
Abstract
Health inequality induced by environmental degradation has become a growing global concern. Especially for migrants across different medical insurance pooling regions, the problem is even more serious. Drawing on micro-level data from the China Health and Retirement Longitudinal Survey (CHARLS) and official air pollution data, we employ a two-stage least squares (2SLS) estimation strategy that adopts a relative deprivation perspective to identify causal effects. The findings suggest that air pollution significantly worsens health inequality, particularly among women, the elderly, and socioeconomically disadvantaged groups. Furthermore, the analysis reveals that Cross-regional Medical Insurance Scheme(CRMIS) plays a mitigating role in reducing inequality caused by air pollution. For migrants, choosing the medical insurance in the inflow region can alleviate the severity of health inequalities caused by air pollution. This research contributes to the global literature on environmental inequality by highlighting how institutional mechanisms, such as portable health insurance, can buffer the unequal health impacts of pollution. The insights derived from China’s experience offer valuable policy implications for other countries facing rapid urbanization, internal migration, and rising environmental health risks.
Similar content being viewed by others

Introduction
Health inequality has long been a core topic of research in health economics. In addition to traditional socio-economic factors such as income, education, and urban-rural divides, the impact of air pollution on health inequality has received growing global attention(Chen et al., 2023; Ebenstein et al., 2017; M. Liu et al., 2017; Lu et al., 2017). According to a 2021 UN report, 92% of the global population lived in areas where PM2.5 levels exceeded the WHO guideline of 10 μg/m3, in 2019. The 2019 Global Burden of Disease report identified air pollution as the world’s fourth leading cause of death, responsible for 1.85 million deaths. In China, rapid economic growth since 1978 has led to serious environmental degradation. In 2020, the national annual average AQI was 80.49 μg/m3, far above WHO standards. Key economic regions such as Beijing-Tianjin-Hebei, Yangtze River Delta, and Pearl River Delta had even higher levels—up to nearly nine times the WHO recommendation. These figures highlight the urgency of addressing air pollution as both an environmental and a social justice issue.
In 2017, a substantial proportion of age-standardized disability-adjusted life years (DALYs) from chronic diseases—40.0% for lower respiratory tract infections, 35.6% for diabetes, 26.1% for lung cancer, 25.8% for ischemic heart disease, and 19.5% for stroke—were attributed to air pollution (Yin et al., 2020). Environmental health concerns driven by severe air pollution intersect with socio-economic health disparities related to income, education, and registered residence. This issue is particularly salient for migrant populations, whose health is more adversely affected by sustained exposure to polluted environments. Long-term exposure, particularly to nitrogen dioxide (NO2), significantly impacts migrants’ health, increasing risks of hypertension and diabetes(Downward et al., 2022). Vulnerable groups, such as men and individuals over 30, exhibit heightened sensitivity to pollution, which not only compromises their health but also weakens their willingness to settle in polluted areas (Zhao et al., 2021).
In order to address health inequality, China established three medical insurance systems in 1998, 2003, and 2007, covering urban workers, farmers, and other urban residents, achieving near-universal coverage. However, due to regional enrollment restrictions, migrants often register their insurance in their registered permanent residence (RPR), limiting access to medical services in inflow cities. Cross-city medical treatment is constrained by complex referral and reimbursement procedures, resulting in delays and reduced healthcare accessibility for migrants across different medical insurance pooling regions.
Against this backdrop, the Cross-Regional Medical Insurance System (CRMIS) was introduced, allowing the insured to choose enrollment in either their RPR or current location. This concept first appeared in the 1998 State Council Decision, which enabled sectors with the characteristic of cross-regional work—such as railways and maritime transport—to centralize insurance in work locations. In 2010, the Interim Measures for the Transfer and Continuation of Basic Medical Insurance for Migrant Workers permitted rural migrants with stable employment to join urban insurance schemes. Article 32 of the 2011 Social Insurance Law further supported transferring insurance relationships across regions. Following the 2016 integration of urban and rural schemes, CRMIS reforms promoted unified enrollment and enhanced portability (Cheng et al., 2015; Yang, 2007). Nevertheless, health inequality driven by air pollution continues to undermine these achievements, highlighting the need for further system improvements to safeguard health equity.
Literature review and research hypothesis
Impact of air pollution on health and health inequality
There is a large literature on the impact of air pollution on health, with only a few on health inequality. Rising air pollution levels lead to a significant decline in the mental health of the population (Buoli et al., 2018; Yang et al., 2021). Air pollution also leads to a decline in individual subjective well-being (Zhang et al., 2017). Increased air pollution leads to increased mortality among infants, adults, and the elderly (Cesur et al., 2018; Chay & Greenstone, 2003; Heft-Neal et al., 2018). The increase of air pollution will boost the number and prevalence of respiratory diseases (Schlenker & Walker, 2016).
The health damage consequences caused by different air pollution levels vary among different economic status, regions, races, nationalities, genders, and division between urban and rural (Collins et al., 2017; Evans & Kantrowitz, 2002; Gu et al., 2013). First of all, air pollution is obviously pro-poor (Dell et al., 2012; Kumar & Khanna, 2019), and groups with lower socioeconomic status are more likely to be exposed to pollution. In areas with low economic development, the health economic burden of air pollution is heavier (Finkelstein et al., 2005; Grineski et al., 2013). The results of Richardson et al. (2013) showed that mortality from circulatory diseases in low-income areas of Eastern Europe and respiratory mortality in males in low-income areas of Western Europe were more likely to be affected by air pollution. Only in the poorest areas, the reduction of air pollution is likely to reduce the degree of health inequality (Richardson et al., 2011). The health damage caused by air pollution further exacerbates health inequality across income groups and increases the extent to which income inequality affects health inequality (Yang & Liu, 2018). Secondly, the difference in air pollution suffered by racial and ethnic disparities will also lead to health inequalities (Hackbarth et al., 2011). Woo et al. (2019) concluded that racial and ethnic minorities are exposed to significantly higher levels of air pollution compared to whites, and addressing this uneven environmental burden may be a promising way to improve population health and reduce racial and ethnic disparities among them. Thirdly, there are significant urban-rural and gender differences in health inequality caused by air pollution (Azimi et al., 2019). Rural men aged 30–34 years are more likely to die of cancer, while rural women aged 15–19 years have a 47% higher death rate and 44% higher cancer death rate than urban women (Liu et al., 1999).
