
Abstract
Patient-generated health data (PGHD) from apps and wearables hold significant potential for enhancing personalised care and medical research. Healthcare professionals (HCPs) are key to its successful adoption, as their attitudes can either support or hinder its integration into clinical practice. This review systematically analysed studies on HCPs’ and researchers’ perspectives on PGHD for clinical and research use. Three databases were searched for articles published between January 2013 and April 2023. Of 246 articles screened, 33 met the inclusion criteria. While most participants viewed PGHD positively, concerns around data security, reliability, and workflow integration persist. Addressing these barriers is essential to maximising PGHD’s benefits for participatory medicine and improved clinical outcomes. The included studies presented medium methodological quality, particularly among quantitative and mixed methods with risks of sampling and nonresponse bias, and often low sample sizes in qualitative studies. However, recurring themes across studies allow a valuable interpretation of the findings.
Similar content being viewed by others

Introduction
If you are a physician or allied healthcare professional (HCP), you will likely have had patients present you with printouts of their app-generated health data reports or show you heart rate measurements on their smartwatches, often during time-pressured consultations. The rise of consumer health technologies, such as smartphone health apps and wearables with sophisticated sensors, has led to a new category of medical information: patient-generated health data (PGHD). In contrast to classic clinical data that is collected in clinical settings and interactions with care providers, PGHD are captured outside clinical care settings by patients1. Consumer health devices allow citizens to track various health and wellness parameters throughout their daily activities, including vital signs, lifestyle information and quality of life data1. Interpretive analysis of this data and actionable guidance holds the promise to support individuals in managing their own health2. The value of PGHD extends beyond individual patient care (primary use), as evidenced by the growing interest of researchers, policymakers and related stakeholders in using this data for secondary, population-benefit use cases such as medical research3. Digital infrastructures for a safe and secure exchange of digital health data are a prerequisite for its use and focus of many countries on their way to data-driven, digitalised healthcare systems. The recent EU policy initiative of the European Health Data Space (EHDS) is an example of this movement4. The EHDS aims to establish a data exchange platform for clinical data and PGHD across EU member states for primary and secondary use4.
Given the significant potential of PGHD in patient care and research, it is crucial to understand the attitudes and experiences of HCPs and research staff regarding its use. Several reviews have been conducted summarising research evidence in various areas of PGHD use, care impact and stakeholder opinions. One review looked at PGHD to measure real-world clinical outcomes and found that various PGHD types are currently explored in various disease indications, but their actual impact on health outcomes remains open5. Previous reviews have investigated the role of PGHD in clinical decision-making6 and the effect on the patient-provider relationship7. Our review complements existing literature by summarising opinions from HCPs and researchers from broad professional backgrounds and diverse clinical care settings towards using PGHD from apps and wearables for primary and secondary use. This includes anticipated benefits in care provision, patient management and clinical workflow. It further investigates barriers and concerns about using PGHD of the respective stakeholder groups.
Results
Search results
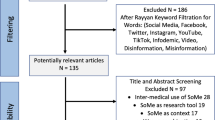
A total of 299 records were retrieved from the electronic databases PubMed, Embase, and Google Scholar (Table 1). After removing duplicates, 246 articles remained for the title-abstract screening, of which 25 were included for the full-text screening. Of these, 15 met the inclusion criteria8,9,10,11,12,13,14,15,16,17,18,19,20,21,22. Six additional articles were identified through a hand search on Google23,24,25,26,27,28 and 12 through reference tracking of included studies (forward tracking29,30,31,32 and backward tracking33,34,35,36,37,38,39,40). A total of 33 studies were included in the thematic analysis8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40. Title–abstract screening and full-text screening reasons for exclusion are summarised in Supplementary Information Table 2.
Characteristics of included studies and quality assessment
Table 2 summarises the key characteristics of the included studies. The complete data extraction including recruitment information, non-healthcare professional participant groups, data collection and analysis can be found in Supplementary Information Table 3. Of the 33 studies, 24 had a qualitative8,9,10,11,14,16,17,18,19,20,21,22,24,26,27,28,30,31,33,35,36,38,39,40, six a quantitative12,13,15,25,29,34 and three studies had a mixed methods study design23,32,37. Most qualitative studies (19/24) were based on interviews9,10,11,14,16,18,19,20,21,22,24,26,27,28,31,33,38,39,40, and the rest (5/24) used focus groups17,35, group discussions8,30 or a card-sorting session36. Mixed methods studies combined surveys with interviews (2/3)23,37 or focus groups (1/3)32. All quantitative studies were based on surveys for data collection12,13,15,25,29,34.
Most studies (22/33) recruited a mix of healthcare professionals for their data collection, including physicians, psychologists, therapists, and nurses among others8,9,10,11,13,16,17,18,20,21,22,25,28,31,32,33,34,38,39. Eight studies focused on physicians only12,15,19,24,26,30,37,40. Three studies specifically focused on the perspectives of researchers and will be separately analysed and can be found in the Supplementary Information Note 314,23,27.
Fifteen studies explored opinions toward health apps and/or wearables generally8,15,16,19,22,23,24,26,27,28,30,31,33,39,40, and 18 focused on a specific disease indication9,10,11,12,13,14,17,18,20,21,25,29,32,34,35,36,37,38, such as mental health conditions21,36 or cancer10,25.
Six studies9,11,18,28,37,38 investigated perspectives of HCPs within a clinical trial/research programme piloting apps and wearables for PGHD collection for patient care (Table 3). One study used a medical device app to monitor ECG in patients with Atrial Fibrillation38. Another study investigated a prototype medical device to monitor diabetes and two studies explored non-medical device data handling apps to track symptoms of rheumatoid arthritis based on validated questionnaires9 and an image-based wound healing tracker for post-discharge surgical site infection18. HCPs in those studies accessed the shared PGHD through web dashboards/portals18,38 or reports within9 or separate from the EHR37. Another study by the U.S. Department of Veterans Affairs piloted the fitness and activity tracker Fitbits for veterans that synced the PGHD via a data sync app to a web-based provider dashboard28. Another study interviewed HCPs from five different studies with focus on PGHD sharing. In these studies, PGHD were collected using various, unspecified consumer mHealth devices, with provider access either facilitated through a special dashboard/platform or at the patient’s discretion, e.g., during consultation on their device11. In 24 studies, the opinions on PGHD were assessed without actually sharing PGHD; of those, 23 did not differentiate the type of device for data collection.
