
Abstract
In Greek hospitals, all deaths with a positive SARS-CoV-2 test are counted as COVID-19 deaths. Our aim was to investigate whether COVID-19 was the primary cause of death, a contributing cause of death or not-related to death amongst patients who died in hospitals during the Omicron surge and were registered as COVID-19 deaths. Additionally, we aimed to analyze the factors associated with the classification of these deaths. We retrospectively re-viewed all in-hospital deaths, that were reported as COVID-19 deaths, in 7 hospitals, serving Athens, Greece, from January 1, 2022, until August 31, 2022. We retrieved clinical and laboratory data from patient records. Each death reported as COVID-19 death was characterized as: (A) death “due to” COVID-19, or (B) death “with” COVID-19. We reviewed 530 in-hospital deaths, classified as COVID-19 deaths (52.4% males; mean age 81.7 ± 11.1 years). We categorized 290 (54.7%) deaths as attributable or related to COVID-19 and in 240 (45.3%) deaths unrelated to COVID-19 In multivariable analysis The two groups differed significantly in age (83.6 ± 9.8 vs. 79.9 ± 11.8, p = 0.016), immunosuppression history (11% vs. 18.8%, p = 0.027), history of liver disease (1.4% vs. 8.4%, p = 0.047) and the presence of COVID-19 symptoms (p < 0.001). Hospital stay was greater in persons dying from non-COVID-19 related causes. Among 530 in-hospital deaths, registered as COVID-19 deaths, in seven hospitals in Athens during the Omicron wave, 240 (45.28%) were reassessed as not directly attributable to COVID-19. Accuracy in defining the cause of death during the COVID-19 pandemic is of paramount importance for surveillance and intervention purposes.
Similar content being viewed by others


Introduction
Death is the most reliable hard outcome used to assess the impact of a pandemic on public health and monitor its evolution. Researchers have mentioned an information bias related to case and mortality definitions for COVID-19, that can vary among studies and sometimes within studies1. Therefore, accuracy in defining the cause of death during a pandemic, is of paramount importance for surveillance and intervention purposes. Since the beginning of the SARS-CoV-2 pandemic, there has been an ongoing debate on the definition of the COVID-19-attributable death. The European Center for Disease Control (ECDC) uses the guidelines issued by the World Health Organization (WHO), defining for surveillance purposes as COVID-19-attributable deaths all deaths “resulting from a clinically compatible illness in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID disease (e.g., trauma)”2. In the UK, Denmark, and other countries all deaths, for which a positive SARS-CoV-2 PCR test was recorded within the 30 days prior to the date of death, were registered as COVID-19 deaths3,4,5.
In Greece, a more concise and simple definition was used, defining as COVID-19-associated death, any death occurring in a person with positive testing for SARS-CoV-2 at the time of death. Nevertheless, throughout the pandemic, none of the above definitions has been able to determine accurately who has died ‘from’ or ‘with’ COVID-19. All the above definitions served the surveillance purposes well, at least during the initial pandemic waves, including the Delta variant. Researchers from the UK reported that during the first pandemic waves, COVID-19 deaths were accurately attributed to the virus itself approximating an impressive 92-97% accuracy5. In Denmark, during the Delta wave, only an estimated 10-20% of deaths registered as COVID-19 deaths were in fact due to other, non-COVID-19-related, causes4.
However, in Greece and worldwide, the epidemiological characteristics of the pan-demic changed dramatically with the advent of the Omicron variant, in January 20226, when a sharp increase in the number of cases, and a lesser increase in admissions and deaths were recorded7. The higher infectivity8,9 and lower morbidity of the new variant, associated with lower risks of COVID-19–related hospitalization and death10,11,12, along with the high percentage of vaccination coverage of the population achieved at the time in Greece13 made plausible that a substantial percentage of hospitalized patients with comorbidities, who died with a positive test for SARS-CoV-2 and were registered as COVID-19 deaths, in fact died from other causes “with” COVID-19, and not “be-cause of” COVID-19.
