suicidal predictors in a university mental health clinic. Sci Rep 15, 13843 (2025). https://doi.org/10.1038/s41598-025-97387-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-97387-4
