
Abstract
We evaluated the reliability and validity of the Korean translation of the quality of oncology nursing care scale (K-QONCS) and verified its suitability as a tool to assess the quality of cancer patient care in Korea. To validate the content validity of the K-QONCS, five oncology nurse experts assessed the suitability of the adapted tools. Exploratory factor analysis (EFA) was used to assess construct, convergent, discriminant, and criterion validity. A survey of 235 adults aged > 18 years who had been diagnosed with cancer and were receiving treatment was conducted to validate the K-QONCS. The QONCS was translated and appropriately modified to reflect expert opinion, and its content validity was confirmed to be high through indicators such as item-level content validity index, scale-level content validity index using an averaging calculation (S-CVI/Ave), and S-CVI/universal agreement. Eight factors were derived by EFA; each factor reflected different aspects of quality of care. The scale exhibited convergent and discriminant validity, demonstrated by multitrait-multimethod matrix analysis and correlation analysis with the Nursing Satisfaction Scale. The Cronbach’s alpha coefficient was 0.92, indicating high overall internal consistency. We demonstrated the reliability and feasibility of the K-QONCS. The K-QONCS may help oncology nurses to improve patient care experiences and outcomes as well as advance oncology nursing practices in South Korea.
Similar content being viewed by others

Introduction
Ensuring high-quality oncological nursing care is a critical objective for healthcare providers1,2. Nurses play an indispensable role in attaining and maintaining high-quality, personalized care of patients with cancer3,4. Their impact is attributed to the time spent with patients, establishment of intimate relationships, development of trust, and effective communication5,6,7.
Patients undergoing cancer treatment encounter multiple health-related challenges and have specific needs that require complex and individualized care, necessitating a multidisciplinary approach and comprehensive support to patients and their families8,9. Within this multidisciplinary framework, clinical nurse specialists and advanced nurse practitioners identify and address the physical, psychological, and social needs of patients8,10. The timely identification of care gaps that may negatively impact the perceived level of patient-care is important. Nurses rely on their advanced communication skills to bridge the gap between service providers and patients to achieve a holistic assessment of patients’ needs and promote patient-centered care11,12.
Despite the complexity of cancer care and the importance of quality nursing care, no consensus for defining quality cancer care is available13,14 and only few disease-specific questionnaires are available. Existing questionnaires, such as the oncology patients’ perceptions of the quality of nursing care scale (OPPQNCS)15, the quality patient care scale16, and the palliative care quality of life instrument17, are restricted in their use as lack a clear definition of quality nursing care and a theoretical framework informing their development15. Furthermore, some questionnaires are not based on patients’ perceptions, thereby limiting their validity. The holistic aspects of care, including patients’ spiritual needs, are not adequately addressed in existing questionnaires, including the OPPQNCS. Given that cancer patients frequently experience psychological distress, fear of cancer recurrence (FCR), and existential concerns in addition to their physical symptoms, a more comprehensive measurement tool that accounts for these multidimensional aspects is necessary (13)18. Most existing questionnaires focus on the overall quality of care rather than on nursing care, and often fail to focus on the unique needs stemming from cancer diagnosis and treatment.
Additionally, previous studies have highlighted the impact of nursing quality on clinical outcomes, patient satisfaction, and adherence to treatment, emphasizing the need for precise assessment tools in oncology nursing3,6. Nursing care that effectively addresses patients’ emotional and informational needs has been linked to improved psychological well-being and reduced symptom burden among cancer patients19. Therefore, a validated tool that captures the specific components of high-quality oncology nursing care is essential for improving patient outcomes and guiding evidence-based nursing practice.
Adapting assessment tools developed abroad to the unique characteristics of oncology nursing care in South Korea presents with several challenges. Cultural, language, and healthcare systems differences must be considered to ensure the relevance and applicability of the instrument13,14. For instance, cultural differences in patient expectations, communication styles, and perceptions of nursing care may influence how patients interpret and respond to questionnaire items, necessitating careful linguistic and contextual adaptation (21)20. Without an appropriate evaluation criteria, patients cannot effectively communicate their expectations to staff members. Consequently, an evaluation tool designed specifically to assess the quality of oncology nursing care in Korean oncology units is needed.