The limitations of current research and the marginal contributions of this article
To sum up, while existing studies have made significant progress in exploring the relationship between air pollution and health inequality, several limitations remain. Firstly, due to the limitation of research indicators, most studies analyze the health consequences of air pollution from the perspective of the differences between urban-rural areas, regions, and other populations, while there are few research results on the direct effects of air pollution on health inequality. The second is the lack of explanation from the perspective of medical insurance policy, which is hidden behind the health inequality problem. In light of the problems above, this article conducts research. The marginal contributions of this paper are as follows. First, this paper employs the relative deprivation index to construct an individual-level health inequality index, and based on this, the quantitative analysis reveals that air pollution exacerbates health inequality—an increase in air pollution further intensifies disparities in individual health inequality. Second, it examines the effect of the CRMIS targeting migrants in mitigating health inequality induced by air pollution. The findings indicate that for migrants across different medical insurance pooling regions in China, enrolling in medical insurance in the inflow region rather than in their registered residence region can effectively reduce the health inequality caused by air pollution.
Building upon the existing literature and addressing the above-mentioned research gaps, this study attempts to further explore the mechanisms through which air pollution contributes to health inequality. In particular, we draw upon the theory of relative deprivation to provide a more nuanced understanding of how disparities in environmental exposure translate into unequal health outcomes across individuals.
Relative deprivation theory
In the concept of relative deprivation, health inequality means that in a group, the lower the individual’s health level, the higher the relative deprivation degree will be in the accumulation of health disadvantage, and the higher the degree of health inequality will be. The idea behind the concept, which has been used by a wide range of scholars (Smith et al., 2012; Wilkinson, 1997), is that a person’s health or health-related behaviors depend on both his own resources and his relative position with respect to those resources (Caner & Yiğit, 2019). Differentiated air pollution exposure will lead to differences in the relative degree of individual health deprivation. Compared with those at low levels of air pollution (Bell & Ebisu, 2012), individuals at high levels of air pollution will face a higher risk of worse health. When individuals’ access to goods, services, and social activities is limited (Kuo & Chiang, 2013), the relative degree of individual health deprivation caused by air pollution will be deepened; thus air pollution will aggravate the health inequality among individuals (Currie et al., 2009; Currie et al., 2011). Therefore, we put forwarda hypothesis:
H1: The more severe the air pollution, the higher the relative health deprivation of individuals caused by air pollution, and the higher the level of health inequality will be.
The moderating effect of CRMIS
The choice of CRMIS will greatly affect the availability and accessibility of individual health care services. Individuals with local medical insurance are more likely to obtain timely medical intervention to avoid health deprivation caused by air pollution, thus reducing the harm of air pollution on health inequality (Chen et al., 2013; Currie & Neidell, 2005). By increasing the probability of individuals living in air pollution areas accessing health care services, reducing the economic burden of disease, and avoiding the level of health deprivation of migrants, the CRMIS alleviates the harm of air pollution on health inequality (Meng et al., 2018; Onwujekwe et al., 2010). Therefore, this paper puts forward a hypothesis:
H2: The harm of air pollution on the level of health inequality among individuals is regulated by the location of medical insurance enrollment. Compared with the migrants insured in the permanent registered residence, the migrants insured in the inflow region suffer less harm from the relative deprivation of health caused by air pollution, and the level of health inequality is also lower.
Methodology
Material, methods, and data sources
The data come from the China Health and Retirement Longitudinal Survey (CHARLS). The survey is a large-scale interdisciplinary survey project conducted by the National School of Development at Peking University and the China Social Science Survey Center. CHARLS conducted surveys and interviews in 150 counties and 450 communities (villages) in 28 provinces (autonomous regions and municipalities directly under the Central Government) in 2011, 2013, 2015, and 201,8 respectively. By the time the national follow-up was completed in 2018, its sample had covered 19,000 respondents from a total of 12,400 households. Considering that the core explanatory variables (AQI) before 2014 are seriously missing, this paper chooses the data of 2015 and 2018 in CHARLS as samples for research. After deleting the missing values of health inequality and the sample observations under 45 years old, we obtain 32479 valid samples from 7305 households in 28 provinces, and 28752 valid samples after deleting the missing values of main control variables. Finally, after taking the moderating variable of medical insurance participation into account in the measurement model, there are 26,526 valid samples. In addition, the data of AQI, PM10, NO2, and CO were collected from the National Urban Air Quality real-time publishing platform of the China Environmental Monitoring Station and the China Environmental Statistical Yearbook of the National Bureau of Statistics and the Ministry of Environmental Protection of China. PM2.5 in the air pollution data comes from the Atmospheric Composition Analysis Group (ACAG) of Washington University (St. Louis).