Table 4 summarises the detailed quality assessment of all included studies. All studies passed the initial screening questions “Are there clear research questions?” and “Do the collected data allow to address the research question?”. The methodological quality of the included studies was medium. The most frequently found issue in studies with quantitative methods was the risk of sampling bias and non-response bias12,13,15,23,25,29,32,34,37. The most frequent issue with qualitative methods in studies was the underreporting of quotes to prove findings. Two studies stood out because of their very low number of HCP participants of five8,16,17,23,27,30 or two9, respectively.
Thematic synthesis
The thematic synthesis yielded a multitude of analytical themes that were grouped into five main categories: 1) Benefits of PGHD for patient care; 2) Improving patient management and clinical workflows; 3) Barriers to use PGHD; 4) Evolving roles of patients and HCPs in a changing healthcare system; and 5) Researchers perspectives on PGHD in medical research. The following sections describe the results for categories one to four. The fifth category is separately analysed and can be found in Supplementary Information Note 3.
Benefits of PGHD for patient care
HCPs in various medical specialities and professional groups across studies identified various benefits that access to outside-of-clinic PGHD from health apps and wearables could provide by filling long-existing gaps in the traditional clinical data. Figure 1a summarises the findings. Insights derived from PGHD can support the monitoring and understanding of disease progression and the overall health status (1)9,10,11,12,13,16,17,19,20,21,26,28,29,30,34,35,39,40. Continuous data collection can help to identify trends, triggers and behaviours impacting patient, health (2)9,10,11,16,20,21,22,28,32,35,37,38,39 Further, PGHD can be used to establish, monitor and adjust treatment plans (3)9,15,16,17,21,25,28,32,34,39, enabling collaboration between patient and provider to align and monitor the health goals of patients (4)16,17,21,22,28,38,39,40. PGHD utilisation is further seen as valuable for supporting lifestyle and behaviour changes and promoting prevention (5)15,19,20,30,40 and empowering patients to self-manage their diseases (6)10,11,12,16,17,19,22,28,29,30,34,35,37,38,39,40. In addition to its potential in patient care, HCPs in three studies also highlighted PGHD value for medical research (7)15,25,30. Two of those studies were quantitative: one with cancer care physicians found that 93% of participants supported using oncology app data for research25, and another with physicians from 36 different medical specialities found that 56% saw benefits or medical research15. Overall, HCPs found that PGHD utilisation offers significant benefits for both patient care and medical research by providing continuous, personalised health insights and fostering a collaborative approach to health management.

a displays benefits in patient care and (b) in patient management and clinical workflows. (Author’s summary).
Four studies quantitatively assessed which types of PGHD HCPs considered as useful. For this review, PGHD types rated as useful by at least 50% of the surveyed HCPs qualified for the reporting. For epilepsy patients, heart rate, sleep quality, body movement29,34, breathing rate, mood and concentration29 were identified as useful. Sleep quality was also considered valuable for mental health and multiple sclerosis patients29. In geriatric care, HCPs rated heart rate, blood pressure, blood glucose, weight, body fat, body/skin temperature, physical activity, sedentariness, step count and electrodermal activity as useful32. In a study involving oncology care physicians, useful features for an oncology app would allow the tracking of side effects, quality of life, test results, and treatment satisfaction25. A few studies report on patient-reported outcome measures (PROMs), a subset of PGHD that is collected through standardised and validated questionnaires10,11,21,24,25,32,33. One study with mental healthcare professionals highlighted the value of combining PGHD from different sources, e.g., PROMs and app behavioural data, for a holistic view of a patient’s health status21. In contrast, GPs in another study valued PROMs collected through their own clinical system more valuable than other types of patient-collected data, such as wearable data24. For oncology patients, app-collected PROMs such as quality of life25 and therapy-related measures10 were considered valuable. One study specifically excluded PROMs from their investigation11. Table 3 shows a summary of all devices and respective PGHD types shared and/or discussed in the studies.
Despite the anticipated benefits of PGHD in patient care, HCP participants across the studies expressed mixed opinions about its nature, including both actively- (user input) and passively-sensed data. GPs of one study equated heart and sleep data from wearables to verbal symptom descriptions, not as concrete measures24. Conversely, others viewed PGHD as a more objective and potentially accurate source of medical information20,26,35, comparing it to “hard data”28 and considering it less prone to recall bias35,37,39. This digital data can also help avoid “doctor-pleasing” bias, where patients report what they think physicians want to hear16,37. Some HCPs appreciated the subjective nature of PGHD as a feature, acknowledging that it requires an understanding of how individual patients express themselves39.
For instance, a cardiologist in the same study described that managing atrial fibrillation often relies on patients’ subjective symptom experiences39. Additionally, a HCP in another study found that PGHD can provide a holistic view of a patient’s daily life, offering insights beyond what can be discussed in a single clinical visit and fostering greater empathy with patients11.
Even when PGHD did not directly impact care plans37 or was not seen as valuable evidence24,35, HCPs still found it a useful starting point for patient conversations and setting the consultation agenda24,35,37. The initiation of the PGHD tracking itself can help HCPs understand intrinsic patient behaviour and motivation22,39.
Improving patient management and clinical workflows
In addition to its various benefits for patient care, HCPs across studies highlighted the potential of PGHD to enhance patient management and streamline clinical workflows. Figure 1b provides a summary of these findings.
In several studies, HCPs noted the utility of PGHD in preparing consultations. By tailoring appointments to specific patient issues identified in the PGHD, consultations could become more patient-centred and efficient9,10,20,22,25,29,37,40. For example, 77.8% of oncology care professionals in one study anticipated more efficient consultations with PGHD access25, while only 18% of HIV-care professionals in another study expected similar time savings12. In a study piloting a diabetes report, HCPs described a possible successful PGHD integration in clinical workflow by standardising and automating patient self-assessment and providing HCPs with a structured report, preferred directly in the EHR system before the consultation37. A study involving rheumatoid arthritis patients who tracked daily, weekly, and monthly symptoms in an app directly synced with the EHR found that accessing this data during consultations was considered useful by treating HCPs9. The longitudinal view of the patient’s health status provided by the app was seen as a potential time-saving alternative to standard disease history-taking during consultations.