Thus, this study aimed to address this need by translating the QONCS into Korean and adapting it to the South Korean context; the QONCS was originally developed by Charalambous and Adamakidou14. This adaptation process followed rigorous translation and validation procedures, ensuring that the Korean version maintains conceptual equivalence with the original while reflecting the unique cultural and healthcare characteristics of South Korea21. The Korean version of the QONCS (K-QONCS) would support ongoing efforts to enhance the overall quality of oncology nursing care provided to patients with cancer in South Korea.
Methods
Participants
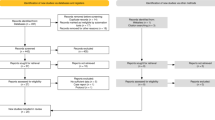
The study included patients with cancer aged ≥ 18 years who were undergoing cancer treatment. As the number of participants for the exploratory factor analysis (EFA) of the composition validity test should be 5–10 times the number of items22, a minimum of 204 participants were needed (i.e., 6 times the number of items, based on 34 items). Considering a dropout rate of 20%, we planned to recruit 255 participants. Finally, 245 participants were recruited, and the data of 235 participants were obtained after excluding four duplicates and six dishonest survey responses (e.g., all responses answered with the same number). This resulted in a final response rate of 95.9%.
Instrument: QONCS
The QONCS is a tool14 used to explore the quality of nursing care provided in oncology settings from the patient’s perspective. It consists of five sub-dimensions and 34 questions. The sub-dimensions are as follows: being supported and confirmed (16 items), spiritual care (6 items), sense of belonging (5 items), being valued (4 items), and being respected (3 items). Scores are measured on a 5-point Likert scale, graded between 1 (completely disagree) and 5 (completely agree). Higher scores indicate a higher quality of oncology nursing care, and vice-versa. The Cronbach’s alpha for the 34 items was 0.9514.
Process
Translation
The translation process followed the World Health Organization guidelines21. First, two bilingual English and Korean translators translated the tool from English to Korean. The authors then checked the translation for terminology, wording, and clarity. The translation was then back-translated by an independent researcher fluent in both English and Korean. The authors checked the original tool and the Korean version for inconsistencies. After a consensus was achieved, the translation was finalized.
Content validity
To validate the content validity of the K-QONCS, five experts, including two nurses with 10 years of experience in caring for cancer patients and three professors specialized in basic and adult nursing, evaluated the adapted tool for suitability. The expert group rated content equivalence on a 4-point Likert scale (1 = not relevant, 2 = somewhat relevant but needs modification, 3 = quite relevant but needs some modification, 4 = highly relevant)23. After evaluating the validity, we calculated the item-level content validity index (I-CVI) and scale-level content validity index using an averaging calculation (S-CVI/Ave). Content validity was considered adequate if the I-CVI was ≥ 0.78 and the S-CVI was ≥ 0.9024.
Data collection
Convenience sampling was used to recruit participants and an online survey link was distributed through blogs and forums in which patients with cancer participate. Before participation, potential respondents were provided a written explanation of the study’s purpose, methodology, and voluntary nature of participation on a web page. They were assured that their privacy and confidentiality were protected. To obtain informed consent, participants were asked to indicate their agreement by clicking a “Next” button to proceed with the online survey. Participants could withdraw from the study at any time without any consequences. All methods in this study were performed in accordance with the relevant guidelines and regulations, ensuring compliance with ethical and procedural standards.
Data quality control
To ensure data quality and reliability, several measures were implemented. The survey was conducted through the Embrain survey platform, a reputable and widely used online survey service in South Korea, ensuring access to a structured and diverse respondent pool beyond informal online forums. Participants were required to meet specific inclusion criteria (e.g., age ≥ 18 years, current cancer treatment) before proceeding with the survey to ensure that only relevant participants contributed data.
To improve data integrity, consistency checks were implemented to identify and exclude low-quality responses. This included screening for duplicate entries, unusually fast completions, and uniform response patterns (e.g., selecting the same number for all questions). Additionally, participants were informed about the importance of providing accurate and truthful responses and were assured of data anonymity to minimize potential biases.
Validity test
To assess construct validity, an EFA was conducted. Additionally, convergent validity, discriminant validity, and criterion validity were verified.
Exploratory factor analysis
EFA used principal component analysis and varimax rotation to extract potential factors from the data.
