
Abstract
Despite the well-established association between the apolipoprotein B/apolipoprotein A1 (apoB/apoA1) ratio and ischemic stroke, its specific relationship with the underlying vascular pathologies contributing to stroke remains poorly understood. This study aims to investigate the association between the apoB/apoA1 ratio and intracranial or extracranial atherosclerosis. We enrolled 408 patients with acute ischemic stroke who had never been treated with statins or fibrates. Based on the images from computed tomography angiography (CTA), the patients were categorized into four groups: intracranial atherosclerosis stenosis (ICAS, n = 136), extracranial carotid atherosclerosis stenosis (ECAS, n = 45), combined intracranial and extracranial atherosclerosis stenosis (COAS, n = 73), and non-cerebral atherosclerosis stenosis (NCAS, n = 154). Demographic characteristics, clinical factors, and serum lipid levels were collected and then compared across groups. The apoB/apoA1 ratio was significantly higher in patients with ICAS, ECAS and COAS compared to those in the NCAS group. Multivariable logistic regression analysis demonstrated that the ApoB/ApoA1 ratio was independently associated with ICAS, but not with ECAS. ROC curve analysis showed that the ApoB/ApoA1 ratio had a good diagnostic ability for ICAS, with an area under the curve (AUC) of 0.764, an optimal cut-off value of 0.8122, a sensitivity of 81.3%, and a specificity of 59.8%. An higher apoB/apoA1 ratio is associated with ICAS in ischemic stroke patients.
Similar content being viewed by others


Introduction
Despite improvements in life expectancy, stroke has become the second leading cause of death and disability worldwide1. It is widely recognized that stenosis of extracranial and intracranial arteries represents a significant risk factor for ischemic stroke, with its progression closely linked to an increased likelihood of future ischemic events2,3. Identifying the risk factors associated with cerebral atherosclerosis stenosis is therefore critical for the prevention of both initial and recurrent strokes.
The apoB/apoA1 ratio has been widely recognized as a crucial indicator of lipid metabolism imbalance and a strong predictor of cardiovascular and cerebrovascular disease severity4. This ratio reflects the balance between atherogenic and anti-atherogenic lipoproteins, with higher values indicating an increased risk of vascular pathology5. Its predictive value extends beyond traditional lipid markers, offering important insights into disease progression and prognosis6.
In the context of cardiovascular diseases, extensive research has demonstrated the significance of the apoB/apoA1 ratio in assessing coronary artery disease (CAD) risk and predicting long-term cardiovascular outcomes. Specifically, Zhang et al. found that the apoB/apoA1 ratio outperformed conventional lipid markers in predicting major adverse cardiovascular events7, while Rasouli suggested that combining the apoB/apoA1 ratio with inflammatory markers significantly enhanced its predictive accuracy for coronary artery disease8, both highlighting its potential role in risk stratification. Additionally, Huang et al. explored the genetic determinants of this ratio and their associations with CAD, further reinforcing its mechanistic link to cardiovascular pathology9.
Beyond cardiovascular disease, the apoB/apoA1 ratio has also been implicated in ischemic stroke. For example, Park et al. demonstrated that higher apoB/apoA1 ratios were associated with an increased risk of ischemic stroke in the Korean population10, Lee et al. revealed that an elevated apoB/apoA1 ratio was predictive of post-stroke cognitive impairment11, and Huang et al. reported significant correlations between this ratio and white matter lesion severity as well as cerebral microvascular dysfunction12. Together, these findings highlight the robust association between the apoB/apoA1 ratio and ischemic stroke, encompassing multiple aspects from disease susceptibility and prognosis to underlying pathophysiological mechanisms, thereby reinforcing its significance in cerebrovascular research.
However, despite the well-established association between the apoB/apoA1 ratio and ischemic stroke, its specific relationship with the underlying vascular pathologies contributing to stroke remains poorly understood. Previous studies have primarily focused on stroke risk prediction or post-stroke outcomes10,11,12, without systematically examining how this ratio relates to the different vascular abnormalities that underlie ischemic stroke. In order to address these gaps, this study aims to investigate the relationship between the apoB/apoA1 ratio and intracranial and extracranial atherosclerotic stenosis, as well as to determine whether this ratio serves as an independent risk factor for these conditions. By doing so, this study seeks to provide a deeper understanding of how the apoB/apoA1 ratio is linked to specific vascular mechanisms in ischemic stroke, which may further enhance its role as a biomarker in cerebrovascular disease assessment.
