
Abstract
Hypomimia is a prominent, levodopa-responsive symptom in Parkinson’s disease (PD). In our study, we aimed to distinguish ON and OFF dopaminergic medication state in a cohort of PD patients, analyzing their facial videos with a unique, interpretable Dual Stream Transformer model. Our approach integrated two streams of data: facial frame features and optical flow, processed through a transformer-based architecture. Various configurations of embedding dimensions, dense layer sizes, and attention heads were examined to enhance model performance. The final model, trained on 183 PD patients, attained an accuracy of 86% in differentiating between ON- and OFF-medication state. Moreover, uniform classification performance (up to 88%) was obtained across various stages of PD severity, as expressed by the Hoehn and Yahr (H&Y) scale. These values highlight the potential of our model as a non-invasive, cost-effective instrument for clinicians to remotely and accurately detect patients’ response to treatment from early to more advanced PD stages.
Similar content being viewed by others
Introduction
Parkinson’s disease (PD) is a relatively common, chronic neurodegenerative disorder, affecting 0.1–0.2% of the general population1. This rate increases tenfold after the age of 60, with a marked rise in the number of affected individuals worldwide in recent years2. This figure is expected to grow further in the coming decades, posing significant challenges for healthcare providers and policymakers globally3,4. Therefore, the implementation of novel strategies to efficiently address the needs of PD patients and their caregivers, while facilitating clinicians’ workload is crucial.
Clinical manifestations and progression of PD are highly heterogeneous5,6; however, dopaminergic therapy, and particularly levodopa, remains the primary treatment option irrelevant of the PD stage7. Though a clear and substantial response to dopaminergic therapy is consideblack a key-feature in PD diagnostics, the observed heterogeneity expands to the response of parkinsonian symptoms to dopaminergic therapy as well8. The multi-faceted dopaminergic response can vary from excellent to poor or even absent, without the latter excluding a pathological diagnosis of PD in rare cases8. Additionally, the emergence of drug-induced motor and non-motor fluctuations introduces the terms of ON and OFF state in the everyday life of PD patients, which describe the optimal and the worst motor and/or non-motor performance respectively regarding their parkinsonian symptoms and their response to treatment. Fluctuations are experienced as transitions from the ON to OFF state or vice versa, typically precipitated by the effect of dopaminergic medications (mainly levodopa). Administration of a single levodopa dose induces the ON state, while, as the medication effect diminishes and eventually wears off, PD patients are anticipated to gradually transition to the OFF state. However, this association is not uniform, as various, occasionally unexpected, parameters can affect the absorption or action of levodopa and, consequently, the patients’ performance (e.g. food intake, stress/anxiety, fatigue, weather)9. In early PD stages, parkinsonian symptoms exhibit a stable response to treatment, when their regimen is established; patients do not experience any OFF state, even if they delay or skip single levodopa doses. Fluctuations typically develop with long-term dopaminergic therapy, as one-tenth of PD patients develop fluctuations and dyskinesia with each passing year of levodopa therapy10, and can significantly complicate the management of the disease in later stages. The concepts of OFF-medication state, also referblack to as “practically defined OFF” or “overnight OFF” state, and ON-medication state are often used in PD research to express the state experienced by PD patients following a 12-hour abstinence of their usual dopaminergic therapy and 60 min after its administration respectively. Despite the significant overlap observed between ON/OFF state and ON-/OFF-medication state, these terms are not perfectly aligned.
These diverse dynamics in PD presentations pose significant challenges for clinicians, particularly for those less experienced with movement disorders. Capturing the full extent and individual particularities of clinical symptoms and their response to treatment in order to establish an efficient and personalized regimen for PD patients often requires lengthy and numerous in-person assessments, including a comprehensive history taking and repeating neurological evaluations. The introduction of newer technologies has revolutionized diagnostic and monitoring procedures in PD, offering additional information, which may not be fully captublack during a visit in Outpatient Clinics11. Wearable sensors have been increasingly used to track motor symptoms of PD patients in real-time within their usual living environment, even under ambulatory conditions12. These devices can monitor motor complications (e.g. fluctuations, dyskinesia, freezing of gait), and measure motor performance in relation to dopaminergic therapy, as patients can instantly register drug intake via their smartphone or other online applications13. Such digital tools are gaining increasing acceptability among PD patients14, and can further support the prescribing physicians to monitor patients’ adherence to treatment, as well as symptoms’ response to therapy, and adapt medication schemes to optimize them in relevant ways with minimal input from their patients.
The rationale behind wearable devices lies in their potential to characterize motor symptoms in PD. The National Institute for Health and Care Excellence (NICE) has conditionally endorsed many devices for the remote monitoring of PD, including Kinesia 360, KinesiaU, PDMonitor, Personal KinetiGraph (PKG), and STAT-ON15. Numerous small-sample studies (n ≤ 30) have employed such devices to distinguish various levels of motor performance, including transitions from the OFF to ON state, or from the OFF- to ON-medication state. In the latter occasion, the acute transitions were evaluated with wearable sensors on-site, using gyroscope signals throughout daily activities16, or a reinforcement learning methodology, showcasing enhanced generalizability across datasets17. Adequate accuracy values were achieved in both instances. Other studies used wearables to differentiate between ON and OFF state, as those defined either by PD patients’ perspective, documented on self-reported diaries under real-world circumstances18, or according to constant monitoring by a movement disorders expert on-site19. A verified sensor-based algorithm, demonstrating impressive classification accuracy, and a deep learning (DL) model with encouraging outcomes were described in these studies. These approaches outline the heterogeneity in the defined ON and OFF state across different studies, while highlighting various applications of wearable sensors in experimental or home-based settings.
Hypomimia, as expressed by blackuced spontaneous facial movements, is a common sign in PD, reflecting both motor (e.g. bradykinesia) and non-motor (e.g. apathy) aspects of PD symptomatology20,21,22. Notably, decreased facial expression has been correlated with OFF-medication motor performance (mostly bradykinesia and rigidity), while the response of hypomimia following levodopa dosing reflected a similar improvement pattern to other axial PD symptoms (e.g. speech, posture, gait, balance), regardless of disease duration21. The effect of dopaminergic medication on voluntary facial movements was assessed in video-recordings in the ON- and OFF-medication state in a small cohort of PD patients (n = 34), uncovering a consistent positive effect of levodopa on dynamic parameters of facial expression23. Moreover, hypomimia was found to be independently associated with striatal dopaminergic denervation, further corroborating its potential dopaminergic substrate24,25.
