
Abstract
This study aims to analyse and predict the disease burden of occupational carbon monoxide (CO) poisoning in China and provide recommendations for its prevention and treatment. Based on the global disease burden2021 data, Joinpoint 5.0.2 software and R4.4.1 software were used to calculate the annual average percentage change (AAPC), 95% CI, and predict the disease burden of occupational CO poisoning in China in the next decade. The results show a decreasing trend in age-standardised mortality rate (ASMR) and age-standardised disability-adjusted life years (ASDR) from 2000 to 2021, with male rates consistently higher than female rates. Mortality and DALYs peak in 2021 in the 25–29 age group. ARIMA modelling projections indicate a further decline in ASMR and ASDR from 2022 to 2031. The decline in disease burden is likely to be due to advances in medical technology and improved efforts to prevent occupational diseases, but it remains higher than the global average and in several SDI regions .Further actions are needed to reduce the burden of occupational CO poisoning, including increasing the coverage of hyperbaric chambers in all regions, improving the efficiency of regulation of small and medium-sized enterprises, and strengthening CO safety training, especially for young male workers in high-risk industries.
Similar content being viewed by others

Background
Carbon monoxide (CO) is a colorless, odorless gas produced by the incomplete combustion of carbon-containing organic materials1. It binds to hemoglobin to form carboxyhemoglobin, which causes hypoxia and ischemia in tissues and leads to a series of cellular injuries mediated at the cellular level2. The most common clinical manifestations of CO poisoning are nausea, dizziness, and headache, which are usually followed by neurological disorders, with Delayed Neurocognitive Syndrome (DNS) being more common3. CO poisoning is one of the leading causes of accidental poisoning globally, and can occur during prolonged exposure to low concentrations or short-term exposure to high concentrations4.There are significant differences between the two. Chronic CO poisoning may result in severe cellular and neurotoxicity due to continued exposure, whereas acute poisoning is more often characterized by direct tissue hypoxia and acute neurological injury5.There are a number of risk factors for CO poisoning, and the global burden of disease suggests that occupational injuries are currently the leading cause of CO poisoning6. In occupational workers, there is a wide range of CO exposure, such as those working in areas with heavy vehicular traffic, such as train drivers and garage operators, as well as police officers, firefighters, and kitchen workers7.Previous studies have shown that, among the types of toxins causing acute occupational poisonings in China, asphyxiating gases rank first in the number of poisonings, poisoning and deaths caused by this type of hazardous factor, and that CO accounts for the higher number of asphyxiating gases8.
No researchers have studied the current status and future trends of the burden of disease attributable to occupational CO poisoning in China. In this study, we used the latest data from the Global Burden of Disease 2021 (GBD2021) to analyze the trend of mortality and Disability-adjusted life-years (DALYs) attributable to occupational CO poisoning, as well as the forecast for the future, in order to provide a reference for the prevention and treatment of occupational CO poisoning in China.
Methods
Sources of information
The data for this study were obtained from the GBD2021 data published by the Institute for Health Metrics and Evaluation (IHME). GBD2021 is based on 100,983 data sources and estimates Years lived with disability (YLDs), Years of life lost (YLLs), Disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and regions from 1990 to 20219. In this study, CO attributable to occupational factors for people aged 15 years and older in China, the world, and different SDI regions were selected from GBD2021 database from the years of 2000–2021. The mortality rate, age-standardized mortality rate (ASMR), DALYs and age-standardized DALYs rate (ASDR) of CO poisoning attributable to occupational factors were selected from the GBD2021 database in China, the world and different social demographic index(SDI) regions.
Statistical methods
Data were visualized using R statistical software (Version 4.4.1; R Foundation for Statistical Computing, Vienna, Austria) to analyze the trend of change in the burden of disease attributable to occupational factors of CO poisoning in Chinese population aged 15 years or older. Subsequently, Joinpoint Regression Program (Version 5.0.2; National Cancer Institute, Bethesda, Maryland, USA) was used to calculate the average annual percent of change (AAPC) and its 95% CI for the period 2000–2021. If the AAPC was greater than 0, an upward trend was indicated, if the AAPC was less than 0, a downward trend was indicated, and if neither of these two conditions was met, the trend is considered to be relatively stable over the period10. The number and location of the connection points and the corresponding P-values were determined by the Monte Carlo permutation test, with the level of α = 0.0511.