Methods
Participants
Participants were consecutively recruited from January 2020 to June 2021 from patients with cerebral infarction who underwent computed tomography angiography (CTA) examinations at the Neurology Department of The Second Affiliated Hospital of Fujian Medical University.
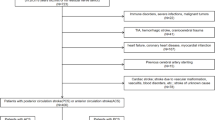
The inclusion criteria for subject selection were as follows: (1) patients diagnosed with acute cerebral infarction, (2) evaluated using computed tomography angiography (CTA), (3) admitted to the hospital within seven days of stroke onset, and (4) aged > 18 years. The following exclusion criteria were applied: (1) incomplete laboratory tests (missing essential blood lipid measurements) or vascular imaging (the absence of intracranial and extracranial vascular assessments); (2) prior use of statins or fibrates, as these lipid-lowering agents may influence apoB and apoA1 levels; (3) stroke due to other determined etiologies, such as atrial fibrillation, cardiac embolism, arteritis, moyamoya disease, or muscular fiber dysplasia; (4) a history of chronic liver disease, tumors, infections, or renal failure.
This study was approved by the Ethics Committee of The Second Affiliated Hospital of Fujian Medical University, Quanzhou, Fujian Province, China. Written informed consent was obtained from all participants prior to enrollment. For patients who were unable to provide consent due to severe stroke, coma, or impaired consciousness, informed consent was obtained from their legally authorized representatives. All procedures involving human participants were conducted in accordance with the Declaration of Helsinki.
Serum lipid analysis
Fasting blood samples were collected in the morning within 24 h of admission. Blood samples were drawn into standard serum-separating tubes without anticoagulants and allowed to clot at room temperature for 30 min. The samples were then centrifuged at 3,000 × g for 10 min to separate the serum.
The serum levels of triglycerides (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), apolipoprotein B (apoB), apolipoprotein A1 (apoA1), and hemoglobin A1C (HbA1C) were measured using a Beckman AU680 Chemistry System and a Beckman LH 780 Hematology Analyzer, following the manufacturer’s instructions (Beckman Coulter, Brea, CA, USA).
Vascular imaging and participant grouping
Vascular imaging was performed for all enrolled participants to evaluate intracranial and extracranial arterial stenosis using a Siemens AG 64-slice dual-source CT scanner. The intracranial arteries assessed included the middle cerebral artery (MCA), anterior cerebral artery (ACA), posterior cerebral artery (PCA), basilar artery (BA), the intracranial segment of the internal carotid artery (I-ICA; C4-C7), and the intracranial portion of the vertebral artery (I-VA; V4). The extracranial arteries included the external carotid artery (ECA), common carotid artery (CCA), the extracranial segments of the vertebral artery (V1-V3), and the extracranial portion of the internal carotid artery (E-ICA; C1). The vascular images were independently assessed by two experienced reviewers who were blinded to the clinical data to ensure objectivity. Based on the imaging results, participants were categorized into four groups: (1) intracranial atherosclerosis stenosis (ICAS) group, (2) extracranial carotid atherosclerosis stenosis (ECAS) group, (3) combined intracranial and extracranial atherosclerosis stenosis (COAS) group, and (4) non-cerebral atherosclerosis stenosis (NCAS) group.
In summary, based on the TOAST classification system, we primarily included patients with large-artery atherosclerosis (LAA) stroke. Patients with cardioembolic stroke (e.g., atrial fibrillation, cardiac embolism) and strokes due to other determined etiologies (e.g., arteritis, moyamoya disease, muscular fiber dysplasia) were excluded. All participants underwent CTA to assess intracranial and extracranial arterial stenosis, ensuring the inclusion of patients with an atherosclerotic origin of stroke. However, some patients did not exhibit significant intracranial or extracranial arterial stenosis on CTA and were classified into the NCAS group. These patients were diagnosed with small-artery occlusion lacunar stroke (SAO) based on clinical and imaging findings. While they did not meet the criteria for LAA, they were included as a reference group, i.e., NCAS, for comparison with the ICAS, ECAS, and COAS groups.