Researchers have attempted to dissect the COVID-19 mortality and differentiate deaths “due to” COVID-19, where SARS-CoV-2 infection was the direct cause of death or triggered a series of events that ultimately led to death, from deaths “with” COVID-19, when the SARS-CoV-2 infection has nothing to do with the fatal outcome. These studies were based on data from death certificates, a method with limitations and potential inaccuracies14,15.
The aim of this study was to assess whether in-hospital deaths, registered as COVID-19-associated deaths, in seven tertiary-care hospitals in the greater area of Athens, Greece, during the Omicron surge, were attributed to COVID-19 or to other causes. Additionally, we aimed to analyze the factors associated with the classification of these deaths. To avoid the shortcomings of death certificates, we also examined the chart file of each patient and interviewed the caring physicians.
Methods
Study design
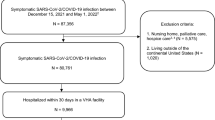
This is a retrospective observational study. Deaths registered as COVID-19-related were identified from the death certificates records of participating hospitals. In Greece, a paper copy of all death certificates issued by a hospital is kept in the hospital archives. As a parallel database, researchers used the Hellenic National Archive of COVID-19, a digital archive where physicians enter epidemiological, and clinical information, as well as out-comes for patients treated in hospitals for COVID-19. All patients, who died in the participating hospitals between 1st January 2022 and 31st August 2022, with COVID-19 being mentioned on their death certificate, and consequently registered as COVID-19 death, were included in the study. This study has received ethical approval from the Ethical Review Boards of participating hospitals. Informed consent was waived as the data was anonymized when included in the database for analysis and no risk or harm would come to participants. All methods used for this study were performed in accordance with institutional and national guidelines and in accordance with the Declaration of Helsinki regarding medical research. This article is a revised and expanded version of a paper entitled “Deaths of and with COVID-19 during the Omicron surge in seven tertiary care hospitals, Athens, Greece”, which was presented at the 33rd European Congress of Clinical Microbiology and Infectious Diseases, Copenhagen, Denmark16.
Classification of recorded deaths
We categorized all study deaths into two groups: (a) deaths “due to” COVID-19, where the infection was either the direct or sole cause of death, or it triggered a sequence of events that ultimately led to death, and (b) deaths “with” COVID-19, where the death was unrelated to the infection. To classify each death, we used data from three sources: (a) the death certificate, (b) the chart file of the patient (paper and electronic files) and (c) we interviewed the caring physician with a structured questionnaire. We extracted epidemiological, clinical, and treatment data, including demographics, comorbidities, vaccination status, the reason for admission to the hospital, in-hospital transmission of SARS-CoV-2, the department where the patient was admitted, clinical signs and symptoms of COVID-19, laboratory and imaging findings attributed to COVID-19, need for supplementary oxygen, COVID-19 specific treatment (including early antiviral treatment for high-risk patients), and outcomes. We ascertained the presence of the following comorbidities: chronic obstructive pulmonary disease, diabetes, asthma, chronic kidney disease, liver disease or cirrhosis, autoimmune disorder, immunocompromised status (e.g., HIV infection, solid organ transplantation), rheumatoid arthritis, inflammatory bowel disease, ischemic heart disease, congestive heart failure, and transient ischemic attack or stroke. We also determined each person’s modified Charlson Comorbidity Index score. Then, the senior physician, who was the caring physician for the specific patient before death, reviewed the data and by answering to a structured questionnaire provided his/her opinion on the cause of death. Finally, two senior researchers, each with experience treating over 2,500 COVID-19 patients, served as independent reviewers. They carefully considered all available data, including the opinion of the attending physician and their own medical judgment, to classify each death into one of three categories, as outlined above. More specifically, we characterized a death as “due to” COVID-19 if the patient had signs, symptoms and laboratory findings of COVID-19 at the time of death, including pneumonia, confirmed by imaging findings, need for supplemental oxygen, receiving COVID-19 specific treatment, and had no other clear cause of death. For example, the in-hospital death of a patient admitted with recent-onset fever, hypoxia, a positive SARS-CoV-2 test, diffuse chest X-ray infiltrates, and a need for supplemental oxygen, who was treated with standard COVID-19 protocols but died despite treatment, was classified as a death “due to” COVID-19. As death “with” COVID-19 we characterized deaths of patients who were admitted for another reason, with no signs and symptoms attributed to COVID-19, no need for COVID-19 specific treatment, with the exception of early antiviral treatment to prevent progression in high-risk patients and had another obvious cause of death. As an example, a patient admitted for routine surgery, who tested positive for SARS-CoV-2 without showing any COVID-19 signs or symptoms, received no COVID-19 treatment, and died from a confirmed surgical complication, was classified as a death “with” COVID-19. Finally, COVID-19 was characterized as “contributing to” death, in patients with another clear cause of death but simultaneously with signs, symptoms and laboratory findings of COVID-19. This category has been incorporated into the deaths “due to” COVID-19 category, in the analysis.
