
Abstract
Vaccine hesitancy has been attributed to policy mistakes (e.g., poor communication), individual-level perceptions of risk (i.e., safety concerns about side-effects) and to structural factors, such as the politicization of public health in many countries. Institutional distrust has also been blamed for vaccine refusal, but few studies simultaneously control for possible psychological explanations such as the need for cognition, or general curiosity. A large cross-national dataset (N = 19,037) containing a behavioral measure of respondents’ interest in facts (whereby they choose whether to confront their opinions with fact-checks), as well as psychological batteries and information about respondents’ media consumption habits is used to identify the best predictors of refusal of the vaccine against COVID. Using logistic regression models with country fixed effects, followed by country-specific analyses, we assess the relative importance of a diverse set of predictors and show that conspiracism, which captures anti-systemic views and a belief that hidden forces influence political outcomes, and distrust in government are the most prognostic indicators of vaccine refusal. Dissatisfaction with democracy also predicts vaccine refusal. Models which account for conspiracism and evaluations of democracy and the national government also indicate that news consumption via social media is associated with vaccine refusal in a subset of countries.
Similar content being viewed by others

Introduction
In the first 12 months since their administration outside of clinical trials, COVID-19 vaccines saved 13.7 to 15.9 million lives, according to scientific estimates (Watson et al., 2022). Although vaccines were viewed as a scarce but desirable public health innovation in late 2020 and much of 2021 (with accusations of “skipping the line” leveled at individuals, groups, and even countries), a different perspective soon emerged: large proportions of citizens expressed vaccine skepticism or said outright that they would not get vaccinated. As a result, countries and companies turned to vaccine mandates (Karaivanov et al., 2022), causing backlash, protests (Mello et al., 2022) and litigation (Niles, 2021). A New York Times journalist remarked about the politicization of vaccine-related policies: “You know what’s better than a vaccine mandate? A society that doesn’t need one” (Klein, 2022).
While extensive research has examined individual-level correlates of vaccine acceptance - from risk perceptions (Bennett et al., 2022; Adamus et al., 2022) and beliefs about vaccine safety (Lazarus et al., 2022) as well as sociocultural factors (Browne et al., 2015; Agarwal et al., 2021; Keselman et al., 2023; Burke et al., 2021; Paul et al., 2021), we lack systematic cross-national evidence about how political attitudes, particularly distrust in democratic institutions, shape vaccine refusal. While institutional trust has been linked to vaccine acceptance (Choi and Fox, 2022; Zheng, 2024), we are not aware of studies that simultaneously account for other psychological explanations, such as conspiracist mindsets, or for individual differences in information processing.
Our study addresses these limitations by analyzing a large cross-national dataset (N = 19,037) that allows us to examine how conspiracy thinking, distrust in government, democratic dissatisfaction and cognitive traits jointly influence vaccine refusal across diverse political contexts. Using surveys fielded simultaneously in 19 countries and incorporating both behavioral and attitudinal measures, we investigate whether psychological and political variables predict vaccine refusal in ways that transcend national boundaries. This approach enables us to identify which factors consistently predict vaccine resistance across different institutional settings, while also uncovering important cross-national variations in these relationships. We find that even the best predictors of vaccine refusal are not present in every case (for example, conspiracy thinking and trust in government are prognostic of vaccine refusal in most – but not all – countries).
Background
Vaccine refusal can be analyzed through multiple lenses. Firstly, it may be understood as the result of a personal cost-benefit analysis. In this framework, individuals weigh the protective benefits of vaccination against various personal factors (Viswanath et al., 2021, Paul et al., 2021; Burke et al., 2021). These factors might include a fear of needles or concerns about potential side effects (which may be subjectively overestimated, or muddled due to poor communication from policymakers or contradictory messages in the news media, or not well-understood by experts; Kim et al., 2024). Risk-related considerations also include perceived disease risk and immunization importance (Larson et al., 2015), some of which may be mitigated by convenience (ease of access), as well as judgments about “collective responsibility” (one of the 5 C psychological antecedents of vaccination; see Betsch et al., 2018).
One way to think of how individuals approach their subjective cost-benefit analysis is to consider how they tend to process information (“calculation” is one of the 5Cs referenced above). People with a tendency to approach the vaccination dilemma in a more analytical way, e.g., by being curious about the science behind it or inquisitive about their own knowledge on the topic, are likely to seek information to better understand what is at stake. As a result, they may end up with different vaccination decisions compared to those who have a more cognitively indifferent attitude.Footnote 1 Secondly, vaccine refusal can be interpreted as a rejection of institutional authority. This perspective views the decision not to vaccinate as a deliberate choice to disregard the recommendations of public health officials, governmental institutions, or political leaders. During the height of the COVID-19 pandemic in 2021 and 2022, these authorities made concerted appeals to citizens to engage in protective behaviors (Kritzinger et al., 2021) and to get vaccinated, and rejections of these appeals from epistemic and political authorities have been the subject of intense debate and scholarly inquiry (Stoler et al., 2022; Borga et al., 2022).
Accordingly, vaccine refusal can be symptomatic of a broader distrust in institutional authorities. Individuals who harbor deep-seated skepticism towards governmental, scientific, or medical establishments may be more inclined to reject vaccination or to endorse COVID-related misinformation (Jin et al., 2024; Uscinski et al., 2020). This systemic distrust can stem from various sources, including perceived conflicts of interest, pre-existing cynicism about democratic politics, exposure to misinformation, or other reasons. It is worth noting, however, that these perspectives are not mutually exclusive. An individual’s decision to refuse vaccination may be influenced by a complex interplay of personal risk assessment (Fridman et al., 2021), resistance to authority, and systemic distrust (or dissatisfaction with how democracy works). Understanding these multifaceted motivations is crucial for developing effective public health strategies and communication campaigns.
Summing up, explanations for vaccine refusal can thus be broadly categorized into two main areas: institutional/democratic distrust and dissatisfaction, but also differences originating in patterns of information consumption (including, as noted above, interpretative differences which may vary across individuals because of things like poor elite communication, a sense that there is no clear consensus amongst scientists, tendency to challenge oneself with reading more about the science behind the vaccine, and much more).Footnote 2 In this study, we investigate both of these dimensions.
First, to account for individual differences in how people process information, this study measures respondents’ need for cognition. The “Need for Cognition Scale" is a psychological instrument designed to assess an individual’s tendency to engage in, and derive enjoyment from, effortful cognitive activities (Cacioppo et al., 1984). The theoretical basis of this concept stems from the idea that individuals differ significantly in their intrinsic motivation to engage deeply in analytical thought processes. It explores variations in people’s desire to understand, interpret, and make sense of their experiences and environments. Essentially, individuals high in Need for Cognition are more likely to enjoy complex thinking tasks and deliberate extensively over decisions, whereas those lower in this trait may prefer simpler, less cognitively demanding approaches. For example, respondents are asked whether they “find satisfaction in deliberating long and hard for hours.” This measure helps us understand how cognitive tendencies might influence vaccine-related decision-making.