Statistical analysis
SPSS Statistics software version 20.0 (IBM Corp., Armonk, NY, USA) was used for all statistical analyses. Continuous variables were expressed as mean ± standard deviation (SD), and categorical variables were presented as n (%). The normality of continuous variables was assessed using the Kolmogorov-Smirnov test, which indicated that all continuous data approximately followed a normal distribution, except for glycosylated hemoglobin. For normally distributed data, one-way analysis of variance (ANOVA) was used for group comparisons, followed by post hoc least significant difference (LSD) t-tests for pairwise comparisons. For non-normally distributed data, the Kruskal-Wallis test was applied to assess differences among groups, with post hoc Mann-Whitney U tests, and Bonferroni correction was used to adjust for multiple comparisons. Categorical variables were analyzed using the chi-square test.
To determine independent predictors of ICAS and ECAS, we conducted a multivariate logistic regression analysis. Variables such as age, hypertension, gender, apoB/apoA1 ratio, apoA1, apoB, glycosylated hemoglobin, TC, TG, HDL, and LDL were included in the model. The results were presented as odds ratios (OR) with corresponding 95% confidence intervals (CI), to estimate the independent effect of each variable on the likelihood of ICAS or ECAS.
Receiver operating characteristic (ROC) curve analysis was performed to assess the diagnostic accuracy of the apoB/apoA1 ratio for detecting ICAS. The discriminatory ability of the apoB/apoA1 ratio was quantified using the area under the curve (AUC), with higher values indicating better diagnostic performance. Sensitivity, specificity, and the optimal cut-off point were determined based on Youden’s index to maximize diagnostic performance.
In this study, statistical significance was set at P < 0.05.
Results
Baseline characteristics
A detailed overview of patient selection is presented in the flowchart (Fig. 1). As summarized in Table 1, a total of 408 patients with acute stroke (263 men and 145 women; mean age: 65.52 ± 12.15 years) were included in the final analysis. The patients were categorized into four subgroups: 154 (37.75%) in the NCAS group, 136 (33.33%) in the ICAS group, 45 (11.03%) in the ECAS group, and 73 (17.89%) in the COAS group. Among patients with ICAS, 27 (19.85%) had three or more stenotic lesions, while 8 (17.77%) also had concurrent ECAS. Table 1 presents the baseline characteristics of the study participants.

Flowchart of the patient selection process.
Regarding lipid-related parameters, we observed the following significant differences among the study groups. Compared to the NCAS group, TC levels were significantly higher in the ICAS (t = 3.048, P = 0.003), ECAS (t = 3.328, P = 0.001), and COAS (t = 3.809, P < 0.001) groups. Similarly, LDL-C levels were significantly elevated in the ICAS (t = 4.437, P < 0.001), ECAS (t = 4.187, P < 0.001), and COAS (t = 5.291, P < 0.001) groups. However, HDL-C levels were only significantly declined in the ICAS (t =-2.871, P = 0.008) groups. In addition, apoB levels showed a significant increase in the ICAS ( t = 6.816, P < 0.001), ECAS (t = 5.324, P < 0.001), and COAS (t = 7.576, P < 0.001) groups.ApoA1 levels showed a significant decrease in the ICAS ( t = -3.362, P = 0.001) and COAS (t =-3.278, P = 0.001) groups. Finally, the apoB/apoA1 ratio was significantly higher in the ICAS (t = 6.811, P < 0.001), ECAS (t = 5.351, P < 0.001), and COAS (t = 9,310, P < 0.001) groups compared to the NCAS group.
In addition, the prevalences of hypertension and diabetes were significantly higher in the ICAS, ECAS, and COAS groups compared to the NCAS group. However, no significant differences were observed in age or gender among the four groups.
Comparison of ApoB/ApoA1 ratio across stenosis numbers
To further explore the relationship between the ApoB/ApoA1 ratio and the severity of atherosclerosis, we compared the ratio across different numbers of stenotic lesions within the ICAS and ECAS groups to determine whether it varied with the progression of arterial stenosis.