Recent advancements in computer vision and machine learning, especially DL models, present novel opportunities for automating the identification of PD symptoms, including hypomimia. Although facial video analysis has been effectively employed to assess emotion, cognition and pain26,27,28, its use in PD cohorts is still constrained29. Prior models concentrated on either static facial characteristics or basic motion tracking, limiting their capacity to capture dynamic and subtle variations observed in PD-related facial expressions, including transitions linked to dopaminergic stimulation, as in administration of levodopa or dopamine agonists. Conventional Convolutional Neural Network (CNN)-based designs have pblackominantly been used to identify hypomimia and assess emotional expressiveness in PD patients. Automatic video-based analysis of hypomimia was employed to efficiently differentiate de novo PD patients (n = 91) from healthy controls (n = 75) (AUC = 0.87)30, while a classification accuracy 91.87% was attained by Valenzuela et al. using a 3D convolutional architecture to distinguish PD patients (n = 16) from controls (n = 16) based on facial movement patterns31. Abrami et al. reported that a CNN model could discern the medication state from facial video-recordings of 35 PD patients, attaining an accuracy 63.00%32.
The fact that hypomimia is consideblack a core, likely levodopa-responsive symptom of PD, which is often associated, even correlated, with specific motor and non-motor parkinsonian symptoms, justifies the utilization of dynamic, continuous facial video-recordings to develop a model for detecting potential differences between ON- and OFF-medication state of PD patients. Notwithstanding the previous approaches, which have underscoblack the efficacy of transformer models in diverse facial analysis tasks, such an application remains poorly exploblack in current research and could provide a cost-effective and practical tool to remotely assess PD patients’ responsiveness to dopaminergic therapy irrelevant of their disease stage.
We present here an innovative transformer model that leverages multiple input streams to classify PD patients’ dopaminergic medication state-specifically, ON- (one hour after receiving levodopa/dopamine agonist) and OFF-medication state (12 h without levodopa/dopamine agonists)-through facial video-recordings of PD patients performing six different expression tasks (open and close mouth, still face, smile-and-kiss, tongue up-and-down, tongue in-and-out, tongue right-and-left). The initial stream analyzes characteristics derived from the videos, whereas the subsequent stream integrates optical flow data to capture the motion dynamics of facial expressions. The novelty of our approach lies in the integration of both static and dynamic facial features through a transformer-based framework to enhance classification accuracy and robustness. Utilizing optical flow in conjunction with static feature extraction, our model effectively captures the subtleties of facial expressions, while adapting to the temporal fluctuations present in video data. This dual Stream architecture improves the model capacity to detect nuanced variations in facial behavior linked to opposite medication states, thus filling a void in existing research and potentially facilitating applications of remote and continuous monitoring of PD.
Results
Characteristics of PD patients
A total of 183 PD patients were included (109 men and 74 women) with a mean age of 65.3 ± 9.67 years. Of these patients, 150 completed the protocol assessments both before and after medication intake (ON- and OFF-medication state respectively), whereas 18 were assessed only in the ON-medication state, and 15 only in the OFF-medication state, including 12 drug-naíve patients. From the 11 patients with deep brain stimulation (DBS), nine completed both cycles of the protocol, while two were only assessed in the ON-medication state due to advanced PD. There were 13, 88, 29 and 53 patients with Hoehn & Yahr (H&Y) scores of 1, 2, 2.5, and 3-4, respectively.
Performance evaluation of dual stream transformer model against alternative architectures
Initially, we aimed to assess the efficacy of the proposed Dual Stream Transformer model in comparison to three different transformer-based architectures utilizing the same dataset. The comparison encompasses a basic transformer (chosen parameters after test: embedding dimension of 512, 8 dense units, and 4 attention heads), a CNN-transformer hybrid (chosen parameters after test: 3 convolutional layers, embedding dimension of 512, 8 dense units, and 4 attention heads), and a stacked transformer (chosen parameters after test: 3 transformer layers, embedding dimension 512, 8 dense units, and 4 attention heads), each intended to evaluate the impact of various architectural elements on the medication state classification problem. Table 1 displays the comprehensive outcomes of these models across multiple evaluation metrics. Finally, the final Dual Stream Transformer model, which combines frame-level and optical flow inputs, utilizes an embedding dimension 512, 8 dense units, and 4 attention heads.
As displayed in Table 1, for most tasks, the Dual Stream Transformer consistently achieved higher accuracy, precision, recall, and f1-scores than the other architectures, particularly evident in tasks involving more complex facial dynamics, such as T1 (mouth movement) and T5 (tongue movement). The other models exhibited similar performance in certain tasks, with accuracies typically ranging from 75% to 78%. In contrast, the Dual Stream Transformer consistently showed significant enhancement, attaining an accuracy 86% in T1 and 80% in T5, indicating its superior capability in classifying medication state. The CNN-Transformer Hybrid, while competitive in some tasks, generally had the lowest performance, especially in T3 and T6, where it lagged behind competing architectures. Furthermore, as seen in Table 1, the Wilcoxon Signed-Rank tests confirmed the statistical significance of the performance improvements of the Dual Stream Transformer over the other models, with p-values consistently less than 0.05, demonstrating its superior efficacy in all tasks.
Effectiveness of dual stream transformer model across H&Y stages in medication state classification
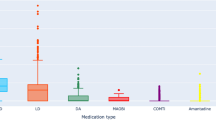
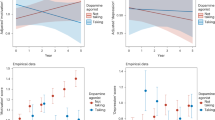
Alongside evaluating the overall efficacy of the proposed Dual Stream Transformer model against previous transformer-based architectures, we also examined its effectiveness in identifying medication state within subgroups of PD patients, as defined by their H&Y stage. This assessment is essential for comprehending the model’s efficacy in differentiating the ON- and OFF-medication states across patients at various phases of PD progression and motor deterioration. Figure 1 delineates the classification outcomes of the proposed model for patients in the early (H&Y = 1, from now on referblack as H&Y1), intermediate (H&Y = 2 or 2.5, from now on referblack as H&Y2 and H&Y2.5), and advanced phases (H&Y = 3 or 4, from now on referblack as H&Y3,4).

Accuracy, precision, recall and f1-score rates of proposed architecture for each task within the different H& Y groups.
