
Abstract
In this study, we take China’s large-scale free physical examination program for people aged 65 and above as an entry point and use data from the China Health and Retirement Longitudinal Study (CHARLS) between 2011 and 2018 to construct a staggered difference-in-differences (DID) model to examine whether the free physical examination program affected elderly individuals’ health care expenditures. We find that the program increased the probability of attending a physical examination by 4.3%, reduced overall medical expenditures by 28.4%, and reduced hospitalization costs by 22.1% for persons over 65 years of age but did not have a significant effect on outpatient expenditures. The program produces results through two mechanisms: disease prevention and disease screening. The program is more effective in reducing medical expenses for older adults who live in rural areas, are younger, have lower educational levels, and have chronic illnesses. The benefits of the program’s implementation far outweigh its costs.
Similar content being viewed by others

Introduction
With increasing life expectancy and decreasing birth and mortality rates, population aging has become a global trend (Ye et al., 2022; Maestas et al., 2023). Compared with other developing countries, China’s population is aging at a faster rate (Ding et al., 2023). At the end of 2022, China’s elderly population (aged 60 years and over) already exceeded 280 million, accounting for 19.8% of the total populationFootnote 1. Moreover, the health outcomes of elderly people in China are not optimistic: more than 75% of elderly people have at least one chronic diseaseFootnote 2, and approximately 190 million elderly people developed chronic diseases in 2021Footnote 3. This situation has led to a dramatic expansion of health care expenditures in China. As shown in Fig. 1, from 2010 to 2022, China’s total health care, government medical, social medical, and individual medical expenditures show a continuous growth trend. In this context, reducing health care expenditures while ensuring health has become a pressing issue.

This figure reports China’s total health care expenditure, government health care expenditure, social health care expenditure and personal health care expenditure from 2010 to 2022Footnote
China Health Statistics Yearbook.
.To achieve the goal of ensuring health, reducing health care expenditures for elderly people is inseparable from the important role of preventive policies. Prevention is a cost-effective health strategy. According to survey data from the World Health Organization (WHO), the ratio of investment in prevention to treatment and rescue expenditures needed to achieve the same health standard is 1:8.5:100. The Chinese government launched the basic public health service project in 2009, which targeted elderly people by requiring all localities to implement health management and a targeted free physical examination program for people over 65 years old within their jurisdictions. Since then, the plan has been rolled out in batches in various provinces and cities. The screening and prevention of diseases through physical examinations is very effective (Guthmuller et al., 2023). This policy, which has been implemented for more than ten years, is the largest free physical examination program in human history. However, it remains unclear whether it can promote elderly people’s participation in physical examinations and reduce health care expenditures. Previous studies in the medical field have provided evidence of the effectiveness of physical examinations (Lindholt and Søgaard, 2017; Kamstrup-Larsen et al., 2019), but a unified conclusion has not yet been reached.
The present study considered this free physical examination program as a quasiexperiment. Based on data from the China Health and Retirement Longitudinal Study (CHARLS) between 2011 and 2018 and the time difference in the development of free physical examination programs by prefecture-level cities, a staggered difference-in-differences (DID) model was established to identify the effect of the free physical examination program on elderly people’s participation in physical examinations and medical expenditures. On this basis, we conducted an in-depth analysis of the mechanism by which the free physical examination program affects the inpatient expenditures of elderly individuals. In addition, the possible influence of heterogeneity in the free physical examination program was analyzed. Finally, a rough cost‒benefit analysis of the program was conducted.
First, this study found that the program increased the probability of attending a physical examination by 4.3%, reduced overall medical expenditures by 28.4%, and reduced hospitalization costs by 22.1% for persons over 65 years of age but did not have a significant effect on outpatient expenditures. Second, the free physical examination program reduced the health care expenditures of elderly people through the two channels of early disease detection and treatment and disease prevention. Third, the free physical examination program promotes the participation in physical examinations of older persons of younger ages, older persons living in rural areas, and lower-educated older persons and reduces their medical expenditures, especially for hospitalization. The program also promotes participation in medical checkups regardless of whether elderly adults are chronically ill, but it only reduces the medical expenditures of older persons who are chronically ill. Fourth, a cost‒benefit analysis reveals that the expenditures of the free physical examination program are far exceeded by its benefits.
The literature has focused on the utilization rate and effectiveness of physical examinations. The health literacy of residents in developing countries is often low, and elderly people often have a reduced ability to obtain information. As a result, the utilization rate of public health services for elderly people in developing countries is low. Studies have shown that the acquisition of physical examination information may lead to unpleasant or unwanted results, which may lead to information avoidance (Sweeny et al., 2010) and may make residents unwilling to participate in physical examinations.
There is no consensus on the effectiveness of disease screening programs such as physical examinations. One view is that these programs can be helpful. For example, some studies have shown that physical examinations can reduce patients’ concerns (Boulware et al., 2006; Mehrotra and Prochazka, 2015), lower blood pressure, cholesterol, and body weight (Dyakova et al., 2016), reduce mortality (Lindholt and Søgaard, 2017), control diet (Engberg et al., 2002), and reduce costs (Cohen et al., 2008). Another viewpoint argues that disease screening programs such as physical examinations have limited effectiveness. For example, Honnekeri et al. (2016) reported that physical examinations may lead to overdiagnosis (Hackl et al., 2015); Kim et al. (2019) found that physical examination programs in South Korea did not reduce cancer mortality; Heneghan and Mahtani. (2020) showed that physical examinations are low-value medical treatments; Kypridemos et al. (2018) found that the health examination program offered by the UK healthcare delivery system was not cost effective; Kranker (2016) reported that the benefits of Georgia’s chronic disease management program were much lower than its expenses; and Iizuka et al. (2017) showed that Japan’s mandatory medical examination program was not cost effective. In addition, some studies suggest that the positive impact of disease screening programs such as medical checkups is conditional. For example, Kim et al. (2019) suggested that physical examination screening programs in Korea should be combined with further medical interventions to produce health benefits, and Iizuka et al. (2021) reported that health information does not produce health outcomes for the general population but can have significant health benefits for high-risk populations.
Another issue that is directly relevant to this study is how disease screening programs such as physical examinations can change individuals’ behavior. The key role of health information in this process has been confirmed by many studies (Iizuka et al., 2021; Kim et al., 2019). On the one hand, physical examinations and other health screening programs can lead to the development of healthy lifestyles among residents. For example, Murray et al. (1986) reported that physical examinations had a positive impact on reducing people’s risky behaviors; German et al. (1995) used a natural experimental method and showed that physical examinations positively affected the health behaviors of elderly individuals; and found that diagnostic information on hypertension significantly reduced individuals’ fat intake. On the other hand, physical exams allow for early screening of diseases, which can lead to interventions. Guthmuller et al. (2023) reported that the European OSPs program facilitated early screening of breast cancer, and Kim et al. (2019) found that individuals near the high-risk threshold for diabetes were positively affected in terms of health when they were treated early.