As shown in Fig. 2, the median (IQR) ApoB/ApoA1 ratio across 0, 1, 2, and ≥ 3 intracranial stenotic lesions was 0.7614 (0.6189–0.9456), 0.9663 (0.8177–1.144), 0.9604 (0.8709–1.082), and 1.052 (0.8424–1.172), respectively. Similarly, in the ECAS group (Fig. 3), the median (IQR) ApoB/ApoA1 ratio for 0, 1, 2, and ≥ 3 extracranial stenotic lesions was 0.8318 (0.6633–1.019), 0.9600 (0.8333–1.145), 0.9604 (0.9206–1.042), and 1.026 (0.8169–1.176), respectively.

ApoB/apoA1 ratio across different numbers of intracranial stenoses. The box represents the IQR, with the median indicated by the horizontal line inside the box.

ApoB/apoA1 ratio across different number of extracranial stenosis. The box represents the IQR, with the median indicated by the horizontal line inside the box.
However, the Kruskal-Wallis test and post hoc Mann-Whitney U tests revealed that there were no significant differences in the ApoB/ApoA1 ratio across different numbers of stenotic lesions in both the ICAS and ECAS groups.
Association between apoB/apoA1 ratio quartiles and cerebral atherosclerosis stenosis
To further investigate the relationship between the apoB/apoA1 ratio and cerebral atherosclerosis stenosis, we classified patients into quartiles based on the distribution of their apoB/apoA1 ratio (1st ≤ 0.7238; 0.7238 < 2nd ≤ 0.8926; 0.8926 < 3rd ≤ 1.057; 4th > 1.057). The analysis revealed that higher quartiles of the apoB/apoA1 ratio were associated with an increased incidence of cerebral atherosclerosis stenosis (P < 0.005, Fig. 4).

Distribution of study groups across apoB/apoA1 ratio quartiles. Values represent the percentage of patients in each quartile. ICAS intracranial atherosclerotic stenosis, ECAS extracranial carotid stenosis atherosclerosis, COAS combined intracranial and extracranial atherosclerosis stenosis, NCAS non-cerebral stenosis atherosclerosis.
Risk factors for ICAS and ECAS
To further determine whether the apoB/apoA1 ratio serves as an independent risk factor for intracranial and extracranial atherosclerosis, we performed the logistic regression analysis.
As reported in Table 2, we first performed univariable logistic regression analysis for each variable and included those with P < 0.05 in the multivariable logistic regression model. As a result, age, ApoB/ApoA1 ratio, TC, HDL-C, and LDL-C were selected for further analysis. Then, the multivariable regression results (Table 3) demonstrated that the ApoB/ApoA1 ratio was independently associated with ICAS (OR: 2.67, 95% CI: 1.53–4.87), whereas it was not identified as an independent risk factor for ECAS.
Subsequently, to further validate the robustness of this association, we conducted additional sensitivity analyses (Table 4). We found that, across all models, the ApoB/ApoA1 ratio consistently remained a significant independent predictor of ICAS, reinforcing the reliability of this finding.
Diagnostic performance of the apoB/apoA1 ratio
To assess the diagnostic value of the apoB/apoA1 ratio for intracranial stenosis, we conducted a ROC analysis. The results revealed that the area under the curve (AUC) of the apoB/apoA1 ratio for diagnosing intracranial stenosis was 0.764 (95% CI: 0.717–0.810, P < 0.001). The optimal cut-off value was determined to be 0.8122, yielding a sensitivity of 81.3% and a specificity of 59.8% (Fig. 5).

ROC curve analysis of the apoB/apoA1 ratio for predicting ICAS.
Discussion
In this study, the apoB/apoA1 ratio was significantly higher in patients with ICAS, ECAS and COAS compared to those in the NCAS group. Furthermore, multivariable logistic regression analysis revealed that ICAS was independently associated with the apoB/apoA1 ratio, but not with ECAS. According to the ROC analysis, the optimal cut-off value for this ratio in identifying ICAS was determined to be 0.8122. However, no significant differences in the apoB/apoA1 ratio were observed across different ICAS segment counts suggesting that while the ApoB/ApoA1 ratio is associated with the presence of atherosclerosis, it may not vary significantly with increasing stenosis severity.
Meanwhile, compared to other conventional cholesterol measurements, our research demonstrated that the apoB/apoA1 ratio had a stronger prognostic value for vascular diseases. These findings are consistent with those of previous studies13,14.