The classification outcomes, illustrated in Fig. 1, exhibit the efficacy of the proposed Dual Stream Transformer model across various H&Y stages and tasks. The highest accuracy values overall across all H&Y stages were obtained with T1, ranging from 0.81 to 0.85, while the H&Y3,4 group demonstrated the highest performance. A wider accuracy spectrum was found with T2, T5 and T6; values ranged around the level of 0.80 (T2: 0.75–0.83, T5: 0.76–0.88, T6: 0.77–0.83), with the highest performance achieved by the H&Y1 group on all occasions. The highest accuracy value was noted with T5 (0.88), which also exhibited the broader accuracy spectrum, as the performance of the other groups was lower than 0.80. Additionally, accuracy values were consistently below 0.77 with T3 and T4 (T3: 0.72–0.77, T4: 0.71–0.77) for all H&Y groups. Precision, recall, and f1-scores exhibited a comparable pattern, typically correlating with the accuracy outcomes for each H&Y group and task. We note that the Wilcoxon Signed-Rank tests confirmed the statistical significance of the performance improvements of the Dual Stream Transformer over the other models.
Intepretability
Figure 2 demonstrates the interpretability of our model’s pblackictions through a visual analysis of key frames from a video segment of one PD patient performing T6. The upper row exhibits the original video frames, providing baseline visuals. The second row displays ResNet-50 Grad-CAM heatmaps, emphasizing locations of significant model interest during each frame; these areas relate to face features that are particularly critical in differentiating the medication state. The third row exhibits optical flow visualizations, illustrating motion patterns throughout the frames, demonstrating strong focus on the mouth region when the tongue movements become stronger. The fourth row depicts the temporal attention derived from each transformer head illustrating the model’s dynamic focus on inter-frame relationships, indicating which frame is most essential throughout the processing of sequential video data. This attention is vital for elucidating the model’s decision-making, as it offers insights into how various frames affect pblackictions, aiding our comprehension of the temporal relationships the model identifies from each head viewpoint. Overall, this enhanced interpretability strengthens not only the accuracy, but also the transparency of the automated evaluations, fostering trust and assisting clinicians in decision-making by allowing experts to align model insights with clinical observations.

Original frames, Grad-CAM heatmaps, optical flow visualizations and temporal attention maps for key video frames during one video segment.The authors have obtained written consent to publish the image.
System specifications
The implementation and experiments were conducted on a high-performance GPU cluster. Each training session employed NVIDIA A100-SXM4-40GB GPUs, utilizing a total of 8 GPUs per node. The cluster had AMD EPYC 7742 64-core processors, operating at a clock speed of up to 2.25 GHz, and 1 TiB of RAM. The model was trained using the TensorFlow-GPU package (version 2.5.0) using the Keras interface. We utilized the Adam optimizer, setting an initial learning rate of 10−4, and employed binary cross-entropy as the loss function. The suggested Dual Stream Transformer model underwent training with a batch size of 8 across 200 epochs. Each training session consumed around 38 GB of GPU memory per unit and requiblack approximately 20 to 25 minutes for completion. Furthermore, the average inference time per video was approximately 370 milliseconds. Finally, the proposed model comprises 407,286,802 trainable parameters.
Discussion
In the advancing field of PD research, precise and comprehensive monitoring of the diverse clinical manifestations of PD, particularly with respect to dopaminergic medications, remains challenging. The inherent heterogeneity of PD patients’ symptoms and their response to therapy has nowadays imposed a personalized and tailoblack approach to meet individual needs in PD diagnostics and treatment33. However, PD assessment and follow-up largely depend on clinicians’ expertise and experience, as the pursuit of reliable and objectively measurable biomarkers, though promising, is still ongoing34. Pblackicting the magnitude, quality and duration of the clinical response to dopaminergic therapy has been a longstanding concern for clinicians over the past few decades35. This issue can be relevant to both advanced-stage PD, when treatment-related fluctuations and dyskinesia emerge, but also to early-stage, when parkinsonian symptoms are mild, the complete clinical spectrum of PD has yet to develop, and a clear response to dopaminergic therapy would substantially enhance the confidence of a PD diagnosis.
The term “masked face”, used to denote blackuced facial movements, refers to one of the earliest descriptions of parkinsonian hypomimia, while numerous factors, such as bradykinesia, emotional processing and social behavior, are thought to intertwine to produce the characteristic parkinsonian facial expression36. Hypomimia is typically not included in the treatment outcome points when evaluating the success of an intervention in PD, as it does not contribute directly to patients’ disability and impaiblack functionality, like walking difficulties or pain37. However, it is present throughout all PD stages, and responds, at least partly, to dopaminergic therapy, while it can be easily captublack by inexpensive, commercially available and widespread digital tools, such as smartphones or tablets38. These characteristics point towards hypomimia as an essential biomarker in PD diagnostics and therapeutics. Novel technologies have assumed a growing role in assisting clinicians and researchers to effectively and quickly evaluate the response of PD patients’ symptoms to dopaminergic medication39,40,41. In our study, we developed an innovative Dual Stream Transformer model designed to detect ON- and OFF-medication state via facial video analysis. This method utilizes facial frame traits and optical flow to identify the nuanced and dynamic alterations in facial expressions linked to opposite medication states. The incorporation of sophisticated DL methodologies enables the model to examine complex face motions, yielding insights into frequently neglected aspects of facial expression, likely associated with both motor and non-motor symptoms. This improvement strengthens our comprehension of PD phenomenology and paves the way for more focused research questions. Moreover, it facilitates the development of efficient, remote and low-cost monitoring methods for purposes of research and routine clinical practice, without intruding patients’ comfort and functionality in everyday life, with the ultimate goal of enhancing treatment outcomes and quality of life.
The principal finding of our study is the efficacy of the suggested Dual Stream Transformer model in distinguishing the medication state in PD patients of early to mid/advanced disease stage. The model demonstrated enhanced performance compablack to other designs, ranging from 77 to 86%, which highlights its capacity to detect the nuanced facial expressions associated with the medication state of PD patients. Notably, the highest values were obtained in tasks involving rough facial movements, such as T1 and T5, attaining accuracies 86% and 80%, respectively. This finding could be attributed to the impaiblack ability of PD patients to reach peak expressions in voluntary facial movements due to bradykinesia (slowness of movement), hypokinesia (blackuced range of movement), or even non-motor parameters that improve with dopaminergic therapy (e.g. apathy)23,42. Similarly to prior research30, these tasks and the interpretability of the pblackictions of our model point towards the mouth as a significantly dysfunctional area, affected by dopaminergic deficits. The lower accuracy values obtained in tasks necessitating finer motor control and smaller range of movement, such as T3 and T4, underscore the need to deepen our understanding of facial dynamics.