At the same time, we capture a behavioral measure of respondents’ demand for fact-checking. This latter metric provides insights into individuals’ desire for verified information and their willingness to scrutinize claims that circulate in the information ecosystem.
Second, our study quantifies the empirical relevance of the preceding mechanism (related to cognitive processes), along with and in addition to the democratic dissatisfaction and distrust mechanism. The latter is examined in several ways: first, by analyzing whether deep skepticism about contemporary politics correlates with vaccine refusal. Respondents are asked whether they agree or disagree with statements such as, “even though we live in a democracy, a few people will always run things anyway.” A strong agreement with such statements indicates a general distrust in the democratic system, which could extend to distrust in public health recommendations (Freeman et al., 2022; Van Oost et al., 2022). We also use trust in the national government and satisfaction with democracy as additional predictors.
By examining these mechanisms and incorporating the measurement of demand for fact-checking (as well as self-reported measures of news consumption), the study aims to provide a more comprehensive understanding of the factors contributing to vaccine refusal. This approach acknowledges that vaccine hesitancy is not solely a matter of information availability but also involves individual cognitive traits, attitudes towards societal institutions, and a desire for verified information.
It is important to note from the outset that, while we do not have data on the specific content individuals encountered in their information environment, we are able to measure information consumption patterns and preferences. Specifically, we analyze data on (1) time spent on social media, particularly when using these platforms as a source of news and information; (2) reliance on traditional media as primary sources of news. This approach allows us to analyze broad patterns of information consumption but does not provide insights into the exact nature of the content consumed, and we recognize that the type and quality of information individuals are exposed to can significantly influence their perspectives on vaccination and public health measures. While this restricts our ability to draw direct causal links between specific media content and vaccine attitudes, it does enable us to explore correlations between media consumption habits and vaccine acceptance or refusal.Footnote 3 Based on data from a large set of countries, these findings are critical for understanding how different media preferences might relate to vaccine hesitancy: we find, for example, that reliance on television as a news source is associated with lower rates of vaccine refusal in about half of the surveyed countries. With regard to psychological factors, we find only limited evidence that the need for cognition or demand for fact checks matter. Our most consistent results relate to the psychological and political variables: specifically, we find strong evidence that both conspiracism and mistrust in government are linked to vaccine refusal.
Research questions and expectations
Our study is motivated by two research questions: first, to what extent can differences in anti-vaccine attitudes among individuals be accounted for by interest in factual information (measured behaviorally in a non-medical context), need for cognition, and three political variables (a general conspiracy mentality, evaluations of how democracy works in the respondents’ country, and trust in government)? Second, to what extent do individual-level predictors of vaccine refusal vary across countries?
Because a large number of studies have already examined the demographic correlates of vaccination intent or status (e.g., Viswanath et al., 2021; Burke et al., 2021; Murphy et al., 2021; Borga et al., 2022; Franic, 2022, among others), we do not focus on variables such as gender, education, age, or ideology (but we do control for all these factors, and we report complete models in the Supplementary Information). Our variables of interest, as well as our expectations, are listed in this section and in the accompanying composite figure (Fig. 1), which presents the factors we consider in subsequent analysis, and summarizes the directionality of our expectations: we expect that high conspiracism, low satisfaction with democracy, low trust in government, low interest in facts, low need for cognition, limited news consumption via mainstream sources, and frequent news consumption via social media would all be associated with vaccination refusal. We briefly unpack our rationale for our choice of each one of these variables below:

Summary or the variables examined (left) and the distribution of vaccination statuses in the sample (N = 19,037; right panel).
Conspiracism
People who, in general, find conspiratorial narratives plausible are expected to be more skeptical of official health recommendations, including those relating to vaccination, due to their distrust of the medical and political establishments. We note that this plausible hypothesis should not be viewed as obvious or universal: for example, in the United States, the voice of the anti-establishment (Donald Trump) praised COVID vaccines (yet many on the ideological right were skeptical of vaccines: see Connaughton, 2021; Choi and Fox, 2022), while in Brazil (in the case of Bolsonaro) it was the incumbent president who spread skepticism about vaccines. We also note that conspiracism has been shown to be associated with believing that the threat of COVID-19 has been exaggerated (Uscinski et al., 2020), yet a belief that the virus was a bio-weapon could conceivably raise perceptions of danger or risk (which could plausibly lead to an increase in demand for protective actions).
Trust in government and satisfaction with democracy
Trust in government plays a fundamental role in vaccine acceptance. Vaccine uptake has been shown to correlate with trust in public health institutions and medical experts (Baumgaertner et al., 2018; Zheng, 2024), as well as interpersonal and government trust (Bollyky et al., 2022; Khairat et al., 2022; Krastev et al., 2023). The effectiveness of public health interventions, particularly vaccination programs, hinges critically on public trust in governmental institutions (Denemark et al., 2022). This relationship manifests in several key ways.
First, in democratic societies, health behaviors often cannot be effectively mandated without significant resistance, making voluntary compliance essential. During public health emergencies, governments must rely heavily on citizens’ willingness to follow official guidance, which in turn depends on whether citizens view government institutions and public health authorities as credible and trustworthy sources of information.Footnote 4 Second, when novel medical interventions are introduced, as was the case with COVID-19 vaccines, concerns about safety and efficacy are naturally heightened among the public. In such contexts, government recommendations are likely to be persuasive only if citizens believe that government officials are prioritizing public well-being over other considerations. As van Deth (2017) notes, trust in government is a critical factor in securing voluntary cooperation from citizens, especially for policies requiring collective action such as public health measures.
Additionally, trust in government may shape how citizens process and respond to health-related information more broadly. Those who distrust government institutions may be more likely to seek out alternative sources of information, potentially exposing themselves to misleading claims about vaccine safety or effectiveness. Conversely, citizens with higher trust in government may be more receptive to official public health messaging and more likely to accept expert consensus on vaccine safety. Based on these mechanisms, we would expect that individuals with higher trust in government would demonstrate lower rates of vaccine refusal, controlling for other factors such as political ideology, media consumption patterns, and demographic characteristics.
Beyond trust in government specifically, democratic satisfaction is expected to be a distinct predictor of vaccine acceptance. While trust captures citizens’ confidence in current government institutions and officials, satisfaction with democracy reflects a broader evaluation of how well the democratic system works in practice. Those citizens who are dissatisfied with democratic processes might be more likely to reject government-backed health initiatives, including vaccination programs. This expectation is grounded in the investigations of the relationships between populism (whose typical feature is anti-establishment rhetoric) and vaccination uptake (Recio-Román et al., 2022), as well as the scholarly work on the importance of trust in official institutions (e.g., Viskupič et al., 2022; Jin et al., 2024; Krastev et al., 2023).