Statistical analysis
Descriptive statistics are presented as counts (%) for categorical variables and as medians [25th, 75th percentile] for non-normally distributed continuous variables or as means ± standard deviation (SD) for normally distributed continuous variables. Normality of distribution was examined using the Kolmogorov–Smirnov test. Group comparisons were performed using Student’s t-test and Mann Whitney U test for normally and non-normally distributed variables respectively, chi-square for categorical variables.
Multivariable analyses were performed using binary logistic regression. All variables with a p-value < 0.1 in the univariate analysis, as well as variables that would be reasonable to be added in the model based on known literature, were included17. We did not apply multiple comparison corrections for the logistic regression model. Each variable included was selected based on biological plausibility and prior evidence of potential association with COVID-19 mortality classification. Results of the logistic regression are presented as Odds Ratios (OR), with 95% confidence intervals (CI). Statistical findings with a p-value < 0.05 were considered statistically significant. The analysis was performed using SPSS Statistics for Windows, Version 25.0 (2017, Armonk, NY, IBM Corp.).
Results
We reviewed a total of 530 in-hospital deaths, registered as COVID-19 deaths, over the study period. Demographic and clinical data are shown on Table 1. Of note, in our population, only 12 (2.3%) patients reported a previous episode of SARS-CoV-2 infection. The vast majority (95.6%) of our patient population had at least one comorbidity. After reviewing the death certificates, medical charts, and interviewing the attending physicians, we concluded that in 240 (45.3%) of the 530 reviewed cases, COVID-19 was not related to the death (deaths “with” COVID-19). In 133 (25.1%) cases, COVID-19 was determined to be the direct cause of death, while in 157 (29.6%) cases, COVID-19 was not the primary cause but contributed to the chain of events leading to death. These two latter categories combined accounted for 290 (54.7%) deaths classified as “due to” COVID-19.
In Greece, the death certificate contains two distinct categories of death causes: condi-tions that directly caused the death and conditions that contributed to death. COVID-19 has been listed as direct cause of death in 204 of the study certificates and as contributing factor in 324 death certificates. In both cases, deaths were registered officially as COVID-19 deaths. Among the 204 deaths where COVID-19 was listed as direct cause of death on the death certificate, after our evaluation only 132 (64.7%) deaths were attributed to COVID-19; in 71 deaths (34.8%) COVID-19 was not the direct cause but contributed to death, and in only one case we classified death as not related to COVID-19. On the other hand, among the 324 deaths where COVID-19 was listed on the death certificate as contributing factor, after our evaluation, one death was attributed to COVID-19, in 85 (26.2%) cases COVID-19 was not the direct cause but a contributing factor and in 239 (73.5) cases we considered COVID-19 as not related to death. Among the 240 patients dying “with” COVID, leading cause of death was bacterial sepsis/septic shock (105/240), followed by aspiration pneu-monia (63/240), acute renal failure (10/240), stroke (15/240), heart failure (19/240), and solid organ or hematological cancers (28/240). We also investigated potential variation in classification discrepancies across participating hospitals, but the differences did not reach statistical significance, although different study hospitals serve different study populations.