Convergent and discriminant validity
A multitrait-multimethod (MTMM) matrix was used to verify convergent and discriminant validity. When the correlation coefficient exceeded 0.40 after accounting for the overlap between the subfactors to which the item belonged, it was considered to have adequate convergent validity25. If the difference between the item’s correlation with its subscale and its correlation with other subscales was larger than twice the standard error of correlation coefficients, the item was considered to have discriminant validity25,26.
Criterion validity
To evaluate the validity of the K-QONCS, we used the Patient Satisfaction Instrument (PSI) developed by Hinshaw and Atwood27 that was adapted into Korean by Yang28. This tool was developed to measure nursing satisfaction among hospitalized patients and consists of the following domains: technical-professional care (7 items), patient education (7 items), and trust (11 items). The reliability and validity of this instrument have been reported29 and it has been used in several studies30,31. The validity of the instrument has been verified through correlation analysis, with higher correlations indicating higher validity.
Reliability
Reliability was measured by calculating Cronbach’s ⍺ value, which measures acceptable internal consistency. Cronbach’s ⍺ for each factor of the 34-item K-QONCS and Cronbach’s ⍺ for the total items were analyzed.
Data analysis
SPSS version 26.0 (SPSS Inc., Chicago, IL, USA) was used to analyze the data. Descriptive statistics were used for general characteristics and item analysis. Construct validity was verified using EFA. Convergent and discriminant validity was verified through MTMM. Pearson’s correlation coefficient was used to assess validity and reliability.
Results
Characteristics of study participants
Table 1 shows the general characteristics of study participants The mean age of the participants was 42.80 years (standard deviation [SDa = 7.99), and more than two-thirds were female. Over 70% of the participants were married, and about three-quarters had a university degree or higher education. Breast cancer was the most common cancer type, followed by stomach and thyroid cancers. Stage 2 was the most common cancer stage and chemotherapy was the most common treatment modality. Most patients had been diagnosed 1–2 years earlier, followed by those diagnosed in less than a year.
Validity
Content validity
Content validity was verified using the I-CVI and the S-CVI/Ave and the S-CVI/universal agreement (S-CVI/UA) (Online Resource 1). The I-CVI was ≥ 0.8, whereas the S-CVI/Ave was 0.95 and S-CVI/UA was 0.74. No questions were deleted based on the results of content validity verification. Additionally, appropriate modifications were made to reflect the opinions of experts and words were corrected.
EFA
The factor structure was validated by EFA. The Kaiser–Meyer–Olkin (KMO) score was 0.88 and the Bartlett sphericity was 3012.22 (p < .001), indicating a suitable fit for EFA32. Principal component analysis and varimax rotation revealed that the communality of the 34 items ranged from 0.33 to 0.79, with all items having a value > 0.3. Eight factors in the K-QONCS had eigenvalues > 1.00 and were above the elbow of the curve in the scree plot. These factors explained 58.59% of the total variance, with all factors having a loading of 0.33–0.79 (Table 2).
Factor 1 is “Spiritual care and sense of belonging” and includes nine items (items 17, 18, 19, 20, 21, 22, 23, 24, 27) and has an explanatory power of 13.75%. Factor 2 is “Be supported” and contains six items (items 1, 6, 10, 12, 29,33) and has an explanatory power of 8.33%. Factor 3 is “Be valued” and includes four items (items 4, 16, 30, 32) and has an explanatory power of 6.93%. Factor 4 is “Get sufficient information” and includes three items (items 8, 11, and 34) and has an explanatory power of 6.69%. Factor 5 is “Trustfulness” and includes three items (items 5, 9, 13) and has an explanatory power of 6.68%. Factor 6 is “Be understood” and includes four items (items 3, 7, 14, 25) and has an explanatory power of 6.62%. Factor 7 is “Be respected” and includes three items (items 15, 26, 28) and has an explanatory power of 5.80%. Factor 8 is “Be cared” and includes two items (items 2, 31) and has an explanatory power of 3.80%.
Furthermore, to assess the presence of common method bias (CMB), we conducted Harman’s Single-Factor Test as part of the exploratory factor analysis (EFA). The results confirmed that the first factor accounted for less than 50% of the total variance, indicating that CMB is not a significant concern in this study.