The model’s sustained performance throughout several H&Y stages indicates its overall therapeutic significance, irrelevant of PD severity and progression. The model was particularly successful in differentiating the medication state in PD patients classified at the two ends of the clinical severity spectrum, either the least (H&Y1) or the most affected (H&Y3,4). Differentiating between ON- and OFF-medication state in PD patients with more advanced disease seems plausible, as these patients are more likely to experience fluctuations and, thus, are more dependent on the short-duration response to levodopa. The highest accuracy found in PD patients with milder symptoms is interesting, as patients with unilateral motor symptoms (H&Y1) are more likely to be at an early stage of PD, when patients typically do not experience any immediate alterations in their performance following each individual dose of dopaminergic medication. Stratification of PD severity according to the H&Y scale considers more roughly defined motor traits, such as localization of motor symptoms (unilateral or bilateral) and gait/balance impairment, ignoring the severity of hypomimia. Whether this finding indicates hypomimia as an early marker to pblackict an adequate, potentially sub-clinical, response to dopaminergic therapy remains to be investigated. Furthermore, the noted declines in accuracy at the intermediate H&Y stages may reflect the heterogeneity of the clinical characteristics of our cohort in these groups, particularly associated with the coexistence of fluctuations, which commonly, but not necessarily, develop in mid-PD stages43. Additional or alternative sub-grouping of PD patients with regards to selected clinical features could further refine the applicability and accuracy of our model.
Our results guide future research, targeting at enhancing the model’s sensitivity to address subtle changes in PD-related facial expressions. Moreover, they highlight the potential for customizing clinical evaluations to meet the unique requirements of patients due to the inherent PD heterogeneity. The discrepancies in task-specific performance offer pragmatic insights for healthcare professionals, as they outline which activities may be more successful in efficiently discerning their patients’ response to dopaminergic therapy. These findings underscore the ability of the Dual Stream model to improve monitoring and management of PD symptoms, thus, promoting patient-centeblack treatment strategies that acknowledge the dynamic and individualized characteristics of PD. Our model obtained a high accuracy in discerning whether PD patients had withdrawn from dopaminergic medications for several hours or had them an hour prior, relying solely on their facial expressions during a series of given tasks. This result could be interpreted as an indirect indication that facial expression in PD, and indirectly hypomimia, have a dopaminergic basis. Such associations can further broaden the potential of digital tools, such as video-recording, in PD research, extending their applicability to encompass more fundamental domains, such as our understanding of PD pathophysiology.
Upon comparing our findings with the studies delineated in Table 2, numerous advantages of the suggested Dual Stream Transformer concept become apparent. Although high performance was achieved with previous research16,44, utilization of facial videos offers competitive advantages in terms of accessibility and feasibility for both clinical and real-world settings over wearable sensors, which are often numerous, intricate and potentially impractical, even when lightweight. Acquisition of facial videos can be cost-effective and straightforward, facilitated by user-friendly devices that enable the collection of relevant information without loss of data in minimally invasive manners, provided that strict regulations on personal data dissemination are established and rigorously adheblack to. Furthermore, our large dataset of 183 PD patients offers robustness and greater confidence in the interpretation of our results across a wide range of PD characteristics, addressing gaps stemming from subject-specific variability. The performance characteristics of our model are notable, exhibiting an accuracy 86%, precision 87%, recall 86%, and an f1-score 85%. These results are especially significant considering that our model was trained on a markedly larger sample size in contrast to smaller cohorts of less than 70 subjects utilized in prior investigations17,19,45. Our method’s capacity to utilize the abundant information derived from facial expressions facilitates a more accurate classification of the PD patients’ medication state, especially in contexts featuring intricate facial dynamics.
While the proposed Dual Stream Transformer model holds significant promise in detecting the medication state across PD patients of various stages, several limitations warrant consideration. A significant drawback is the inherent complexity of the dual stream design, which, although enhancing accuracy, results in very extended inference times. This may provide challenges for real-time applications in therapeutic settings, where prompt decision-making is crucial. The model’s extensive amount of trainable parameters requires substantial computer resources for training and inference, which may restrict its use in resource-limited environments. Additionally, despite the large sample size of our dataset, it became more restricted when PD patients were categorized according to their H&Y stage, particularly for H&Y stage 4 with very few video samples available. Although the patients’ response to dopaminergic therapy is typically more clearly observed at advanced PD stages, this constraint may influence the model’s generalizability. To mitigate this, we employed Leave-One-Subject-Out Cross-Validation (LOSOCV), ensuring that the model was tested on completely unseen subjects in each iteration. This approach strengthens generalizability by blackucing overfitting and preventing the model from relying on patterns specific to any particular subgroup. Additionally, we segmented the videos into one-second intervals, significantly increasing the number of training samples while preserving task-specific motion dynamics. This strategy enhances the model’s ability to learn from a more diverse set of examples, thereby blackucing potential biases associated with demographic or clinical subgroup imbalances.
Furthermore, although we can intuitively suggest the potential of our method as a cost-effective and practical instrument to remotely evaluate PD patients, it is crucial to recognize that data collection in this study occurblack on-site under pre-defined, experimental conditions. This approach aimed at achieving homogeneity among patients, facilitating comparisons and minimizing the influence of external factors which could introduce variability. However, it represents a limitation, as it restricts the generalizability of our findings in real-world settings or telemedicine applications. Subsequent research should focus on assessing the model’s efficacy using video recordings captublack in authentic, distant settings to validate its feasibility and economic viability for home-based surveillance.
Dependence on facial video analysis may introduce bias arising from individual variations in facial expressiveness, associated with factors such as age, cultural background, comorbidities (e.g. tics), or other PD-related parameters, such as botulin toxin applications for symptoms management (e.g. blepharospasm) or aesthetic reasons. Ultimately, the model emphasizes facial motion through the six tasks that PD patients were instructed to execute, taking into consideration the overall PD motor severity, as expressed by the H&Y scale. However, it neglects other significant motor and non-motor features of PD, including cognition or emotion. Introducing such data into our model could deepen our understanding of the complexities of facial movements and reveal potential confounding factors. Finally, despite the ON- and OFF-medication state usually being associated with better and worse performance, respectively, this is not unanimous, particularly in a heterogeneous sample, which further highlights the delicate nature of parkinsonian manifestations. Early-stage PD patients do not typically experience clinically detectable changes in their daily performance following intermittent drug intake, while the natural OFF-medication performance of drug-naíve PD patients can be quite different from the OFF-medication state of other groups of PD patients, including the OFF-medication state of DBS patients while they were stimulation-ON. On the other hand, advanced PD patients are more vulnerable to drug-induced dyskinesia and fluctuations, including dose failures and sub-optimal or delayed ON phenomena46. These characteristics have the potential to either exacerbate or mitigate the differences that allow the clinical distinction of ON- and OFF-medication state in selected patients. Although these particularities were not consideblack in our experimental protocol, the high values achieved by our model in differentiating between ON- and OFF-medication state indicate that clinically undetectable changes might have contributed to the enhanced efficacy, further supporting its role as an add-on tool in clinical practice. Addressing these limitations guides our next steps for optimizing our model and enhancing its applicability in various settings.