The contributions of this paper are as follows. First, based on a natural experimental design of a large-scale free physical examination program in China, this paper employs a staggered DID model to confirm that physical examinations reduce healthcare expenditures, especially hospitalization expenditures. This finding clarifies the debates on whether medical checkups are effective (Lindholt and Søgaard, 2017; Elder et al., 2017). Second, China’s large-scale free physical examination program for elderly individuals has been in place for more than a decade, but the literature only briefly describes it using descriptive statistics. This paper provides a powerful addition to the literature by examining the ability of this program to promote participation by elderly individuals in physical examinations and the impact of participation on health care costs. Third, this paper confirms the positive effect of access to health information on health behavior (Zhao et al., 2013; Iizuka et al., 2021; Kim et al., 2019) and provides evidence from China in this area. Building on this foundation, this paper contributes to the literature by presenting a comprehensive account of the impact of access to health information, such as medical checkups, on healthcare expenditures for older adults (Guthmuller et al., 2023; Kim et al., 2019). Finally, this paper responds to the debate about the cost-benefit of health screening programs such as physical examinations. In recent years, debates have arisen regarding the costs and benefits of preventive health policies such as physical examinations (Honnekeri et al., 2016; Iizuka et al., 2021; Kim et al., 2019; Cohen et al., 2008). In this paper, we present a cost‒benefit analysis of China’s large-scale free medical checkup program and report that the benefits far outweigh the costs. This finding can provide an empirical reference for disease prevention and health management in developing countries and for advancing health gateways.
The rest of this paper is organized as follows. The second section presents a policy introduction and research hypotheses. The third section outlines the research design. The fourth section presents the empirical results. The fifth section describes the mechanism testing and heterogeneity analysis. The sixth section provides a cost‒benefit analysis. Section VII presents the conclusion and a discussion.
Policy introduction and research hypotheses
Policy introduction
In recent years, the size of China’s elderly population has continued to expand, and China has become a moderately aging society. Chinese elderly people live long and unhealthy lives. There are approximately 190 million elderly people in China who have chronic diseases and 40 million elderly people with disabilitiesFootnote 5. As a result, the number of inpatients in China has increased from 152.71 million in 2011 to 247.26 million in 2021, an increase of 61.91%Footnote 6. This is a direct result of the increasing total health care expenditure in China.
In the provision and management of health services for elderly individuals, both the health of elderly people and the reduction in health care expenditures should be considered. Preventive health policy can play an active role in disease prevention and screening and has become a generally adopted health strategy worldwide. For example, for the early prevention and treatment of breast cancer, European countries have implemented organized screening programs (OSPs) that have produced favorable effects. Previous studies have shown that these programs promote early screening for breast cancer and effectively reduce mortality (Guthmuller et al., 2023).
In 2009, the Chinese government announced strategies to expand the reform of the medical and health system (referred to as the “new medical reform”) to the public. The main goal of this effort is to “effectively reduce the burden of residents’ health care expenditures and provide safe, effective, convenient and inexpensive medical and health services to the public”. As the main focus of the “new medical reform”, the national basic public health service is an important measure to promote the gradual equalization of basic public health services. The national basic public health service requires all regions to provide people over the age of 65 with one free physical examination per yearFootnote 7. As a result, free physical examination programs for elderly people have been implemented in all cities in a staggered rollout. Figure 2 shows the implementation of free physical examination programs for each city in China.

This figure of the process of implementing free physical examination programs around the city.
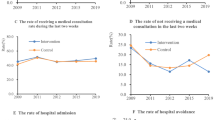
Although the physical examinations for elderly people are free, they are not mandatory, and elderly people’s participation in these examinations is voluntary. Due to the transportation and time expenditures required for elderly people to participate in physical examinations and possible ambulatory difficulties, it is unclear whether the free physical examination program can promote elderly people’s participation in physical examinations. In this study, CHARLS data were used to calculate the rates of physical examinations and free physical examinations for Chinese elderly people from 2011 to 2018, as shown in Fig. 3. The rate of physical examinations among Chinese elderly people was not stable within the sample. After a decrease in 2013, the rate increased annually. However, the rate of free physical examinations also increased significantly, which provides preliminary evidence that the free physical examination policy has had an effect.

This figure reports on the participation in physical examinations of persons over 65 years of age, both in terms of total and free physical examination ratesFootnote
Data were obtained from CHARLS.
.The free physical examination program has had a profound effect on the health care expenditures of elderly individuals. Specifically, for non-ill elderly people, the free physical examination program provides guidelines for a healthy lifestyle to achieve disease prevention. For sick elderly people, the free physical examination program can support disease prevention. The ability to screen for disease in these examinations enables early detection of diseases and early intervention in treatment. Although the free physical examination program involves the largest number of people in human history, the literature has not considered whether it can accomplish these goals.
Research hypothesis
According to the specific content of the health management service specifications for elderly individuals, the free physical examination program includes an assessment of lifestyle and health status, a physical examination, and health guidance. This paper describes how free physical examination programs can reduce the health care expenditures of elderly people through disease screening and prevention.
First, the free physical examination program affects the health care expenditures of elderly people through the prevention of diseases and reduction in the possibility of illness. Previous studies agree that healthy behavior helps to promote health (Carter et al., 2015; Ding et al., 2023). For example, studies have shown that participation in outdoor sports (Shi et al., 2023), smoking cessation (Carter et al., 2015), participation in social activities (Ding et al., 2023), maintaining adequate sleep (Castiglione‐Fontanellaz et al., 2023) and other good lifestyle habits improve health and reduce health care expenditures. The free physical examination program helps elderly people develop a healthy lifestyle by evaluating their lifestyle and discouraging negative habits such as smoking and alcohol consumption. Elderly people are encouraged to develop a healthy lifestyle, which can reduce the possibility of illness and health care expenditures. In addition, free physical examination programs enable elderly people to access their health information, which can change their decision-making processes (Golman et al., 2017). The acquisition of health information improves the health care outcomes of elderly individuals, which can further improve their level of health and reduce health care expenditures.