Variable measurement
Dependent variable
The dependent variable in this paper is health inequality index. Firstly, the physical health indicator was selected with reference to the disease classification of the CHARLS survey, which measures health from the dimension of physical health, considering both acute and chronic shocks. These physical health indicators are closely related to air pollution, and the more serious the air pollution is, the more serious the harm of diseases such as respiratory diseases, cardiovascular diseases, and liver fibrosis will be (C. Liu et al., 2017; Zheng et al., 2015). Secondly, referring to the construction method of physical health index by Wang and Luo (2020), the entropy weight method is used to calculate the health index (Wang et al., 2025; Zhang & Jiang, 2021), and the index and weights are shown in Table 1. Finally, Kakwani (1984) proposed the concept of relative deprivation to convert physical health into an index of physical health inequality. The Kakwani index satisfies both dimensionality and normalization characteristics, and the weighted average of relative deprivation among all individuals is the Gini coefficient, which has good properties in fitting income, consumption, and health distributions(Fukushige et al., 2012). According to the notion of relative deprivation, in a group, the lower the individual’s health level, the greater the health disadvantage, and the higher the degree of relative health deprivation, which means the higher the level of health inequality. Suppose Y represents a reference group, and the sample size is n. We rank the health level y of individuals, and the overall health distribution is obtained as a vector \(Y=({y}_{1},{y}_{2},{y}_{3},\ldots ,{y}_{n-1},{y}_{n})\), where\({y}_{1}\le {y}_{2}\le {y}_{3},...,\le {y}_{n-1}\le {y}_{n}\). Then, compared resident i with another resident j, the relative deprivation index \({RD}\left({y}_{j},{y}_{i}\right)\) of resident i is expressed as:
On the basis of the formula (1), the average value of \({RD}\left(y,{y}_{i}\right)\) received by resident i can be expressed as:
Where \({\mu }_{Y}\) is the average health level in the reference group Y, \({n}_{{y}_{i}}^{+}\) is the number of individuals whose health index exceeds \({y}_{i}\) in the group Y, and \({\mu }_{{y}_{i}}^{+}\) is the average health level of those individuals mentioned above.
Independent variable
The air pollution indicators were measured using the Air Quality Index (AQI) for the year prior to the CHARLS2015 and CHARLS2018 survey, respectively. According to the Ambient Air Quality Standards of the People’s Republic of China (GB3095-2012), the ambient air quality index (AQI) is calculated from the concentrations of six pollutants in the air, namely SO2, NO2, PM10, PM2.5, carbon monoxide, and ozone. The corresponding pollutant air quality sub-index (IAQI) is calculated based on the monitored average concentrations of the six air pollutants over a certain period of time, where the maximum value of the pollutant air quality sub-index (IAQI) is the ambient air quality index (AQI) for that period of time. AQI has good representativeness and applicability (Hu et al., 2015; Lu, 2020). Secondly, in order to verify the robustness of air pollution indicators, we adopt the specific values of PM2.5, PM10, and CO to measure air pollution.
Moderating variable
This paper mainly discusses the CRMIS, and the selected index is the location of enrollment in medical insurance. This index is mainly measured by the question “ place of medical insurance enrollment”, and the main answers are 3 options: the inflow location, the registered residence place, and other places. The insurance in the inflow region means the migrants are insured in their settlement where they work and live, instead of their registered residence places, and there is no overlap with the two kinds of places. Since the proportion of the insured samples in other places is very small, less than 1%, we only discuss the different degrees of the moderating effect caused by the difference of insured place between the inflow region and the registered residence region for the migrants.
Control variable
Referring to the previous studies (Lavaine, 2015; Yang & Liu, 2018), the control variables selected in this study include the characteristics of individual residents’ socioeconomic status and health behavior. The socio-economic status characteristics mainly include gender, age, marital status, education level, registered residence, place of settlement, social medical insurance, commercial medical insurance, household per capita income, and region. Health behavior characteristics mainly include smoking, drinking, and exercise. Table 2 reports the descriptive statistics of main variables. Family income and Ventilation Coefficient(VC) were logarithmized in the regression equation.
Measurement methods
This study aims to explore the impact of air pollution on health inequality, and uses the two-stage least squares (2SLS) method for estimation, which is widely used in the research on air pollution, health and its inequality (Anwar et al., 2021; Kim et al., 2003; Wang et al., 2021). The 2SLS regression model is set as follows:
Where \({{pollution}}_{{ij}}\) is the AQI and six kinds of air pollution indicators of prefecture-level administrative region j where resident i is located, indicating the degree of air pollution; \({{VC}}_{{ij}}\) is the Ventilation Coefficient of the prefecture-level administrative region j where resident i is located, which is used as the instrumental variable of air pollution in 2SLS regression. \({{Inequlity}}_{{ij}}\) is the degree of health inequality of resident i in area j; \({X}_{{ij}}\) is the control variables, which include a series of factors affecting health inequality at the individual, family, and regional levels; \({\varepsilon }_{{ij}}\) and \({\omega }_{{ij}}\) are the random term.
This study refers to the construction method of \({\rm{VC}}\) (Broner et al., 2012). The formula for calculating \({VC}\) is as follows, where \({WS}\) is the wind speed at a height of 10 meters and \({BLH}\) is the Boundary Layer Height.
The \({VC}\) satisfies the constraints of correlation and exclusivity, meets the requirements of instrumental variable method, and can effectively solve the problems of reverse causality, measurement error, and omitted variables. The reasons are as follows: firstly, the wind speed determines the diffusion speed and range of pollutants, while the height of the boundary layer determines the height of diffusion. Therefore, ceteris paribus, regions with larger air mobility coefficients have stronger transmission, diffusion capacity of air pollution,n and lower concentrations of pollutants, thus satisfying the correlation hypothesis. Secondly, the \({VC}\) is determined by meteorological conditions such as wind speed and boundary layer height, and has nothing to do with economic activities such as economic growth, capita,l and technology (Broner et al., 2012), so it will not affect residents’ ability to invest in health. Moreover, the calculation results show that meteorological conditions such as wind speed will not affect the health inequality among residents by affecting daily activities or outdoor sports, so as to satisfy the exclusivity constraint. Data on wind speed and boundary layer height were obtained from the European Centre for Medium-Range Weather Forecasts (ECMWF). In this study, ArcGIS is used to transform and extract global raster meteorological data, and the mean value of \({VC}\) one year before the survey is calculated asan instrumental variable.