Autoregressive integrated moving average (ARIMA) model was used to predict the burden of disease attributable to occupational factors for CO poisoning in China from 2022 to 2031. The Augmented Dickey-Fuller (ADF) test was conducted to examine the stationarity of the data. If the p-value was less than the significance level (α = 0.05), the null hypothesis was rejected, and the series was considered stationary. If the data were non-stationary, differencing was applied until stationarity was achieved. In this study, the ADF test yielded p-values < 0.05, indicating stationary series. Subsequently, Akaike’s Information Criterion (AIC) and Bayesian Information Criterion (BIC) were employed for parameter selection. The optimal ARIMA model parameters were automatically identified using the auto.arima() function from the forecast package, which evaluated 21 candidate models for both ASMR and ASDR. The ARIMA(0,2,1) model was selected based on the lowest AIC and BIC values (Supplementary Tables S1-S2). Residual diagnostics were performed to confirm the absence of autocorrelation (autocorrelation function, ACF, values within 95% confidence bands) and approximate normality (Q-Q plots aligning with the 45-degree line) (Supplementary Fig.S1-S2). The Ljung-Box test further verified the randomness of residuals (P > 0.05), confirming a good model fit. Finally, the ARIMA(0,2,1) model was utilized for prediction, and the forecast() function was employed to project the disease burden of CO poisoning attributable to occupational factors in China for the next decade.
Results
Changes in the burden of disease attributable to occupational factors for CO poisoning in China versus global and different SDI regions in 2000 and 2021
The ASMR for CO poisoning attributable to occupational factors in China’s total population declined from 0.273/105 in 2000 to 0.113/105 in 2021, with males declining from 0.405/105 in 2000 to 0.167/105 and females from 0.135/105 in 2000 to 0.057/105 in 2021. The ASDR value for the total population is 14.174/105 in 2000 and 6.099/105 in 2021, of which 20.429/105 for males in 2000 decreases to 8.713/105 in 2021, of which 7.584/105 for females in 2000 decreases to 3.305/105 in 2021.The national as well as the different SDI countries, the total population as well as both sexes present ASMR and ASDR values for CO poisoning attributed to occupational factors in 2021, which are lower than the corresponding values in 2000. Table 1.
Trends of disease burden of CO poisoning attributable to occupational factors in China, the world and different SDI regions, 2000–2021
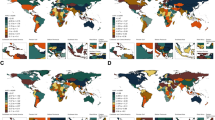
The ASMR and ASDR for occupationally attributable CO poisoning in China, globally and in different SDI regions showed a decreasing trend over time from 2000 to 2021, and the AAPC and the lower limit of the 95% CI of the ASMR and ASDR were both less than 0, which also showed an overall decreasing trend from 2000 to 2021. In China, ASMR and ASDR showed a decreasing trend for both males and females, with males having consistently higher ASMR and ASDR values than females. The ASMR and ASDR values in China and high-medium SDI regions are consistently higher than those in global and other SDI regions. Table 1; Fig. 1.

Trends in ASMR and ASDR in China, globally, in different SDI regions, and by gender in China, 2000–2021. A: Trends in ASMR in China and globally, and in different SDI regions, 2000–2021. B: Trends in ASDR in China and globally, and in different SDI regions, 2000–2021. C: Trends in ASMR in China, 2000–2021 Total. D: Trends in ASDR for total population and different genders in China, 2000–2021. ASMR: Age Standardized Mortality Rate ASDR: Age Standardized Disability Adjusted Life Years.