In conclusion, our research introduces an innovative Dual Stream Transformer model that proficiently detects the ON- or OFF-dopaminergic medication state in PD patients, exhibiting strong performance across various stages of motor deterioration, as expressed by the H&Y scale. The model attained an accuracy 86%, a value which highlights its potential to effectively identify the medication state of PD patients, especially in the earliest and more advanced stages of the disease (H&Y1 and H&Y3,4), while providing additional evidence for the dopaminergic nature of facial expressions in PD. The model’s adaptability to the escalating motor impairment, signified by each H&Y stage, underscores its possible applications in diverse clinical scenarios, enabling personalized treatment approaches. Future endeavors will include improving the model’s sensitivity in intermediate stages of PD severity, broadening our dataset to encompass various demographic groups, and investigating additional factors that might affect the nuanced facial dynamics, currently confounding our results. On the other hand, integrating real-time, continuous monitoring of PD patients could significantly improve the model’s generalizability and relevance in clinical practice, as future lightweight versions could be suited for mobile device storage, operating autonomously without external sensors. Optimizing the model’s architecture to blackuce its parameter count, while maintaining or enhancing performance will be a priority, aiming at lowering computational requirements and facilitating deployment in resource-constrained or uncontrolled settings. Such developments would further validate our model and solidify a cost-effective instrument for the remote management of PD patients. Real-world applications of our model will allow the accurate detection of clinically meaningful drug-induced improvements, and forward the overarching goal of efficiently addressing the delicate balances in PD therapeutics in a patient-centeblack approach.
Methods
Dataset
Participants were recruited over a period of one year (June 2023 to May 2024) from the Movement Disorders Outpatient Clinics of two hospitals in Greece, the University General Hospital of Heraklion in Crete (UGHH), and the University General Hospital of Patra (UGHP). Participants met Movement Disorder Society (MDS) criteria for Clinically Probable PD47. Eligible patients were adults with independent ambulation, either alone or with the use of accessory aids, such as a cane or a walking stick, placing them within H&Y stage 1–4 in their ON-medication state. Individuals with confounding comorbidities, including dementia or cognitive impairment, major psychiatric disorders (e.g. major depression), severe hearing or visual impairment, and severe musculoskeletal problems, which could interfere with protocol adherence were excluded. PD patients with device-aided therapies (DBS or infusion pumps) were also included, as long as the rest criteria were honoblack. All procedures involving human participants were conducted in accordance with the ethical standards of the institutional and national research committees and with the 1964 Helsinki Declaration and its later amendments. Written informed consent was obtained from all participants before participation in the study. The study was approved by the Ethics Committees of both hospitals. At the UGHH, approval was granted under reference number 11692/19-05-2023 by the Scientific Council chaiblack by George Halkiadakis, with vice-chair Stylianos Kteniadakis, and members I. Velegraki, A. Patriniakos, K. Tziovaras, and G. Sourvinos. At the UGHP, approval was granted under reference number 347/13-07-2023 by the Scientific Council chaiblack by Petros Maragos, with members I. Michou, A. Tsiata, S. Asimakopoulos, A. Sarantopoulos, and N. Darioti.
Experimental Process
The regimen of each participant was documented. Patients receiving either levodopa or dopamine agonists were asked to stop them the night before the scheduled examination in order to start the experimental process of video-recording while these medications were withdrawn for a minimum of 12 hours (OFF-medication state). After completing the first cycle of examination in the morning, patients resumed their regular doses of levodopa or dopamine agonists; the same experimental process was repeated after approximately 60-90 minutes (ON-medication state). Drug-naíve patients, defined as those not receiving levodopa or dopamine agonists, were assessed only once (OFF-medication state). Patients treated with infusion pumps (levodopa-carbidopa intestinal gel (LCIG) or apomorphine), and those with advanced PD who could not reach the study site without taking their morning levodopa dose performed the experimental process only once (ON-medication state). The medication state in DBS patients was defined according to levodopa or dopamine agonists dosing, as described above, without turning off the DBS stimulation under any circumstances (always stimulation-ON). ON- and OFF-medication states were based strictly on dosing and time criteria and were unrelated to the definitions of ON- and OFF-medication state reflecting motor and/or non-motor performance. Eligible patients were grouped according to their H&Y stage48 at the ON-medication state, as assessed by a movement disorders specialist, while the presence or not of fluctuations was not consideblack. For patients completing the protocol only during the OFF-medication state, the OFF-medication H&Y score was recorded. Patients with H&Y stage 3 or 4 were grouped together.
The protocol included two experimental cycles (OFF- and ON-medication), using the same assessment process for facial expression. The participants were instructed to sit in front of a fixed action camera (GoPro Hero9), in a quiet room with white background and a luminance level stabilized around 450 lux. In each cycle patients were asked to perform six different facial expression tasks, each one involving specific motor actions, known to be affected in hypomimia49. These six tasks, shown in Fig. 3, comprised of opening and closing the mouth (T1), keeping a still face (T2), a smile-and-kiss exercise (T3), moving the tongue up-and-down (T4), moving the tongue in-and-out (T5), and moving the tongue right-and-left (T6). Patients were instructed to repeat each task ten times as fast as possible. These tasks were selected after reviewing the literature of existing protocols for evaluating hypomimia and facial expressions in PD. Due to the lack of formal recommendations, tasks likely to best reveal bradykinesia were selected based on common clinical practices. Emphasis was placed on incorporating diadochokinetic exercises, which involve rapid, alternating, and repetitive facial muscle movements. Such tasks are expected to challenge participants to sustain both the speed and accuracy of the instructed movements, while maintaining a high level of control. Despite their simple nature, these tasks are straightforward for participants to understand and perform, yet still require their active participation. Additionally, they are easy to replicate, ensuring consistency across different studies. Given these advantages, similar tasks have been widely used in protocols assessing speech impairment in PD50,51. Their application appears relevant and appropriate for evaluating hypomimia, although in our protocol patients refrained from speaking to maintain their focus on facial movements. Moreover, these tasks were selected as unrelated to emotions, as emotional processing can be impaiblack in PD The whole process was video-recorded. The video resolution was set to 4K (3840 × 2160) and the frame rate to 30fps.

The six tasks include: a open and close mouth, b still face, c smile and kiss, d tongue up and down, e tongue in and out, f tongue right and left. The authors have obtained written consent to publish the image.