Results
Regression results of two-stage least squares method
Table 3 shows the results of the first-stage regression based on two-stage least squares. Firstly, the validity of instrumental variables is examined, and the F-values are all greater than 10 and significant at 1% confidence level, indicating that there is no weak instrumental variable problem. In addition, the air mobility coefficient is significantly negative, indicating that the increase of air mobility coefficient favors the diffusion of air pollutants and reduces the concentration of pollutants, which is negatively correlated with each other. Columns 1 and 2 in Table 4 report the regression results by 2SLS without and with control variable, respectively. To verify the robustness, columns 3 and 4 of Table 4 report the regression results by the ordinary least squares method (OLS) without and with control variable, respectively. From the results, the results of 2SLS are better than those of OLS, and the OLS method underestimates the direct role of air pollution on health inequality. The regression of 2SLS needs to first test the validity of the instrumental variables. In the first-stage regression, the \({VC}\) is significantly negative, indicating that the increase of \({VC}\) is conducive to the diffusion of air pollutants and reduces the pollution concentration, and the two have a negative correlation. In addition, the F values are all greater than 10 and significant at the 1% confidence level, indicating that there is no weak instrumental variable problem. In the second-stage regression, the estimated coefficients of the inequality of AQI on physical health are significantly positive in both columns (1) and (2), indicating that air pollution has caused an increase in the inequality of physical health. Specifically, the regression coefficients in columns (1) and (2) are 0.0030 and 0.0040, respectively. which means that for every 1 unit increase in annual average AQI, the inequality of physical health will increase by 0.0030 and 0.0040 units, respectively. This result shows that air pollution will aggravate the degree of health inequality among individuals, which verifies Hypothesis 1.
Robustness test
Replace self-rated health inequality indicators
This paper conducts robustness test from three aspects. Firstly, the health inequality indicator is reconstructed based on self-rated health, which is assigned 5, 4, 3, 2, 1, and 0 points in order of excellent, very good, good, fair, bad, and very bad for robustness test. And then the self-rated health indicator is transformed into health inequality index by relative deprivation index method. According to the results in Column (1) of Table 5, air pollution significantly increases the inequality of self-rated health among residents, and the regression results are still robust after replacing the index.
Replace instrumental variable
We use the “inverse temperature” indicator as an instrumental variable of air pollution for robustness testing. The number of annual occurrences of inversions at the city level in China provided by NASA is calculated. The validity tests for the inverse temperature variable revealed that all F-statistics exceeded 10 and were statistically significant at the 1% level, indicating the absence of a weak instrument problem. Column (2) of Table 5 shows the regression results. It is found that a one-unit increase in AQI significantly increases physiological health inequality by 0.0026 units at the 1% significance level. This indicates that the effect of air pollution on worsening health inequality remains significant when using IV for air pollution, and the conclusions of this paper are robust.
Using fixed effects models
To verify the reliability of the instrumental variable (IV) approach, this study further employs a fixed effects model to analyze the panel data. The model incorporates both individual fixed effects and year fixed effects to identify the dynamic effects of air pollution on health inequality. As shown in Column (3) of Table 5 the direction of the regression coefficient for air pollution remains consistent with that of the IV approach. This suggests that the positive effect of air pollution on health inequality remains robust even after controlling for unobserved fixed differences across regions and time-varying confounders, further supporting the reliability of the study’s conclusions.
Select different pollutant indicators
PM2.5, PM10, and CO were selected to replace AQI as indicators to measure air pollution levels, because these are main air pollutants, which are very harmful to the human body. The results are shown in column 2, column 3 and column 4 of Table 6, respectively. If PM2.5, PM10, and CO increase by one unit, the health inequality of residents will increase by 0.0028, 0.0066, and 0.3603 units, respectively.
Heterogeneity analysis
Heterogeneity analysis of different populations
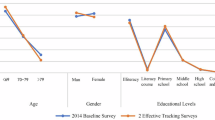
To further investigate the heterogeneity in the impact of air pollution on health inequality, we introduce interaction terms between AQI and key individual characteristics, including gender, age, and self-rated health status. The heterogeneity analysis is also conducted using the two-stage least squares (2SLS) instrumental variable approach to ensure consistency with the baseline estimation and address potential endogeneity. As shown in Table 7, the interaction between AQI and gender is significantly negative (−0.0076, p < 0.01), indicating that air pollution increases health inequality for both men and women, with a stronger effect observed among women. For age, the sample is divided into a middle-aged group (45–59 years) and an elderly group (60 years and above). The interaction term is also significantly negative (−0.0025, p < 0.01), suggesting that the elderly are more vulnerable to the inequality-increasing effects of air pollution compared to the middle-aged. Regarding self-rated health, individuals with poorer health—classified as those who rated their health as “fair,” “poor,” or “very poor”—are found to be more severely impacted, as indicated by the significant interaction term (−0.0026, p < 0.01). These results collectively demonstrate that air pollution exacerbates health inequality more substantially among women, the elderly, and those with poor health status.
Analysis of heterogeneity by socioeconomic status
To analyze the heterogeneity of the impact of air pollution on health inequality across different socioeconomic groups, Table 8 presents 2SLS regression results based on registered residence, income level, and educational attainment. In terms of registered residence, the interaction term between AQI and rural registration is significantly negative (−0.0116, p < 0.01), indicating that air pollution significantly increases health inequality among rural residents, while the effect for urban residents is relatively weaker. For income level, using the average annual household income of CNY 39,162 as the threshold, results show that air pollution significantly exacerbates health inequality in the low-income group (−0.0007, p < 0.01), but the effect is not significant for the high-income group. Regarding education, individuals with lower educational attainment experience a greater worsening of health inequality due to air pollution, as shown by a significantly negative interaction coefficient (−0.0003, p < 0.01), whereas the effect is less pronounced for those with higher education levels.