Convergent and discriminant validity
According to the MTMM matrix, the correlation coefficients among the 34 items and their factors were 0.57–0.83 (all > 0.4); thus, convergent validity was verified. Regarding discriminant validity, the correlation coefficients of each item with the factors to which they did not belong ranged from 0.10 to 0.50. In addition, the correlations between the items and their corresponding factors were larger than between the items and other factors by double the standard error of correlation coefficients, for all items. Therefore, discriminant validity was confirmed (Table 3).
Criterion validity
Discriminant validity was verified through correlation analysis of the K-QONCS and the Nursing Satisfaction Scale. The K-QONCS and Nursing Satisfaction Scale showed a significant moderate level of correlation (r = .41, p < .001). In addition, each factor of the K-QONCS showed a significantly lower level of correlation with the Nursing Satisfaction Scale. These results confirmed the validity of the K-QONCS (Table 4).
Item analysis
The results of the questionnaire analysis are shown in Table 5. Each question had a mean score of 3.39–4.11 and an SD of 0.72–1.28, with no outliers. The skewness of each question ranged from − 0.99 to − 0.32, and the kurtosis ranged from − 0.98 to 0.95, with no skewed values. The item-total correlation coefficient ranged from 0.57 to 0.79, indicating that no item was a low contributor to the instrument18. In addition, the alpha obtained if an item was deleted ranged from 0.32 to 0.87.
Reliability
Internal validity tests showed that Cronbach’s alpha coefficients for all items of the K-QONCS were 0.92, ranging from 0.50 to 0.87 for individual factors.
Discussion
In this study, we translated the QONCS to Korean and adapted it for patients diagnosed with cancer. Content validity ensures that the items included in the instrument adequately represent the construct of interest. Here, content validity of the K-QONCS was assessed using I-CVI, S-CVI/Ave, and S-CVI/UA. The high I-CVI values (≥ 0.8) obtained for each individual item indicate strong agreement among experts regarding the relevance and representativeness of the scale items. The S-CVI/Ave and S-CVI/UA values further confirmed the overall content validity of the K-QONCS. The S-CVI/Ave, exceeded the commonly recommended threshold of 0.90, indicating a high level of agreement among experts regarding the overall content validity of the scale. Additionally, the S-CVI/UA, which considers the proportion of items rated as content-valid by all experts, provides a more stringent assessment of content validity. While the S-CVI/UA value of 0.74 falls slightly below the ideal threshold of 0.80, it still indicates substantial agreement among experts regarding the content validity of the scale. By retaining all items without modification, the K-QONCS maintains its comprehensiveness and inclusivity, ensuring that it captures a broad range of dimensions relevant to the quality of oncology nursing care. Moreover, appropriate modifications were made to reflect the opinions of experts and address any concerns regarding item wording or clarity. The comprehensive assessment of content validity in this study provides a solid foundation for the use of the K-QONCS in evaluating the quality of oncology nursing care in the South Korean context. Considering the strong content validity here, healthcare providers and researchers can rely on the K-QONCS as a valid and reliable tool for assessing and improving oncology nursing care quality.
EFA identified the underlying dimensions of the adapted scale, provided insights into the specific aspects of oncology nursing care being measured, and determined the key factors contributing to the overall quality perceived by patients. The KMO measure of sampling adequacy (0.88) and Bartlett’s test of sphericity (p < .001) both indicated that the data were suitable for EFA. These findings suggested that the correlations among the items were sufficiently strong to support factor analysis. Additionally, the high communalities of most items indicated that the majority of items shared substantial variance with the underlying factors, supporting their inclusion in the analysis. The decision not to delete the only item with a communality slightly below 0.4 (item 5) was justified based on its proximity to the threshold and on the researchers’ judgment.