We then compared patients whose death was attributed or related to COVID-19 (death “due to” COVID-19) vs. patients whose deaths were classified as not related to COVID-19 (deaths “with” COVID-19), to identify risk factors for death “with” COVID-19. In univariable analysis (Table 2), patients who died “with” COVID-19, compared to those who died “from” COVID-19 were significantly more likely to be younger (mean ± SD 79.9 ± 11.8 vs. 83.6 ± 9.8, P < 0.001), to have solid organ malignancy, end-stage liver disease, to be immunosuppressed and to be infected via hospital transmission. Conversely, patients who died “due to” COVID-19, were more likely to be older, to be admitted to an infectious disease ward, to have symptoms and laboratory compatible with COVID-19, to receive supplementary oxygen, and/or COVID-19-specific treatment.
In multivariate analysis, by using binary logistic regression multivariable model, transmission of infection in the hospital, end-stage liver disease, immunosuppression and younger age were predictors that the ensuing death was “with” COVID-19 (Table 3).
Discussion
In this retrospective, observational study, we found that of 530 in-hospital deaths, who have been registered as COVID-19 deaths, in seven Greek hospitals during the Omicron wave, only 290 (54.7%) were “due” to COVID-19. The rest were found to be deaths “with” COVID-19. This is the first study based not solely on death certificates, but also on data extracted by expert physicians from the chart file of each individual patient, and on the opinion of the caring physician. We found that patients who died “with” COVID-19 were more likely to be younger, to be admitted for any other cause but COVID-19, to have had malignancy or immunosuppression, and to have been infected in the hospital. Patients who did not exhibit COVID-19-related symptoms essentially did not experience the active effects of the infection. As a result, their deaths were not considered to be directly caused by COVID-19. This suggests that the absence of symptoms may indicate a lack of significant COVID-19-related impact, even if the virus was present.
Our findings suggest that the higher number of deaths reported form Greece during the Omicron wave was reflecting the higher level of transmission of the virus in the community and not necessarily higher morbidity or attributable mortality. Similarly, because community transmission was high, a person who was admitted for a reason unrelated to COVID-19 was more likely to have had a positive antigenic test for SARS-CoV-2 on admission, or to have been infected via in-hospital transmission and the ensuing death caused by the underlying disease to be misclassified as COVID-19 death. Assessing the importance of a positive antigenic or even PCR test on admission is not as simple as it might seem. The differences in prognosis in patients being admitted with an incidental positive test as opposed to true infection have been discussed in a study from the United States, where patients admitted for true infection were more likely to receive mechanical ventilation and die, but also the CDC classification system used on admission had a sensitivity of 83% in detecting true infections18. Onder et al., in Italy also discussed in an opinion paper that using COVID-19 positivity as the sole criterion for determining causality in relation to COVID-19 would only lead to an over-estimation of COVID-19 deaths19.
Deaths of older patients, admitted to dedicated COVID-19 Units, with signs and symptoms of active COVID-19, and who received COVID-19 specific treatment were more likely to be characterized as deaths “due” to COVID-19. On the contrary, patients who died “with” COVID-19 were younger but with more severe underlying diseases, were ad-mitted to non-COVID-19 wards, and were more likely to get infected after their admission in the hospital. Obviously, as the population had experienced a rise in cases during the Omicron era, many of which were less serious than previously, a rise was also seen in the proportion of deaths that were incorrectly recorded as COVID-19 deaths rather than deaths “with” COVID-19. Therefore, the daily figures describing COVID-19 deaths might have been less accurate than during the previous pandemic waves. In our instance, not-related deaths included deaths due to other infections, cardiovascular events (stroke and heart failure), aspiration pneumonia and solid organ or hematological cancers.