Moderating effect
In order to further explore the mechanism of air pollution on health inequality, we use the “place of medical insurance enrollment” as the moderating variable for analysis.
The regression results in columns 1 and 2 of Table 9 show that air pollution worsens health inequality. The impact of the interaction term between air pollution and the insured place on health inequality in column 1 and column 2 is significantly negative. The coefficient of the interaction term in column 2 is −0.0031 and passes the significance test at the level of 1%, which is consistent with Hypothesis 2. This result shows that the health inequality caused by the air pollution suffered by the insured individuals in the inflow region is lower than that of the insured individuals in registered residence areas. This study reveals that the choice of medical insurance enrollment location (particularly migrants opting for coverage in their inflow regions) significantly moderates air pollution’s impact on health inequality. By enhancing healthcare accessibility and reimbursement rates (compared to hometown-based insurance), inflow-region enrollment enables timely medical interventions, reduces out-of-pocket costs, and alleviates household financial burdens, thereby mitigating health disparities caused by pollution.
Discussion
First of all, this study found that air pollution (AQI) can increase the degree of health inequality, and different pollutants (PM2.5, PM10, CO) have a similar effect. Differentiated air pollution exposure will lead to differences in individual health inequality, and high air pollution will aggravate individual health inequality through relative deprivation. This finding further verified previous studies (Azimi et al., 2019; Bell & Ebisu, 2012), and Hypothesis 1 is verified. This paper provides new insights into the mechanisms behind these results, arguing that the reasons for this result are through differentiated air pollution exposure levels related to socioeconomic status and lack of adequate health care system. High air pollution exposure is highly associated with disadvantaged groups of socioeconomic status (Gray et al., 2014). High-income groups generally live in areas with low air pollution exposure, and air pollution control policies have a significant positive impact on low exposure and middle-income groups (Shen et al., 2020). Low-income people are more likely to be exposed to the working and living environment with high air pollution (Carson et al., 1997; Landrigan, 2017), which will aggravate the degree of health inequality among individuals. The lack of medical insurance system, uneven distribution of medical health resources, and poor accessibility of medical services are also important reasons for the aggravation of health inequality (Matus et al., 2012; Yang & Liu, 2018). Basic medical insurance will reduce the individual’s medical expenditure (Dou et al., 2018), and participating in medical insurance will aggravate the inequality of the poor’s medical care utilization (Zhang et al., 2023). When individuals suffer from the damage caused by air pollution, health inequalities can be alleviated through timely treatment, improving health status, and reducing the economic burden of individuals. This study adds to the existing literature by linking air pollution exposure to structural barriers in healthcare access.
Secondly, this study also finds that the impact of air pollution on health inequality is heterogeneous, and the air pollution impact on the degree of health inequality is greater for female groups. The reason why women are more vulnerable to air pollution may be due to the influence of physiological and social factors. Previous studies have also shown a similar view that women’s lungs and immune system may be more sensitive to air pollution, making them more vulnerable to the pollutants (Ghosh et al., 2007). Moreover, women may engage in more household and community activities, thus increasing their exposure to indoor air pollution (Parikh et al., 1999; Pitt et al., 2005). These research conclusions are consistent with this paper that air pollution has a greater impact on women’s health inequality. Moreover, the air pollution impact on health inequality is greater for the group over 60 years old, rural registered residence, low income, and low education level, respectively. This paper further advances previous findings by highlighting these subgroup disparities. Due to the decline of physiological function, weakened immune system, and chronic diseases, air pollution may further reduce the health level of the elderly, leading to health inequality (Brook et al., 2010; India State Level Dis, B (2019); Pope et al., 2002). Low-income groups and those with low education levels generally tend to live in areas with high air pollution, and when faced with air pollution, they take fewer relative measures and suffer more health damage (Bowe et al., 2018; Chakraborty, 2021). This study sheds new light on how environmental inequality and social vulnerability interact to reinforce health disparities, using the relative deprivation index approach to measure health inequality.
Finally, the moderating effect in this study finds that the place of medical insurance participation can moderate the relationship between air pollution and health inequality. Specifically, the migrants choosing the enrollment locations where they inflow into and settle down can reduce the health inequality caused by air pollution. Although the moderating effect of medical insurance has been documented by many studies (Lee et al., 2019; Lee et al., 2012; Yang & Hu, 2022), previous studies mainly focused on the relationship between length of residence, chronic diseases, and health expenditure, rarely addressing the moderating effect of medical insurance in the relationship between air pollution and health inequality. This study innovatively finds that choosing the inflow region for medical insurance enrollment can play a positive role in moderating the health inequality caused by air pollution. The reason may be that compared with the insurance in the registered residence, the insurance in the inflow region can improve the convenience of individual medical treatment and the reimbursement ratio. Through timely medical treatment, individuals can reduce the health damage caused by air pollution, reduce the personal medical expenses, and reduce the family burden, so as to increase the relative investment in health, improve their own health level, and reduce the degree of health inequality. Those research conclusions verify Hypothesis 2.
Conclusions
Air pollution remains one of the most significant environmental threats to human health, and the health inequality it induces—particularly among migrants—requires urgent attention. Drawing on longitudinal micro data from the 2015 and 2018 waves of the CHARLS, combined with official air pollution data, this study employs a 2SLS estimation approach to identify the causal effects of air pollution on health inequality. The findings confirm that air pollution significantly exacerbates health inequality, particularly among women, older adults, and socioeconomically disadvantaged populations. Furthermore, the CRMIS demonstrates a mitigating effect, alleviating the severity of pollution-induced health disparities among migrants who are enrolled in local insurance programs.