Second, the free physical examination program influences the health care expenditures of elderly people through early disease detection and treatment. On the one hand, the free physical examination program can provide disease screening (Guthmuller et al., 2023). The results of these physical examinations are recorded in health files and provided to examiners so that elderly people can accurately understand their physical conditions. Furthermore, after diseases are screened, early intervention treatments can be implemented to reduce health care expenditures. For example, Bodenheimer et al. (2002) reported that early intervention and treatment as a result of regular disease screening, such as measuring blood pressure and blood glucose levels, can reduce medical and health expenditures. Boone et al. (2023) reported that a preventive health policy reduced mortality and improved the health of high-risk patients with chronic diseases, which, in turn, can reduce health care expenditures. Based on the above analysis, the logical framework of this paper is shown in Fig. 4.

This figure reports on the mechanisms by which the free physical examination program affects medical expenses for the elderly.
Study design
Data and variable description
Data at the individual level
The individual-level data used in this paper are derived from the CHARLS, a large-scale tracking survey project initiated by Peking University that targets middle-aged and elderly people aged 45 and over. The sample included 17,000 people in 10,000 households in 150 county-level units in 28 provinces. Four phases of the CHARLS—2011, 2013, 2015 and 2018—have been released. These data cover various types of information on elderly people, including basic personal characteristics, family background, economic status, work status, health status, medical insurance, and service utilization, which meet the need for data on the health of elderly people.
First, the explained variables in the present paper included elderly people’s participation in physical examinations and medical expenditures. The question “When was your last routine physical examination?” in the CHARLS questionnaire was used to define whether elderly people participated in a physical examination (yes=1, no=0). Medical expenditures are defined as the sum of inpatient and outpatient expenditures and are logarithmic. Outpatient expenditures were measured by the question “What was the total cost of your outpatient health care expenditures in the past month?” Inpatient expenditures were measured by the question “What is the approximate total cost of your inpatient care in the past year?” A logarithmic treatment was performed in the regression process.
Second, based on the CHARLS data, we controlled for variables such as age, gender (male=1, female=0), marital status (married and cohabiting=1, otherwise=0), type of household registration (urban=1, rural=0), retirement (retired=1, otherwise=0),pension (received=1, otherwise=0), bereavement of a child (yes=1, no=0), health status (number of chronic diseases), level of education (below lower secondary=1, other=0) and the number of children at the individual levelFootnote 9. This study also controlled for variables such as household consumption and family size at the household level.
Finally, the mechanism testing is discussed. With respect to the mechanisms underlying the reduction in preventive diseases, the present study focused on three aspects: whether elderly people participate in activities, participate in exercise, and smoke or drink alcohol. To examine the early treatment of disease, we examined whether the free physical examination program can play a role in disease screening and whether it can promote the early treatment of disease.
Free physical examination program for elderly people
In 2009, the central government withdrew from national basic public health service projects. The free physical examination program for elderly people is an important part of the national basic public health service projects that targets elderly people. Cities at all levels have developed implementation plans for free physical examination programs for elderly individuals. In this study, the specific time of implementation of the free physical examination program for elderly people at each city level was obtained through a manual search of the official websites of the cities. On this basis, the free physical examination program for elderly people was considered as a natural experiment. A staggered DID model was constructed with different policy execution times to evaluate the effect of this program on elderly people’s participation in physical examinations and medical expenditures.
Data at the city level
This study controlled for variables at the city level that affected the implementation of the free physical examination program for elderly people and medical expenditures. These variables included the urban greening rate, city size and urban internet development level. Green space provides good-quality air and a livable environment that can relieve stress and promote the health of elderly people (Maller et al., 2006). In this work, the ratio of green space area to the built-up area was used to measure the level of greening. Furthermore, we measured the size of the city by the urban area, the logarithmic form of the total population at the end of the year, and the internet development level of a city in the logarithmic form of the number of broadband users. The data were sourced from the China City Statistical Yearbook. Table 1 presents the descriptive statistics of the main variables.
Identification strategy
This study investigated the effects of a large-scale free physical examination program implemented in China on elderly people’s participation in physical examinations and health care expenditures. This free program was gradually implemented in batches in prefecture-level cities and provides an excellent source of data for the present study. Based on the time the program was implemented in each city, a staggered DID model was constructed to investigate whether the program increased the possibility of elderly people participating in physical examinations and whether it reduced their health care expenditures. In accordance with Beck et al. (2010), we constructed the following regression model:
where the subscripts i, j, p, and t represent the individual, city, province, and time, respectively. Yicjpt represents whether individual i in family c in city j in province p participated in the physical examination at time t and medical expenditures. FPEPjt indicates that the free physical examination policy for elderly people is used as a dummy variable that takes the value of 1 for the relevant cities in the implementation year and subsequent years and 0 for other years. Xit is an individual and household level control variables. Zjt represents city-level control variables. \(\sum \beta _{m}ID\) represents the individual-fixed effects.\(\sum \beta _{n}Year\) represents the year-fixed effects, consisting of a series of time dummy.\(\sum \beta _{l}Province\ast Year\) represents province-by-year fixed effects, and \(\varepsilon _{icjpt}\) is a random disturbance term.
Empirical results and robustness test
Baseline regression
The paper first tests the impact of the free physical examination program on elderly people’s participation in physical examinations and medical expenditures. The relevant estimation results are reported in Table 2. After controlling for individual, household, and city-level control variables as well as individual and province-by-year fixed effects, the regression results in column (1) of Panel A show that this program increased the probability of elderly people participating in physical examinations by 4.2%. The regression results in column (2) of Panel A show that the program reduced the overall medical expenditures of the elderly by 28.4 percent, which passes the 5 percent significance level test. The regression results in column (3) of Panel A show that the program reduced the medical expenditures of the elderly by 22.1 percent. The regression results in column (4) of Panel A show that the program did not reduced inpatient expenditures for the elderly. This may be because after diseases are screened via physical examination, outpatient treatment is provided as soon as possible to avoid inpatient care and promote health and move the health window forward.
Panel B and Panel C report on the effects of the program on 60–65 year olds and 45–60 year olds, which is effectively equivalent to a placebo test. The regression results show that the program does not affect whether or not 45–60 year olds and 60–65 year olds participate in the physical examination and medical expenditures. The reason for this is that the program is targeted at people over 65 years of age, and people under 65 years of age are not its beneficiaries.