We report that 240 (45.28%) of the 530 deaths registered as GOVID-19 deaths were not related to COVID-19. Several reports from national cohorts have addressed disparities regarding attributed mortality and reporting of deaths during the pandemic. A review of COVID-19 deaths in Denmark, based on death certificates registered in the Danish Causes of Death Registry showed a similar proportion of deaths “with” COVID-19, not “due to” COVID-19, since the beginning of 2022. More specifically, probability calculations based on the weekly number of deaths and the incidence of COVID-19 community transmission, showed that, by the end of week 6 in 2022, almost 40% of all deaths occurring within 30 days after a COVID-19-positive PCR test should be classified as deaths “with” COVID-19 not “due to” COVID-19. Before the emergence of the Omicron variant, this proportion ranged from 10 to 20%. As a result, the 30-day COVID-19 death count increasingly over-estimated the fatalities “due to” COVID-19. In reality, the actual number of deaths directly caused by COVID-19 has risen only slightly, even as community transmission of the Omicron variant leads to a surge in cases4. In another study from Sweden, researchers examined the concordance between COVID-19 mortality statistics derived from clinical audit and death certificates in Ostergotland county. They assessed roughly 1000 deaths recorded as attributable or related to COVID-19 infection and found that in 24% of cases, were not related to COVID-19 infection at all20. Another example of bias in COVID-19 death reporting is found in China. Starting in December 2022, the definition for COVID-19 deaths was restricted to those specifically linked to respiratory disease. This change resulted in significantly lower reported death numbers compared to the country’s earlier estimates21.
A review by JPA Ioannidis highlighted that countries in Africa were likely to underreport deaths attributed to COVID-19, whereas in countries with intensive testing and heightened awareness, deaths were more likely to be reported as COVID-19-related early in the pandemic. The review also noted that while excess death estimates provide a more reliable metric, they could still be influenced by indirect effects of the pandemic, such as missed cancer treatments22. Nevertheless, comparing reported deaths with excess mortality data can offer valuable insights into the quality of global mortality data and reveal differences between countries23. In a 2021 report, the authors commended France and Belgium for the quality of their mortality data and contrasted this with Tajikistan, where there was a significant undercount. Of particular interest was the case of Peru, where a change in the definition of cause of death regarding COVID-19 led to a dramatic improvement in data quality23. Our study has some limitations, including the absence of data on patients transferred to ICUs. Due to a relative shortage of ICU beds, younger patients with COVID-19-related complications were more likely to receive mechanical ventilation than older patients with multiple comorbidities. Consequently, not including ICU deaths may result in an under-estimation of fatalities “due to” COVID-19 rather than those “with” COVID-19. Furthermore, we did not include deaths that occurred after hospital discharge, which again could skew the results. As with the ICU deaths, not being able to record these deaths due to lack of access to death certificates and data pertaining to these deaths, could have affected our results. Another limitation is the lack of a control group, from the pre-Omicron era, as well as possible subjectivity in the assessment of cases. In our study, we included data from 7 major hospitals in Athens, Greece, reflecting accurately both the overall population of Athens but also of Greece as a whole. However, applicability to other countries should be avoided since both the healthcare system capacity and the intensity of pandemic waves differ between countries. Finally, our study covers several months at the onset of the Omicron wave. Given the emergence of newer variants, it is possible that our findings may not fully apply to subsequent strains.
On the other hand, our study was not based solely on death certificates but also on data extracted from chart files and the opinion of caring physicians, and the independent assessment of two experienced reviewers, making our classification of each death more accurate. The question of death ‘with’ or ‘due to” COVID-19 remains a central issue to understand the impact of the pandemic. This question cannot be answered with any certainty through the sole use of death certificates, particularly given their inherent limitations14. In many hospitals, junior doctors and not senior physicians can often be tasked with signing medical certificates of cause of death, without the availability of autopsies15. The different populations served in each hospital could also have determined the practices of physicians signing death certificates. For example, one of the participating hospitals has a liver, kidney and stem cell transplant units but neither cardiothoracic surgery not neurosurgery units, which might make physicians more prone to recognise infectious complications of immunosuppressants and less likely to attribute causes of death to surgical complications. Prioritizing the condition leading to death can prove difficult: it is affected by the experience of the clinician, their prior knowledge of the patient and the presence of several comorbidities that may compete or co-exist15. This reliance on physician judgement ultimately introduces potential subjectivity and differences of opinion between physicians, inter-rater variability. Performing autopsies for all deceased would have helped address this problem, but it would be unfeasible.