This paper contributes by showing that air pollution worsens individual health inequality using a relative deprivation index, and that the CRMIS helps mitigate this effect for migrants enrolled in inflow-region insurance. A limitation of this study is that the temporal scope of the AQI data is limited, which prevents us from capturing the relationship between air pollution and health inequality prior to 2014. Future research could extend the time frame to explore the long-term impacts of air pollution on health inequality more comprehensively.
Focusing on air pollution in China and its impact on the health of internal migrants, this study offers insights that are relevant to other countries confronting comparable challenges. The findings highlight the critical importance of incorporating health equality into environmental policy objectives and provide practical recommendations for policymakers to mitigate pollution-induced health disparities.
Data availability
The data used in this study are derived from the CHARLS (https://charls.pku.edu.cn/), the Ministry of Ecology and Environment of China (https://www.mee.gov.cn/), and Washington University in St. Louis (https://sites.wustl.edu/acag/datasets/surface-pm2-5-archive/). All the data in this article are publicly available.
References
Anwar A, Ullah I, Younis M, Flahault A (2021) Impact of air pollution (PM2.5) on child mortality: evidence from Sixteen Asian countries. Int J Environ Res Public Health 18(12): Article 6375. 13
Azimi M, Feng F, Zhou CY (2019) Air pollution inequality and health inequality in China: An empirical study. Environ Sci Pollut Res 26(12):11962–11974
Bell ML, Ebisu K (2012) Environmental inequality in exposures to airborne particulate matter components in the United States. Environ Health Perspect 120(12):1699–1704
Bowe B, Xie Y, Li TT, Yan Y, Xian H, Al-Aly Z (2018) The 2016 global and national burden of diabetes mellitus attributable to PM2.5 air pollution. Lancet Planet Health 2(7):E301–E312
Broner F, Bustos P, Carvalho VM (2012) Sources of comparative advantage in polluting industries. CEPR Discussion Paper No. DP9111, Available at SSRN: https://ssrn.com/abstract=2153492
Brook RD, Rajagopalan S, Pope CA, Brook JR, Bhatnagar A, Diez-Roux AV, Holguin F, Hong YL, Luepker RV, Mittleman MA, Peters A, Siscovick D, Smith SC, Whitsel L, Kaufman JD American Heart Association Council on Epidemiology and Prevention, Council on the Kidney in Cardiovascular Disease, and Council on Nutrition, Physical Activity and Metabolism2010) Particulate matter air pollution and cardiovascular disease an update to the scientific statement from the American Heart Association Circulation 121(21):2331–2378
Buoli M, Grassi S, Caldiroli A, Carnevali GS, Mucci F, Iodice S, Cantone L, Pergoli L, Bollati V (2018) Is there a link between air pollution and mental disorders? Environ Int 118:154–168
Caner A, Yiğit YC (2019) Relative deprivation and its association with health indicators: Lower inequality may not improve health. SSM-Popul health 7:100381
Carson RT, Jeon Y, McCubbin DR (1997) The relationship between air pollution emissions and income: US data. Environ Dev Econ 2(4):433–450
Cesur R, Tekin E, Ulker A (2018) Can natural gas save lives? Evidence from the deployment of a fuel delivery system in a developing country. J Health Econ 59:91–108
Chakraborty J (2021) Convergence of COVID-19 and chronic air pollution risks: Racial/ethnic and socioeconomic inequities in the US. Environ Res 193:110586
Chay KY, Greenstone M (2003) The impact of air pollution on infant mortality: Evidence from geographic variation in pollution shocks induced by a recession. Q J Econ 118(3):1121–1167
Chen F, Zhang X, Chen Z (2023) Air pollution and mental health: Evidence from China Health and Nutrition Survey. J Asian Econ, 86. https://doi.org/10.1016/j.asieco.2023.101611
Chen YY, Ebenstein A, Greenstone M, Li HB (2013) Evidence on the impact of sustained exposure to air pollution on life expectancy from China’s Huai River policy. Proc Natl Acad Sci USA 110(32):12936–12941
Cheng LG, Liu H, Zhang Y, Shen K, Zeng Y (2015) The impact of health insurance on health outcomes and spending of the elderly: evidence from china’s new cooperative medical scheme. Health Econ 24(6):672–691
Collins TW, Grineski SE, Morales DX (2017) Environmental injustice and sexual minority health disparities: A national study of inequitable health risks from air pollution among same-sex partners. Soc Sci Med 191:38–47
Currie J, Hanushek EA, Kahn EM, Neidell M, Rivkin SG (2009) Does pollution increase school absences? Rev Econ Stat 91(4):682–694
Currie J, Neidell M (2005) Air pollution and infant health: what can we learn from California’s recent experience? Q J Econ 120(3):1003–1030
Currie J, Ray SH, Neidell M (2011) Quasi-experimental studies suggest that lowering air pollution levels benefits infants’ and children’s health. Health Aff 30(12):2391–2399
Dell M, Jones BF, Olken BA (2012) Temperature shocks and economic growth: evidence from the last half century. Am Econ J -Macroecon 4(3):66–95
Dou GS, Wang Q, Ying XH (2018) Reducing the medical economic burden of health insurance in China: Achievements and challenges. Biosci Trends 12(3):215–219