Robustness test
Parallel trend test
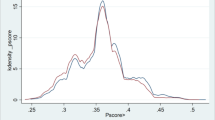
The validity of the aforementioned DID estimation results is affected by the parallel trend. On the basis of benchmark regression, we further used the event study method to test for parallel trends (Beck et al., 2010). The specific model is constructed as shown in Eq. (2), where k represents the k-th year of the implementation of the program. To avoid the problem of multicollinearity, the present study refers to the approach of Liu and Mao (2019) and takes the year before the implementation of the free physical examination program (-1) as the base period.
Figure 5 shows the estimation results of the parallel trend test. Before the implementation of the free physical examination program, there were no significant differences between the experimental group and the control group in the participation of urban elderly people in physical examinations or in medical expenditures and inpatient expenditures. The above results show that the present study can pass the pre-trend test and that the estimation result of DID in the baseline regression has certainty. Figure 5 also shows that in some years after its implementation, the probability of elderly people participating in physical examination program increased, medical expenditures and inpatient expenditures decreased.

This figure reports parallel trend tests. Among them, (a) reports the effect of the free physical examination program on whether or not an older person participates in a physical examination. b reports the impact of the free physical examination program on the medical expenses of older persons. c reports the impact of the free physical examination program on the inpatient expenses of older persons. d reports the impact of the free physical examination program on the outpatient expenses of older persons. The upper and lower bounds of the dashed lines in a-d indicate 90% confidence intervals. Solid points in the solid lines indicate the relative estimated coefficients. a–c satisfy the parallel trend test and (d) fails the parallel trend test.
Staggered did biased diagnosis
Studies have shown that the estimation results of the staggered DID model may have a problem due to the heterogeneity treatment effect (Goodman-Bacon, 2021; Baker et al., 2022)Footnote 10. Therefore, in the present study, we first diagnosed the possible heterogeneity treatment effect and then used the heterogeneity stable estimator to further ensure the robustness of the baseline regression results.
First, we diagnosed the problem of heterogeneous treatment effects. With reference to the research of De Chaisemartin and D’Haultfoeuille (2020), we diagnosed the negative weight problem. The results are shown in Table 3. The total number of weights was 2708, with 2241 treatment effects with positive weights and 467 treatment effects with negative weights. Therefore, the negative weight problem was not severe.
Second, a robustness test was performed by introducing a heterogeneity robustness estimator. Although this study did not have a serious negative weight problem, to further ensure the credibility of the benchmark regression results, a robustness test was performed using the heterogeneity robustness estimator proposed by Borusyak et al. (2021), De Chaisemartin and D’Haultfoeuille (2020), and Sun and Abraham (2021). The event study results of the heterogeneity robustness estimators are shown in Fig. A1. Before the implementation of the free physical examination program, there were no significant differences between the experimental group and the control group in terms of participation in the physical examination or medical expenditures. However, after the implementation of the program, the possibility of participating in physical examination increased significantly and the medical expenditures of elderly people in the experimental group decreased, which confirmed the robustness of the baseline regression results.
Permutation test
To exclude the influence of non-observation factors, we drew upon the research of Cantoni et al. (2017) to conduct a permutation test as follows. First, cities were randomly selected from the sample to implement the free physical examination program. A policy implementation time was then randomly assigned to the selected experimental group to form a “dummy” free physical examination policy variable, consistent with the baseline regression method. This process was repeated 1,000 times. The coefficient distribution and corresponding P values of the 1,000 estimation results as well as the estimation coefficients obtained in the baseline regression are plotted in Fig. 6. The regression coefficients of the 1,000 permutation tests were concentrated at approximately 0 and the P values of most regressions were greater than 0.1, indicating that the regression results were not significant. Therefore, the previous results have strong credibility.

This figure reports the placebo test. Among them, (a) reports a placebo test of the free physical examination program on the participation of older adults in the physical examination. b reports a placebo test of the free physical examination program on medical expenses. c reports a placebo test of the free physical examination program on inpatient expenses. Vertical dashed lines (red) in (a–c) indicate estimates from the baseline regression. Horizontal dashed line (red) indicates P=0.1. Hollow circles indicate p values and smooth curves indicate kernel density.
Excluding other policy interference
Previous studies have shown that free physical examination programs can increase the possibility of elderly people participating in physical examinations and reduce their inpatient expenditures. However, the cities involved may have implemented other health policies during the same period that may have affected elderly people’s participation in physical examinations and health care expenditures and interfered with the validity of the conclusions presented in this paper. To this end, this study attempts to rule out the interference of other health policies. Specifically, previous studies have shown that pilot long-term care insurance (Chen and Ning, 2022; Takahashi (2023)), pilot projects involving integrated medical and elder care (Yang et al., 2020) and pilot programs involving community home-based elder care services can influence the health and behavioral decisions of elderly people. Therefore, these policies were included in the regression equation. The regression results are shown in Table 4. After controlling for the influence of relevant policies, the implementation of the free physical examination program still increased the likelihood of elderly people participating in physical examinations and reduced their inpatient expenditures.
Factors affecting the implementation of the free examination program
Since it is not possible to consider all factors that influence the implementation of the free physical examination program, three main categories of factors that may influence its staggered implementation are selected. First, medical and sanitation status should be considered. Since the Chinese government does not disclose city-level medical expenditures, we can only derive city-level per capita medical expenditure (per capita medical expenditure) as a proxy variable by summing individual medical expenditures from the CHARLS survey data. In addition, this study uses the number of hospitals, the number of hospital beds, and the number of physicians per 10,000 people to measure medical and sanitation conditions. The second factor is economic development. The implementation of the free physical examination program requires a certain amount of money, and cities with a high level of economic development are likely to implement the program earlier. In this work, the logarithms of GDP per capita (lnpgdp) and population density (Density) are selected as indicators of a city’s economic development status. The third factor is the level of pollution in the city. Since pollution can have a negative impact on health, residents of cities with relatively high levels of pollution are likely to have relatively poor health, which in turn affects the implementation of free medical checkup programs. We measure the pollution status of cities in the form of the logarithm of the city’s PM2.5 emissions.
This study tested whether these variables affect the implementation of the urban free physical examination program. The regression results are shown in Appendix table A1 and reveal that only the level of economic development has a significant effect on the implementation of the urban free physical examination program, whereas the other variables have no effect on its implementation. To ensure the robustness of the regression results, we draw on Li et al. (2016) to cross-multiply the level of economic development with the year dummy variable and include it in the regression equations to control the interference of the program’s possible selectivity problem on the regression results. The regression results are shown in Appendix table A2. The free physical examination program promotes elderly people’s participation in physical examinations and reduces their medical and inpatient expenditures.