HCPs in several studies identified the value of accessing PGHD between clinical visits. This data can help prioritise patients for follow-up visits and reduce unnecessary consultations18,19,25,29,31,35, freeing up crucial resources in an overburdened healthcare system. For example, HCPs considered post-discharge wound data tracked by at-risk-patients at home with their phone valuable for triage18. Additionally, PGHD can facilitate remote monitoring8,9,10,11,16,17,18,19,20,25,28,29,30,37,38,39,40, which is particularly useful for conditions like diabetes, where therapy adjustments can be made without in-person visits19,30. This approach helps manage increasing service demands and staff shortages effectively. Similarly to the diabetes case, a study on epilepsy, depression, and multiple sclerosis found that using patients’ devices to collect data at home and directly send it to the EHR system allowed for review between consultations if the system flagged reasons for concern29.
An important discussion point for many participants was the timing (when) and tool (how) for accessing PGHD. Many HCPs preferred access to the PGHD directly before a consultation20,34,37, while others favoured during the visit19,21,26,34,35 or in between appointments11,16,19,25,26,28. Regardless of timing, most HCPs who were open to using PGHD preferred it integrated into the electronic health records (EHR) to streamline their workflow8,9,10,11,15,16,17,18,19,20,21,22,25,28,33,37,39,40. Some suggested labelling PGHD separately from clinical data within EHRs28,33, though a minority preferred keeping raw PGHD out of the EHR28. Additionally, some HCPs were positive about accessing PGHD through patient portals16,22,33,34,38 or on the device during consultations19,21,22,25,26,34,39.
PGHD are often unfamiliar data types and structures for the HCPs, as they are collected with consumer health technologies that are designed for the general public, not a medical audience. Following from this, HCPs expressed the need to rearrange the data and allow tailored visualisation options to make the PGHD more comprehensive and actionable11,16,18,21,22,26,39.
Preferences ranged from summary reports with labels for highlights or out-of-range values18,26,37,40 to full data access28.
For remote access to PGHD, HCPs emphasised the need for clear protocols and responsibilities for dealing with incoming data and suggested building on existing workflow strategies18,22,25,34,37,40. Many called for dedicated nurses or care coordinators to pre-process PGHD before involving physicians8,17,18,22,25,29,34,37,40. Gerontologic care clinicians expressed a desire for decision support systems to pre-process data and issue alerts32. However, physicians in a study piloting a diabetes PGHD report preferred to receive the report directly37.
It is important to note that the report in this study was tailored to the specific information needs of the treating physicians. When oncology HCPs were surveyed about an alert feature in an app, 64.8% supported notifications for critical data entries25. Of those, 49% wanted an alarm for the treating physician within 24 to 48 hours, 40% preferred immediate alarms for the physician on duty, and 14% wanted an independent query system. Epilepsy care professionals were less supportive of real-time alarm systems, preferring to use PGHD for assessing seizure events before or during consultations rather than for real-time monitoring34.
Barriers to using PGHD in clinical practice
HCPs from various professional roles and medical specialities across studies, were enthusiastic about using PGHD to deliver better patient care, optimise patient management and streamline clinical workflows. However, the HCPs also reflected a variety of barriers and concerns when using this data. This shows a dual attitude of HCPs towards PGHD from health apps and wearables. Figure 2 summarises the barriers and concerns HCPs expressed in the studies included in this review.

HCP concerns on integrating PGHD into care. Synthesised summary of HCPs’ concerns regarding the use of PGHD in clinical practice. (Author’s summary).
A central barrier to HCPs was the quality and reliability of PGHD and the impact on data evaluation. Across studies, worries around data accuracy13,21,22,32,33,39,40, validity16,20,21,24,30,33,40, and reliability13,21,22,24,29,30,32,39,40 were found as a major concern, indicating an underlying mistrust in consumer technologies. On one hand, this is rooted in HCPs not knowing how the devices work and how they measure data. On the other hand, HCPs doubt patients’ ability to use the device correctly and trustworthy. Some HCPs feared that their patients could purposely try to manipulate the data to mislead physicians and force specific actions, e.g. a specific diagnosis or insurance premium32,39. Additionally, just like in classic therapies, digital approaches are facing big challenges in patient compliance. A non-compliant or discontinued use of the device could make the PGHD further unreliable, as some HCPs noted13,29,32,33,38,40. While access to more data is generally valued, HCPs in many studies are worried about data overload12,18,20,22,29,30,32,33,39,40. This could become particularly stressful for HCPs when patients gather data deemed to have no medical relevance8,19,20,22,24,25,32,33,39,40. Regarding passively sensed PGHD, HCPs expressed concerns about the missing contextual information, which makes it difficult to interpret the data36,39,40.
Another big concern theme was the integration of PGHD into current clinical practice. In several studies, HCPs noted that PGHD are not integrated into the current clinical workflow, e.g., missing interoperability with running information management systems in clinics10,11,16,18,26,39. It is time-consuming and burdensome for HCPs to assess PGHD in a separate software from their EHR system. Another barrier is the workload10,11,16,18,19,22,26,30,32,34,39,40 caused by the additional data. Processing and reviewing the data would require additional time and staff resources, especially in remote monitoring settings. Asynchronously sharing PGHD with HCPs brings the additional challenge of patients’ expectations on response time18,30,33,38 and HCPs noted the need for a clear alignment (and control over) when and how patients would receive a response to shared PGHD11,18,38.
Another important concern raised by HCPs in several studies that made the integration of PGHD in clinical routines difficult was the varying levels of digital health and data literacy among healthcare professionals, which can negatively impact how they interact with the tools and the data collected by patients21,24,25,35,40. On the other hand, patients lacking digital health literacy were also of concern, as this can result in wrong application usage or misinterpretation of data13,19,26,31,32,34,35,40.
While apps and wearables are often celebrated as empowering tools for patients, HCPs in several studies worried about their potential negative impact on patient health. HCP worried that PGHD tracking could lead to obsessive behaviour in some patients or exacerbate existing tendencies in others19,22,30,31,36,39,40. The tracking could become an additional work for patients who already deal with a severe condition20,40. Here, HCPs not only recognise their own extra work but also respect the workload on the patient site. A constant engagement with one’s own health status can also cause distress and anxiety16,18,29,30,31,36,38,40, for example, when data shows unfavourable behaviour of the patient or certain goals are not achieved. The increasing digitalisation of the healthcare and the patient-provider relationship was also negatively seen by some HCPs who worried about reduced personal contact of patients with their HCPs could have on them19,25,40.