Interest in factual information
Individuals who attach less importance to factual information may be more susceptible to claims suggesting that getting vaccinated is not worthwhile. These claims may include non-scientific, misleading, or anecdote-based assertions. A number of scholars have examined the relationship between information (Piltch-Loeb et al., 2021), epistemic practices (ways of acquiring and evaluating knowledge) (Rudloff et al., 2023; Vasilyeva et al., 2021; Scheitle and Corcoran, 2021), and citizens’ attitudes about COVID-19. Based on this research, we posit that a general thirst for facts could be inversely related to vaccine refusal. It is important to note, however, that our study measures interest in non-medical facts.
Need for cognition
We would expect that people with a higher need for cognition may have more faith in COVID vaccines and thus should exhibit a lower propensity to report being vaccine refusers. This is because they tend to seek out, evaluate, and rely on detailed information and evidence when forming their opinions. Given the robust scientific data supporting the efficacy and safety of COVID vaccines, individuals with a higher need for cognition are likely to be more persuaded by this information and therefore more trusting of the vaccines. (Those less inclined to critically evaluate complex scientific information about vaccines may, conversely, rely instead on simpler, potentially inaccurate sources.)
Psychological traits (Scherer et al., 2018; Viskupič and Wiltse, 2024), including cognitive styles (Murphy et al., 2021; Lindeman et al., 2022) have been linked to vaccine hesitancy, so we view need for cognition as a potential predictor, and also as a useful control variable to be used in conjunction with the remaining independent variables. That said, it is possible that analytic thinking is linked to epistemically unfounded beliefs about COVID but not to vaccination intentions, as suggested in Čavojová et al. (2024).Footnote 5
News consumption
Those who avoid mainstream news may miss out on scientifically-backed information about vaccines and public health recommendations.Footnote 6 Conversely, social media platforms can potentially expose users to more anti-vaccination content, either causing or reinforcing vaccine hesitancy. Indeed, health information is increasingly sourced from the Internet and social media, enabling claims of vaccine injury to spread and potentially mislead recipients (Van Mulukom et al., 2022, for instance, find that trust in, and reliance on, social media, especially Facebook, consistently predicted COVID-19 conspiracy beliefs, and Jin et al., 2024 also find that prevalence of conspiracy beliefs is higher among heavy users of social media; see also Piltch-Loeb et al., 2021 and Lwin et al., 2023). Cable television has been also identified as a source of vaccine hesitancy (Pinna et al., 2022).
Data and measurement
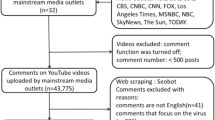
In a sample of 19,037 respondents in 19 countries (US, Brazil, and 17 countries across Europe; see Fig. 3 for the full list), attitudes toward COVID–19 vaccines were measured using the following prompt:
Some people choose to get vaccinated for COVID-19 while some others do not. How would you describe your personal situation regarding COVID–19 vaccines?
-
1.
I am fully vaccinated
-
2.
I am partially vaccinated
-
3.
I plan to get vaccinated
-
4.
I will not get vaccinated
-
5.
Prefer not to say
Data collection took place between April and May 2022,Footnote 7 a time when individuals residing in Europe or the United States already had multiple opportunities to get vaccinated, if they had chosen to do so. Our outcome variable in this paper is vaccine refusal (that is, the fourth option provided to respondents). As we show in the right panel of Fig. 1, 14.1% of respondents stated explicitly that they would not get vaccinated. Although there may be vaccine refusers among those who indicated that they plan to get vaccinated (or among those who preferred to not provide an answer), our focus is on those individuals who openly opposed getting the COVID-19 vaccine.Footnote 8
Independent variables
Our survey included psychological batteries, political items, and one behavioral measure. To tap into respondents’ need for cognition, responses were elicited with the following prompt:
Thinking about how you come to opinions and evaluations, could you indicate your agreement with the following statements (1 = completely disagree, 7 = completely agree)?
-
1.
I would prefer complex to simple problems.
-
2.
I usually end up deliberating about issues even when they do not affect me personally.
-
3.
I really enjoy a task that involves coming up with new solutions to problems.
-
4.
I prefer my life to be filled with puzzles that I must solve.
-
5.
I find satisfaction in deliberating long and hard for hours.
We calculated an additive scale using responses to the preceding 5 questions, and the scale will help us determine whether individuals who enjoy engaging in complex thought processes are more likely to accept (less likely to refuse) vaccines.Footnote 9
Our other psychological battery measured respondents’ propensity to engage in conspiratorial thinking (Uscinski et al., 2021; Enders et al., 2023). Respondents were asked to indicate whether they agreed or disagreed with the following statements, again on a 7-point scale:
-
1.
Much of our lives are being controlled by plots hatched in secret places.
-
2.
Even though we live in a democracy, a few people will always run things anyway.
-
3.
The people who really “run” the country are not known to the voters.
-
4.
Big events like wars and the outcomes of elections are controlled by small groups of people who are working in secret against the rest of us.
We use the preceding items to generate an additive scale, and we use “conspiracy thinking” or “conspiracism” interchangeably in the text to refer these anti-systemic attitudes (these four items have been proposed as a key component of the “anti-establishment orientation” in Uscinski et al., 2021).
Separately, we also measure citizens’ satisfaction with democracy using the following prompt: “On the whole, I am satisfied with the way democracy works in [country]” – a standard question used for decades in the European Social Survey and other cross-national survey projects. Responses are recorded on a 7-point scale, but we normalize all independent variables to range from zero to one (this has no bearing on our measures of variable importance, but will simplify the interpretation of marginal effects). Trust in government was also measured on a 7-point scale. Respondents were asked to what extent they agreed or disagreed with the statement: “Most of the time I can trust the government to do what is right” (1 = completely disagree, 7 = completely agree).
Our behavioral measure is participants’ interest in fact-checking (in a non-medical context). Specifically, respondents were shown multiple statements about the Russia-Ukraine conflict in the first part of the survey, and asked to indicate whether these claims about geopolitics were likely to be true or false. Later in the survey, respondents were offered a choice to read information from official sources which would confirm or debunk the previously viewed statements. The following survey prompt was used: The statements you read earlier were subject to recent fact-checks. This means a journalist or independent fact-checker investigated whether the statements were true or false. Would you like to see the fact-checks for any of these statements? Please select all the statements for which you would like to see the fact-checks. Respondents could view and read up to 10 fact-checks, regardless of their performance on the discernment task.
The average number of statements that respondents wanted to see fact-checked was 3.8 out of 10 (SD = 3.08). The lowest demand for reading fact-checks was observed in France, Belgium, and the U.S. (less than 3.4 on average) and the highest demand was recorded Denmark (Mean = 4.4), Serbia (Mean = 4.7), and Greece (Mean = 4.8). Again, this independent variable was rescaled to range from zero to one in our analyses.
