
Abstract
Despite the critical need for data to support public health policies in Brazil, there is a glaring lack of national epidemiological studies on neurogenic lower urinary tract dysfunction (NLUTD). This study aimed to illuminate the factors associated with the urological management of NLUTD among individuals with traumatic spinal cord injury (TSCI) and non-traumatic spinal cord injury (NTSCI). Employing a quantitative, cross-sectional, and descriptive design, this study analyzed electronic medical records of NLUTD and SCI patients monitored within the SARAH network from 2007 to 2017. Sociodemographic and clinical data were collected, including the ASIA Impairment Scale, and statistical analyses such as the Mann–Whitney and Pearson’s Chi-square tests were conducted. The findings revealed that out of 903 patients, 67% had TSCI and 33% had NTSCI. Clean intermittent catheterization (CIC) was the primary bladder emptying method, utilized by 66.11% of the participants. The average emptying frequency was 4.71 times a day, and urinary incontinence was reported in 58.4% of cases. A significantly higher rate of positive urinary colonization was found among TSCI patients. The study highlighted significant differences in NLUTD management between TSCI and NTSCI patients, with NTSCI patients more frequently achieving voluntary urination and using maneuvers to stimulate urination. These distinctions underscore the need for more individualized approaches and deeper understanding of each type of spinal cord injury, aiming to enhance bladder rehabilitation programs in Brazil.
Similar content being viewed by others

Introduction
The term neurogenic lower urinary tract dysfunction (NLUTD), also referred to as neurogenic bladder, refers to any dysfunction of the lower urinary tract arising from an injury or disease in the central or peripheral nervous system. Since NLUTD is not limited to the bladder, it is also the correct term to describe the various urinary tract issues in patients with neurological disorders1. Moreover, NLUTD is often associated with traumatic spinal cord injury (TSCI) and non-traumatic spinal cord injury (NTSCI). The treatment of NLUTD mainly involves protecting the upper urinary tract, ensuring full emptying of the bladder and urinary continence, and, thus, promoting a better quality of life2,3,4.
In the past, kidney failure was considered one of the leading causes of death among people with spinal cord injury (SCI). Due to improvements in urological management5, pneumonia, pulmonary embolism, and septicemia are currently among the main causes of death in those patients6. However, diseases of the genitourinary system are the main cause of readmissions after SCI and the fifth most common cause of death. People with SCI usually have difficulty in accurately reporting symptoms related to urinary tract infection2. According to estimates, the prevalence of kidney disease in people with NLUTD is three times higher than in the general population, despite advancements in urological rehabilitation care, which includes adequate bladder emptying and use of anticholinergic drugs, among other procedures and surgical management7,8.
Clean intermittent catheterization (CIC), or intermittent self-catheterization, was instituted by Lapides et al.9 and is still considered the main bladder emptying method for the treatment of lower urinary tract dysfunctions and the prevention of renal deterioration resulting from complications of NLUTD10,11. The technique of intermittent self-catheterization is the most similar to normal bladder function and does not entail risks for renal function or the life expectancy of these patients9,11. In association with CIC, anticholinergic drugs, alpha-blockers, and tricyclic antidepressants can be used to help control intravesical pressure and facilitate bladder emptying4,5.
Bladder care is one of the fundamental steps involved in the rehabilitation of the person with SCI7. CIC is one of the most complex self-care activities for patient empowerment and adherence to treatment12. Many factors can interfere with this care, such as gender, lifestyle, manual dexterity, access to the health team, and the neurological level of people with SCI. An efficient bladder re-education program can reduce the risk of urinary incontinence and, consequently, improve quality of life4,12,13,14.
Despite the importance of knowing the number of people with NLUTD in Brazil to support public health policies, national epidemiological studies and statistical data are practically non-existent3,15,16,17. In Brazil, this population faces challenges such as access to adequate rehabilitation programs and high costs of materials needed for the CIC. Within this context, an important network of rehabilitation hospitals with units in 8 Brazilian states was considered a rich field to carry out studies on NLUTD. The SARAH network is among the most important centers of reference in rehabilitation in Brazil and Latin America. The main research question was to determine the prevalence of individuals with spinal cord injury and NLUTD and to understand the difference in bladder management between individuals with TSCI and NTSCI. In this regard, this study aimed to shed light on the factors related to the urological management of NLUTD in these individuals.