Another set of concerns can be grouped as regulatory, legal and ethical concerns connected to using PGHD. An often cited concern by HCPs related to data privacy11,12,18,19,22,25,30,31,34,40, protection and security11,12,18,19,22,25,29 issues, such as third-party access and storage of PGHD from consumer mHealth devices. Some HCPs were generally worried by the idea of using tools from commercial companies, so the source of the app or device mattered to them10,19. HCPs in several studies were further concerned about medical liability, especially about their responsibility of reviewing large amounts of data or using the information for patient prioritisation10,12,18,19,24,25,33,40. Another important concern raised by HCPs in several studies is the fear of deepening social inequalities among patients with varying socio-economic levels10,13,19,34,37,40. Patients of lower socioeconomic status often have limited access to technology, including the internet and devices, and can lack the ability to use digital tools effectively. As a result, patients who would benefit the most can not participate or can participate less effectively. This could be further exacerbated in a scenario identified by HCPs in a Swiss study30. They worried that apps and wearables could be used by insurers to incentivise and reward “good patients” for achieving health goals while leaving other patients with higher needs for activation behind.
HCPs recommendation to address PGHD challenges
To address concerns around PGHD quality and reliability, HCPs in several studies demanded evidence proof for apps and wearables to be used in clinical care8,10,15,26,33. Making this information available to PGHDs would help them to identify appropriate tools and boost trust to use them with their patients. Greater involvement of HCPs in developing apps and devices could further enhance clinical usefulness13,30 and allow for the integration of customised features like tailored tracking features or data displays11,18,26,28,39.
To integrate PGHD in clinical workflows, the majority of HCPs wished to access the PGHD directly through their EHR system or patient portal15,17,18,20,22,25,28,32,33,34,37. HCPs in one study, however, expressed the need to clearly label the source of this information to differentiate it from other forms of clinical data33. For remote monitoring settings, HCPs suggested a dedicated nurse or care coordinator who could preprocess data and alarm physicians accordingly8,17,18,22,29,34. This suggestion builds on existing clinical structures where nurses are often the first point of contact for the patients. Clear reimbursement plans were also recommended by HCPs in several to compensate the extra work created by guiding patients in PGHD collection and using the data16,18,22,33.
Educational programmes for both HCPs and patients were identified as necessary to improve digital literacy15,26,29,30. For HCPs, this would enhance their ability to recommend and interact with PGHD tools, including data interpretation. For patients, these programmes could help to ensure correct usage and accurate data collection.
HCPs called for a clear regulatory framework addressing regulatory and ethical concerns such as data privacy and data security measures as well as third-party access to data19,30. Additionally, HCPs called for financial support to help patients from lower socioeconomic backgrounds to access PGHD tools31.
Evolving patient-provider roles in a changing system
Traditionally, the healthcare system has been dominated by paternalistic structures, with physicians being the primary decision-makers in patients’ care journeys. This is rooted in the belief that physicians possess superior medical knowledge and expertise, making them the most capable of judging what’s best for patients. However, in recent years, medicine has become gradually more participatory. This trend is supported by the emerging use of consumer health technologies that offer individuals unprecedented access to health information, health tracking features and personalised data insight reports. These advancements create opportunities for shared decision-making and a participatory approach to medicine, transforming the patient-provider relationship into a more equitable, empowered dynamic. HCPs in numerous studies in this review noted the potential of apps and wearables for collaboration on personal health goals and jointly deciding on PGHD to be integrated into care plans11,16,18,19,22,28,33,35,39,40. This approach effectively balances patients’ needs with clinical relevance while mitigating the risk of overburdening HCPs with excessive and unnecessary PGHD. However, acceptance of this approach varied depending on the clinical setting, highlighting the contrast between acute and paternalistic versus chronic and participatory medicine. For instance, physicians and cardiologists in two studies found limited utility of PGHD in acute or emergency care settings, where such data might impede timely care delivery24,40. Another study reported a lack of interest in PGHD from surgeons, whereas cardiologists found the data valuable and speculated that paternalistic structures may remain relevant in acute care settings but are outdated for long-term chronic disease management39. Given the increasing prevalence of chronic conditions and the subsequent rising demand for health services, engaging patients in proactive self-management will be crucial.
Some HCPs in chronic care20,37, acute, post-surgery care settings18 or not-specified care22 prefer to control which patients track what types of data to ensure medical relevance and integration into care plans, avoiding unnecessary workload18,20,22,37. They were holding on to traditional paternalistic thinking. Many HCPs also wanted only selected patients to share PGHD11,18,20,35,37. Suggested criteria included patients with memory issues35,37, poorly managed conditions11,37, patients at risk18, or with sufficient digital literacy20. HCPs emphasised the need to protect patients for whom an excessive focus on PGHD could be stressful19,22,29,30,39, particularly those predisposed to obsessive behaviour or mental disorders19,22,39. Some GPs expressed concerns about an emerging “entertainment medicine”, where healthy individuals who need it the least engage in excessive tracking and over-medicalisation of health40. Other GPs worried about “body estrangement” when measured data and bodily experiences do not match. Balancing these diverse perspectives is essential for the effective integration of PGHD into clinical practice30.
Discussion
This review summarises HCPs’ and researchers’ perspectives on integrating PGHD from apps and wearables into clinical practice and research. HCPs and researchers across various professional roles and medical specialities have high expectations for PGHD, particularly for its ability to provide novel insights into patients’ daily lives. This enriches the understanding of diseases and has the potential to improve patient care9,10,11,12,13,15,16,17,19,20,21,25,26,28,29,30,32,34,35,37,38,39,40. Identifying personal health goals in collaboration with the patient can encourage patients to greater ownership, self-management and compliance11,12,15,16,17,19,20,21,22,28,29,30,34,35,37,38,39,40. This is particularly important for ageing populations with rising prevalences of chronic diseases. However, the scientific evidence on the effectiveness of health apps and wearables is still limited and further research is needed41,42.