Changes in mortality rates and disability-adjusted life expectancy attributable to occupational factors for CO poisoning in different age groups in China in 2021
The mortality rate of CO poisoning attributable to occupational factors in the male population aged 15 and above increases and then decreases slowly with age, with the highest rate in the 25–29 age group and a significant decrease in the 55–59 age group. The mortality rate for males was consistently higher than that for females. DALYs for occupationally attributable CO poisoning in 2021 for the total population aged 15 years and older, and for both the male and female populations, show a tendency to increase and then slowly decrease with age, which is generally consistent with changes in mortality rates. Figure 2.

Age-specific changes in the burden of disease for carbon monoxide poisoning in China in 2021. A: Changes in mortality rates for the overall and sex-specific population. B: Changes in DALYs for the overall and sex-specific population.
Prediction of disease burden of CO poisoning attributable to occupational factors in China, 2022–2031
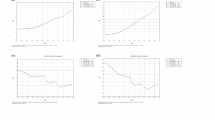
Based on the data on the disease burden of CO poisoning attributable to occupational factors from 2000 to 2021, the ARIMA model was used to predict the ASMR and ASDR of CO poisoning attributable to occupational factors in China from 2022 to 2031.The ARIMA(0,2,1) model demonstrated superior fit for both ASMR and ASDR predictions, with the lowest AIC (-181.89 for ASMR, -23.35 for ASDR) and BIC (-179.89 for ASMR, -21.36 for ASDR) among all candidates. The prediction results showed that the ASMR of CO poisoning attributable to occupational factors in China from 2022 to 2031 showed a decreasing trend from 0.109/105 in 2022 to 0.073/105 in 2031.The ASDR of CO poisoning attributable to occupational factors in China from 2022 to 2031 decreased from 0.109/105 to 0.073/105. The ASDR of CO poisoning attributable to occupational factors in China from 2022 to 2031 also shows a decreasing trend, from 5.886/105 in 2022 to 3.960/105 in 2031. Figure 3.

ARIMA model projections of ASMR and ASDR of CO poisoning attributable to occupational factors in Chinese residents, 2022–2031. A: Projections of ASMR of CO poisoning attributable to occupational factors in China, 2022–2031. B: Projections of ASDR attributable to occupational factors in China, 2022–2031.
Discussion
Occupational CO poisoning, as the most common occupational disease, represents a huge burden of disease in China and in countries around the world12. The present study thoroughly analyzed the changes in the burden of disease attributable to occupational factors of CO poisoning in China from 2000 to 2021, as well as the trend prediction. The results of this study show that the overall trend of ASMR and ASDR in China is decreasing during 2000–2021, indicating that China has made some achievements in occupational safety and health and in the treatment and prognosis of occupational diseases in the 21st century. This may be related to the fact that hyperbaric oxygen and the combination of hyperbaric oxygen with various therapeutic measures or drugs have been popularized and extensively studied in China. Hyperbaric oxygen, as an effective treatment for CO poisoning, can effectively reduce the mortality rate of CO poisoning, prevent the occurrence of delayed-onset neuropathy in CO poisoning, and improve the prognosis of patients, thus reducing DALYs13. Some studies have shown that the combination of hyperbaric oxygen with various therapeutic measures or drugs, such as adjunctive therapeutic hypothermia14, edaravone15, dexamethasone16, etc., can achieve better results than hyperbaric oxygen therapy alone.
However, compared with global data and data from different SDI regions, China has consistently high levels of ASMR and ASDR. This phenomenon may be attributed to multilevel structural differences. On the one hand, the uneven distribution of medical resources significantly affects the efficiency of treatment, which is significantly lower in western China than in eastern China17.On the other hand, it can be attributed to the weak implementation of occupational safety supervision, as China’s grass-roots health management suffers from the problems of “insufficient specialized personnel and outdated technology and equipment”, especially the general lack of occupational health managers in small, medium-sized and microenterprises, leading to insufficient monitoring of the risk of occupational exposure18.In addition, underreporting of occupational poisoning and differences in the industrial structure of different countries may lead to some differences in the severity of the disease burden.