Methods
This is a quantitative, cross-sectional, and descriptive study that aimed to identify the profile of users with NLUTD and SCI monitored in the SARAH network by analyzing their electronic medical records from 2007 to 2017. This study was approved by the Ethics and Research Committee (CEP) of the SARAH network of rehabilitation hospitals. The need for informed consent was waived by the research Ethics Committee of institution. The study was conducted at the SARAH network of rehabilitation hospitals, which provides rehabilitation for individuals with neurological disorders. This network has units in the various regions of Brazil, such as Brasília-DF, São Luís-MA, Salvador-BA, Belo Horizonte-MG, Fortaleza-CE, and Rio de Janeiro-RJ. The units in the cities of Belém-PA and Macapá-AP were excluded from this study as they exclusively provide care to children, which are not part of our scope. To standardize and organize the information obtained in this study, data were collected using a form created to characterize the sample. This study was exempt from the application of a free and informed consent form, approved by the Research Ethics Committee of Rede Sarah, number CAAE: 46255515.9.0000.0022 as it was a collection of medical records review, respecting confidentiality and confidentiality of selected sample participants. All methods were performed in accordance with the relevant guidelines and regulation.
The variables were related to sociodemographic data, namely age, gender, origin, network, and admission date, and clinical data, such as main diagnosis, etiology, diagnosis of neurogenic bladder and form of bladder emptying. In cases of TSCI, the ASIA Impairment Scale (AIS) was considered, as it is part of the international neurological classification protocol of the American Spinal Injury Association. The diagnosis of SCI and sociodemographic data were extracted from a specific icon in the electronic medical records. Data of the sample were collected in a more detailed way by directly accessing medical evolution or evolution recorded by nurses, thus conferring greater reliability to this prevalence.
For the statistical tests, the Mann–Whitney test was used for two independent samples and Pearson’s Chi-square test for the categorical variables. The significance level was 0.053.
Results
The sample consisted of 903 patients enrolled in the network with a diagnosis of NLUTD. Among the participants, 67.00% (605) had traumatic spinal cord injury (TSCI), and 33.00% (298) had non-traumatic spinal cord injury (NTSCI). Moreover, 69.32 (626) were men and 30.68% (277) were women. Males were prevalent among those with TSCI, and females were prevalent for NTSCI (p ≤ 0.001, Pearson’s Chi-squared test).
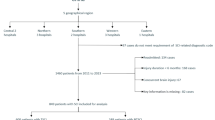
CIC was found to be the main method of bladder emptying, performed by 66.11% of the study participants (n = 597). Of these participants, 434 had TSCI and 163 had NTSCI. Sample distribution of Brazilian participants (n = 903) with NLUTD and use/non-use of clean intermittent catheterization in the SARAH rehabilitation network as shown in Fig. 1.

Distribution of participants with NLUTD according to clean intermittent catheterization (n = 903), Brazil, 2019. Source: Elaborated by the authors.
Intermittent self-catheterization was the most widely used form of catheterization among the participants (74.04%), both by people with TSCI and NTSCI, as shown in Fig. 2.

Distribution of participants with NLUTD according to traumatic and non-traumatic cause of injury and use of clean intermittent catheterization (n = 597), Brazil, 2019. Source: Elaborated by the authors.
Most of the participants who performed CIC, 94.63% (565), maintained an average emptying frequency of 4.71 times a day (SD = 0.69). Five times a day was the most common frequency of 50.92% (304) of the participants, followed by four times a day for 30.49% (182), six times a day for 10.05% (60), and three times a day for 3.18% (19). A small number of participants did not perform CIC regularly, that is, 5.36% (32), and it was not possible to establish a daily frequency. Moreover, 88 participants had interrupted CIC and no longer performed the procedure. Of these participants, 64 had TSCI and 24 had NTSCI.
Regarding the presence of urinary loss, 58.4% of the participants had incontinence. The presence of urinary loss was more expressive among those for which CIC was performed by third parties than those who performed self-catheterization (p ≤ 0.002, Pearson’s Chi-squared test). No difference was observed in relation to the presence of urinary loss and type of SCI (p ≤ 0.802, Pearson’s Chi-squared test).
Still in relation to other forms of bladder emptying, 31 participants used a long-term catheter and 18 had a cystostomy. Six participants were found with continent diversions and two with incontinent diversions. Of those with continent diversion, two had a diagnosis of myelomeningocele and four were quadriplegic due to SCI. Of the participants with incontinent diversion, both had SCI from birth, one due to myelomeningocele and the other due to hypoxic myelopathy.