The EFA further validated the underlying structure of the K-QONCS, revealing eight distinct factors related to different dimensions of oncology nursing care. Factors were named based on the items strongly loaded onto them and their conceptual themes. The original instrument14 consisted of five factors, whereas this study has eight factors. “Spiritual care” and “Sense of Belonging” from the original instrument were combined into one factor, and the four additional factors were “Get sufficient information”, “Trustfulness”, “Be understood”, and “Be cared for”. It was noteworthy that “Get sufficient information” emerged as a factor in that it was a factor that did not emerge in other studies that validated the instrument33,34,35. This suggests that Korean cancer patients have a high information need for nursing care, supporting previous studies. In a previous study that identified unmet needs among South Korean esophageal cancer survivors, information was the most frequently mentioned domain36. Also the domains with the highest levels of unmet need among Korean breast cancer survivors were information and education37. Furthermore, a study on digital healthcare for Korean cancer patients found that there was a significant need for cancer education and information among these patients38. This shows that information provision is an important factor in the care of Korean cancer patients, and this tool can be evaluated as an appropriate tool that takes into account the characteristics of the Korean population. “Be understood” can be seen as a reflection of Korean culture. As a collectivist culture where emotional suppression is seen as more adaptive39, Koreans tend to shy away from direct and open emotional expression compared to Western cultures, which are more individualistic40. This can lead to a tendency to implicitly expect the other person to understand rather than directly express their feelings, which may be related to the occurrence of this factor. The identification of these factors provides a comprehensive framework for understanding the multifaceted nature of oncology nursing care quality and informs targeted interventions to enhance patient experiences and outcomes. The explanatory power of each factor, as indicated by the percentage of variance explained, ranged from 3.80 to 13.75%. This variability in explanatory power underscores the heterogeneity of oncology nursing care quality and the multidimensional nature of the construct. Considering the unique contributions of each factor, healthcare providers can prioritize areas for improvement and tailor their interventions appropriately.
Clinically, the identification of distinct factors within the K-QONCS highlights the importance of addressing multiple dimensions of oncology nursing care quality according to patients’ needs. Focusing on aspects, such as spiritual support, communication, and respect, can help healthcare providers deliver more holistic and patient-centered care. In research, the validated factor structure provides a reliable framework for assessing and comparing nursing care quality across different contexts and populations. Future studies may further explore the predictive validity of the scale factors in relation to patient outcomes and satisfaction. The EFA results have improved our understanding of oncology nursing care quality and provided a validated framework for assessing and improving care practices in our country.
The results of the MTMM matrix analysis demonstrated strong convergent validity, with correlation coefficients between the 34 items and their respective factors ranging from 0.57 to 0.83. These coefficients exceeded the commonly accepted threshold of 0.40, indicating that each item correlated strongly with its intended factor, supporting the scale’s ability to measure the construct of interest consistently. For discriminant validity, the observed coefficients ranged from 0.10 to 0.50, indicating that the items had significantly lower correlations with unrelated factors, thus supporting the scale’s ability to discriminate between related and unrelated constructs. Additionally, the correlations between the items and their corresponding factors were notably larger than those with other factors, further validating the distinctiveness of each factor and the discriminant validity of the scale overall.
Criterion validity, specifically discriminant validity, was further assessed by assessing the correlation of the K-QONCS scores with those of the Nursing Satisfaction Scale. The significant moderate correlation observed between the two scales (r = .41, p < .001) suggests a certain degree of overlap in the constructs being measured. However, the significantly lower correlations between each factor of the K-QONCS and the Nursing Satisfaction Scale provide evidence of discriminant validity, indicating that the K-QONCS measures distinct aspects of nursing care quality beyond overall satisfaction with nursing care.
The item analysis conducted on the K-QONCS provides valuable insights into the performance and reliability of individual items within the scale. Examining various statistical parameters can help assess the contribution of each item to the scale’s overall reliability and validity. According to the mean scores of each item, the participants generally perceived a moderate to high level of oncology nursing care quality across all items. The narrow range of SDs (0.72–1.28) suggested that responses were relatively consistent and did not exhibit extreme variability. Similarly, the skewness and kurtosis values fell within an acceptable range, indicating that the distribution of responses for each item was approximately symmetrical and normally distributed, without any significant outliers or extreme values. The item-total correlation coefficients ranged from 0.57 to 0.79, indicating that all items correlated positively with the total score of the scale. Higher correlations indicate stronger associations between individual items and the underlying construct being measured. Clinically, healthcare providers can use the K-QONCS to identify specific areas of strength and areas for improvement in oncology nursing care delivery. Also, nurses can use items with lower means or weaker correlations to enhance patients’ overall care experiences. In research, the item analysis provides evidence of the scale’s reliability and validity, supporting its use as a robust measurement tool in studies assessing oncology nursing care quality. Future research could further explore the psychometric properties of the K-QONCS. Additionally, qualitative research methods could be employed to gain a deeper understanding of patient perspectives on oncology nursing care quality. By employing rigorous psychometric analyses, researchers and healthcare providers can enhance the quality of care provided to cancer patients and contribute to the advancement of oncology nursing practice and research.