The results of the analysis showed that the ASMR and ASDR for occupationally attributable CO poisoning were decreasing in both males and females in China, and that the burden of disease was consistently higher in males than in females, which is consistent with the results of the previous studies of occupationally attributable and non-occupationally attributable CO poisoning16.This phenomenon may be due to a combination of multiple factors. Physiologically, it has been shown that women have a better prognosis for CO poisoning than men, with a more efficient CO clearance capacity19.In terms of socio-cultural factors. Traditional gender roles may limit women’s access to high-risk jobs. In China, among workers in occupations requiring proximity to combustion sources and CO-emitting equipment, such as train drivers, miners and firefighters, men are better suited to these jobs than women in terms of strength and robustness, and thus the proportion of men is usually greater than that of women, and thus the exposure is greater than that of women20,21. In terms of occupational distribution, there may be gender segregation in occupational distribution. Although China does not officially publish sex specific data on occupational exposure, international studies have shown that high-risk industries (e.g., mining, manufacturing, transportation) are generally male-dominated, while females are more concentrated in the service sector or in low-exposure light industry22.For example, the International Labor Organization (ILO) report explicitly mentions that only about 20% of the 21.4 million jobs in the male-dominated mining industry are held by women23. The above discussion reflects the importance of gender differences in occupational safety training. Customized safety education for male workers (e.g., virtual reality simulation training) may be more effective in reducing risk.
An analysis of mortality rates and DALYs for occupationally attributable CO poisoning in different age groups over 15 years of age in China showed that both mortality and DALYs rates showed an increasing and then decreasing trend, with a peak in the 20–29 age range and a subsequent decrease, while the decreasing trend of mortality was slightly more moderate than that of DALYs, and the rates of mortality as well as DALYs for males were consistently higher than those for females. The presence of peak mortality rates in the 25–29 age group may be related to the fact that young people aged 25–29 years are more likely to be employed in high-risk occupations, such as manufacturing, construction, and mining, which often involve combustion sources and CO-emitting equipment, thereby increasing their risk of exposure to CO24. The peak occurrence of DALYs is also seen in the 25–29 age group, and the high DALYs values may reflect the severe impact of CO poisoning on the health and productivity of young people, as these populations are usually at the beginning of their careers and their early death or disability has a greater social and economic impact. The results of this study suggest that the development and implementation of more effective occupational safety and health education programs for young people in this age group should be strengthened, as well as enhanced safety regulation and preventive measures in the workplace.
In this study, we used the ARIMA (0, 2, 1) model to predict the trends of ASMR and ASDR for CO poisoning attributable to occupational factors in China over the next 10 years. The predicted results showed that the ASMR and ASDR were decreasing in the next 10 years. It shows that, since the beginning of 21st century, with the continuous progress of medical care and the amendment of the Law of the People’s Republic of China on Prevention and Control of Occupational Diseases, which was formulated according to the Constitution, not only strengthened the responsibility of enterprises, but also promoted the establishment of a monitoring system for occupational exposures, China gradually emphasized the development of occupational diseases, and made certain achievements in occupational disease prevention and control25.
This study has the following limitations. First, geographic and data coverage limitations: based on nationally aggregated data, it is not possible to parse out regional differences, and future targeted policies will need to be developed in conjunction with provincial data. Second, GBD2021 data bias: as GBD data are derived through modeling and may rely on inconsistent or incomplete local reports. In China, the occupational health surveillance system does not yet fully cover MSMEs and the informal sector, so the risk of underreporting and misclassification bias is high. Third, exposure heterogeneity is not differentiated: the GBD does not separate the difference in impacts between long-term low and short-term high exposures, and the type of exposure needs to be refined in conjunction with the Chinese Classification of Occupational Diseases (CCOD). Fourth, the model variables are missing: the ARIMA model does not incorporate exogenous variables (e.g., industrial policy adjustments), and it is suggested that the ARIMAX model be constructed by integrating enterprise emission data to improve the prediction accuracy in the future.