Many studies15,16 have suggested that, compared with other lipoprotein particles, apoA1 and apoB may remain moderately elevated in older individuals and in those receiving statin therapy. ApoA1, the major apolipoprotein in HDL-C, has been shown to play a critical role in anti-atherosclerosis due to its antioxidant activity17. Previous studies have indicated that apoA1 deficiency may underlie the pathological mechanism of intracranial atherosclerotic stenosis18. On the other hand, apoB, the primary apolipoprotein in LDL-C, is considered a marker of atherogenic properties19. An elevated apoB/apoA1 ratio is likely to promote cholesterol deposition in the arterial wall, accelerating atherogenesis and increasing the risk of vascular disease20.
Additionally, we discovered that the apoB/apoA1 ratio was an independent risk factor for ICAS but not for ECAS. Low wall shear stress and hyperlipidemia have been identified as key hemodynamic risk factors in the development of atherosclerotic plaques in extracranial arteries21. Autopsy studies of patients with cerebral infarction have shown that atherosclerotic plaques differ between intracranial and extracranial arteries22. Furthermore, unaffected intracranial arteries exhibit a stronger antioxidant response compared to extracranial arteries, although this antioxidant protection declines significantly with age23. Therefore, differences in risk factors exist between extracranial and intracranial atherosclerotic stenosis. The apoB/apoA1 ratio may serve as a valuable indicator of vascular damage and a potential target for preventing vascular injury, particularly in the case of the intracranial artery. Previous studies have proposed that a high ApoB/ApoA1 ratio may reflect a loss of antioxidant and anti-atherosclerotic protection, which could contribute to deep subcortical ischemic burden and consequently increase the risk of cognitive decline and stroke recurrence11,12,24. These findings are largely consistent with our results. The underlying mechanisms likely involve multiple pathophysiological pathways, primarily oxidative stress imbalance and matrix metalloproteinase (MMP) activation. ApoA1 plays a crucial anti-atherosclerotic role by promoting cholesterol efflux, inhibiting lipid oxidation, and maintaining endothelial function25,26. However, in individuals with a high apoB/apoA1 ratio, reduced ApoA1 levels may compromise these protective effects, accelerating atherosclerotic plaque formation and vascular inflammation. Moreover, an elevated ApoB/ApoA1 ratio reflects increased ApoB levels, which can upregulate MMP-2 and MMP-9 activity17,27. MMPs are critical regulators of extracellular matrix degradation, and their overexpression has been linked to endothelial dysfunction and blood-brain barrier disruption27. Consequently, excessive MMP activation promotes vascular inflammation, smooth muscle cell apoptosis, and plaque rupture—key contributors to ICAS progression. In essence, a high ApoB/ApoA1 ratio indicates both increased ApoB and decreased ApoA1, collectively heightening the risk of ICAS.
Our ROC analysis demonstrated that the apoB/apoA1 ratio has a good diagnostic ability for intracranial atherosclerosis stenosis, with an AUC of 0.764, a sensitivity of 81.3%, and a specificity of 59.8%. These findings suggest that the apoB/apoA1 ratio may serve as a useful biomarker for identifying patients at higher risk of intracranial atherosclerosis stenosis. It is widely recognized that the sensitivity of a diagnostic test reflects its ability to correctly identify patients with the condition, thereby minimizing missed diagnoses, while specificity measures its ability to correctly exclude those without the condition, reducing incorrect diagnoses28. Here, we found that apoB/apoA1 ratio demonstrated a high sensitivity and a moderate specificity. In the context of stroke prevention, sensitivity is more critical than specificity, as failing to identify high-risk individuals could delay appropriate intervention, increasing the risk of stroke occurrence. Therefore, the apoB/apoA1 ratio may serve as a valuable initial screening tool, enabling the early identification of high-risk populations who would benefit from further diagnostic assessments and timely preventive strategies to reduce stroke incidence, highlighting its practical utility in clinical settings.