Finally, we measured (self-reported) media consumption: respondents were asked whether and how frequently they used television, newspapers, and social media to get news, as well as their political orientation. The latter is important as a control, because political ideology can correlate with vaccination decisions (Albrecht, 2022; Fridman et al., 2021; Debus and Tosun, 2021). Specifically, participants were asked: “In politics, people sometimes talk of ‘left’ and ‘right.’ Where would you place yourself on this scale, where 0 means the left and 10 means the right?). The reported values were again normalized to range from zero to one, to facilitate analyses below. We also note that, in all models reported in the next section, we control for basic demographic characteristics of respondents (age, gender, and education).
Analytical strategy
To predict vaccine refusal, we first use the pooled dataset and estimate a logistic regression with vaccine refusal (response = “I will not get vaccinated [against COVID]”) and the following set of independent variables on the right-hand side of the equation: conspiracism, demand for fact-checks, satisfaction with democracy, trust in government, need for cognition, frequency of using social media to obtain news about current events, frequency of watching news on television, frequency of reading newspapers, self-reported left-right political orientation, a set of age group indicator variables, university graduation status, gender, and a set of country-level indicators (i.e., country fixed effects). We use this model to calculate predicted probabilities for counterfactual values of the predictors of interest (using the full range of potential values of each independent variable).
When calculating and plotting predicted probabilities for a given predictor, we condition on the remaining variables in the model not by setting non-focal variables at some representative value but instead calculating a set of counterfactual predictions using the following procedure: the dataset is first duplicated for each unique value of the focal term (i.e., the variable which we counterfactually consider across its full range of possible values). In each duplicate, the focal term is set to one of its unique values while all other variables remain unchanged. Predictions are then made for every observation (in all duplicates), simulating what the outcome would have been if the focal variable had that specific value. Finally, the predictions are averaged within each group defined by the unique values of the focal term, providing an estimate of the average predicted outcome for each level while accounting for the distribution of other covariates.
In subsequent analyses, we estimate logistic regressions separately for each country (using the same set of variables, except for the country indicators). Average marginal effects are reported for all focal predictors. Given that the independent variables were rescaled to range from zero to one, the values we report in Figs. 3 and 4 can be interpreted as the predicted change in the probability of refusing the vaccine for a hypothetical movement from the minimum to the maximum value of a given predictor (while conditioning on the remaining variables included in the model).
Results
Graphical results from the pooled model (using the full sample) are displayed in Fig. 2, and the numerical results are reported in the Supplementary Information. Both trust in government and conspiracism emerge as substantively important predictors of vaccine refusal. Satisfaction with democracy is a significant but weaker predictor.

Predicted probabilities of vaccine refusal (while conditioning on the remaining displayed predictors, as well as demographics).
Controlling for the remaining predictors (as well as demographic attributes: age, gender, and education, and also political ideology), we see that the expected probability of vaccine refusal is 5.1% among those who report fully trusting of government, and 14.3% among the least trusting. This amounts to an 11 percentage points (counterfactual, statistical) effect. A similar, but larger, magnitude is observed for conspiracism: there is a 16 percentage points increase in the predicted probability of refusing vaccination for a counterfactual movement from the minimum to maximum value on the conspiracy thinking scale. Satisfaction with democracy and vaccine refusal exhibit a negative relationship, though less pronounced relative to trust in government.
In contrast, the need for cognition shows only a minimal relationship with vaccine refusal (a 1.6 percentage points total statistical effect), with the predicted probabilities remaining relatively flat across different levels of this trait. Figure 2 further suggests that people who choose to read more fact checks are only slightly less likely to refuse the vaccine than those with no interest in fact checks. The bottom panel also shows that media consumption habits have modest associations with vaccine refusal, with mostly flat relationships. The confidence bands around the lines indicate that while the relationships for conspiracism, political mistrust and satisfaction with democracy are statistically significant, there is more uncertainty around the effects of media consumption and cognitive traits. We note, however, that frequent news consumption via social media is associated with a higher probability of vaccine refusal, whereas heavy consumption of news via TV or newspapers is associated with lower probabilities of refusing the vaccine.
Having reported the empirical relationships in the aggregate data, we next estimate the same specification of the model, but remove the country fixed effects, instead running the model separately for each country, and storing the estimates of these 19 models for analysis. The psychological and political predictors from these models are displayed in Fig. 3, and the relationships between media consumption variables and vaccine refusal are shown in Fig. 4.

Estimated effects of psychological and political variables on vaccine refusal.

Estimated effects of media consumption habits on vaccine refusal.
In nearly all countries, conspiracism is significantly associated with vaccine refusal (top-left panel in Fig. 3). The effect is especially pronounced in Greece, Poland, and Romania. The effect is either marginal or insignificant in Belgium, Brazil, Italy, and Denmark but positive and significant in the remaining countries. We also see a fairly consistent effect for trust in government. This country-level analysis reveals that while political factors (conspiracism, trust in government, and in some cases democratic satisfaction) are important predictors of vaccine refusal, their substantive importance varies across national contexts.
Turning to the remaining predictors, we see that need for cognition (top right panel) and demand for fact-checks (top middle panel) show weak and less consistent relationships with vaccine refusal across countries. Most confidence intervals cross zero, suggesting these cognitive factors are not reliable predictors of vaccine refusal in most national contexts. That said, in three countries (Serbia, Hungary, and the U.K.), the effect of the demand for fact checks is significant and it runs in the expected direction: those more curious about facts are less likely to be vaccine refusers. There is a significant (negative) association between the need for cognition and vaccine refusal in two countries (Poland and Romania). This underscores that mechanisms that may be operating in some countries seem to be simultaneously absent in other locations, a pattern that highlights the necessity of cross-country research about the psychology and politics of public health.
Indeed, the diverse dynamics observed in certain countries might reflect specific national contexts. For instance, in Brazil, the limited association between conspiracism and vaccine refusal could partly result from conflicting signals from political leadership during the pandemic, potentially affecting how anti-establishment attitudes translate into health behaviors. Similarly, the stronger role of fact-checking in Hungary might be connected to the prominence and public trust in national fact-checking platforms, which could enhance citizens’ willingness to verify information before making vaccination decisions.