The high Cronbach’s alpha coefficient of 0.92 for all items on the K-QONCS indicates high correlation between items and the reliability of the scale in assessing the quality of nursing care across a range of dimensions. Additionally, Cronbach’s alpha coefficients ranged from 0.50 to 0.87 for each factor, further validating the reliability of the K-QONCS at the factor level. Although there were variations, all factors fell within an acceptable range, suggesting that each factor captures distinct yet internally consistent dimensions of oncology nursing care quality. Healthcare providers and researchers can confidently use the scale to identify areas for improvement, knowing that it yields consistent and stable measurements over time and across different patient populations. Additionally, the assessment of reliability at the factor level provides insights into the internal consistency of specific dimensions of care quality, guiding future research efforts aimed at understanding the multidimensional nature of oncology nursing care.
This study has some limitations. Convenience sampling was used, which might have limited the generalizability of the results. Although the survey was conducted through the Embrain survey platform, a professional online survey service, selection bias may still exist, as participation was voluntary and limited to individuals with access to online platforms. Additionally, as this study focused on patients currently undergoing cancer treatment, the results may not reflect the experiences of patients at different stages of cancer. To strengthen the utility and impact of the K-QONCS on oncology nursing practice, further studies with larger, more diverse sample populations and alternative recruitment strategies, such as randomized or stratified sampling, are warranted. Future research should also explore the scale’s applicability across various healthcare settings and its association with patient outcomes to enhance its validity and broader relevance.
Conclusion
We developed a reliable and valid evaluation tool, tailored to assess the quality of oncology nursing care in the unique context of South Korea. By providing a standardized and validated measurement tool, we aim to raise awareness of the pivotal role of oncology nursing care and enhance understanding of the essential competencies required by oncology nurses to deliver high-quality care. The K-QONCS can potentially empower oncology nurses in tailoring their care approaches to meet the unique and evolving needs of patients with cancer, thereby contributing to the enhancement of their overall quality of life. Additionally, ongoing validation and refinement efforts will further strengthen the utility and reliability of the K-QONCS.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Li, Y. et al. Oncology nursing on the move: A contemporary issue on Chinese oncology nursing in cancer care. Front. Public Health 11, 1061572. (2023). https://doi.org/10.3389/fpubh.2023.1061572
Naito, T. Uniting for greater impact: The crucial role of oncology nurses in cancer care. Asia Pac. J. Oncol. Nurs. 11, 100370. (2023). https://doi.org/10.1016/j.apjon.2023.100370
Bashkin, O., Asna, N., Amoyal, M. & Dopelt, K. The role of nurses in the quality of cancer care management: Perceptions of cancer survivors and oncology teams. Semin. Oncol. Nurs. 39, 151423. (2023). https://doi.org/10.1016/j.soncn.2023.151423
Mojarad, F. A., Sanagoo, A. & Jouybari, L. Exploring the experiences of oncology nurses about the factors facilitating their presence at the bedside of patients with cancer: A qualitative study. Indian J. Palliat. Care 25, 236–241. (2019). https://doi.org/10.4103/IJPC.IJPC_187_18
Moghadam, M. P., Nasiri, A. & Mahmoudirad, G. Exploring the emotional concerns of oncology nurses: A qualitative study. Iran. J. Nurs. Midwifery Res. 27, 425–431. (2022). https://doi.org/10.4103/ijnmr.ijnmr_258_21
Rajcan, L., Lockhart, J. S. & Goodfellow, L. M. Generating oncology patient trust in the nurse: An integrative review. West. J. Nurs. Res. 43, 85–98. (2021). https://doi.org/10.1177/0193945920930337
Zamanzadeh, V. et al. Factors influencing communication between the patients with cancer and their nurses in oncology wards. Indian J. Palliat. Care 20, 12–20. https://doi.org/10.4103/0973-1075.125549 (2014).