However, this study has several limitations that should be acknowledged. First, this was a single-center study, with data collected from a single institution, which may limit the generalizability of our findings to broader populations since ethnic, regional, and healthcare system differences may also influence the applicability of our results. Hence, future multicenter studies are required to validate these findings. Second, our study only included individuals with ischemic stroke, and we did not assess those with asymptomatic intracranial atherosclerosis stenosis. Since a significant proportion of intracranial atherosclerosis cases remain asymptomatic until a major vascular event occurs, our results may not fully capture the entire spectrum of disease progression. As a result, future research should consider evaluating both symptomatic and asymptomatic individuals to better understand the role of the apoB/apoA1 ratio in early detection. Third, blood samples were collected within seven days of stroke onset, meaning that apoB and apoA1 levels were measured during the acute phase of ischemic stroke. While previous research suggests that apoB and apoA1 levels remain relatively stable within four weeks after a stroke29 acute-phase responses could still have slight influences on the results. Fourth, while these criteria helped ensure a more homogenous study cohort, we acknowledged that they may introduce certain selection biases. Therefore, future studies should consider serial measurements of apoB/apoA1 ratios at different time points post-stroke to assess potential variations over time.
Conclusion
This study demonstrated that the apoB/apoA1 ratio may serve as a valuable biomarker for ICAS risk assessment. Early identification of high-risk individuals through ApoB/ApoA1 ratio screening could enable timely intervention strategies, ultimately helping to mitigate stroke risk and reduce the associated healthcare burden.
Data availability
The datasets supporting the conclusions of this article are available from the corresponding author upon reasonable request.
References
GBD 2021 Diseases and Injuries Collaborators. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. Lancet 403 (10440), 2133–2161 (2024).
Bonati, L. H., Jansen, O., de Borst, G. J. & Brown, M. M. Management of atherosclerotic extracranial carotid artery stenosis. Lancet Neurol. 21 (3), 273–283 (2022).
de Havenon, A. et al. Large vessel occlusion stroke due to intracranial atherosclerotic disease: identification, medical and interventional treatment, and outcomes. Stroke 54 (6), 1695–1705 (2023).
Liu, D., Zhang, Y., Wang, C. & Zuo, H. Association of the ApoB/ApoA-I ratio with stroke risk: findings from the China health and nutrition survey (CHNS). Nutr. Metab. Cardiovasc. Dis. 32 (1), 203–209 (2022).
Ordóñez-Llanos, J. & Escolà-Gil, J. C. Apolipoproteins in health and disease. Int. J. Mol. Sci. 25 (13), 7048 (2024).
Li, S., Xie, X., Zeng, X., Wang, S. & Lan, J. Serum Apolipoprotein B to Apolipoprotein A-I ratio predicts mortality in patients with heart failure. ESC Heart Fail. 11 (1), 99–111 (2024).
Zhang, J. et al. ApoB/ApoA-Ι is associated with major cardiovascular events and readmission risk of patients after percutaneous coronary intervention in one year. Sci. Rep. 15 (1), 996 (2025).
Rasouli, M. & Kiasari, A. M. Interactions of serum HsCRP with ApoB, ApoB/AI ratio and some components of metabolic syndrome amplify the predictive values for coronary artery disease. Clin. Biochem. 39 (10), 971–977 (2006).
Huang, G. et al. Coalition of DNA polymorphisms of ApoB and ApoAI genes is related with coronary artery disease in Kazaks. J. Geriatr. Cardiol. JGC. 9 (1), 33–37 (2012).
Park, J. H., Hong, K. S., Lee, E. J., Lee, J. & Kim, D. E. High levels of Apolipoprotein B/AI ratio are associated with intracranial atherosclerotic stenosis. Stroke 42 (11), 3040–3046 (2011).
Lee, M. et al. High ApoB/ApoA-I ratio predicts post-stroke cognitive impairment in acute ischemic stroke patients with large artery atherosclerosis. Nutrients 15 (21), 4670 (2023).
Huang, W. et al. Fang Yi Ke Da Xue Xue Bao 38(8), 992–996 (2018).
Walldius, G. et al. Long-term risk of a major cardiovascular event by ApoB, apoA-1, and the apoB/apoA-1 ratio-experience from the Swedish AMORIS cohort: A cohort study. PLoS Med. 18(12), e1003853 (2021).
Ding, M. et al. The association of apolipoproteins with later-life all-cause and cardiovascular mortality: a population-based study stratified by age. Sci. Rep. 11 (1), 24440 (2021).