Using PGHD for remote check-in and prioritisation of care can reallocate staff and time resources in overstrained healthcare systems and enhance patient management and clinical workflows8,9,10,11,16,17,18,19,20,22,25,28,29,30,34,35,36,37,38,39,40.
PGHD from consumer health technologies presents several challenges. HCPs had major concerns regarding data quality, validity and reliability13,16,20,21,22,24,29,30,32,33,39,40. These concerns are not only rooted in a mistrust of the technology itself but also in patients’ ability to use the tools correctly, especially if they lack necessary digital health literacy13,29,32,33,39,40. Unfamiliar data types24,39 and unclear medical evidence8,16,26,30,33,39,40 further complicate the integration of PGHD. Additionally, missing integration in EHR systems10,11,16,18,20,21,22,26,39, along with concerns about data privacy, security, and protection11,12,18,19,22,25,29,30,31,34,40, poses significant barriers. Researchers further highlighted the importance of multidisciplinary teams14,27 and adaptation of protocols when working with PGHD16.
The benefits of PGHD, such as continuous monitoring, personalised treatment, and patient empowerment, align with evolving regulatory and policy frameworks aimed at enhancing patient-centred and data-driven healthcare, like the European Health Data Space4 or Health Data Usage Act43 in Germany. Moreover, integrating the large, diverse datasets collected through health apps and wearables with existing health data sets (e.g., clinical data) can support data-intensive secondary use cases such as medical research and health AI development44. The concerns among HCPs about the quality and reliability of the data from apps and wearables13,16,20,21,22,24,29,30,32,33,39,40 highlight the need for regulatory standards for consumer health technologies when data is supposed to be used for patient care or research. Regulatory bodies must establish and enforce guidelines for data accuracy, validation, and interoperability to address concerns. For instance, Germany developed an approach for apps on prescription, enabling app manufacturers to qualify for the statuary health insurance reimbursement scheme if the app meets the specific criteria on evidence, interoperability and data privacy and security45. It remains to be seen how the EHDS can fulfil the high expectations of HCPs, researchers, industry players and related stakeholders on a safe and secure data exchange platform.
Apps and wearables on the consumer health technology market are primarily designed to meet the needs of their (paying) end users, typically individuals from the general public. However, integrating these tools into clinical care requires a collaborative effort involving app manufacturers, HCPs, health systems, patients, and researchers throughout the product development cycle. Such collaboration can facilitate the creation of tools that are user-friendly, scientifically validated, and clinically relevant46. Figure 3 illustrates this collaborative ecosystem to leverage the potential of PGHD. These practices are more common in the development of medical device apps - apps with a medical intended purpose, such as diagnosis or treatment - that are regulated by medical device regulations (e.g., FDA in the USA or MDR in the European Union)47. In contrast, wellness or lifestyle tools, such as fitness trackers or sleep monitors, are not designed for specific medical indications or with HCPs in mind but remain the most widely used. Making such data accessible to patients and HCPs will require innovative approaches, and as part of these, it is likely that artificial intelligence will be used in the processing and appropriate contextualising of information. For example, customised smart algorithms in EHR systems could be utilised to highlight to HCPS out-of-range data from individual or combinations of wearable devices, thereby enhancing accessibility48.

A collaborative framework for patient-generated health data (PGHD) in healthcare and innovation. (Author’s summary).
As identified by HCPs in several studies10,13,19,30,34,37,40, ethical and equity concerns must be addressed, as they hold significant societal implications. Digital transformation has the potential to create more equitable access to healthcare, alleviating current barriers for underserved populations. But without clear policies and social support systems, it can also reinforce existing social, economic, and health disadvantages, for example for the elderly or people with disabilities, subsequently deepening the digital divide49. A current initiative by the United States Food and Drug Administration FDA explores how healthcare at-home settings have to be designed to allow integrated digital care with a particular focus on equity50. For PGHD to be effectively integrated into healthcare, reimbursement schemes must cover the costs of devices and training, ensuring inclusive participation. Additionally, safeguards must be implemented to prevent data exploitation by commercial entities providing devices and apps.
Our review adds valuable insights into the perspectives and everyday experiences of PGHD from apps and wearables among HCPs and researchers, contributing to the growing body of evidence in this area. A recent review specifically focusing on HCPs’ real-world primary use cases of PGHD identified three motivational areas of HCPs to use PGHD: supporting patients in self-management, enhancing the patient-provider-relationship and supporting HCPs in their clinical roles51. The findings of our review on anticipated patient care benefits, patient management and clinical workflows align and expand on those findings while additionally reflecting in depth on a variety of concerns and barriers to PGHD usage, for example, fundamental data work challenges and worries of an over-technologized approach to medicine with reduced in-person contacts that could negatively impact the patient-provider relationship. Those findings are consistent with those in other literature7. Hence, at the core of PGHD and participatory medicine paradigm is the principle of collaboration, which requires compromises on patient and provider sites to leverage its greatest potential. Digital transformation often necessitates a fundamental reworking of processes and structures, not merely the addition of new tools to existing clinical workflows. As healthcare becomes more data-driven, roles and workflows will evolve. While some patients will become more participatory on their own, it will be particularly important for physicians to activate the less engaged but who would benefit the most from digital health interventions. It will be important to educate HCPs and patients on digital health literacy13,15,19,21,24,25,26,29,30,31,32,35,40. This topic not only has to be more integrated into the medical study curricula and continued training of physicians52, but also in the training of non-physician care professionals53. They are often the first point of contact for patients and are crucial in guiding them on the digital journey.
The strength of this review is that it considers studies of a broad range of care settings (clinic and outpatient care), healthcare provider and researcher professions and medical specialities. It was further not restricted to a specific disease indication or purpose of PGHD collection. Overall, it summarises a variety of opinions from healthcare providers and researchers that hold valuable insights into motivations to use this data as well as concerns around this usage.
This review has some limitations. First, there is a risk of missing studies during the search, despite our efforts to minimise this by searching multiple databases and refining search terms. We piloted search terms and used various synonyms to maximise the sensitivity of the search. There might be studies on data from apps and wearables that use less common words for describing PGHD or tracking devices and were missed by our search strings. Second, we limited our search to English and German original research articles. Third, this review did not select studies only involving HCPs with experiences in PGHD usage, which may have introduced complexity due to a heterogenic experienced population. However, the analysis of the included studies showed similar benefits and barriers themes across all studies and stakeholders, suggesting a limited impact of this factor. As more apps and wearables are implemented in clinical care, focusing on assessing real-world experiences and needs might reveal additional insights.