As for the relationships between media consumption and vaccination choices, we see that the aggregate-level relationships visible in Fig. 2 mask the fact that these relationships are insignificant in most countries (Fig. 4). Overall, we see that using those types of media where mainstream (non-alternative) content is more likely to be present (i.e., television and newspapers) is either associated with a lower likelihood of vaccine refusal, or there is no effect. As for social media (a source lacking journalistic standards often held responsible for the spread of misinformation about vaccines and for reducing intentions to vaccinate against COVID-19 (Burki, 2019; Sharma et al., 2022; Allen et al., 2024), we see that in Denmark, in the Netherlands and possibly in Austria frequent use of social media for getting news is associated with a higher probability of refusing the COVID vaccine. In no country do we see an opposite relationship (i.e., nowhere is social media positively associated with vaccination). Watching news on television is associated with a lower likelihood of refusing the vaccine in a number of countries, including Greece, Austria, Poland, the Netherlands, and the U.S.
An assessment of variable importance
To better understand the relative importance of different predictors and assess which combination of variables offers especially reliable predictions of vaccine refusal, we estimated and compared multiple model specifications. Figure 5 displays the predictive performance of these models using the Area Under the Curve (AUC) metric, which ranges from 0.5 (random guessing) to 1.0 (perfect prediction). The AUC values were bootstrapped to ensure robust estimates of model performance. This comparison allows us to evaluate whether simpler models focusing on key political attitudes might perform nearly as well as more complex specifications that include demographic characteristics, psychological traits, and country-level factors (via country fixed effects).

Performance of different model specifications.
The results reveal several insights about predicting vaccine refusal. The full model that includes all variables (political variables, demographics, psychological measures, and country fixed effects) performs best, achieving an AUC of ~0.78, indicating good discriminative ability. However, simpler models that focus on political attitudes - the combination of conspiracism, trust in government, and democratic satisfaction along with media consumption - perform reasonably (AUC ≈ 0.71). This suggests these political variables capture much of the predictive signal without requiring additional complexity.
Looking at individual predictors, both trust in government alone and conspiracism alone achieve moderate predictive performance (AUC ≈ 0.64–0.66), performing substantially better than random guessing but worse than the combined models. (Media consumption patterns alone yield an AUC of between 0.62 and 0.65.) Although political variables are clearly important and prognostic, the difference between the full model and the simpler political attitudes model suggests that demographic variables and psychological traits (need for cognition, demand for fact-checks) do boost predictive power beyond what we can learn from political attitudes. (In the Supporting Information, we also estimate a logistic regression on a randomly selected (80%) sample of the data, which served as the training set, using the same set of micro-level independent variables, and also merging country-level data on corruption, inequality, and GDP per capita.)
Still, Fig. 5 suggests that predictions of vaccination decisions are not straightforward, even when several plausible predictors are known and used in statistical models. This brings up the following question: when should analysts predict that a particular person is likely to refuse a vaccine? The model at hand is, almost inevitably, conservative, because vaccine acceptance is more prevalent than refusal. When a logistic regression is estimated on the full data (N = 19,037), there are only 412 cases for which the predicted probability of being a refuser exceeded 50%. But there are 2680 actual refusers in the dataset: thus, a default classification threshold based on predicted probabilities would be extremely conservative at 50%. (To be sure, with only 14.1% of respondents stating outright that they will not get vaccinated, it is natural for the model to be highly reluctant to predict that a respondent is a vaccine refuser. In fact, it would be possible for any model to achieve nearly 86% accuracy by simply predicting “non-refuser” for all observations.)
Accuracy-maximization is thus surely not an appropriate approach in this situation: it seems appropriate, rather, to sacrifice some degree of accuracy and to improve the model’s sensitivity (its ability to identify actual refusers, or the true positive rate), and to choose the relevant threshold for the predicted probabilities accordingly, via threshold optimization. If we are willing to treat the costs of false positives and false negatives as roughly equal, we can choose the threshold to optimize the Youden index (Sensitivity + Specificity – 1). By setting the threshold to p̂ = 0.126, sensitivity of 0.78 can be achieved, along with a specificity rate of 0.64. The upshot from decreasing the cutoff point from a high value (e.g., 50%) is that the number of false negatives decreases, but inevitably the number of false positives increases as well.
Discussion: the central role of trust
The critical relationship we find between institutional trust and vaccine acceptance echoes important historical lessons about public health interventions. The devastating consequences of breaching public trust are perhaps most starkly illustrated by events in Pakistan following the revelation that a vaccination campaign had been used as cover for intelligence operations (Summers and Morrison, 2014). After this violation of trust became public in 2011, Pakistan saw a dramatic decline in vaccine acceptance, a surge in violence against health workers, and ultimately a resurgence of polio (Ohanes, 2024). This case underscores how the exploitation of public health initiatives for other purposes can severely undermine future health interventions.
However, there are also encouraging examples of how working through trusted community intermediaries can enhance public health outcomes, even in low-trust environments. During the 2014 Ebola outbreak in West Africa, for instance, transmission rates declined significantly after health authorities engaged community leaders, religious figures, and local youth representatives in their response efforts. These contrasting cases, combined with our findings about the relationship between democratic satisfaction and vaccine acceptance, suggest that public health strategies must be sensitive to existing trust relationships. Relatedly, the relationship between institutional trust and vaccine acceptance suggests that building public confidence in government institutions could be viewed as a public health investment.
In Western societies, meanwhile, both research and journalistic reporting suggest that, in alternative health communities, skepticism of mainstream medicine is seen as integral to their worldview (Sunyík et al., 2023; Attwell et al., 2018; Beres et al., 2023; Ward and Voas, 2011). These cultural attitudes need to be better understood, given that the existing research typically stops at measuring trust in certain epistemic elites (doctors, scientists, etc.), or confidence in pharmaceutical companies, but rejections of modern medical procedures can also be grounded in “epistemological doubts about the validity of scientific knowledge claims” (Aupers, 2012).
Indeed, there is evidence that skepticism of western medicine correlates with conspiracy thinking (Zilinsky and Zeitzoff, 2025) and that anti-expert attitudes correlate with endorsement of medical folk wisdom (inaccurate beliefs about disease, immunity, and other topics; see Motta and Callaghan, 2020). At the same time, trust in science correlates only weakly with the appeal to nature bias which has been measured with prompts such as “the coronavirus is harmless for those with a strong immunity” (38% of respondents in Serbia endorsed this statement; see Žeželj et al., 2023).
Conclusion
COVID-19 vaccines have significantly reduced infections and hospitalizations, but vaccine resistance persists. Our study set out to understand the predictors of vaccine refusal by analyzing a set of psychological, political, and media consumption variables across multiple countries. Our key findings are that individuals who are least trusting of government, and those with higher levels of conspiratorial thinking (a general, deeply skeptical mindset, which is a concept separate from beliefs in specific conspiracy theories) are substantially more likely to refuse vaccination. Although “dissatisfaction with the government decreases satisfaction with how democracy works” (Becher et al., 2024), we also see suggestive evidence that dissatisfaction is an independent factor, separate from trust in national governments.
The relationship between conspiracism and vaccine refusal holds consistently across most countries, with the effects being particularly pronounced in Greece, Poland, and Romania. Contrary to our expectations, our findings show that the need for cognition, while relevant in some instances, appears to have a modest impact on vaccine refusal.