Among the participants who performed CIC, 83.13% had positive colonization in the urine (p ≤ 0.001, Pearson’s Chi-squared test). Most of the participants with positive colonization in the urine (70.53%) had TSCI (p ≤ 0.005, Pearson’s Chi-squared test).
Only 32.12% (290) of the sample participants had voluntary urination. These cases are shown in Fig. 3, most of which had a diagnosis of NTSCI (p ≤ 0.001, Pearson’s Chi-squared test).

Distribution of participants with NLUTD according to the cause of SCI and presence of voluntary urination (n = 903), Brazil, 2019. Source: Elaborated by the authors.
Among the participants who performed voluntary urination, the majority, 66.20% (191), used some kind of manouevre for bladder emptying. Participants with NTSCI performed more bladder emptying manouevres (30.20%) than those with TSCI (15.86%) (p ≤ 0.001, Pearson’s Chi-squared test).
The Valsalva manouevre was used by 73.44% (141) of the participants, being the most popular, followed by the Credé manouevre, used by 10.42% (20) of the participants, programmed urination, used by 5.21% (10), and Tapping, used by only one participant. Moreover, 19 participants (9.89%) performed more than one manouevre to trigger urination. Data in Fig. 4.

Distribution of participants with voluntary urination according to bladder emptying method (n = 191), Brazil, 2019. Source: Elaborated by the authors.
Regarding drug treatment for NLTUD, 64.67% (584) of the participants used medication and 319 (35.33%) did not use any medication. Of these participants, most had TSCI (p ≤ 0.001, Pearson’s Chi-squared test), as shown in Table 1.
The most commonly used medications for ensuring correct bladder function were those of the antimuscarinic class (91.26%), especially oxybutynin, both by participants with TSCI (93.04%) and NTSCI (86.82%), followed by alpha-adrenergic blockers, antibiotics, and B3 agonist. No statistical difference was observed between the different classes of drugs used by the participants and the cause of SCI.
Discussion
The high prevalence of SCI (67%) and male participants (69.32%) corroborate findings from previous studies, in which men are more likely to be injured in high-risk situations, such as car accidents, physical aggression, or even at work16,17,18,19,20.
Intermittent catheterization was the main form of bladder emptying found in the study (66.11%), with self-catheterization being the most prevalent form among the participants. No difference was observed between the causes of SCI. This result is consistent with those of other studies and reflects observance of international urological management protocols for people with SCI and the standard practice of urological conduct in the different rehabilitation units of the SARAH network2,3,21. More recent studies confirm that CIC is the most commonly used bladder emptying method by people with SCI, with a frequency between 42 and 77%22. Despite the challenges, CIC is still considered an effective and safe short- and long-term treatment5,23.
Among the study participants who regularly performed CIC, most maintained an emptying frequency of four to six times a day (91.45%). The recommended catheter size is between 12 and 16 Fr. The emptying frequency indicated, considering bladder physiology, usually varies from four to six times a day according to bladder capacity and water consumption in 24 h. Ideally, the volume of the bladder in catheterization should not, as a rule, exceed 400–500 mL. In this regard, emptying frequency with adequate technique and materials are critical factors for successful follow-up5,24.
Around 8.54% of the participants performed CIC three times a day or less than the frequency recommended by the literature. The low frequency can result in greater urinary residue and, consequently, a higher frequency of urinary tract infections. However, an increased frequency may increase the risk of urethral complications24. Urodynamic testing can objectively evaluate NLUTD and indicate the best frequency of bladder emptying based on the measured bladder compliance and detrusor hyperactivity1,2,4. Prospective studies will be needed to better understand the reasons of participants performed CIC less frequently than recommended as well to confirm clinical significance associated with this.
In this study, 88 participants stopped performing CIC for unknown reasons. Of those participants, most had TSCI. CIC performance rates often decrease during long-term follow-up10. Population studies revealed that 50% of people with SCI stop performing CIC within 5 years of follow-up25. Another study showed that the main causes reported by the participants for interrupting the technique were inconvenience, urinary loss, and UTI26. This interruption may also be associated with difficulties in maintaining a caregiver who performs the procedure or due to lack of materials for CIC, mainly related to financial restriction, which further confirms the importance of studies that support public policies12. In Brazil, this population faces challenges such as access to adequate rehabilitation programs and high costs of materials needed for the CIC12. For this retrospective study, it was not possible to collect socioeconomic data, as these are not available in the electronic medical record. To understand the reasons for interrupted CIC, more prospective studies with deeper analysis are still needed.