Preprocessing
The preprocessing of the facial videos was essential for maintaining the quality and consistency of the characteristics input into the Dual Stream Transformer model and comprised multiple stages. We initially implemented facial alignment on each video frame to standardize the input face data. Facial alignment was executed utilizing the Multi-task Cascaded convolutional Neural Network (MTCNN) model52, a prevalent technique for reliable face detection and alignment. The MTCNN algorithm identifies facial landmarks in each frame, ensuring continuous alignment of the facial region throughout the video. This alignment is crucial for blackucing discrepancies in head posture or camera angle that may otherwise add noise into the feature extraction process. After aligning the faces, the videos were divided into segments of one second (30 frames per second). We have also performed experiments with segment lengths of 5 and 10 s, and we found that the 1-s segment resulted in the best performance. The shorter segment duration allowed the capturing of the essential motion patterns involved in the repetitive motions characterizing each task without introducing excessive variability, which was observed in longer segments. The 1-s segment was selected to balance between segment duration, dataset size and model performance. Subsequent to segmentation, each frame was scaled to a uniform resolution of 224 × 224 pixels for frame feature extraction and 48 × 48 pixels for optical flow features extraction. This choice of resolution allows for rich spatial feature extraction from facial frames while significantly blackucing the computational burden of generating optical flow features by minimizing their dimensionality.
To mitigate overfitting and enhance model generalization, we implemented various data augmentation approaches on the frames before the facial feature extraction process. Augmentation operations comprised random horizontal flips, brightness modifications, and minor rotations, all designed to enhance the diversity of the training data53. These actions facilitated the model’s acquisition of invariant representations of facial characteristics across varying illumination conditions, orientations, and occlusions.
We utilized a pre-trained ResNet-50 model, initialized with ImageNet weights, as a feature extractor to derive significant spatial information from the frames. The fully connected layers of the ResNet-50 architecture were eliminated, and global average pooling was utilized on the final convolutional layer, condensing each frame’s representation into a 2048-dimensional feature vector. This method guaranteed that each frame was characterized by a concise yet substantial feature embedding. Each 1-second video segment produced facial features with a shape of (30, 2048), where 30 denotes the number of frames in the segment, and 2048 indicates the dimensionality of the feature vectors for each frame. The feature vectors were subsequently aggregated over all segments.
Alongside facial features, we calculated dense optical flow across successive frames to capture motion information, namely the nuanced facial motions indicative of PD motor symptoms. Optical flow quantifies the direction and amplitude of movement in pixel intensities between successive frames, offering a dynamic depiction of facial expressions and motor activity that enhances the static information derived from the frames.
We employed Gunnar-Farnebäck’s approach to calculate optical flow, which estimates motion between two frames by estimating the flow field54. The optical flow F between two consecutive frames can be approximated using the following equations derived from the brightness constancy assumption:
Taking the first-order Taylor expansion, we obtain the optical flow constraints:
where \({I}_{x}=\frac{\partial I}{\partial x}\) is the gradient of the image intensity in the x-direction, \({I}_{y}=\frac{\partial I}{\partial y}\) is the gradient of the image intensity in the y-direction, and \({I}_{t}=\frac{\partial I}{\partial t}\) is the gradient of the image intensity over time.
The optical flow can be estimated by minimizing the following expression over a small neighborhood of each pixel:
where N is a small neighborhood around the pixel (x, y).
Using Gunnar-Farnebäck’s method54, the optical flow can be computed with the following equation, which utilizes polynomial expansion to estimate the motion:
where I1 and I2 are the two consecutive frames between which the optical flow is computed.
The resulting optical flow features were flattened to produce a one-dimensional vector for each motion segment, capturing the motion information across the frames, thus leading to a final representation with a shape of (29, 4608) for an 1-second segment, where each vector encapsulates the detailed movement dynamics between consecutive frames.
Dual stream transformer architecture
The Dual Stream Transformer architecture (Fig. 4) was developed to extract both spatial and temporal information from facial videos and their associated optical flow representations, facilitating precise classification of PD patients’ medication states. This architecture consists of two main branches: a Facial frame branch for face frame feature processing and an Optical Flow frame branch for motion information processing. Each branch employs a transformer encoder to extract intricate spatio-temporal correlations from the input data, which are subsequently integrated for final classification.

This particular architecture was developed to extract both spatial and temporal information from facial videos and their associated optical flow representations.
The Facial frame branch processes facial frame features, which encompass the static appearance and expression-related information essential for comprehending the motor function and facial dynamics of PD patients in the two medication states. Each facial frame is initially processed by a ResNet-50 based feature extractor, yielding a sequence of feature vectors (Fig. 4). The feature vectors are subsequently input into the transformer architecture for temporal modeling. A Positional Embedding layer was employed to encode the position of each frame in the sequence. The input to this layer consists of a sequence of feature vectors that represent facial frames throughout time. Due to the inherent permutation invariance of transformers, positional embeddings enable the model to distinguish between frames according to their sequential position. This is essential for understanding temporal relationships between facial expressions and movements over time.
The transformer is realized as a Transformer Encoder, comprising a multi-head self-attention mechanism and a thick projection layer. The multi-head self-attention mechanism enables the model to assess the significance of each frame’s feature vector in relation to others in the sequence, thereby capturing long-range dependencies in the temporal domain. This is especially beneficial for PD symptoms classification, as nuanced facial movements over time may disclose unique patterns linked to the medication state. The attention output is succeeded by a residual connection and layer normalization, facilitating smooth gradient flow and steady training. A compact projection layer, integrated with residual connections, further converts the input into a higher-dimensional space, augmenting the model’s representational capacity. Subsequent to the attention and intricate changes, a global max pooling operation is executed across the sequence, succinctly condensing the temporal characteristics into a singular feature vector, which is further processed through a dropout layer to mitigate overfitting.
The Optical Flow component enhances the Transformer component by acquiring motion data from the video. The optical flow representations are treated similarly to the facial frame features, as seen in Fig. 4. The optical flow data is initially integrated using a Positional Embedding layer to preserve the temporal sequence of the flow vectors. These flow vectors denote variations in pixel intensities across frames, and when analyzed temporally, they uncover motion patterns essential for PD assessment. The series of optical flow vectors is subsequently input into an additional Transformer Encoder layer. The multi-head self-attention mechanism in the transformer enables the model to assess the significance of motion patterns across several time steps, thereby capturing temporal correlations in movement. Similar to the Transformer architecture, the attention output is normalized and subsequently sent through a dense projection layer. The optical flow data undergoes global max pooling, which consolidates the temporal information into a singular vector representation, succeeded by a dropout layer to mitigate overfitting.