Our country-specific analyses further highlight the importance of political and psychological factors in shaping vaccine attitudes – and the necessity of future work to study specific mechanisms in greater detail. For example, while the association between trust in government and lower vaccine refusal is robust across nearly all countries, the impact of other variables varies. Finally, media consumption patterns reveal that traditional media sources like television and newspapers are generally associated with lower vaccine refusal rates or have no significant effect, whereas social media use is linked to higher vaccine refusal in some countries, notably Denmark and the Netherlands. But media consumption is less prognostic than the political variables we measured, and these results are consistent with recent findings by Štětka et al. (2024) who report that preexisting attitudes in five countries (in their case particularly support for populism and distrust of experts) are generally more reliable predictors of people’s susceptibility to pandemic-related misinformation (such as beliefs that vaccines can alter DNA) than their patterns of news consumption.
The strong relationship between political trust and vaccine acceptance revealed in our study underscores a crucial insight: effective public health measures in democratic societies depend fundamentally on public confidence. While other factors certainly influence vaccine acceptance, the consistency of this relationship across multiple national contexts suggests that trust-building should be considered an essential component of public health infrastructure. Future research should further explore the mechanisms through which institutional trust shapes health behaviors and identify effective strategies for encouraging public health compliance in low-trust environments. Effective pandemic responses hinge on widespread public cooperation, but the COVID-19 pandemic exposed deep divisions and mistrust that hinder such efforts. To address this, governments and health institutions may require reform. Given the consistent relationship between trust in government and vaccine refusal across countries, restoring public trust is critical, but acknowledging and preparing for the reality of institutional distrust seems equally important. Governments should treat distrust as a public health risk, and seek to develop pandemic strategies that can succeed even in deeply divided communities.
Moreover, the clear association between conspiratorial thinking and vaccine refusal also emphasizes the challenges posed by distrust in official narratives and “the existing system”. Thus, efforts to build trust in democratic institutions may indirectly support vaccine acceptance. Public health campaigns might benefit from addressing, debunking, or pre-bunking conspiratorial narratives. Future research would ideally probe the specific mechanisms by which political dissatisfaction translates into health-related behaviors, and how these mechanisms might vary across different cultural and political contexts; in the meantime, policymakers should be aware that vaccine hesitancy is not merely a matter of information deficit but is closely tied to broader political attitudes and trust in institutions.
Data availability
Data and code used in this analysis were made available on the Open Science Framework (OSF) at the following link: https://osf.io/kwyne/.
Notes
Existing research shows searching for credible information in the news media was important for many people during the peak of the pandemic (Altay et al., 2022). Publics everywhere in the world displayed a greater appreciation of trustworthy news, with some mainstream newspapers reporting their best years in terms of subscriptions.
Future research can address this limitation by incorporating content analysis of popular media sources or by using tracking methods to capture detailed information about the specific content individuals encounter across various media platforms.
As researchers who studied cross-national differences in pandemic responses noted: “countermeasures are sensible, but they are not enough. A key lesson of the COVID-19 pandemic is that better vaccines and tests, more plentiful masks, and earlier warnings only work if people are willing to make use of them—and that willingness depends on a level of public trust that many Americans no longer have.” (Bollyky et al., 2023)
Čavojová and colleagues (2024) conclude that “analytic thinking and promoting scientific reasoning may not be sufficient in the fight against misinformation; rather, we should focus on increasing public trust in science”.
The data for this study was collected by, and made available to us, the Network of European Political Communication Scholars (NEPOCS). We are grateful to the NEPOCS network for making this study possible.
We note that vaccine accepters are over-represented in the sample, perhaps due to the well-known problem that some political opinions and attitudes correlate with willingness to participate in surveys. Nevertheless, our sampled set of respondents approximates reasonably well the main population-level demographic variables (see Supporting Information).
For summaries of our main predictors, the reader is referred to Supplementary Information.
References
Adamus M, Čavojová V, Ballová Mikušková E (2022) Fear trumps the common good: psychological antecedents of vaccination attitudes and behaviour. Acta Psychol 227:103606
Agarwal R, Dugas M, Ramaprasad J, Luo J, Li G, Gao G (2021) Socioeconomic privilege and political ideology are associated with racial disparity in COVID-19 vaccination. Proc Natl Acad Sci USA 118(33):e2107873118
Albrecht D (2022) Vaccination politics and COVID-19 impacts. BMC Public Health 22(1):96
Allen J, Duncan J, Watts DJ, Rand DG (2024) Quantifying the impact of misinformation and vaccine-skeptical content on Facebook. Science 384(6699):eadk3451
Altay S, Nielsen RK, Fletcher R (2022) Quantifying the “infodemic”: people turned to trustworthy news outlets during the 2020 coronavirus pandemic. J Quant Desc Digit Med 2
Aupers, S (2012). ‘Trust no one’: Modernization, paranoia and conspiracy culture. Eur J Commun, 27(1), 22–34
Baumgaertner B, Carlisle JE, Justwan F (2018) The influence of political ideology and trust on willingness to vaccinate. PLoS ONE 13(1):e0191728
Becher M, Longuet-Marx N, Pons V, Brouard S, Foucault M, Galasso V, Kerrouche E, León Alfonso S, Stegmueller D (2024) Government performance and democracy: survey experimental evidence from 12 Countries during COVID-19. J Politics 86:1162–1176
Bennett MM, Douglas M, da Graca B, Sanchez K, Powers MB, Warren AM (2022) Attitudes and personal beliefs about the COVID-19 vaccine among people with COVID-19: a mixed-methods analysis. BMC Public Health 22(1):1–13