NLTUD is known to present a greater number of complications and a higher risk to the upper urinary tract in individuals with SCI, especially when it is related to the presence of high pressure, low compliance, and reduced bladder capacity27. Treatment is primarily aimed at converting an overactive, high-pressure bladder into a low-pressure reservoir. The reduction of detrusor pressure helps prevent UTIs and promotes urinary continence leading to improved social rehabilitation and quality of life2. Thus, these patients may need more care, such as CIC associated with medications, to ensure effective bladder emptying, incontinence control, and protection for the upper urinary tract. However, complete continence cannot always be obtained. In this study, a significant number of participants had urinary leakage (58.47%) even with the CIC. Urinary incontinence can also be related to inadequate technique or failures during CIC, such as delayed or irregular catheterization frequency and dependence on third parties for effective bladder emptying. This shows the complexity involved in treating NLUTD and the acquisition of urinary continence even with the best measures for adequate bladder emptying and protection of the upper urinary tract. In this regard, when proposing the performance of CIC, health workers should consider the patient’s expectation of acquiring continence and address the points brought by each patient to minimize interruptions of the procedure in the future due to the frustration of not acquiring continence4,10.
Of the participants who performed voluntary urination (290), most had a diagnosis of NTSCI and performed some type of manouevre to try to stimulate urination. The Valsalva manouevre was the most widely performed (73.44%), followed by Credé (10.42%). Manouevres to stimulate urination only provide quality of life and reduce treatment costs when safely indicated after confirmatory examinations and if the urinary tract situation remains stable over the years23. Studies show that these bladder compression techniques can generate increased intra-abdominal pressure, which may result in potentially dangerous increased hyperactivity and detrusor pressure. Thus, these techniques should be discouraged unless urodynamic testing show that intravesical pressure remains within safe limits2,4.
A small number of participants used a long-term bladder catheter (3.43%) and suprapubic cystostomy (1.66%). Both techniques are not indicated as regular treatment for NLUTD or for safe long-term treatment given the risk of recurrent urinary tract infections and a greater number of significant complications in the long term5. Silicone catheters are preferred because they are less susceptible to encrustation and due to the high incidence of latex allergy in the neurological patient population27.
Most participants with SCI who performed CIC had positive bacterial colonization in the urine. The literature indicates that individuals with SCI have a high prevalence of bacteriuria and a high incidence of urinary tract infection. In people who perform CIC, asymptomatic bacteriuria can range from 23 to 69%28. Antibiotic treatment is usually not recommended, except in cases of pregnancy or before specific urological procedures5,28,29.
Most of the participants underwent CIC and used medications for the urinary tract. Even today, anticholinergic drugs are the first line of choice for the treatment of detrusor hyperactivity, as they reduce intravesical pressure and improve bladder compliance and urinary incontinence5. However, these drugs have a high incidence of causing adverse events, such as xerostomia, which can lead to early discontinuation of therapy. Different routes of administration are suggested, such as intravesical, which can minimize side effects4,5,13,27,30.
Neurogenic lower urinary tract dysfunction and intestinal dysfunction and its related problems are often important factors in daily life after a spinal cord injury, which can affect reintegration into society. Both managements require several interventions, demands substantial time, and considerably impacts the quality of life of people with SCI7,22,31.
Study limitations
Cross-sectional studies and data obtained from secondary sources can lead to limitations during data collection. In this study, a limitation was the absence of information in the electronic medical records. Another limitation is the nature of the study, which, despite providing relevant information about the selected population, results in retrospective data. Moreover, pre-established conditions prevent any action.
To better characterize data on the occurrence of urinary tract infection, data should include clinical aspects of the patient. However, the medical records consulted in this study did not provide data with the necessary reliability for the research. Therefore, this information was not used. The incomplete data cited in the study limitations did not affect the reliability of this research. Future studies will be necessary to better understand the impact of urinary tract infections in this population.
Other point is that no consistent information was found on the type of urethral catheter used, caliber, and reuse. The absence of information on these factors may have occurred because, during the selected period, this data was not yet widely systematized.
Conclusion
This study showed the differences in the urological management of NLUTD between participants with TSCI and NTSCI. The main form of bladder emptying found was CIC, performed by most participants, especially by people with TSCI. Associated with CIC, the participants also used drug treatment, mostly anticholinergics. The cause of SCI showed no difference in the ability to perform CIC.