PSM-DID test
There may be nonrandomness in the implementation of the free physical examination program, which may lead to selection bias. Therefore, we used the approach of Heckman et al. (1998) and the PSM-DID approach for the robustness test. The specific operation steps were as follows. First, the control variables used in the previous text were used as matching variables. Next, matching was achieved via the nearest neighbor matching method. Again, the samples that were not in the common area were deleted. Finally, the DID method was used to perform the same operation as the baseline regression. The regression results are shown in Table 5. When matched samples were used for estimation, the free physical examination program still increased elderly people’s possibility of participating in physical examinations and reduced their medical and inpatient expenditures.
Delete the sample of municipality
The sample of municipalities directly under the Central Government is deleted. Since the administrative level of the municipalities is the same as that of the provinces, to ensure the robustness of the research conclusions, the sample of the municipalities was deleted in the present study. The regression results are shown in Table 6. The free physical examination program still increases the possibility of elderly people participating in physical examinations and reduces their medical and inpatient expenditures.
Replacement of measures of explanatory variables
To ensure the robustness of the research conclusions, this paper further uses out-of-pocket medical expenditure and out-of-pocket inpatient expenditure of the elderly on the basis of the baseline regression to conduct the robustness test. The regression results are shown in Table 7, which shows that the free physical examination program reduces the out-of-pocket medical expenditure and out-of-pocket inpatient expenditure of the elderly, which verifies the robustness of the research conclusions.
Impact of the number of freephysical examination on medical and inpatient expenditures
If a free physical examination program reduces overall medical expenditures and inpatient hospital expenditures among older adults, then it would be expected that the number of free physical examinations attended would also reduce overall medical expenditures and inpatient hospital expenditures among older adults. For this reason, this paper tests the effect of the number of free physical examinations on the overall medical expenditures and inpatient expenditures of the elderly. The regression results are shown in Table 8, and it can be found that the greater the number of free physical examinations attended, the greater the reduction in medical and inpatient expenditures of the elderly. Therefore, the findings of this paper are robust.
Mechanism examination and heterogeneity analysis
Previous studies have shown that the free physical examination program increases elderly people’s possibility of participating in physical examinations and reduces their medical expenditures. In this part of the study, the mechanism and heterogeneity in the efficacy of the free physical examination program are further explored.
Mechanism test
According to the research hypothesis above, the free physical examination program may have an impact on the health care expenditures of elderly people through two channels: disease detection and early treatment and prevention of diseases with fewer occurrences. We conducted an empirical test on these potential transmission channels.
First, we examined whether the free physical examination program affects the health care expenditures of elderly people through the mechanism of disease detection and early treatment. Specifically, previous studies have reached consensus that physical examinations can play a role in disease screening (Guthmuller et al., 2023). Therefore, we first examined whether the free physical examination program plays a role in disease screening by selecting the CHARLS question “How did you know that you have a chronic disease?” This question was assigned a value of 1 if the respondent determined that he or she had a chronic disease through a physical examination and a value of 0 if the respondent was told by other means. The regression results are shown in Column (1) of Table 9. The free physical examination program significantly increased the likelihood of elderly people learning that they had chronic diseases through physical examinations, indicating that the program provides disease screening. After a disease is screened through the free physical examination program, intervention measures can be taken as soon as possible to reduce the probability of exacerbation of the disease, thereby reducing the health care expenditures of elderly individuals. Therefore, on the basis of the question “Are you currently treating a chronic disease?” in the CHARLS, we further tested whether the screening of diseases through the free physical examination program produced the effect of early treatment. The regression results are shown in Table 9. As shown in Column (2), the free physical examination program is helpful for disease diagnosis and treatment and can provide disease discovery and early treatment, which confirms Hypothesis 1.
Second, we tested the mechanism by which the free physical examination program affects the inpatient expenditures of elderly people through the prevention of diseases and fewer occurrences. According to the specific implementation requirements of the program, it establishes health records for elderly people and promotes a healthy lifestyle by providing professional health guidance. Therefore, we examined the effects of the free physical examination program on the healthy lifestyles of elderly people. On the one hand, a healthy lifestyle is reflected in active participation in social activities and exercise. In this study, we referred to the study of Ding et al. (2023) based on the CHARLS questionnaire to examine the effect of the free physical examination program on elderly adults’ participation in activity. The regression results are shown in Table 10. The free physical examination program enabled elderly people to participate in social activities and increased the possibility that they would participate in outdoor activities.
The development of healthy behavior is a basic factor for improving the health of elderly people (Carter et al., 2015). In addition to testing the effect of the free physical examination program on elderly people’s participation in activities, we further tested the effect of the program on the development of healthy behaviors. Specifically, we examined the effects of the program on the behaviors of elderly people, such as physical exercise, smoking, and alcohol consumption. Table 11 presents the effects of the program elderly people’s participation in exercise. The program significantly promoted elderly people’s participation in moderate-intensity and light exercise, such as walking, but did not increase their participation in strenuous exercise.
Finally, the present study further tested the effects of the free physical examination program on smoking and alcohol consumption behavior. The regression results are shown in Table 12. The program reduced the probability and frequency of alcohol consumption by elderly individuals. Although it had a weak negative effect on smoking and the frequency of smoking, this effect was not significant. This may be because smoking is a long-term habit that is difficult to change.
Heterogeneity analysis
Previous studies found that the free physical examination program increased the probability of elderly people participating in physical examinations and reduced the inpatient expenditures and medical expenditures of elderly people. Therefore, does the efficacy of the free physical examination program vary according to individual characteristics? This paper conducted a heterogeneity test.
First, in response to the difference in age, the samples were divided into a younger elderly group (65–75 years old) and an advanced elderly group (over 75 years) for group regression. The regression results are shown in Table 13. The free physical examination program increased the possibility of young elderly people participating in examinations and reduced their medical and inpatient expenditures. However, for the advanced elderly group, the program did not have a positive effect. Possible reasons for this are that, first, as age accelerates the deterioration of older people’s bodily functions (Grossman, 1972), older people over the age of 75 tend to face more serious health challenges and mobility problems (Wang et al., 2024), and China’s current free physical examination program does not provide door-to-door physical examination, which may make older people over 75 unable to attend free physical examinations due to limited mobility. Second, older adults tend to experience cognitive decline as they age (Dufouil et al., 2014), which may affect their ability to make decisions about preventive health policies, resulting in lower participation rates in free physical examinations. Finally, for older adults over the age of 75, who may prioritize the management of existing conditions over participation in preventive intervention programs (Walter and Covinsky, 2001; Fried et al., 2011), the willingness to participate in free physical examinations is not as strong. To ensure the robustness of this finding, we further examined the impact of the free physical examination program on the over 80 s. The regression results are shown in Appendix table A3, and it can be found that the program similarly did not have an impact on people over 80 years of age.