Conclusions
In conclusion, we found that 45,28% of the deaths registered as COVID-19 deaths, in seven hospitals in Athens Greece, were reassessed as not directly attributable to COVID-19 in our analysis, but reflected the wide transmission of the Omicron variant in the community. However, to make reliable inferences about mortality from COVID-19, we must eliminate important biases that may lead to inaccurate conclusions, based on the use of inaccurate definitions.
Data availability
Data is available at the Pergamos Repository affiliated with the National and Kapodistrian university of Athens. https://pergamos.lib.uoa.gr/uoa/dl/frontend/el/home/research/item/3429316.
References
Pan, D., Nishimura, H. & Tang, J. W. Information bias for case definitions and mortality between and within studies over time undermines our understanding of COVID-19 transmission and disease severity. Clin. Microbiol. Infect. 30(6), 700–702. https://doi.org/10.1016/j.cmi.2024.02.002 (2024).
Surveillance definitions for COVID-19. ECDC. [Online] [Cited: January 22, 2023.] https://www.ecdc.europa.eu/en/covid-19/surveillance/surveillance-definitions
Paglino, E. et al. Differences between reported COVID-19 deaths and estimated excess deaths in counties across the united States, March 2020 to February 2022. medRxiv https://doi.org/10.1101/2023.01.16.23284633
Statens Serum Institutation. Surveillance of mortality related to the COVID-19 epidemic in Denmark. Memo from the SSI on the surveillance methods applied and the interpretation of collected data. [Online] February 17, 2022. [Cited: September 15, 2024.] https://www.ssi.dk/sygdomme-beredskab-og-forskning/sygdomsovervaagning/d/overvaagning-af-doedelighed
Slater, T. A. et al. Dying ‘due to’ or ‘with’ COVID-19: A cause of death analysis in hospitalised patients. Clin. Med. (Lond). 20(5), e189–e190. https://doi.org/10.7861/clinmed.2020-0440 (2020).
Viana, R. et al. Rapid epidemic expansion of the SARS-CoV-2 Omicron variant in Southern Africa. Nature 603(7902), 679–686. https://doi.org/10.1038/s41586-022-04411-y (2022).
National Public Health Organization (NPHO). Respiratory Infections Surveillance Weekly Overview. [Online] [Cited: Sep-tember 24, 2024.] https://eody.gov.gr/en/epidemiological-statistical-data/weekly-epidemiological-reports/respiratory-infections-surveillance-weekly-overview/
Lyngse, F. P. et al. Household transmission of the SARS-CoV-2 Omicron variant in Denmark. Nat. Commun. 13(1), 5573. https://doi.org/10.1038/s41467-022-33328-3 (2022).
Klompas, M., Pandolfi, M. C., Nisar, A. B., Baker, M. A. & Rhee, C. Association of Omicron vs wild-type SARS-CoV-2 variants with hospital-Onset SARS-CoV-2 infections in a US regional hospital system. JAMA 328 (3), 296–298. https://doi.org/10.1001/jama.2022.9609 (2022).
Bhattacharyya, R. P. & Hanage, W. P. Challenges in inferring intrinsic severity of the SARS-CoV-2 Omicron variant. N Engl. J. Med. 386(7), e14. https://doi.org/10.1056/NEJMp2119682 (2022).
Ward, I. L. et al. Risk of covid-19 related deaths for SARS-CoV-2 Omicron (B.1.1.529) compared with delta (B.1.617.2): Retrospective cohort study. BMJ 378, e070695. https://doi.org/10.1136/bmj-2022-070695 (2022). Published 2022 Aug 2.
Wolter, N. et al. Early assessment of the clinical severity of the SARS-CoV-2 Omicron variant in South Africa: A data linkage study. Lancet 399(10323), 437–446. https://doi.org/10.1016/S0140-6736(22)00017-4 (2022).