Participants with NTSCI tend to be able to perform bladder emptying with voluntary urination more frequently and use manouevres to stimulate urination.
Urinary losses occurred in a large part of the sample, but a significant difference was observed according to the type of CIC, being more prevalent in those who performed catheterization assisted by third parties. The participants who performed self-catheterization had a lower incidence of losses, probably associated with greater autonomy and control of schedules, which reflects on the success of achieving urinary continence. This is an important fact to be considered in bladder rehabilitation programs since it provides greater insight into patient expectations and clarifies the main objective of neurogenic bladder, namely, to protect the upper urinary tract and, secondly, continence, which is not always achieved.
Bladder disorders can negatively affect the quality of life and social participation of people with SCI. The differences found in the study confirm the need for a more individualized approach and a more thorough view of each type of SCI, in a long-term follow up care. Prospective longitudinal studies should be conducted using validated instruments to understand the variables raised in this study and to develop practical measures for bladder rehabilitation in the different rehabilitation programs in Brazil.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Ginsberg, D. A. et al. The AUA/SUFU guideline on adult neurogenic lower urinary tract dysfunction: Diagnosis and evaluation. J. Urol. 206(5), 1097–1105 (2021).
EAU Guidelines. Edn. presented at the EAU Annual Congress Milan 2023. EAU Guidelines Office, Arnhem, the Netherlands (2023).
Pelosi, G., Faleiros, F., Pereira, M. R. C., Bimbatti, K. F. & Tholl, A. D. Study on the prevalence of neurogenic bladder in Brazilians with traumatic and non-traumatic spinal cord injury. J. Spinal Cord Med. 46(4), 677–681 (2023).
Panicker, J. N. Neurogenic bladder: Epidemiology, diagnosis, and management. Semin. Neurol. 40(5), 569–657 (2020).
Ginsberg, D. A. et al. The AUA/SUFU guideline on adult neurogenic lower urinary tract dysfunction: Treatment and follow-up. J. Urol. 206(5), 1106–1113 (2021).
Hamid, R. et al. Epidemiology and pathophysiology of neurogenic bladder after spinal cord injury. World J. Urol. 36(10), 1517–1527 (2018).
Tate, D. G. et al. Recommendations for evaluation of neurogenic bladder and bowel dysfunction after spinal cord injury and/or disease. J. Spinal Cord Med. 43, 141–164 (2020).
Sung, B. M., Oh, D. J., Choi, M. H. & Choi, H. M. Chronic kidney disease in neurogenic bladder. Nephrology (Carlton) 23(3), 231–236 (2018).
Lapides, J., Diokno, A. C., Silber, S. J. & Lowe, B. S. Clean, intermittent self-catheterization in the treatment of urinary tract disease. J. Urol. 107, 458–461 (1972).
Seth, J. H., Haslam, C. & Panicker, J. N. Ensuring patient adherence to clean intermittent self-catheterization. Patient Prefer Adherence. 8, 191–198 (2014).
Klausner, A. P. The Lapides legacy: 42 years and cathing. Can. J. Urol. 21(2), 7194 (2014).
Faleiros, F., Toledo, C., Gomide, M. F. S., Faleiros, R. G. & Käppler, C. Right to health care and materials required for intermittent catheterization: A comparison between Germany and Brazil. Qual. Prim. Care 23(3), 127–133 (2015).
Taweel, W. A. & Seyam, R. Neurogenic bladder in spinal cord injury patients. Res. Rep. Urol. 7, 85–99 (2015).
Tang, D. H. et al. Impact of urinary incontinence on health-related quality of life, daily activities, and healthcare resource utilization in patients with neurogenic detrusor overactivity. BMC Neurol. 14, 74 (2014).
Faleiros, F. et al. Epidemiological profile of spinal cord injury in Brazil. J. Spinal Cord Med. 46(1), 75–82 (2023).
Cipriano, M. A. B. et al. Revisão integrativa de estudos sobre ações educativas para portadores de bexiga neurogênica. Rev. Enferm. UERJ. 20(6), 819–824 (2013).
Faleiros, F. et al. Surveying people with spinal cord injuries in Brazil to ascertain research priorities. Sci. Rep. 13(1), 654 (2023).
National Spinal Cord Injury Statistical Center. Spinal cord injury facts and figures at a glance. J. Spinal Cord Med. (2020).