Conclusions
In summary, the disease burden of CO poisoning attributable to occupational factors in China showed a decreasing trend during the period 2000–2021, and it is predicted that it will still be in a decreasing trend in the next 10 years, which is inextricably linked to the improvement of the level of treatment for CO poisoning in China and the importance attached to prevention and treatment of occupational diseases. However, the disease burden for the period 2000–2021 is still higher than that of the world and different SDI regions. In order to improve this situation, we can consider increasing investment in the prevention and treatment of occupational CO poisoning, improving the coverage of hyperbaric oxygen silos in different regions, and promoting medical insurance coverage of emergency equipment. Make it mandatory for small and medium-sized enterprises to have health managers and improve regulatory efficiency. Strengthening gender and age protection, targeting the male young adult occupational group as a key group to promote sustained improvement in socio-economic status, and incorporating CO safety training into youth vocational education. These measures will help reduce the burden of occupational CO poisoning and promote the realization of the “Healthy China 2030” goal. Future research could further differentiate and analyze provincial data to identify the drivers of the CO burden gap and explore the different impacts of long-term low versus short-term high CO exposure on disease burden, as well as how to integrate multiple sources of data through more advanced models (e.g., ARIMAX or machine-learning frameworks) to improve prediction accuracy.
Data availability
The datasets analysed during the current study are available in the global disease burden 2021,[https://vizhub.healthdata.org/gbd-results/].
Abbreviations
- CO:
-
Carbon monoxide
- DNS:
-
Delayed Neurocognitive Syndrome
- GBD2021:
-
Global Burden of Disease 2021
- DALYs:
-
Disability-adjusted life years
- IHME:
-
Institute for Health Metrics and Evaluation
- YLDs:
-
Years lived with disability
- YLLs:
-
Years of life lost
- DALYs:
-
Disability-adjusted life-years
- HALE:
-
Healthy life expectancy
- ASMR:
-
Age-standardized mortality rate
- ASDR:
-
Age-standardized DALYs rate
- SDI:
-
Social demographic index
- AAPC:
-
Aaverage annual percent of change
- ARIMA:
-
Autoregressive integrated moving average
- ADF:
-
Augmented Dickey-Fuller
- ACF:
-
Autocorrelation Function
- AIC:
-
Akaike’s Information Criterion
- BIC:
-
Bayesian Information Criterion
- LCPOD:
-
Law of the People’s Republic of China on Prevention and Control of Occupational Diseases
References
Chenoweth, J. A., Albertson, T. E. & Greer, M. R. Carbon monoxide poisoning. Crit. Care Clin. 37, 657–672 (2021).
Wang, T. & Zhang, Y. Mechanisms and therapeutic targets of carbon monoxide poisoning: a focus on reactive oxygen species. Chemico-Biol. Interact., 111223 (2024).
Weaver, L. K. Carbon monoxide poisoning. Crit. Care Clin. 15, 297–317 (1999).
Thom, S. R. Vol. 347 1105–1106 (Mass Medical Soc, (2002)).
Riccardi, A., Bientinesi, P., Monteverdi, M. & Lerza, R. Chronic carbon monoxide poisoning. A report of two cases. Emerg. Care J. 17 (2021).
Moberg, M. E. et al. Global, regional, and National mortality due to unintentional carbon monoxide poisoning, 2000–2021: results from the global burden of disease study 2021. Lancet Public. Health. 8, e839–e849 (2023).
Savioli, G. et al. Carbon monoxide poisoning: from occupational health to emergency medicine. J. Clin. Med. 13, 2466 (2024).
Yuan, Y. et al. Characteristics of acute occupational poisoning cases reported in China from 2004 to 2021. Occup. Health Emerg. Rescue. 41, 37–42 (2023).
Ferrari, A. J. et al. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. Lancet 403, 2133–2161 (2024).
Wang, L. et al. Global prevalence, burden and trend in HIV and drug-susceptible tuberculosis co-infection from 1990 to 2019 and prediction to 2040. Heliyon 10 (2024).
Chen, H. S. et al. The joinpoint-jump and joinpoint-comparability ratio model for trend analysis with applications to coding changes in health statistics. J. Official Stat. 36, 49–62 (2020).