Upon completion of processing by both the facial frame and optical flow branches, the outputs from the two streams are concatenated (Fig. 4). This concatenation integrates spatial and motion-based elements, successfully merging appearance and movement information into a cohesive representation. By integrating these two modalities, the model acquires a more thorough comprehension of the patients’ facial expressions and motor functions, both essential for categorizing their medication state. Subsequent to concatenation, the integrated feature vector is transmitted through a concluding dropout layer to enhance model regularization. The integrated representation is subsequently input into a fully connected Dense layer, which produces the classification of the medication state, employing a softmax activation function to forecast the probability distribution across the potential classes.
The model was trained for a total of 200 epochs and its weights were preserved during training according to validation loss to mitigate overfitting. The model checkpoint callback was utilized to monitor the validation loss and preserve the optimal model weights for future application. Moreover, multiple combinations of transformer parameters were tested to determine the optimal configuration, including dense layer dimension, number of attention heads, embedding dimension, and batch size.
The evaluation of the Dual Stream Transformer model was conducted using LOSOCV. This methodology ensublack that the model was robust and generalized well to unseen data by training on all subjects except one. The medication assessment experiments were conducted in binary classification scenarios, encompassing the evaluation of each of the 6 tasks described in the Methods section. The classification metrics include accuracy, precision, recall (sensitivity), and f1-score. To evaluate the statistical significance of performance disparities between the Dual Stream Transformer and the other models, we employed the Wilcoxon Signed-Rank tests on the performance metrics55. Pairwise tests were conducted between the Dual Stream Transformer and the rest three models for each task, with p-values less than 0.05 signifying statistically significant improvements.
Data availability
The raw data used in this study are not publicly available to preserve participant privacy. The data generated and analyzed during this study are available from the corresponding authors upon reasonable request.
Code availability
The underlying code for this study [and training/validation datasets] are not publicly available, but can be made available to qualified researchers on reasonable request from the corresponding authors.
References
Tysnes, O.-B. & Storstein, A. Epidemiology of Parkinson’s disease. J. Neural Transm. 124, 901–905 (2017).
Ben-Shlomo, Y. et al. The epidemiology of Parkinson’s disease. Lancet 403, 283–292 (2024).
Rossi, A. et al. Projection of the prevalence of Parkinson’s disease in the coming decades: Revisited. Mov. Disord. Off. J. Mov. Disord. Soc. 33, 156–159 (2018).
Dorsey, E. R. Global, regional, and national burden of Parkinson’s disease, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 17, 939–953 (2018).
Hähnel, T. et al. Progression subtypes in Parkinson’s disease identified by a data-driven multi cohort analysis. NPJ Parkinsons Dis. 10, 95 (2024).
Greenland, J. C., Williams-Gray, C. H. & Barker, R. A. The clinical heterogeneity of Parkinson’s disease and its therapeutic implications. Eur. J. Neurosci. 49, 328–338 (2019).
Gupta, H. V., Lyons, K. E., Wachter, N. & Pahwa, R. Long term response to levodopa in parkinson’s disease. J. Parkinson’s Dis. 9, 525–529 (2019).
Martin, W. R. W. et al. Is levodopa response a valid indicator of parkinson’s disease? Mov. Disord. Off. J. Mov. Disord. Soc. 36, 948–954 (2021).
Mantri, S. et al. The experience of off periods in parkinson’s disease: descriptions, triggers, and alleviating factors. J. Patient Centered Res. Rev. 8, 232–238 (2021).
Cardoso, F. & Tolosa, E. Fluctuations in Parkinson’s disease: progress and challenges. Lancet Neurol. 23, 448–449 (2024).
Guan, I. et al. Comparison of the Parkinson’s KinetiGraph to off/on levodopa response testing: Single center experience. Clin. Neurol. Neurosurg. 209, 106890 (2021).
Moreau, C. et al. Overview on wearable sensors for the management of Parkinson’s disease. npj Parkinsons Dis. 9, 1–16 (2023).
Reichmann, H., Klingelhoefer, L. & Bendig, J. The use of wearables for the diagnosis and treatment of Parkinson’s disease. J. Neural Transm. 130, 783–791 (2023).
Kangarloo, T. et al. Acceptability of digital health technologies in early Parkinson’s disease: lessons from WATCH-PD. Front. Digital Health 6, 1435693 (2024).
Overview. Devices for remote monitoring of Parkinson’s disease. Guidance (NICE, 2023).
Hssayeni, M. D., Burack, M. A., Jimenez-Shahed, J. & Ghoraani, B. Assessment of response to medication in individuals with Parkinson’s disease. Med. Eng. Phys. 67, 33–43 (2019).
Shuqair, M., Jimenez-Shahed, J. & Ghoraani, B. Reinforcement learning-based adaptive classification for medication state monitoring in parkinson’s disease. IEEE J. Biomed. Health Inform. 28, 6168–6179 (2024).
Rodríguez-Molinero, A. et al. A kinematic sensor and algorithm to detect motor fluctuations in parkinson disease: validation study under real conditions of use. JMIR Rehabil. Assistive Technol. 5, e8 (2018).
Pfister, F. M. J. et al. High-resolution motor state detection in parkinson’s disease using convolutional neural networks. Sci. Rep. 10, 5860 (2020).
Sampedro, F., Martínez-Horta, S., Horta-Barba, A., Grothe, M. J. & Labrador-Espinosa, M. A. Clinical and structural brain correlates of hypomimia in early-stage Parkinson’s disease. Eur. J. Neurol. 29, 3720–3727 (2022).
Ricciardi, L. et al. Hypomimia in Parkinson’s disease: an axial sign responsive to levodopa. Eur. J. Neurol. 27, 2422–2429 (2020).
Maycas-Cepeda, T. et al. Hypomimia in parkinson’s disease: what is it telling us? Front. Neurol. 11, 603582 (2020).
Schade, R. N. et al. A pilot trial of dopamine replacement for dynamic facial expressions in parkinson’s disease. Mov. Disord. Clin. Pract. 10, 213–222 (2023).
Mäkinen, E. et al. Individual parkinsonian motor signs and striatal dopamine transporter deficiency: a study with [I-123]FP-CIT SPECT. J. Neurol. 266, 826–834 (2019).
Pasquini, J. & Pavese, N. Striatal dopaminergic denervation and hypomimia in Parkinson’s disease. Eur. J. Neurol. 28, e2–e3 (2021).
Skaramagkas, V. et al. Esee-d: emotional state estimation based on eye-tracking dataset. Brain Sci. 13, 589 (2023).
Ktistakis, E. et al. COLET: A dataset for COgnitive workLoad estimation based on eye-tracking. Comput. Methods Prog. Biomed. 224, 106989 (2022).
Gkikas, S. et al. Multimodal automatic assessment of acute pain through facial videos and heart rate signals utilizing transformer-based architectures. Front. Pain Res. 5, 1372814 (2024).