Downward G, de Lange T, Beune E, Meeks K, Owusu-Dabo E, Bakhendeka S, Danquah I, Mockenhaupt F, Schulze M, Smeeth L, Stronks K, Addo J, Agyemang C, Klipstein-Grobusch K, Boateng D (2022) International variations in air pollution and cardiometabolic risk among Ghanaian migrants: The RODAM study. ISEE Conference Abstracts, 2022(1). https://doi.org/10.1289/isee.2022.P-0721
Ebenstein A, Fan M, Greenstone M, He G, Zhou M (2017) New evidence on the impact of sustained exposure to air pollution on life expectancy from China’s Huai River Policy. Proc Natl Acad Sci 114(39):10384–10389
Evans GW, Kantrowitz E (2002) Socioeconomic status and health: The potential role of environmental risk exposure. Annu Rev Public Health 23:303–331
Finkelstein MM, Jerrett M, Sears MR (2005) Environmental inequality and circulatory disease mortality gradients. J Epidemiol Community Health 59(6):481–487
Fukushige M, Ishikawa N, Maekawa S (2012) A modified Kakwani measure for health inequality. Health Econ Rev 2(1):10
Ghosh R, Rankin J, Pless-Mulloli T, Glinianaia S (2007) Does the effect of air pollution on pregnancy outcomes differ by gender? A systematic review. Environ Res 105(3):400–408
Gray SC, Edwards SE, Schultz BD, Miranda ML(2014) Assessing the impact of race, social factors and air pollution on birth outcomes: a population-based study. Environ Health 13: Article 4. https://doi.org/10.1186/1476-069x-13-4
Grineski SE, Collins TW, Chakraborty J, McDonald YJ (2013) Environmental health injustice: exposure to air toxics and children’s respiratory hospital admissions in El Paso, Texas. Profess Geogr 65(1):31–46
Gu D, Wang Y, Smeltzer C, Liu Z (2013) Reduction in NOx emission trends over China: regional and seasonal variations. Environ Sci Technol 47(22):12912–12919
Hackbarth AD, Romley JA, Goldman DP (2011) Racial and ethnic disparities in hospital care resulting from air pollution in excess of federal standards. Soc Sci Med 73(8):1163–1168
Heft-Neal S, Burney J, Bendavid E, Burke M (2018) Robust relationship between air quality and infant mortality in Africa. Nature 559(7713):254–258
Hu JL, Ying Q, Wang YG, Zhang HL (2015) Characterizing multi-pollutant air pollution in China: Comparison of three air quality indices. Environ Int 84:17–25
India State Level Dis, B (2019) The impact of air pollution on deaths, disease burden, and life expectancy across the states of India: the Global Burden of Disease Study 2017. Lancet Planet Health 3(1):E26–E39
Kakwani N (1984) The relative deprivation curve and its applications. J Bus Economic Stat 2(4):384–394
Kim CW, Phipps TT, Anselin L (2003) Measuring the benefits of air quality improvement: a spatial hedonic approach. J Environ Econ Manag 45(1):24–39
Kumar S, Khanna M (2019) Temperature and production efficiency growth: empirical evidence. Clim Change 156(1-2):209–229
Kuo CT, Chiang TL (2013) The association between relative deprivation and self-rated health, depressive symptoms, and smoking behavior in Taiwan. Soc Sci Med 89:39–44
Landrigan PJ (2017) Air pollution and health. Lancet Public Health 2(1):e4–e5
Lavaine E (2015) An econometric analysis of atmospheric pollution, environmental disparities and mortality rates. Environ Resour Econ 60(2):215–242
Lee H-Y, Oh J, Hoang VM, Moon JR, Subramanian S (2019) Use of high-level health facilities and catastrophic expenditure in Vietnam: can health insurance moderate this relationship? BMC health Serv Res 19(1):1–12
Lee S, O’Neill A, Park J, Scully L, Shenassa E (2012) Health insurance moderates the association between immigrant length of stay and health status. J Immigr Minority Health 14(2):345–349
Liu C, Chen RJ, Zhao YH, Ma ZW, Bi J, Liu Y, Meng X, Wang YF, Chen XX, Li WH, Kan HD (2017) Associations between ambient fine particulate air pollution and hypertension: A nationwide cross-sectional study in China. Sci Total Environ 584:869–874
Liu M, Huang Y, Ma Z, Jin Z, Liu X, Wang H, Liu Y, Wang J, Jantunen M, Bi J, Kinney PL (2017) Spatial and temporal trends in the mortality burden of air pollution in China: 2004–2012. Environ Int 98:75–81
Liu YL, Hsiao WC, Eggleston K (1999) Equity in health and health care: the Chinese experience. Soc Sci Med 49(10):1349–1356
Lu JG (2020) Air pollution: A systematic review of its psychological, economic, and social effects. Curr Opin Psychol 32:52–65
Lu Z-N, Chen H, Hao Y, Wang J, Song X, Mok TM (2017) The dynamic relationship between environmental pollution, economic development and public health: Evidence from China. J Clean Prod 166:134–147
Matus K, Nam KM, Selin NE, Lamsal LN, Reilly JM, Paltsev S (2012) Health damages from air pollution in China. Glob Environ Change-Hum Policy Dimens 22(1):55–66
Meng YY, Han JQ, Qin SQ (2018) The impact of health insurance policy on the health of the senior floating population-evidence from China. Int J Environ Res Public Health 15(10):Article 2159. 17
Onwujekwe O, Okereke E, Onoka C, Uzochukwu B, Kirigia J, Petu A (2010) Willingness to pay for community-based health insurance in Nigeria: do economic status and place of residence matter? Health Policy Plan 25(2):155–161
Parikh J, Smith K, Laxmi V (1999) Indoor air pollution: A reflection on gender bias. Economic Political Wkly 34(9):539–544
Pitt, MM, Rosenzweig, MR, & Hassan, MN (2005). Sharing the burden of disease: gender, the household division of labor and the health effects of indoor air pollution. CID Working Paper Series. http://nrs.harvard.edu/urn-3:HUL.InstRepos:42482318