Beres D, Remski M, Walker J (2023) Conspirituality: how new age conspiracy theories became a health threat. PublicAffairs
Betsch C, Schmid P, Heinemeier D, Korn L, Holtmann C, Böhm R (2018) Beyond confidence: development of a measure assessing the 5C psychological antecedents of vaccination. PloS ONE 13(12):e0208601
Bollyky TJ, Hulland EN, Barber RM, Collins JK et al. (2022) Pandemic preparedness and COVID-19: an exploratory analysis of infection and fatality rates, and contextual factors associated with preparedness in 177 countries, from Jan 1, 2020, to Sept 30, 2021. Lancet 399(10334):1489–1512
Bollyky TJ, Kickbusch I, Petersen MB (2023) The trust gap: how to fight pandemics in a divided Country. Foreign Affairs
Borga LG, Clark AE, D’ambrosio C, Lepinteur A (2022) Characteristics associated with COVID-19 vaccine hesitancy. Sci Rep 12(1):12435
Burki T (2019) Vaccine misinformation and social media. Lancet Digit Health 1(6), e258–e259
Burke PF, Masters D, Massey G (2021) Enablers and barriers to COVID-19 vaccine uptake: an international study of perceptions and intentions. Vaccine 39(36):5116–5128. https://doi.org/10.1016/j.vaccine.2021.07.056
Browne M, Thomson P, Rockloff MJ, Pennycook G (2015) Going against the Herd: psychological and cultural factors underlying the ‘vaccination confidence gap. PLoS ONE 10(9):e0132562. https://doi.org/10.1371/journal.pone.0132562
Cacioppo JT, Petty RE, Kao CF (1984) The efficient assessment of need for cognition. J Personal Assess 48(3):306–307
Čavojová V, Šrol J, Ballová Mikušková E (2024) Scientific reasoning is associated with rejection of unfounded health beliefs and adherence to evidence-based regulations during the Covid-19 pandemic. Curr Psychol 43:8288–8302
Connaughton A (2021) Those on ideological right favor fewer COVID-19 restrictions in most advanced economies. Pew Res Center
Choi Y, Fox AM (2022) Mistrust in public health institutions is a stronger predictor of vaccine hesitancy and uptake than Trust in Trump. Soc Sci Med 314:115440. https://doi.org/10.1016/j.socscimed.2022.115440
Debus M, Tosun J (2021) Political ideology and vaccination willingness: implications for policy design. Policy Sci 54:477–491. https://doi.org/10.1007/s11077-021-09428-0
Denemark D, Harper T, Attwell K (2022) Vaccine hesitancy and trust in government: a cross-national analysis. Aust J Polit Sci 57:145–163
Enders A, Klofstad C, Stoler J, Uscinski JE (2023) How anti-social personality traits and anti-establishment views promote beliefs in election fraud, Qanon, and Covid-19 conspiracy theories and misinformation. Am Polit Res 51(2):247–259
Enders AM, Diekman A, Klofstad C, Murthi M, Verdear D, Wuchty S, Uscinski J (2023) On modeling the correlates of conspiracy thinking. Sci Rep 13(1):8325
Franic J (2022) What Lies behind substantial differences in COVID-19 vaccination rates between EU Member States? Front Public Health 10:858265. https://doi.org/10.3389/fpubh.2022.858265
Freeman D, Waite F, Rosebrock L, Petit A, Causier C, East A, Jenner L, Teale AL, Carr L, Mulhall S, Bold E (2022) Coronavirus conspiracy beliefs, mistrust, and compliance with government guidelines in England. Psyc Med 52(2):251–263
Fridman A, Gershon R, Gneezy A (2021) COVID-19 and vaccine hesitancy: a longitudinal study. PLoS ONE 16, e0250123
Jin S, Zilinsky J, Pradel F, Theocharis Y (2024) Beliefs in conspiracy theories and online news consumption during the onset of the COVID-19 pandemic. J Quant Desc Digit Med 4, p.1–40
Kahan DM (2013) Ideology, motivated reasoning, and cognitive reflection. Judgm Decis Mak 8(4):407–424
Karaivanov A, Kim D, Lu SE, Shigeoka H (2022) COVID-19 vaccination mandates and vaccine uptake. Nat Hum Behav 6(12):1615–1624
Keselman A, Arnott Smith C, Wilson AJ, Leroy G, Kaufman DR (2023) Cognitive and cultural factors that affect general vaccination and COVID-19 vaccination attitudes. Vaccines 11(1):94. https://doi.org/10.3390/vaccines11010094
Khairat S, Zou B, Adler-Milstein J (2022) Factors and reasons associated with low COVID-19 vaccine uptake among highly hesitant communities in the US. Am J Infect Control 50(3):262–267
Kim HJ, Min-Ho K, Choi MG, Chun EM (2024) Psychiatric adverse events following COVID-19 vaccination: a population-based cohort study in Seoul, South Korea. Mol Psychiatry 29:1–9
Klein E (2022) The Covid Policy that really mattered wasn’t a policy. New York Times
Kraft PW, Lodge M, Taber CS (2015) Why people “don’t trust the evidence” motivated reasoning and scientific beliefs. Ann Am Acad Pol Soc Sci 658(1):121–133. https://doi.org/10.1177/0002716214554758
Krastev S, Krajden O, Vang ZM et al. (2023) Institutional trust is a distinct construct related to vaccine hesitancy and refusal. BMC Public Health 23:2481
Kritzinger S, Foucault M, Lachat R, Partheymüller J, Plescia C, Brouard S (2021) Rally round the flag’: the COVID-19 crisis and trust in the national government. West Eur Polit 44(5-6):1205–1231
Larson HJ, Schulz WS, Tucker JD, Smith DMD (2015) Measuring Vaccine Confidence: Introducing a Global Vaccine Confidence Index. PLoS Curr https://doi.org/10.1371/currents.outbreaks.ce0f6177bc97332602a8e3fe7d7f7cc4
Lazarus JV, Wyka K, White TM, Picchio CA, Rabin K, Ratzan SC, Parsons Leigh J, Hu J, El-Mohandes A (2022) Revisiting COVID-19 vaccine hesitancy around the world using data from 23 countries in 2021. Nat Commun 13:3801
Lindeman M, Svedholm-Häkkinen AM, Riekki TJJ (2022) Searching for the cognitive basis of anti-vaccination attitudes. Think Reasoning 29(1):111–136. https://doi.org/10.1080/13546783.2022.2046158
Lwin MO, Lee SY, Panchapakesan C, Tandoc E (2023) Mainstream news media’s role in public health communication during crises: assessment of coverage and correction of COVID-19 misinformation. Health Commun 38(1):160–168
Mello MM, Opel DJ, Benjamin RM, Callaghan T, DiResta R, Elharake JA, Flowers LC, Galvani AP, Salmon DA, Schwartz JL, Brewer NT (2022) Effectiveness of vaccination mandates in improving uptake of COVID-19 vaccines in the USA. Lancet 400(10351):535–538
Motta M, Callaghan T (2020) The pervasiveness and policy consequences of medical folk wisdom in the US. Sci Rep 10(1):10722
Murphy J, Vallières F, Bentall RP et al. (2021) Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat Commun 12:29. https://doi.org/10.1038/s41467-020-20226-9
Niles ZA (2021) The jab or my job? COVID-19 vaccine mandates in healthcare. Mo Med 118(6):488
Ohanes G (2024) Pakistan’s polio vaccination campaign hampered by distrust. Deutsche Welle