O’Donnell, M. J. et al. Association of lipids, lipoproteins, and apolipoproteins with stroke subtypes in an international case control study (INTERSTROKE). J. Stroke. 24 (2), 224–235 (2022).
Lin, J., Si, Z. & Wang, A. Predictive value of ApoB/ApoA-I for recurrence within 1 year after first incident stroke. Front. Neurol. 14, 1308442 (2024).
Sacher, S., Mukherjee, A. & Ray A.Deciphering structural aspects of reverse cholesterol transport: mapping the knowns and unknowns. Biol. Rev. Camb. Philos. Soc. 98 (4), 1160–1183 (2023).
Kalani, R. et al. Apolipoproteins B and A1 in ischemic stroke subtypes. J. Stroke Cerebrovasc. Dis. 29 (4), 104670 (2020).
Behbodikhah, J. et al. Apolipoprotein B and cardiovascular disease: biomarker and potential therapeutic target. Metabolites 11 (10), 690 (2021).
Pikkemaat, M. et al. Lipids and apolipoproteins and the risk of vascular disease and mortality outcomes in women and men with type 2 diabetes in the ADVANCE study. Diabetes Obes. Metab. 26 (12), 5669–5680 (2024).
Malek, A. M., Alper, S. L. & Izumo S.Hemodynamic shear stress and its role in atherosclerosis. JAMA 282 (21), 2035–2042 (1999).
Rosário, M. & Fonseca, A. C. Update on biomarkers associated with large-artery atherosclerosis stroke. Biomolecules 13 (8), 1251 (2023).
D’Armiento, F. P. et al. Age-related effects on atherogenesis and scavenger enzymes of intracranial and extracranial arteries in men without classic risk factors for atherosclerosis. Stroke 32 (11), 2472–2479 (2001).
Li, Z. et al. Elevated ApoB/ApoA-Ι ratio is associated with poor outcome in acute ischemic stroke. J. Clin. Neurosci. 107, 138–143 (2023).
Wang, Y. et al. Intracranial atherosclerotic disease. Neurobiol. Dis. 124, 118–132 (2019).
Hahn, B. H. & McMahon, M. Atherosclerosis and systemic lupus erythematosus: the role of altered lipids and of autoantibodies. Lupus 17 (5), 368–370 (2008).
Botham, K. M. & Wheeler-Jones, C. P. Postprandial lipoproteins and the molecular regulation of vascular homeostasis. Prog Lipid Res. 52 (4), 446–464 (2013).
Obuchowski, N. A. & Bullen, J. A. Receiver operating characteristic (ROC) curves: review of methods with applications in diagnostic medicine. Phys. Med. Biol. 63 (7), 07TR01 (2018).
Kargman, D. E. et al. Lipid and lipoprotein levels remain stable in acute ischemic stroke: the Northern Manhattan stroke study. Atherosclerosis 139 (2), 391–399 (1998).
Acknowledgements
We thank all the study participants for their assistants and supports.
Funding
Quanzhou City Science and Technology Program of China (No. 2024 NY026). Startup Fund for scientific research, Fujian Medical University(No.2023QH1125).
Author information
Authors and Affiliations
Contributions
Mimi Li and Chunnuan Chen conceptualized the study, analyzed and interpreted the data, and drafted and revised the manuscript.Lichao Ye analyzed and interpreted the data, drafted and revised the manuscript, did the statistical analysis, and prepared all the figures.Mimi Li did the interpretation of the data and revision of the manuscript. All authors contributed to the writing and revisions of the paper and approved the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics declarations
This study was approved by the Ethics Committee of The Second Affiliated Hospital of Fujian Medical University, Quanzhou, Fujian Province, China. Written informed consent was obtained from all participants prior to enrollment. For patients who were unable to provide consent due to severe stroke, coma, or impaired consciousness, informed consent was obtained from their legally authorized representatives. All procedures involving human participants were conducted in accordance with the Declaration of Helsinki.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, M., Ye, L. & Chen, C. Association of ApoB/apoA1 ratio with stenosis of intracranial and extracranial arteries in patients with ischaemic stroke. Sci Rep 15, 13622 (2025). https://doi.org/10.1038/s41598-025-97625-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-97625-9