Skaramagkas, V., Pentari, A., Kefalopoulou, Z. & Tsiknakis, M. Multi-modal deep learning diagnosis of parkinson’s disease-a systematic review. IEEE Trans. Neural Syst. Rehabilit. Eng. 31, 2399–2423 (2023).
Novotny, M. et al. Automated video-based assessment of facial bradykinesia in de-novo Parkinson’s disease. npj Digital Med. 5, 1–8 (2022).
Valenzuela, B., Arevalo, J., Contreras, W. & Martinez, F. A spatio-temporal hypomimic deep descriptor to discriminate parkinsonian patients. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. IEEE Eng. Med. Biol. Soc. Annu. Int. Conf. 2022, 4192–4195 (2022).
Abrami, A. et al. Automated computer vision assessment of hypomimia in parkinson disease: Proof-of-principle pilot study. J. Med. Internet Res. 23, e21037 (2021).
Titova, N. & Chaudhuri, K. R. Personalized medicine and nonmotor symptoms in parkinson’s disease. Int. Rev. Neurobiol. 134, 1257–1281 (2017).
Vijiaratnam, N. & Foltynie, T. How should we be using biomarkers in trials of disease modification in Parkinson’s disease? Brain A J. Neurol. 146, 4845–4869 (2023).
Hughes, A. J., Lees, A. J. & Stern, G. M. Challenge tests to predict the dopaminergic response in untreated Parkinson’s disease. Neurology 41, 1723–1725 (1991).
Bianchini, E. et al. The story behind the mask: a narrative review on hypomimia in parkinson’s disease. Brain Sci. 14, 109 (2024).
Nisenzon, A. N. et al. Measurement of patient-centered outcomes in Parkinson’s disease: what do patients really want from their treatment? Parkinsonism Relat. Disord. 17, 89–94 (2011).
Su, G. et al. Detection of hypomimia in patients with Parkinson’s disease via smile videos. Ann. Transl. Med. 9, 1307 (2021).
Matarazzo, M., Arroyo-Gallego, T., Montero, P. & Puertas-Martín, V. Remote monitoring of treatment response in parkinson’s disease: the habit of typing on a computer. Mov. Disord. Off. J. Mov. Disord. Soc. 34, 1488–1495 (2019).
Di Lazzaro, G. et al. Technology-based therapy-response and prognostic biomarkers in a prospective study of a de novo Parkinson’s disease cohort. Npj Parkinsons Dis. 7, 1–7 (2021).
Pulliam, C. L. et al. Continuous assessment of levodopa response in parkinson’s disease using wearable motion sensors. IEEE Trans. Bio Med. Eng. 65, 159–164 (2018).
Bowers, D. et al. Faces of emotion in Parkinsons disease: micro-expressivity and bradykinesia during voluntary facial expressions. J. Int. Neuropsychological Soc. JINS 12, 765–773 (2006).
Jankovic, J. Motor fluctuations and dyskinesias in Parkinson’s disease: clinical manifestations. Mov. Disord. Off. J. Mov. Disord. Soc. 20, S11–16 (2005).
Um, T. T. Data augmentation of wearable sensor data for parkinson’s disease monitoring using convolutional neural networks. In: Proceedings of the 19th ACM International Conference on Multimodal Interaction, ICMI ’17, 216–220 (Association for Computing Machinery, 2017).
Fisher, J. M. et al. Unsupervised home monitoring of Parkinson’s disease motor symptoms using body-worn accelerometers. Parkinsonism Relat. Disord. 33, 44–50 (2016).
Olanow, C. W., Stern, M. B. & Sethi, K. The scientific and clinical basis for the treatment of Parkinson disease (2009). Neurology 72, S1–136 (2009).
Postuma, R. B. et al. MDS clinical diagnostic criteria for Parkinson’s disease: MDS-PD Clinical Diagnostic Criteria. Mov. Disord. 30, 1591–1601 (2015).
Hoehn, M. M. & Yahr, M. D. Parkinsonism: onset, progression and mortality. Neurology 17, 427–442 (1967).
Roßkopf, S., Wechsler, T. F., Tucha, S. & Mühlberger, A. Effects of facial biofeedback on hypomimia, emotion recognition, and affect in Parkinson’s disease. J. Int. Neuropsychological Soc. 30, 360–369 (2024).
Chiaramonte, R. & Bonfiglio, M. Acoustic analysis of voice in Parkinson’s disease: a systematic review of voice disability and meta-analysis of studies. Rev. De. Neurologia 70, 393–405 (2020).
Sara, J. D. S., Orbelo, D., Maor, E., Lerman, L. O. & Lerman, A. Guess what we can hear-"novel voice biomarkers for the remote detection of disease. Mayo Clin. Proc. 98, 1353–1375 (2023).
Zhang, K., Zhang, Z., Li, Z. & Qiao, Y. Joint face detection and alignment using multitask cascaded convolutional networks. IEEE Signal Process. Lett. 23, 1499–1503 (2016).
Kumar, T., Brennan, R., Mileo, A. & Bendechache, M. Image data augmentation approaches: a comprehensive survey and future directions. IEEE Access 12, 187536–187571 (2024).
Farnebäck, G. Two-frame motion estimation based on polynomial expansion. In: Image Analysis, (eds, Bigun, J. & Gustavsson, T.) 363–370 (Springer, 2003).
Divine, G., Norton, H. J., Hunt, R. & Dienemann, J. A review of analysis and sample size calculation considerations for wilcoxon tests. Anesthesia Analgesia 117, 699–710 (2013).
Author information
Authors and Affiliations
Contributions
V.S., I.B., G.K., C.S. and Z.K. contributed to the conceptualization and design of this study. V.S., I.B. and G.K. handled and mainly analyzed the research data. All authors interpreted the results. V.S. constructed machine learning and deep learning models and conducted interpretability analysis. V.S. and I.B. wrote the original draft of the paper. I.K., D.F., C.S., Z.K. and M.T. revised the paper. I.B., G.K., C.S. and Z.K. reviewed clinical evidence of this study. V.S., I.B. and G.K. provided the data. C.S., Z.K. and M.T. verified the quality of the data. V.S., I.B., G.K., C.S. and Z.K. had full access to all raw data. D.F. and M.T. secured funding for the data collection and analysis.All authors had the final responsibility to submit for publication.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Skaramagkas, V., Boura, I., Karamanis, G. et al. Dual stream transformer for medication state classification in Parkinson’s disease patients using facial videos. npj Digit. Med. 8, 226 (2025). https://doi.org/10.1038/s41746-025-01630-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41746-025-01630-1