Several areas require further investigation to optimise the use of PGHD. Longitudinal studies could investigate the impact on patient outcomes, cost-effectiveness and workflow efficiencies. Research could also focus on developing standardised protocols for data collection, validation and PGHD integration as well as the integration with clinical data. Comparing HCP perspectives before and after the COVID-19 pandemic could offer insights into shifts in attitudes and clinical workflow impacts.
PGHD from apps and wearables hold significant promise for advancing patient care, optimising clinical workflows and supporting medical research. Addressing the challenges identified by HCPs will be crucial for its successful integration into clinical practice. By focusing on regulatory needs, evidence generation, workflow integration, as well as HCP and patient education, stakeholders can work towards harnessing the full potential of PGHD while ensuring its safe and equitable use.
Methods
This review was registered with OSF (registration https://doi.org/10.17605/OSF.IO/PCZAU) and adhered to the Preferred Items for Systematic Reviews and Meta-Analyses statement (PRISMA)54. The PRISMA checklist can be found in Supplementary Information Table 1. Updates are accessible in the registry. Additional deviations to the protocol are listed in Supplementary Information Note 1.
Search strategy
The literature search was conducted between April 11 to April 24, 2024. We searched the databases Pubmed, Embase and Google Scholar with search strings considering variations of the terms “healthcare professionals”, “researchers”, “health apps”, “sharing” and “data” for publications published between January 2013 and April 2023. Complete search strings are shown in Supplementary Information Note 2. To supplement database searches, the reference lists of included publications were searched (backward citation tracking) and articles that referenced the identified publication (forward citation tracking), as well as an additional hand search with Google.
Eligibility criteria
Eligibility of records was assessed using the PICO framework to define inclusion and exclusion criteria based on the four key components: Population, Intervention, Comparison, and Outcome, and the additional criteria of Type of Study, Language of Publication, and Publication Date (Table 5).
Study selection and data extraction
After the search, all retrieved bibliographic data were imported to Rayyan55 and duplicates were removed. A test screening was conducted with 20 publications (8% of the total number of articles) to refine the inclusion criteria and ensure consistency among reviewers in the study selection. First, authors SB and OS independently screened titles and abstracts to find publications that meet the inclusion criteria. Second, SB and OS independently assessed full texts to identify eligible studies for inclusion in the review. SB and OS used a Google Survey Form and Excel to extract data from all included studies. Extracted data consisted of metadata of the article and information related to the research questions, such as study type, mHealth technology investigated, use cases, benefits and concerns. All extracted data can be found in Supplementary Information Table 3. Table 2 shows a summarised version of the extracted data.
Quality assessment
SB and OS independently assessed the quality of the included studies using the Mixed Methods Appraisal Tool (MMAT) Version 2018 (Table 4)56 Disagreements at any stage were resolved by discussion with SG.
Data synthesis and analysis
A data-based convergent synthesis design57 was used to analyse all included studies following a thematic synthesis approach. In this approach, all quantitative data (numerical results from quantitative and mixed methods studies) is transformed into codes and analysed with the qualitative data (qualitative results from qualitative and mixed methods studies). The thematic synthesis was performed based on the method by Thomas and Harden which includes line-by-line coding, grouping codes in descriptive themes and generating analytical themes58. The initial set of codes for the analytical themes was developed during the full-text screening. SB coded all studies using the software MaxQDA (VERBI Software GmbH). The data analysis followed an iterative approach, adding new codes every time a new theme was identified. After coding all articles, SB assessed the coding of all articles again to ensure consistency. Finally, analytical themes were identified and discussed among SB, OS and SG.
Data availability
All data generated and analysed during this study are included in the article and its Supplementary Information.
Abbreviations
- AF:
-
Atrial fibrillation
- AUS:
-
Australia
- BE:
-
Belgium
- CA:
-
Canada
- CGM:
-
Continuous Glucose Monitoring
- CH:
-
Switzerland
- DE:
-
Germany
- DK:
-
Denmark
- EHDS:
-
European Health Data Space
- EHR:
-
Electronic health record
- FR:
-
France
- GP:
-
General practitioner
- HCP:
-
Healthcare professional
- HIV:
-
Human immunodeficiency virus
- IRE:
-
Ireland
- MS:
-
Multiple sclerosis
- NL:
-
Netherlands
- PGHD:
-
Patient-generated health data
- PROMs:
-
Patient-reported outcome measures
- RA:
-
Rheumatoid arthritis
- UK:
-
UK United Kingdom
- USA:
-
United States of America
- VA:
-
U.S. Department of Veterans Affairs
References
Shapiro, M. R., Johnston, D. S., Wald, J. S. & Mon, D. T. Y. Patient-Generated Health Data. White Paper. https://www.healthit.gov/sites/default/files/rti_pghd_whitepaper_april_2012.pdf (2012).
Piwek, L., Ellis, D. A., Andrews, S. & Joinson, A. The rise of consumer health wearables: promises and barriers. PLOS Med. 13, e1001953 (2016).
Taylor, N. FDA qualifies Apple Watch AFib feature for use in clinical trials. MedTech Dive https://www.medtechdive.com/news/fda-apple-watch-atrial-fibrillation-medical-device-development-tool/715210/ (2024).
Proposal for a Regulation of The European Parliament and of the Council on the European Health Data Space. (2022).
Pyper, E., McKeown, S., Hartmann-Boyce, J. & Powell, J. Digital health technology for real-world clinical outcome measurement using patient-generated data: systematic scoping review. J. Med. Internet Res. 25, e46992 (2023).
Demiris, G., Iribarren, S. J., Sward, K., Lee, S. & Yang, R. Patient Generated Health Data Use in Clinical Practice: A Systematic Review. Nurs. Outlook 67, 311–330 (2019).
Lordon, R. J. et al. How patient-generated health data and patient-reported outcomes affect patient–clinician relationships: A systematic review. Health Inform. J. 26, 2689–2706 (2020).