Hellenic Government. COVID-19 vaccination campaign. [Online] [Cited: September 24, 2024.] https://emvolio.gov.gr/en
Pritt, B. S., Hardin, N. J., Richmond, J. A. & Shapiro, S. L. Death certification errors at an academic institution. Arch. Pathol. Lab. Med. 129(11), 1476–1479. https://doi.org/10.5858/2005-129-1476-DCEAAA (2005).
Jefferson, T., Dietrich, M., Brassey, J. & Heneghan, C. Understanding definitions and reporting of deaths attributed to COVID-19 in the UK—Evidence from FOI requests. medRxiv https://doi.org/10.1101/2022.04.28.22274344
Basoulis, D. et al. Deaths of and with COVID-19 during the Omicron Surge in Seven Tertiary Care Hospitals, Athens, Greece [paper presentation] in 33rd European Congress of Clinical Microbiology and Infectious Diseases, Copenhagen, Denmark.
Bursac, Z., Gauss, C. H., Williams, D. K. & Hosmer, D. W. Purposeful selection of variables in logistic regression. Source Code Biol. Med. 3, 17. https://doi.org/10.1186/1751-0473-3-17 (2008).
Hohl, C. M. et al. Comparing methods to classify admitted patients with SARS-CoV-2 as admitted for COVID-19 versus with incidental SARS-CoV-2: A cohort study. PLoS One. 18(9), e0291580. https://doi.org/10.1371/journal.pone.0291580 (2023).
Onder, G., Rezza, G. & Brusaferro, S. Case-Fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA 323(18), 1775–1776. https://doi.org/10.1001/jama.2020.4683 (2020).
Spreco, A., Andersson, C., Sjödahl, R. & Timpka, T. Concordance between COVID-19 mortality statistics derived from clinical audit and death certificates in Östergötland County, Sweden. Public. Health. 221, 46–49. https://doi.org/10.1016/j.puhe.2023.06.007 (2023).
Yu, V. The guardian newspaper. China changes definition of Covid deaths as cases surge. [Online] Dec. 21, [Cited: September 24, 2024.] (2022). https://amp.theguardian.com/world/2022/dec/21/china-covid-infection-surge-puts-end-of-global-emergency-in-doubt-who
Ioannidis, J. P. A. Over- and under-estimation of COVID-19 deaths. Eur. J. Epidemiol. 36(6), 581–588. https://doi.org/10.1007/s10654-021-00787-9 (2021).
Karlinsky, A. & Kobak, D. Tracking excess mortality across countries during the COVID-19 pandemic with the world mortality dataset. Elife 10, e69336. https://doi.org/10.7554/eLife.69336 (2021).
Funding
This study has received no funding.
Author information
Authors and Affiliations
Contributions
DB Data curation, Validation, Formal analysis, Investigation, Writing – original draft, KL Investigation, IP Investigation, MC Investigation, PA Investigation, PM Investigation, VR Investigation, VP Investigation, SS Investigation, VEG Investigation, MNG investigation, CM Investigation, GP investigation, TK Investigation, VP Investigation, GC Investigation, MC Investigation, AA Investigation, NVS Conceptualization, Writing – Original Draft, Supervision All authors participated in reviewing and editing the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study has received ethical approval from the Ethical Review Boards of participating hospitals, i.e. the Laiko General Hospital Scientific and Ethics Review Board, the Red Cross General Hospital Scientific and Ethics Review Board, the Evaggelismos General Hospital Scientific and Ethics Review Board, the Georgios Gennimatas General Hospital Scientific and Ethics Review Board, the Attikon General Hospital Scientific and Ethics Review Board, the Tzaneio General Hospital Scientific and Ethics Review Board and the Sotiria Chest Disease Hospital Scientific and Ethics Review Board. Informed consent was waived as the data was anonymized when included in the database for analysis and no risk or harm would come to participants.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Basoulis, D., Logioti, K., Papaodyssea, I. et al. Deaths “due to” COVID-19 and deaths “with” COVID-19 during the Omicron variant surge, among hospitalized patients in seven tertiary-care hospitals, Athens, Greece. Sci Rep 15, 13728 (2025). https://doi.org/10.1038/s41598-025-98834-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-98834-y