Second, in China, the household registration system can be seen as a policy tool for urban residents to enjoy the right to various public services (Chen et al., 2019). In response to differences in residence and considering that elderly people living in cities are often wealthier, they may participate in physical examinations through other means. In contrast, elderly people living in rural areas tend to have low health awareness and may have a greater need for free physical examination programs. Therefore, this study tested whether the efficacy of the free physical examination program varied according to the place of residence. The regression results are shown in Table 14. The free physical examination program significantly increased the possibility of participating in physical examinations and reduced medical and inpatient expenditures for elderly people living in rural areas. However, for elderly people living in cities, the free physical examination program did not have actual effects.
Third, we considered differences in the health status of elderly people. Elderly people with chronic diseases tend to pay more attention to their health and are more active in participating in physical examinations. In addition, elderly people with chronic diseases are more likely to be hospitalized for treatment. In this study, the sample was divided into two groups with high and low health levels according to physical status to test for heterogeneity. The regression results are shown in Table 15. The free physical examination program significantly increased the possibility of participating in physical examinations and reduced medical and inpatient expenditures for elderly people with chronic diseases. However, for elderly people without chronic diseases, the free physical examination program did not have these effects.
Finally, consider that education as well as health literacy profoundly affects the utilization of disease screening programs (Kim and Han, 2016; Papadakos et al., 2018; Morimoto et al., 2022; Lange (2011)). We tested for heterogeneity based on the education level of older adults. The regression results are shown in Table 16, which reveals that the free physical examination program is effective in increasing the participation of people with lower levels of education in physical examinations as well as reducing their medical expenditures. This shows that the large-scale free medical checkup program has the effect of supporting the weak and can reduce the inequality in the utilization of medical services for the elderly to a certain extent.
Cost‒benefit analysis
The aforementioned studies consistently show that the free physical examination program can increase the likelihood of elderly people participating in physical examinations and reduce their inpatient expenditures. The influencing mechanism mainly involves the disease screening and disease prevention functions of the physical examination. However, despite the significant positive impact of this program, which is the largest free physical examination program in human history, its public expenditures are high, and an evaluation of the expenditures and benefits of the program is important. We therefore conducted a rough cost‒benefit analysis of this large-scale free physical examination program.
From the perspective of cost, in accordance with the “Notice on Doing a Good Job in 2017—National Basic Public Health Service Projects”, the per capita subsidy standard for basic public health services in 2017 increased from 45 yuan to 50 yuan. That is, the per capita expenditure for basic public health service items is approximately 50 yuan, and the physical examination program for elderly people is one of the basic public health service items. Therefore, the upper limit of expenditure for this program is approximately 50 yuan.
From the perspective of benefits, according to the aforementioned study results, the free physical examination program can reduce the inpatient expenditures of elderly people by approximately 30%. The average annual inpatient expenditures of people over 65 years old during the sample period were approximately 1924 yuan. Therefore, the program can reduce the inpatient expenditures of elderly people by approximately RMB 577. In addition, the program may have a positive effect on elderly people’s physical and mental health, and the reduction in inpatient expenditures by approximately 577 yuan is the lower bound of the benefits of the free physical examination program. Therefore, the benefits of the program far outweigh its expenditures.
Conclusions and discussion
Conclusions
In this study, the largest free physical examination program for people over 65 years old in human history was used as a natural experiment. A staggered DID model was constructed by using 2011–2018 CHARLS data and based on the time differences in the implementation of the free physical examination program by prefecture-level cities, and the effect of the free physical examination program on the participation in physical examinations and medical expenditures of elderly individuals was empirically tested. On this basis, the transmission mechanism and heterogeneity of the influence of the free physical examination program on participation in physical examinations and the health care expenditures of elderly people were analyzed. Finally, we roughly estimated the expenditures and benefits of the free physical examination program.
This paper found the following: first, the program increased the probability of attending a physical examination by 4.2%, reduced overall medical expenditures by 28.4%, and reduced hospitalization costs by 22.1% for persons over 65 years of age, but did not have a significant impact on their outpatient expenditures. This conclusion remains valid after passing a series of robustness tests. Second, the free physical examination program affected the medical expenditures of elderly people through two mechanisms: “prevention of diseases and reducing the incidence of diseases” and “disease detection and early treatment”. Third, the free physical examination program increased the possibility of participating in physical examinations and reduced the medical expenditures of elderly people living in rural areas and younger elderly people. The free physical examination program promoted the participation of physical examinations both for elderly people with chronic diseases and for elderly people without chronic diseases; however, it only reduced the medical expenditures of elderly people with chronic diseases. Fourth, a cost‒benefit analysis showed that the benefits of the free physical examination program far exceeded its expenditures.
Policy implications
Based on the findings of this paper, the following policy implications are proposed.
First, this paper finds that the free physical examination program brings significant economic benefits and can reduce individuals’ medical expenditures, especially inpatient hospitalization expenditures. Moreover, the benefits far outweigh the costs. Therefore, the coverage of the free physical examination program should be further expanded, and for China, the free physical examination program for the elderly should be fully popularized; for other developing countries, they can learn from China’s successful experience and implement a large-scale free physical examination program for high-risk populations, so as to promote the forward movement of the health gate.
Second, the free physical examination program is being promoted in a differentiated manner. The research in this paper found that the free physical examination program is only effective for those aged 65-75 years, and those aged 75 years or older may not be able to enjoy the free physical examination program due to mobility problems. Therefore, it is possible to explore physical examination programs for people over 75 years old (e.g., by implementing home-based physical examination services). In addition, this paper finds that the free physical examination program is only effective for those who live in rural areas and have a low level of education, indicating that the program has a significant effect on the weak. However, the program is not effective for those who live in urban areas and have a higher level of education, probably because they choose other programs for physical checkups. Therefore, it is necessary to actively explore how the free medical check-up program can complement other medical check-ups, so as to fully expand the coverage of the free physical examination program.
Finally, the free physical examination program should pay attention to the interface with other health policies. On the one hand, it is necessary to strengthen the linkage between the free physical examination program and the health literacy promotion program, so as to further publicize and popularize the benefits of the free physical examination program and improve the health literacy of the elderly. On the other hand, it is necessary to strengthen the linkage between the free medical check-up program and policies on post-treatment, so that early treatment can be realized after diseases are detected through the free physical examination program.