Silbermann, M. et al. Multidisciplinary care team for cancer patients and its implementation in several middle Eastern countries. Ann. Oncol. 24 Suppl. (7), vii41–vii47. https://doi.org/10.1093/annonc/mdt265 (2013).
Tuggey, E. M. & Lewin, W. H. A multidisciplinary approach in providing transitional care for patients with advanced cancer. Ann. Palliat. Med. 3, 139–143. (2014). https://doi.org/10.3978/j.issn.2224-5820.2014.07.02
Kurniasih, D. A. A., Setiawati, E. P., Pradipta, I. S. & Subarnas, A. Interprofessional collaboration in the breast cancer unit: How do healthcare workers see it? BMC Women’s Health 22, 227. (2022). https://doi.org/10.1186/s12905-022-01818-7
Cadet, T., Davis, C., Elks, J. & Wilson, P. A holistic model of care to support those living with and beyond cancer. Healthcare (Basel Switzerland) 4, 88. https://doi.org/10.3390/healthcare4040088 (2016).
Kwame, A. & Petrucka, P. M. A literature-based study of patient-centered care and communication in nurse-patient interactions: Barriers, facilitators, and the way forward. BMC Nurs.20, 158. https://doi.org/10.1186/s12912-021-00684-2 (2021).
Krishnasamy, M., Hyatt, A., Chung, H., Gough, K. & Fitch, M. Refocusing cancer supportive care: A framework for integrated cancer care. Support Care Cancer 31, 14. https://doi.org/10.1007/s00520-022-07501-9 (2023).
Charalambous, A. & Adamakidou, T. Construction and validation of the quality of oncology nursing care scale (QONCS). BMC Nurs. 13, 1–10. https://doi.org/10.1186/s12912-014-0048-4 (2014).
Vardy, J. & Tannock, I. F. Quality of cancer care. Ann. Oncol. 15, 1001–1006. https://doi.org/10.1093/annonc/mdh275 (2004).
Wandelt, M. A. & Ager, J. W. Quality patient care scale. Am. J. Nurs. 76, 149 (1976).
Mystakidou, K. et al. The palliative care quality of life instrument (PQLI) in terminal cancer patients. Health Qual. Life Outcomes 2, 8. https://doi.org/10.1186/1477-7525-2-8 (2004).
Simard S, Savard J & Ivers H. Fear of cancer recurrence: Specific profiles and nature of intrusive thoughts. J Cancer Surviv. 4, 361–371. https://doi.org/10.1007/s11764-010-0136-8 (2010).
van der Velden, N. C. et al. The effect of prognostic communication on patient outcomes in palliative cancer care: A systematic review. Curr. Treat. Options Oncol. 21, 1–38 (2020).
Lu, W. Examining the effects of empathy and dialogic risk communication in physicians’ text-based messages on patient satisfaction and compliance in Chinese online medical consultations (2024).
World Health Organization. Process of translation and adaptation of instruments. https://www.who.int/substance_abuse/research_tools/translation/en (2015).
Tabachnic, B. & Fidell, L. S. Using Multivariate Statistics (Allyn and Bacon, 2000).
Lynn, M. R. Determination and quantification of content validity. Nurs. Res. 35, 382–386 (1986).
Polit, D. F. & Beck, C. T. The content validity index: Are you sure you know what’s being reported? Critique and recommendations. Res. Nurs. Health 29, 489–497. https://doi.org/10.1002/nur.20147 (2006).
Ware, J. E. Jr & Gandek, B. Methods for testing data quality, scaling assumptions, and reliability: The IQOLA project approach. J. Clin. Epidemiol. 51, 945–952. https://doi.org/10.1016/s0895-4356(98)00085-7 (1998).
Im, M. & Oh, J. The development and validation of a perceived nursing support scale for mothers of preterm infants. Asian Nurs. Res. 15, 317–326. https://doi.org/10.1016/j.anr.2021.10.002 (2021).
Hinshaw, A. S. & Atwood, J. R. A patient satisfaction instrument: Precision by replication. Nurs. Res. 31, 170–191 (1982).
Yang, I. S. Individualized care, satisfaction with nursing care and health-related quality of life-focusing on heart disease. Korean J. Women Health Nurs. 9, 37–56 (2008).