Kumar, R. Lim, J. Mekary, R.A. Rattani, A. Dewan, M.C. Sharif, S.Y. Osorio-Fonseca, E. Park, KB. Traumatic spinal injury: Global epidemiology and worldwide volume. World Neurosurg. (2018) https://doi.org/10.1016/j.wneu.2018.02.033.
Singh, A., Tetreault, L., Kalsi-Ryan, S., Nouri, A. & Fehlings, M. G. Global prevalence and incidence of traumatic spinal cord injury. Clin. Epidemiol. 6, 309–331 (2014).
Videira, L.G.N. Reabilitação da bexiga neurogênica: métodos de manejo, complicações urológicas, estilo de vida e satisfação pessoal em pessoas com lesão medular [Master’s thesis]. Ribeirão Preto: Escola de Enfermagem de Ribeirão Preto. (2022).
Adriaansen, J. J. V. et al. Bladder-emptying methods, neurogenic lower urinary tract dysfunction and impact on quality of life in people with long-term spinal cord injury. J. Spinal Cord Med. 40(1), 43–53 (2017).
Wyndaele, J. J. et al. Neurologic urinary incontinence. Neurourol. Urodyn. 29(1), 159–164 (2010).
Romo, P. G. B. et al. Non-surgical urologic management of neurogenic bladder after spinal cord injury. World J. Urol. 36(10), 1555–1568 (2018).
Crescenze, I. M. et al. Neurogenic Bladder Research Group. Predictors of low urinary quality of life in spinal cord injury patients on clean intermittent catheterization. Neurourol. Urodyn. 38(5), 1332–1338 (2019).
Patel, D. P. et al. Reasons for cessation of clean intermittent catheterization after spinal cord injury: Results from the Neurogenic Bladder Research Group spinal cord injury registry. Neurourol. Urodyn. 39(1), 211–219 (2020).
Linsenmeyer, T. A. Catheter-associated urinary tract infections in persons with neurogenic bladders. J. Spinal Cord Med. 41(2), 132–141 (2018).
Nicolle, L.E et al. Clinical practice guideline for the management of asymptomatic bacteriuria: 2019 update by the infectious diseases society of America. Clin. Infect. Dis. (2019). https://doi.org/10.1093/cid/ciy1121.
Skelton, F., Grigoryan, L., Holmes, S. A., Poon, I. O. & Trautner, B. Routine urine testing at the spinal cord injury annual evaluation leads to unnecessary antibiotic use: A pilot study and future directions. Arch Phys. Med. Rehabil. 99(2), 219–225 (2018).
Stothers, L., Tsang, B., Nigro, M., Lazare, D. M. & A,. An integrative review of standardized clinical evaluation tool utilization in anticholinergic drug trials for neurogenic lower urinary tract dysfunction. Spinal Cord. 54(12), 1114–1120 (2016).
Khadour, F. A. et al. Effect of neurogenic bowel dysfunction symptoms on quality of life after a spinal cord injury. J. Orthop. Surg. Res. 18(1), 458. https://doi.org/10.1186/s13018-023-03946-8 (2023).
Author information
Authors and Affiliations
Contributions
Conceptualization, GP, FF and DRS; Methodology, GP, FF, EF and FL; Validation, GP, FL and FF; Formal Analysis, GP, DGT, and FL; Investigation, GP and FL; Resources, LNC, FF, EF, DRS and GP; Data Curation, FF and DGT; Writing—Original Draft preparation, LNC, GP, FL and EF editing – Review and editing, LNC and GP; visualization, FF; supervision, FF and DGT; Project administration, FF; Acquisition of financing, FF and DGT. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study was considered and approved by the Brazilian Ethics Committee CAAE: CAAE: 46255515.9.0000.0022 The authors declare that [the/all other] data supporting the findings of this study are available within the article.
Declaration of Free and Informed Consent from research participants
The authors declare that the need for informed consent was waived by the Research Ethics Committee of Rede SARAH. This study was approved by the same Committee of institution, number CAAE: 46255515.9.0000.0022 as it was a collection of medical records review, respecting confidentiality and confidentiality of selected sample participants. All methods were performed in accordance with the relevant guidelines and regulation.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Pelosi, G., Corbo, L.N., Lopes, F. et al. Urological management in people with traumatic and non-traumatic spinal cord injury in Brazil. Sci Rep 15, 26215 (2025). https://doi.org/10.1038/s41598-025-97417-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-97417-1