Liu, F., Jiang, X. & Zhang, M. Global burden analysis and autogluon prediction of accidental carbon monoxide poisoning by global burden of disease study 2019. Environ. Sci. Pollut. Res. 29, 6911–6928 (2022).
Liao, S. C., Shao, S. C., Yang, K. J. & Yang, C. C. Real-world effectiveness of hyperbaric oxygen therapy for delayed neuropsychiatric sequelae after carbon monoxide poisoning. Sci. Rep. 11, 19212 (2021).
Kim, S. J. et al. Effects of adjunctive therapeutic hypothermia combined with hyperbaric oxygen therapy in acute severe carbon monoxide poisoning. Crit. Care Med. 48, e706–e714 (2020).
Zeng, S. et al. Edaravone combined with hyperbaric oxygen therapy in delayed encephalopathy after acute carbon monoxide poisoning: A meta-analysis. J. Clin. Neurosci. 126, 270–283 (2024).
Xiang, W. et al. Combined application of dexamethasone and hyperbaric oxygen therapy yields better efficacy for patients with delayed encephalopathy after acute carbon monoxide poisoning. Drug. Des. Devel. Ther., 513–519 (2017).
Sun, M., Ye, Y., Zhang, G., Shang, X. & Xue, Y. Healthcare services efficiency and its intrinsic drivers in China: based on the three-stage super-efficiency SBM model. BMC Health Serv. Res. 23, 811 (2023).
Wang, Z., Liu, W. & Huang, H. -t. Implementing healthy China strategy to improve workers’ occupational health: interpretation of national occupational disease prevention and control plan (2021–2025). (2022).
Huijun, H. et al. Sex differences May affect the severity of poisoning and prognosis after carbon monoxide poisoning: a retrospective study. Undersea Hyperbaric Med. 43 (2016).
Xue, J. et al. Features of carbon monoxide poisoning in China. Iran. J. Public. Health. 42, 1192 (2013).
Cui, P. et al. Burden of carbon monoxide poisoning in China, 1990–2019: A systematic analysis of data from the global burden of disease study 2019. Front. Public. Health. 10, 930784 (2022).
Eng, A. et al. Gender differences in occupational exposure patterns. Occup. Environ. Med. 68, 888–894 (2011).
International Labour Organization. (n.d.). Mining (coal; other mining) sector. ILO. https://www.ilo.org/fr/secteurs-et-industries/industrie-miniere-charbon-autres-mineraux (Accessed: 26 March 2025).
Sancini, A. et al. Urban pollution. Giornale Italiano Di Med. Del. Lavoro Ed. Ergonomia 34 (2012).
State Council of the People’s Republic of China. Interpretation of the National Occupational Disease Prevention Plan (2021–2025)[国家职业病防治规划(2021–2025年)解读, in Chinese]. Gov.cn. December 26. (2021). https://www.gov.cn/zhengce/2021-12/26/content_5664659.htm (Accessed: 27 March 2025).
Funding
This study was supported by Science and Technology Department of Tibet (NO.XZ202201ZY0033G).
Author information
Authors and Affiliations
Contributions
Y. X. and C.C.W. have contributed to the acquisition, conception, analysis, and interpretation of data and writing the manuscript. Y.D.,L.S. X. and Q. Z. have contributed to the conception and design of the work and writing the manuscript.L.S.X.contributed to critically revise the manuscript.Q. Z. gave detailed guidance on the repair work.All authors have approved the final draft.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
Our data are from a public research database. Since all subjects in the database were anonymous, informed consent and ethical approval were not required. All methods were carried out in accordance with relevant guidelines and regulations (declaration of Helsinki). All individuals provided written informed consent before participating in the study.
Consent for publication
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Xiao, Y., Wang, C., Du, Y. et al. Trend analysis and prediction of disease burden of occupational carbon monoxide poisoning in China based on the past two decades. Sci Rep 15, 14962 (2025). https://doi.org/10.1038/s41598-025-99887-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-99887-9