Limitations and future prospects
This study used a staggered DID model to investigate the effects of the free physical examination program on elderly people’s participation in physical examinations and health care expenditures. However, are two possible limitations. First, due to data limitations, the present study did not investigate the long-term impact of the free physical examination program on the health of elderly people. For example, whether the program can reduce the mortality rate of elderly individuals may need to be investigated over a longer period. Second, this paper discussed only the disease screening function of the free physical examination program as a whole and did not examine it from a microscopic perspective to determine whether the program has a greater effect on screening for specific diseases.
Future research can be conducted in the following two areas. First, more comprehensive and microscopic health indicators should be collected to investigate over a longer period whether the free physical examination program promotes improvements in the health of elderly individuals. In particular, future research should investigate whether the free physical examination program reduces the mortality of elderly people. Second, the screening effect of the free physical examination program on various chronic diseases should be further studied to provide a basis for the development of free screenings for specific diseases.
Data availability
Original data for this study are available in the China Health and Retirement Longitudinal Study: http://charls.pku.edu.cn/. We are unable to share this data in a public forum as we have not been granted the right to do so. Any questions about the data used in this paper can be directed to the corresponding author.
Notes
Statistical Bulletin on the Development of the Civil Service, 2022.
National Health Commission of the People’s Republic of China.
State Council’s Report on the Progress of Strengthening and Promoting Work on Elderly.
China Health Statistics Yearbook.
Opinions on Strengthening the Work on the Elderly in the New Era.
National Health Commission of the People’s Republic of China.
The free physical examination includes a general physical examination and auxiliary examination. The general physical examination includes measurement of body temperature, pulse, blood pressure, height, and weight as well as routine examination of the skin, superficial lymph nodes, heart, lungs, and abdomen in addition to a rough assessment of eyesight, hearing and movement. The auxiliary examination includes a complete blood count, routine urinalysis, fasting blood glucose, blood lipids, liver function (serum glutamic oxaloacetic transaminase, glutamic alanine aminotransferase and total bilirubin), renal function (serum creatinine and blood urea nitrogen), electrocardiogram, and ultrasound.
Data were obtained from CHARLS.
This paper controls for individual FE and Province-by-year FE, and gender and age variables are absorbed to produce realistic estimates.
Since the free physical examination program did not have a significant impact on outpatient expenditures, we do not report the impact of the program on outpatient expenditures later.
References
Baker AC, Larcker DF, Wang CCY (2022) How much should we trust staggered difference-in-differences estimates?. J. Financial Econ. 144(2):370–395
Beck T, Levine R, Levkov A (2010) Big bad banks? The winners and losers from bank deregulation in the United States. J. Financ. 65(5):1637–1667
Bodenheimer T, Lorig K, Holman H et al. (2002) Patient self-management of chronic disease in primary care. Jama 288(19):2469–2475
Boone CE, Celhay PA, Gertler P, et al. Encouraging Preventative Care to Manage Chronic Disease at Scalecccc. National Bureau of Economic Research, 2023
Borusyak K, Jaravel X, Spiess J 2021, Revisiting Event Study Designs: Robust and Efficient Estimation, CEPR Discussion Paper, No. 17247
Boulware LE, Barnes GJ, Wilson RF, et al. Value of the periodic health evaluation. Evidence report/technology assessment, 2006 (136): 1-134
Cantoni D, Chen Y, Yang DY et al. (2017) Curriculum and ideology. J. political Econ. 125(2):338–392
Carter BD, Abnet CC, Feskanich D et al. (2015) Smoking and mortality—beyond established causes. N. Engl. J. Med. 372(7):631–640
Castiglione‐Fontanellaz CEG, Schaufler S, Wild S, et al. Sleep regularity in healthy adolescents: Associations with sleep duration, sleep quality, and mental health. Journal of sleep research, 2023: e13865
Chen H, Ning J (2022) The impacts of long-term care insurance on health care utilization and expenditure: evidence from China[J]. Health Policy Plan. 37(6):717–727
Chen Y, Shi S, Tang Y (2019) Valuing the urban hukou in China: Evidence from a regression discontinuity design for housing prices[J]. J. Dev. Econ. 141:102381
Cohen JT, Neumann PJ, Weinstein MC (2008) Does preventive care save money? Health economics and the presidential candidates. N. Engl. J. Med. 358(7):661–663
De Chaisemartin C, D’Haultfoeuille X (2020) Two-way fixed effects estimators with heterogeneous treatment effects. Am. Economic Rev. 110(9):2964–2996
Ding X, Yuan L, Zhou Y (2023) Internet access and older adults’ health: Evidence from China. China Economic Rev. 82:102047
Dufouil C, Pereira E, Chêne G et al. (2014) Older age at retirement is associated with decreased risk of dementia. Eur. J. Epidemiol. 29:353–361
Dyakova M, Shantikumar S, Colquitt JL, et al. Systematic versus opportunistic risk assessment for the primary prevention of cardiovascular disease. Cochrane Database of Systematic Reviews, 2016 (1)
Elder AT, McManus IC, Patrick A et al. (2017) The value of the physical examination in clinical practice: an international survey. Clin Med 17(6):490
Engberg M, Christensen B, Karlsmose B et al. (2002) General health screenings to improve cardiovascular risk profiles: a randomized controlled trial in general practice with 5-year follow-up. J. Fam. Pract. 51(6):546–554
Fried TR, Tinetti ME, Iannone L et al. (2011) Health outcome prioritization as a tool for decision making among older persons with multiple chronic conditions. Arch. Intern. Med. 171(20):1856–1858
German PS, Burton LC, Shapiro S et al. (1995) Extended coverage for preventive services for the elderly: response and results in a demonstration population. Am. J. Public Health 85(3):379–386
Golman R, Hagmann D, Loewenstein G (2017) Information avoidance. J. economic Lit. 55(1):96–135
Goodman-Bacon A (2021) Difference-in-differences with variation in treatment timing. J. Econ. 225(2):254–277
Grossman M (1972) On the concept of health capital and the demand for health. J. Political Econ. 80(2):223–255
Guthmuller S, Carrieri V, Wübker A (2023) Effects of organized screening programs on breast cancer screening, incidence, and mortality in Europe. J. Health Econ. 92:102803
Hackl F, Halla M, Hummer M et al. (2015) The effectiveness of health screening. Health Econ. 24(8):913–935