Soriano, G. P. & Calong, K. A. C. Psychometric evaluation of Filipino version of patient satisfaction instrument. Belitung Nurs. J.5, 251–256. https://doi.org/10.33546/bnj.867 (2019).
Fátima Levandovski, P., Dias da Silva Lima, M. A. & Marques Acosta, A. Patient satisfaction with nursing care in an emergency service. Invest. Educ. Enferm. 33, 473–481. https://doi.org/10.17533/udea.iee.v33n3a11 (2015).
Ferede, A. J. et al. Patients’ perceptions of caring behaviors at referral hospitals in Ethiopia: A cross-sectional survey. Int. J. Nurs. Sci. 10, 391–397. https://doi.org/10.1016/j.ijnss.2023.06.015 (2023).
Kaiser, H. F. An index of factorial simplicity. Psychometrika 39, 31–36. https://doi.org/10.1007/BF02291575 (1974).
Gomes, P. et al. Cross-cultural validation of the Portuguese version of the quality of oncology nursing care scale. Cancers 16 (5), 859. https://doi.org/10.3390/cancers16050859 (2024).
Liu, Q. et al. The Chinese version of the palliative nursing care quality scale: Translation, cross-cultural adaptation, and validity. J. Palliat. Care 39 (1), 47–57. https://doi.org/10.1177/08258597231204593 (2024).
Sharour, L. A., Sabei, A., Al Harrasi, S., Anwar, M., Salameh, A. B. & S., & Translation and validation of the Arabic version of the quality of oncology nursing care scale (QONCS): Psychometric testing in three Arabic countries. J. Healthc. Qual. Res.36 (1), 34–41. https://doi.org/10.1016/j.jhqr.2020.07.004 (2021).
Choi, E. et al. Supportive care needs and health-related quality of life of esophageal cancer survivors. Asia-Pac. J. Oncol. Nurs. 8 (2), 164–171. https://doi.org/10.4103/apjon.apjon_60_20 (2021).
Lee, I. et al. Physicians’ awareness of the breast cancer survivors’ unmet needs in Korea. J. Breast Cancer 24 (1), 85. https://doi.org/10.4048/jbc.2021.24.e3 (2020).
Yoo, S. H. et al. The needs for digital health and eHeath literacy of cancer patients, caregivers, and healthcare providers: A multicenter, descriptive correlational study. Eur. J. Oncol. Nurs. 70, 102581. https://doi.org/10.1016/j.ejon.2024.102581 (2024).
Oyserman, D., Coon, H. M. & Kemmelmeier, M. Rethinking individualism and collectivism: Evaluation of theoretical assumptions and meta-analyses. Psychol. Bull. 128 (1), 3 (2002).
Kim, H., Kwon, S., Jung, S. & Lee, D. The relationship between cultural Self-construal of Korean and alexithymia: A serial mediation process model of ambivalence over emotion expression and emotion suppression moderated by generation. Korean J. Cult. Soc. Issue 29 (2), 171–197. https://doi.org/10.20406/kjcs.2023.5.29.2.171 (2023).
Funding
This work was supported by the National Research Foundation of Korea(NRF) grant funded by the Korea government(MEST) (RS-2023-00272123).
Author information
Authors and Affiliations
Contributions
Hae Jeong An, Hye Young Min and Jungmin Lee conceived and designed the study. Hae Jeong An and Hye Young Min conducted the data collection. Hae Jeong An, Hye Young Min and Jungmin Lee conducted the data analysis. Hae Jeong An, Hye Young Min and Jungmin Lee interpreted the data. Hae Jeong An, Hye Young Min and Jungmin Lee wrote several drafts of the manuscript. Jungmin Lee critically reviewed the manuscript. All authors have read, revised and approved the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study was approved by the Hallym University Institutional Review Board (HIRB-2023-028). Additionally, permission was obtained from the original authors to ensure ethical compliance and the proper adaptation of the tool.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent to publish
All participants provided consent for the publication of anonymized data.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
An, H.J., Min, H.Y. & Lee, J. Adaptation of the quality of oncology nursing care scale for patients undergoing cancer treatment in South Korea. Sci Rep 15, 13652 (2025). https://doi.org/10.1038/s41598-025-98632-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-98632-6