Abdolkhani, R., Gray, K., Borda, A. & DeSouza, R. Quality assurance of health wearables data: participatory workshop on barriers, solutions, and expectations. JMIR Mhealth Uhealth 8, e15329 (2020).
Austin, L. et al. Providing ‘the bigger picture’: benefits and feasibility of integrating remote monitoring from smartphones into the electronic health record. Rheumatology 59, 367–378 (2020).
Berkowitz, C., Zullig, L. & Koontz, B. Prescribing an app? Oncology providers’ views on mobile health apps for cancer care. JCO Clin. Cancer https://doi.org/10.1200/CCI.17.00107 (2017).
Cohen, D. J. et al. Integrating Patient-generated Health Data Into Clinical Care Settings Or Clinical Decision-making: Lessons Learned From Project HealthDesign. JMIR Hum. Factors 3, e26 (2016).
Jacomet, C. et al. E-health. Patterns of use and perceived benefits and barriers among people living with HIV and their physicians. Part 2: Health apps and smart devices. Med. Mal. Infect. 50, 582–589 (2020).
Karduck, J. & Chapman-Novakofski, K. Results of the clinician apps survey, how clinicians working with patients with diabetes and obesity use mobile health apps. J. Nutr. Educ. (2018).
Keogh, A., Taraldsen, K., Caulfield, B. & Vereijken, B. It’s not about the capture, it’s about what we can learn”: a qualitative study of experts’ opinions and experiences regarding the use of wearable sensors to measure gait and physical activity. J. Neuroeng. Rehabil. 18, 78 (2021).
Kong, T., Scott, M. M., Li, Y. & Wichelman, C. Physician attitudes towards-and adoption of-mobile health. Digit Health 6, 2055207620907187 (2020).
Lavallee, D. C. et al. mHealth and patient generat ed health data: stakeholder perspectives on opportunities and barriers for transforming healthcare. Mhealth 6, 8 (2020).
Osborne, C., Juengst, S. Identifying user-centered content, design, and features for mobile health apps to support long-term assessment, behavioral intervention, and transitions of care in. Br. J. Occup. Ther. (2021) https://doi.org/10.1177/0308022620954115.
Sanger, P. C. et al. A patient-centered system in a provider-centered world: challenges of incorporating post-discharge wound data into practice. J. Am. Med Inf. Assoc. 23, 514–525 (2016).
Sarradon-Eck, A., Bouchez, T., Auroy, L., Schuers, M. & Darmon, D. Attitudes of general practitioners toward prescription of mobile health apps: qualitative study. JMIR Mhealth Uhealth 9, e21795 (2021).
Wendrich, K. & Krabbenborg, L. Digital self-monitoring of multiple sclerosis: interview study with dutch health care providers on the expected new configuration of roles and responsibilities. JMIR Mhealth Uhealth 10, e30224 (2022).
Wu, P., Zhang, R., Luan, J. & Zhu, M. Factors affecting physicians using mobile health applications: an empirical study. BMC Health Serv. Res. https://doi.org/10.1186/s12913-021-07339-7 (2022).
Zhu, H., Colgan, J., Reddy, M. & Choe, E. K. Sharing patient-generated data in clinical practices: an interview study. AMIA Annu. Symp. Proc. 2016, 1303–1312 (2016).
Bietz, M. J. et al. Opportunities and challenges in the use of personal health data for health research. J. Am. Med Inf. Assoc. 23, e42–e48 (2016).
Haase, C. B. et al. Data as symptom: Doctors’ responses to patient-provided data in general practice. Soc. Stud. Sci. 53, 522–544 (2023).
Kessel, K. A., Vogel, M. M. E., Schmidt-Graf, F. & Combs, S. E. Mobile apps in oncology: a survey on health care professionals’ attitude toward telemedicine, mhealth, and oncological apps. J. Med Internet Res 18, e312 (2016).
Nguyen, A. D., Frensham, L. J., Baysari, M. T., Carland, J. E. & Day, R. O. Patients’ use of mobile health applications: what general practitioners think. Fam. Pract. 36, 214–218 (2019).
Ostherr, K. et al. Trust and privacy in the context of user-generated health data. Big Data Soc. https://doi.org/10.1177/2053951717704673 (2017).
Saleem, J. J., Wilck, N. R., Murphy, J. J. & Herout, J. Veteran and staff experience from a pilot program of health care system-distributed wearable devices and data sharing. Appl Clin. Inf. 13, 532–540 (2022).
Andrews, J. A. et al. Making remote measurement technology work in multiple sclerosis, epilepsy and depression: survey of healthcare professionals. BMC Med. Inform. Decis. Mak. 22, 125 (2022).
Volpato, L., Del Río Carral, M., Senn, N. & Santiago Delefosse, M. General practitioners’ perceptions of the use of wearable electronic health monitoring devices: qualitative analysis of risks and benefits. JMIR Mhealth Uhealth 9, e23896 (2021).
Watt, A., Swainston, K. & Wilson, G. Health professionals’ attitudes to patients’ use of wearable technology. Digit Health 5, 2055207619845544 (2019).
Kim, B., Ghasemi, P., Stolee, P. & Lee, J. Clinicians and older adults’ perceptions of the utility of patient-generated health data in caring for older adults: exploratory mixed methods study. JMIR Aging 4, e29788 (2021).
Adler-Milstein, J. & Nong, P. Early experiences with patient generated health data: health system and patient perspectives. J. Am. Med. Inform. Assoc. 26, 952–959 (2019).
Bruno, E. et al. Wearable technology in epilepsy: The views of patients, caregivers, and healthcare professionals. Epilepsy Behav. 85, 141–149 (2018).
Huh, J., Le, T., Reeder, B., Thompson, H. J. & Demiris, G. Perspectives on wellness self-monitoring tools for older adults. Int. J. Med. Inform. 82, 1092–1103 (2013).
Kelley, C., Lee, B.& Wilcox, L. Self-tracking for mental wellness: understanding expert perspectives and student experiences. in Proceedings of the 2017 CHI Conference on Human Factors in Computing Systems 629–641 (Association for Computing Machinery, New York, NY, USA, 2017).
Nundy, S., Lu, C.-Y. E., Hogan, P., Mishra, A. & Peek, M. E. Using patient-generated health data from mobile technologies for diabetes self-management support: provider perspectives from an academic medical center. J. Diabetes Sci. Technol. 8, 74–82 (2014).