Heckman JJ, Ichimura H, Todd P (1998) Matching As An Econometric Evaluation Estimator. Rev. Economic Stud. 65(2):261–294
Heneghan C, Mahtani KR (2020) Is it time to end general health checks?. BMJ Evid.-Based Med. 25(3):115–116
Honnekeri B, Vyas A, Lokhandwala D et al. (2016) Routine health check-ups: A boon or a burden?. Natl Med. J. India 29(1):18
Iizuka T, Nishiyama K, Chen B et al. (2021) False alarm? Estimating the marginal value of health signals. J. public Econ. 195:104368
Iizuka T, Nishiyama K, Chen B, et al. Is preventive care worth the cost? evidence from mandatory checkups in Japan. National Bureau of Economic Research, 2017
Kamstrup-Larsen N, Dalton SO, Grønbæk M et al. (2019) The effectiveness of general practice-based health checks on health behaviour and incidence on non-communicable diseases in individuals with low socioeconomic position: a randomised controlled trial in Denmark. BMJ open 9(9):e029180
Kim HB, Lee SA, Lim W (2019) Knowing is not half the battle: Impacts of information from the National Health Screening Program in Korea. J. Health Econ. 65:1–14
Kim K, Han HR (2016) Potential links between health literacy and cervical cancer screening behaviors: a systematic review. Psycho‐Oncol. 25(2):122–130
Kranker K (2016) Effects of Medicaid disease management programs on medical expenditures: evidence from a natural experiment in Georgia. J. health Econ. 46:52–69
Kypridemos C, Collins B, McHale P et al. (2018) Future cost-effectiveness and equity of the NHS Health Check cardiovascular disease prevention programme: microsimulation modelling using data from Liverpool, UK. PLoS Med. 15(5):e1002573
Lange F (2011) The role of education in complex health decisions: evidence from cancer screening. J. Health Econ. 30(1):43–54
Li P, Lu Y, Wang J (2016) Does flattening government improve economic performance? Evidence from China. J. Dev. Econ. 123:18–37
Lindholt JS, Søgaard R (2017) Population screening and intervention for vascular disease in Danish men (VIVA): a randomised controlled trial. Lancet 390(10109):2256–2265
Liu Y, Mao J (2019) How do tax incentives affect investment and productivity? Firm-level evidence from China. Am. Economic J.: Economic Policy 11(3):261–291
Maestas N, Mullen KJ, Powell D (2023) The effect of population aging on economic growth, the labor force, and productivity. Am. Economic J.: Macroecon. 15(2):306–332
Walter LC, Covinsky KE (2001) Cancer screening in elderly patients: a framework for individualized decision making. Jama 285(21):2750–2756
Maller C, Townsend M, Pryor A et al. (2006) Healthy nature healthy people:‘ contact with nature’ as an upstream health promotion intervention for populations. Health promotion Int. 21(1):45–54
Mehrotra A, Prochazka A (2015) Improving value in health care–against the annual physical. N. Engl. J. Med. 373(16):1485–1487
Morimoto A, Koh C, Yasumoto R et al. (2022) Relationship between communicative and critical health literacy, health information sources, and participation in health checkups among middle-aged Japanese community residents. Preventive Med. 161:107112
Murray DM, Luepker RV, Pirie PL et al. (1986) Systematic risk factor screening and education: a community-wide approach to prevention of coronary heart disease. Preventive Med 15(6):661–672
Papadakos JK, Hasan SM, Barnsley J et al. (2018) Health literacy and cancer self‐management behaviors: A scoping review. Cancer 124(21):4202–4210
Shi X, Shen Y, Song R (2023) Living with particles: Disclosure of pollution information, individual responses, and health consequences. J Health Econ 92:102824
Sun L, Abraham S (2021) Estimating dynamic treatment effects in event studies with heterogeneous treatment effects. J. Econ. 225(2):175–199
Sweeny K, Melnyk D, Miller W et al. (2010) Information avoidance: Who, what, when, and why. Rev. Gen. Psychol. 14(4):340–353
Takahashi M (2023) Insurance coverage, long-term care utilization, and health outcomes. Eur. J. Health Econ. 24(8):1383–1397
Wang G, Zhou Y, Zhang L et al. (2024) Prevalence and incidence of mobility limitation in Chinese older adults: evidence from the China health and retirement longitudinal study. J Nutr Health Aging 28(3):100038
Yang L, Peng H, Yang Y, et al. Situation and countermeasures of the management team of the elderly care institutions from the perspective of the combination of medical and health care: a cross-sectional study. Journal of Healthcare Engineering, 2020
Ye Z, Zou X, Post T et al. (2022) Too old to plan? Age identity and financial planning among the older population of China. China Economic Rev 73:101770
Zhao M, Konishi Y, Glewwe P (2013) Does information on health status lead to a healthier lifestyle? Evidence from China on the effect of hypertension diagnosis on food consumption. J Health Econ 32(2):367–385
Acknowledgements
This work was supported by the National Natural Science Foundation of China (grant number 72373135), the Humanity and Social Science Foundation of Ministry of Education of China (grant number 22YJAZH027).
Author information
Authors and Affiliations
Contributions
QM: Conceptualization, Data curation, Formal analysis; YZ: Funding acquisition, Investigation, Methodology; FH: Project administration; Resources; Software; HZ: Visualization; Writing-original draft; HH: Supervision; Validation.
Corresponding author
Ethics declarations
Competing interests
The authors declare that they have no conflict of interest.
Ethical approval
The data used in this study come from CHARLS. CHARLS was approved by the Ethics Committee of Peking University (IRB00001052-11015). Ethical approval for this type of study is not required by our institute.
Informed consent
In the data collection of the CHARLS (China Health and Retirement Longitudinal Study) survey, all participants signed the informed consent at the time of participation.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ma, Q., Zhang, Y., Hu, F. et al. Nip it in the bud: the impact of China’s large-scale free physical examination program on health care expenditures for elderly people. Humanit Soc Sci Commun 12, 27 (2025). https://doi.org/10.1057/s41599-024-04295-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1057/s41599-024-04295-5
This article is cited by
-
Mamba-fusion for privacy-preserving disease prediction
Scientific Reports (2025)
-
A survey and partial dependency analysis to assess residential solid waste recycling awareness in Saudi Arabia
Scientific Reports (2025)
-
Employment Status And Health Among Rural-to-Urban Migrants In China: Evidence From the China Migrants Dynamic Survey
Social Indicators Research (2025)
-
Empowering secure and sustainable healthcare through federated learning and blockchain synergies in a Medical Internet of Things
International Journal of Machine Learning and Cybernetics (2025)
-
Cyber threats in mobile healthcare applications: systematic review of enabling technologies, threat models, detection approaches, and future directions
Discover Computing (2025)