Pope CA, Burnett RT, Thun MJ, Calle EE, Krewski D, Ito K, Thurston GD (2002) Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. Jama-J Am Med Assoc 287(9):1132–1141
Richardson EA, Pearce J, Kingham S (2011) Is particulate air pollution associated with health and health inequalities in New Zealand? Health place 17(5):1137–1143
Richardson, EA, Pearce, J, Tunstall, H, Mitchell, R, & Shortt, NK (2013). Particulate air pollution and health inequalities: a Europe-wide ecological analysis. Int J Health Geogr, 12(1). https://doi.org/10.1186/1476-072x-12-34
Schlenker W, Walker WR (2016) Airports, Air Pollution, and Contemporaneous Health. Rev Econ Stud 83(2):768–809
Shen F, Wang Q, Zou J, Yan H, Wang B (2023) Air pollution and migration decision of migrants in low-carbon society. Int J Environ Res Public Health 20(1):870
Shen MH, He W, Li LY (2020) Incentives to use primary care and their impact on healthcare utilization: Evidence using a public health insurance dataset in China Soc Sci Med 255:112981
Smith HJ, Pettigrew TF, Pippin GM, Bialosiewicz S (2012) Relative deprivation: a theoretical and meta-analytic review. Personal Soc Psychol Rev 16(3):203–232
Wang Y, Zhang Z, Hao Z, Eriksson T (2025) Environmental regulation and mental well-being: Evidence from China’s air pollution prevention and control action plan. Soc Sci Med 365:117584
Wang YZ, Luo NS (2020) Air Pollution, Health Depreciation and Medical Costs: Research Based on the Three Perspectives of Physical Health, Mental Health and Social Adaptability. Economic Res J 55(12):80–97. (in Chinese)
Wang ZX, Qi ZY, Zhu L (2021) Latitudinal and longitudinal variations in the impact of air pollution on well-being in China Environ Impact Assess Rev 90:106625
Wilkinson RG (1997) Socioeconomic determinants of health - Health inequalities: Relative or absolute material standards? Br Med J 314(7080):591–595
Woo B, Kravitz-Wirtz N, Sass V, Crowder K, Teixeira S, Takeuchi DT (2019) Residential segregation and racial/ethnic disparities in ambient air pollution. Race Soc Probl 11(1):60–67
Yang HY (2007) Equality research on the health of rural and urban residents. Financ Econ 03:69–75. (in Chinese)
Yang T, Liu W (2018) Does air pollution affect public health and health inequality? Empirical evidence from China. J Clean Prod 203:43–52
Yang W, Hu B (2022) Catastrophic health expenditure and mental health in the older Chinese population: the moderating role of social health insurance. J Gerontol Ser B-Psychological Sci Soc Sci 77(1):160–169
Yang ZM, Song QH, Li J, Zhang YQ, Yuan XC, Wang WQ, Yu Q (2021) Air pollution and mental health: the moderator effect of health behaviors. Environ Res Lett 16(4): Article 044005. 13
Yin P, Brauer M, Cohen AJ, Wang HD, Li J, Burnett RT, Stanaway JD, Causey K, Larson S, Godwin W, Frostad J, Marks A, Wang LJ, Zhou MG, Murray CJL (2020) The effect of air pollution on deaths, disease burden, and life expectancy across China and its provinces, 1990-2017: an analysis for the Global Burden of Disease Study 2017. Lancet Planet Health 4(9):E386–E398
Zhang J, Jiang Y-Z (2021) A study on mental health assessments of college students based on triangular fuzzy function and entropy weight method. Math Probl Eng 2021:1–8
Zhang LW, Chen R, Fang Y (2023) Effects of urban and rural resident basic medical insurance on healthcare utilization inequality in China Int J Public Health 68:1605521
Zhang X, Zhang X, Chen X (2017) Happiness in the air: How does a dirty sky affect mental health and subjective well-being? J Environ Econ Manag 85:81–94
Zhao Z, Lao X, Gu H, Yu H, Lei P (2021) How does air pollution affect urban settlement of the floating population in China? New evidence from a push-pull migration analysis. BMC Public Health 21(1):1696
Zheng Z, Zhang XB, Wang JM, Dandekar A, Kim H, Qiu YN, Xu XH, Cui YQ, Wang AX, Chen LC, Rajagopalan S, Sun QH, Zhang KZ (2015) Exposure to fine airborne particulate matters induces hepatic fibrosis in murine models. J Hepatol 63(6):1397–1404
Acknowledgements
This work is supported by the General Program of the National Natural Science Foundation of China (72274145, 72174149); the self-set project of the Key Research Institute of Humanities and Social Sciences of the MOE of China (24JDZS01).
Author information
Authors and Affiliations
Contributions
HYY: Conceptualization; Methodology; Resources; Writing - review & editing; Supervision, Project administration; Funding acquisition. LL: Conceptualization; Methodology; Formal analysis; Investigation; Data curation; Writing - original draft; Visualization; WJJ: Writing - review & editing. YY: Formal analysis; Writing-review. MXS: Investigation; Resources; Data curation. QY: Methodology, Writing-review.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
Not applicable.
Informed consent
The data used in this paper is based on secondary data, which has already been collected by Peking University. Therefore, I do not have any informed consent.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yang, H., Li, L., Jiang, W. et al. Air pollution, migrants’ health inequality, and China’s Cross-regional Medical Insurance Scheme: a moderating effect analysis. Humanit Soc Sci Commun 12, 1363 (2025). https://doi.org/10.1057/s41599-025-05502-7
Published:
Version of record:
DOI: https://doi.org/10.1057/s41599-025-05502-7