Reading, M., Baik, D., Beauchemin, M., Hickey, K. T. & Merrill, J. A. Factors influencing sustained engagement with ECG Self-monitoring: perspectives from patients and health care providers. Appl Clin. Inf. 9, 772–781 (2018).
West, P., Van Kleek, M., Giordano, R., Weal, M. J. & Shadbolt, N. Common barriers to the use of patient-generated data across clinical settings. in Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems 1–13 (ACM, Montreal QC Canada, 2018). https://doi.org/10.1145/3173574.3174058.
Gabriels, K. & Moerenhout, T. Exploring entertainment medicine and professionalization of self-care: interview study among doctors on the potential effects of digital self-tracking. J. Med. Internet Res. 20, e10 (2018).
Iribarren, S. J. et al. Effectiveness of mobile apps to promote health and manage disease: systematic review and meta-analysis of randomized controlled trials. JMIR Mhealth Uhealth 9, e21563 (2021).
Mattison, G. et al. The influence of wearables on health care outcomes in chronic disease: systematic review. J. Med. Internet Res. 24, e36690 (2022).
Bundesministerium für Gesundheit. Bundesgesetzblatt Teil I - Gesetz zur verbesserten Nutzung von Gesundheitsdaten - Bundesgesetzblatt. BGBl. 2024 I Nr. 102a 19.
Baumgart, D. C. An intriguing vision for transatlantic collaborative health data use and artificial intelligence development. npj Digit. Med. 7, 1–4 (2024).
DiGAV - Verordnung über das Verfahren und die Anforderungen zur Prüfung der Erstattungsfähigkeit digitaler Gesundheitsanwendungen in der gesetzlichen Krankenversicherung. https://www.gesetze-im-internet.de/digav/BJNR076800020.html.
Scheder-Bieschin, J. et al. Improving emergency department patient-physician conversation through an artificial intelligence symptom-taking tool: mixed methods pilot observational study. JMIR Form. Res 6, e28199 (2022).
Regulation (EU) 2017/ 745 of the european parliament and of the council - of 5 April 2017 - on medical devices, amending Directive 2001/ 83/ EC, Regulation (EC) No 178/ 2002 and Regulation (EC) No 1223/ 2009 and repealing Council Directives 90/ 385/ EEC and 93/ 42/ EEC.
Gilbert, S., Kather, J. N. & Hogan, A. Augmented non-hallucinating large language models as medical information curators. npj Digit. Med. 7, 1–5 (2024).
Saeed, S. A. & Masters, R. M. Disparities in health care and the digital divide. Curr. Psychiatry Rep. 23, 61 (2021).
Brückner, S., Brightwell, C. & Gilbert, S. FDA launches health care at home initiative to drive equity in digital medical care. npj Digit. Med. 7, 1–3 (2024).
Guardado, S., Karampela, M., Isomursu, M. & Grundstrom, C. Use of patient-generated health data from consumer-grade devices by health care professionals in the clinic: systematic review. J. Med. Internet Res. 26, e49320 (2024).
Sorg, H., Ehlers, J. P. & Sorg, C. G. G. Digitalization in medicine: Are German medical students well prepared for the future? Int J. Environ. Res Public Health 19, 8308 (2022).
Isidori, V. et al. Digital technologies and the role of health care professionals: scoping review exploring nurses’ skills in the digital era and in the light of the COVID-19 Pandemic. JMIR Nurs. 5, (2022).
Moher, D., Liberati, A., Tetzlaff, J. & Altman, D. G. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339, b2535 (2009).
Ouzzani, M., Hammady, H., Fedorowicz, Z. & Elmagarmid, A. Rayyan—a web and mobile app for systematic reviews. Syst. Rev. 5, 210 (2016).
Hong, Q. N. et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 34, 285–291 (2018).
Hong, Q. N., Pluye, P., Bujold, M. & Wassef, M. Convergent and sequential synthesis designs: implications for conducting and reporting systematic reviews of qualitative and quantitative evidence. Syst. Rev. 6, 61 (2017).
Thomas, J. & Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol. 8, 45 (2008).
Acknowledgements
This work was supported by the Federal Ministry of Education and Research (Bundesministerium für Bildung und Forschung) through the European Union-financed NextGenerationEU program under grant number 16KISA100K, project PATH - “Personal Mastery of Health and Wellness Data.” This work was supported by the European Commission under the Horizon Europe program as part of the Enhanced cybersecurity for networked medical devices through optimisation of guidelines, standards, risk management and security by design (CYMEDSEC) project (grant 101094218). The views and opinions expressed are those of the authors only and do not necessarily reflect those of the European Union. Neither the European Union nor the granting authorities can be held responsible for them. Responsibility for the information and views expressed herein lies entirely with the authors. The authors acknowledge the use of the ChatGPT language model (versions 3.5 and 4, OpenAI) for assistance with refining some of the text, and acknowledge the use of Canva in designing graphical elements.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
S.B., O.S. and S.G. were responsible for the study design of this review. S.F., M.S. and C.L. provided input to the concept and study design. S.B. and O.S. conducted the search, screening, data extraction and analysis. S.B. and O.S. conducted the quality assessment of the studies. S.B. wrote the first draft of the manuscript. O.S., S.G., S.F., M.S. and C.L. contributed to the writing, interpretation and editing of the manuscript. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
Authors SB, OS, SF, MS and CL declare no competing interest. SG has or has had consulting relationships with Una Health GmbH, 469 Lindus Health Ltd.; Flo Ltd, Thymia Ltd., FORUM Institut für Management GmbH, High-Tech Gründerfonds 470 Management GmbH, Ada Health GmbH, and he holds share options in Ada Health GmbH. SG is a News and Views Editor for npj Digital Medicine. SG played no role in the internal review or decision to publish this article.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Brückner, S., Sadare, O., Fesl, S. et al. Attitudes of healthcare professionals and researchers toward wearable and app derived patient generated health data. npj Digit. Med. 8, 186 (2025). https://doi.org/10.1038/s41746-025-01568-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41746-025-01568-4
This article is cited by
-
A user-driven consent platform for health data sharing in digital health applications
npj Digital Medicine (2025)