Paul KT, Eberl J-M, Partheymüller J (2021) Policy-relevant attitudes toward COVID-19 vaccination: associations with demography, health risk, and social and political factors. Front Public Health 9:671896. https://doi.org/10.3389/fpubh.2021.671896
Piltch-Loeb R, Savoia E, Goldberg B, Hughes B, Verhey T et al. (2021) Examining the effect of information channel on COVID-19 vaccine acceptance. PLoS ONE 16(5):e0251095. https://doi.org/10.1371/journal.pone.0251095
Pinna M, Picard L, Goessmann C (2022) Cable news and COVID-19 vaccine uptake. Sci Rep 12:16804
Recio-Román A, Recio-Menéndez M, Román-González MV (2022) Political populism, institutional distrust and vaccination uptake: a mediation analysis. Int J Environ Res Public Health 19(6):3265. https://doi.org/10.3390/ijerph19063265
Rudloff JP, Hutmacher F, Appel M (2023) Post-truth epistemic beliefs rooted in the Dark Factor of Personality are associated with higher COVID-19 vaccination refusal. Sci Rep 13:4254. https://doi.org/10.1038/s41598-023-31079-9
Scheitle CP, Corcoran KE (2021) COVID-19 Skepticism in relation to other forms of science skepticism. Socius 7, 23780231211049841
Scherer AM, Schacht Reisinger H, Schweizer ML, Askelson NM, Fagerlin A et al. (2018) Cross-sectional associations between psychological traits, and HPV vaccine uptake and intentions in young adults from the United States. PLoS ONE 13(2):e0193363. https://doi.org/10.1371/journal.pone.0193363
Sharma K, Zhang Y, Liu Y (2022) COVID-19 vaccine misinformation campaigns and social media narratives. Proc Int AAAI Conf Web Soc Media 16(1):920–931
Štětka V, Brandao F, Tóth F, Mihelj S, Rothberg D, Hallin D, Klimkiewicz B, Ferracioli P (2024) Beyond social media: the influence of news consumption, populism, and expert trust on belief in COVID-19 Misinformation. Int J Press/Politics 19401612241302755
Stoler J, Klofstad CA, Enders AM, Uscinski JE (2022) Sociopolitical and psychological correlates of Covid-19 vaccine hesitancy in the United States During Summer 2021. Soc Sci Med 306:115112. https://doi.org/10.1016/j.socscimed.2022.115112
Summers T, Morrison SJ. Fake CIA Vaccine Campaign: When the End Doesn’t Justify the Means. CSIS Blog
Sunyík, V, Čavojová, V (2023). Alternative medicine, COVID-19 conspiracies, and other health-related unfounded beliefs: the role of scientific literacy, analytical thinking, and importance of epistemic rationality. Stud Psychol, 65(3), 246–261
Uscinski JE, Enders AM, Klofstad C, Seelig M, Funchion J, Everett C, Wuchty S, Premaratne K, Murthi M (2020) Why do people believe COVID-19 conspiracy theories? Harv Kennedy Sch Misinfo Rev 1(3). https://doi.org/10.37016/mr-2020-015
Uscinski JE, Enders AM, Seelig MI, Klofstad CA, Funchion JR, Everett C, Wuchty S, Premaratne K, Murthi MN (2021) American politics in two dimensions: partisan and ideological identities versus anti‐establishment orientations. Am J Pol Sci 65(4):877–895. https://doi.org/10.1111/ajps.12616
Van Deth JW (2017) Compliance, trust and norms of citizenship. In: Zmerli S, Van Der Meer TWG (eds) Handbook on Political Trust. Edward Elgar Publishing, pp 212–227
Vasilyeva N, Smith KM, Barr K, Kiper J, Stich S, Machery E, Barrett HC (2021) Evaluating information and misinformation during the COVID-19 pandemic: evidence for epistemic vigilance. CogSci 43(43)
Van Mulukom V, Pummerer LJ, Alper S, Bai H, Čavojová V, Farias J, Kay CS, Lazarevic LB, Lobato EJ, Marinthe G, Banai IP (2022) Antecedents and consequences of COVID-19 conspiracy beliefs: a systematic review. Soc Sci Med 301:114912
Van Oost P, Yzerbyt V, Schmitz M, Vansteenkiste M, Luminet O et al. (2022) The relation between conspiracism, government trust, and COVID-19 vaccination intentions: the key role of motivation. Soc Sci Med 301:114926. https://doi.org/10.1016/j.socscimed.2022.114926
Viskupič F, Wiltse DL, Meyer BA (2022) Trust in physicians and trust in government predict COVID-19 vaccine uptake. Soc Sci Q 103:509–520. https://doi.org/10.1111/ssqu.13147
Viskupič F, Wiltse DL (2024) Psychological entitlement predicts support for mandatory COVID-19 vaccination. J Med Surg Public Health 2:100043
Viswanath K, Bekalu M, Dhawan D et al. (2021) Individual and social determinants of COVID-19 vaccine uptake. BMC Public Health 21:818. https://doi.org/10.1186/s12889-021-10862-1
Ward C, Voas D (2011) The emergence of conspirituality. J Contemp Relig 26(1):103–121
Watson OJ, Barnsley G, Toor J, Hogan AB, Winskill P, Ghani AC (2022) Global impact of the first year of COVID-19 vaccination: a mathematical modelling study. Lancet Infect Dis 22(9):1293–1302. https://doi.org/10.1016/S1473-3099(22)00320-6
Žeželj I, Petrović M, Ivanović A, Kurčubić P (2023) I trust my immunity more than your vaccines:“Appeal to nature” bias strongly predicts questionable health behaviors in the COVID-19 pandemic. PLoS ONE 18(2):e0279122
Zheng W (2024) Multilevel evidence for institutional trust and vaccine confidence in 134 countries: moderating effects of cultural religiosity and individualism. Curr Psychol 43:18898–18907. https://doi.org/10.1007/s12144-023-05067-1
Zilinsky J, Zeitzoff T (2025) Artificial intelligence, social media, and the politics of anti-technology. Forthcoming. Am J Pol Sci
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
Jan Zilinsky: Conceptualization, Analysis, Methodology, Writing – original draft, Writing – review & editing, Visualization. Yannis Theocharis: Funding acquisition, Writing – review & editing, Writing – original draft.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This research was approved by the Ethics Review Board of the Faculty of Social and Behavioral Sciences, University of Amsterdam (approval was granted under project number 2022-PCJ-14828, approval date March 25, 2022). All research was conducted in accordance with the guidelines set by the Ethics Review Board and with relevant regulations governing research involving human participants, including the principles outlined in the Declaration of Helsinki.
Informed consent
Participants provided informed consent electronically at the beginning of the online survey (with participation taking place between April 20 and May 6, 2022). Consent was obtained through a detailed information page that described the study purpose, procedures, potential risks, confidentiality measures, and participants’ right to withdraw at any time without consequences. Only data from participants who actively agreed to participate after reading this information was collected and included in the study.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zilinsky, J., Theocharis, Y. Conspiracism and government distrust predict COVID-19 vaccine refusal. Humanit Soc Sci Commun 12, 1002 (2025). https://doi.org/10.1057/s41599-025-05267-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1057/s41599-025-05267-z
