
Abstract
Newborns have an immature brain network responsible for speech processing that resembles the adult language network. However, it remains unclear how prenatal experience modulates this network. To test this, we exposed 39 fetuses to a story in their native language and in a foreign language during the last month of gestation, while another group of 21 fetuses received no experimental prenatal exposure. Within 3 days of life, neonates’ brain responses were recorded using functional near-infrared spectroscopy (fNIRS) whilst they listened to the same story in their native language and in two foreign languages, one of which neonates had been prenatally exposed to. Results revealed that brain responses to the native language and the prenatally exposed foreign language were similar, whereas they differed in the left temporal and right prefrontal regions when listening to a prenatally unexposed foreign language. Findings indicate that foetuses’ linguistic environment influences speech processing at birth.
Similar content being viewed by others


Introduction
In recent years, cumulative evidence helped to better understand the neurobiological foundations of humans’ language abilities1,2,3,4. The newborn brain has a functional network dedicated to speech and language processing that recruits very similar brain regions to those that are associated with adults’ language brain network. Many studies showed that, from birth, speech and language stimuli are processed in bilateral temporal and left inferior frontal areas5,6,7,8,9,10,11. Although some authors reported that newborns, as early as one day after birth, already show an adult-like left hemispheric dominance while processing their native language8,11,12, others reported more bilateral patterns of activation6,7.
An increasing body of literature suggests that speech perception and language processing are shaped by prenatal experience. By the end of the second trimester of pregnancy, fetuses’ auditory system is functional. Structural parts of the ears develop during the first 20 weeks of gestation, whilst the auditory system’s neurosensory part develops between 20 and 25 weeks of gestation13. The brain structures in charge of language processing, including frontal and temporal cortices, are already present and are functionally connected during the third trimester of gestation14. Fetuses are therefore extensively exposed to acoustic stimulation in utero14,15, unlike visual stimulation, which newborns are first exposed to after birth13. Although the pregnant person’s placenta and cardiovascular system provide internal background noise, external sounds with frequencies lower than 250–400 Hz are effectively transmitted through the womb16,17.
Insights from the prenatal period have helped understand the emergence of early brain specialization for voice, speech and language processing. Even before birth, fetuses close to term already show an orienting response towards familiar voices14,18,19. For instance, in utero exposure to a story that had been repeatedly recited by the pregnant person leads to a sustained heart rate deceleration compared to when read by a female stranger; a phenomenon that emerges in fetuses at 34 weeks of gestation20. Newborns also show a general preference toward familiar linguistic stimuli over unfamiliar ones as shown by variations in amplitude of sucking rate according to linguistic familiarity21,22. This early preference for familiar speech, voices, and sounds has also been reported in studies using neuroimaging techniques, including functional near-infrared spectroscopy (fNIRS) and electrophysiology (EEG). Neonates show differentiated brain responses when listening to their mother’s voice23 and speech24 compared to a stranger’s. Enhanced brain responses to the native language compared to unfamiliar languages have been observed in bilateral fronto-temporal areas in some studies6,7, whereas brain responses to the native language were more left-lateralized compared to unfamiliar languages in others11,25. A recent EEG study also reported that newborns showed increased activation and stronger long-range temporal correlations in their neural responses for several minutes after listening to their native language, but not unfamiliar languages, suggesting memory formation and learning for the native language following stimulation26.
The current evidence shows that fetuses and newborns can recognize languages they were exposed to in utero, as differential hemodynamic and electrophysiologic responses are observed when newborns listen to their native language compared to a foreign language. However, the specific cerebral response patterns underlying this ability have not been consistently identified across studies, as confounding results have been found6,7,11,25. Some studies drew their conclusions from observational data and others lacked control over newborns’ prenatal linguistic environment. Furthermore, generalizing the findings is challenging, as most studies focused on one unfamiliar language, with potential confounding effects from acoustic and rhythmical differences between languages, in addition to familiarity and prenatal exposition27. To our knowledge, only one research group has explored how prenatal exposure to musical and linguistic stimuli influences infants’ neural networks involved in auditory processing28,29. Using EEG, these studies showed that repeated exposure to a specific lullaby or the basic speech unit /ta/ during the final month of gestation could alter neural activity associated with the discriminative processing of these stimuli, with some effects lasting up to 4 months after birth. These findings imply that fetal brain development is finely tuned to its auditory environment. However, to what extent in utero experience-dependent plasticity also applies to language networks remains unclear.
To better understand the impact of language familiarity acquired in utero, we used fNIRS to study newborns’ brain responses as a function of language familiarity. This neuroimaging technique is particularly well suited for studies with newborns, infants and young children, as it is relatively tolerant to movements and allows the parent and an experimenter to be present with the child during data acquisition11,30,31. By measuring the absorption of near-infrared light projected through the scalp, fNIRS estimates variations in the concentration of oxygenated and deoxygenated hemoglobin in the blood32,33,34,35. Variations in blood oxygenation reflect underlying cerebral activation and can therefore be used as a proxy for brain activity in the cerebral cortex34,36,37.
French-speaking pregnant people were recruited when fetal gestational age (GA) was between 30 and 40 weeks. From 35 weeks of GA, a subset of pregnant people exposed their child to a story in their native language (French), and a foreign language (either German or Hebrew) using pre-recorded story segments and headphones placed on their abdomen, while participants recruited after 35 weeks of GA had no experimental prenatal exposure. This subgroup only listened to French in utero through their natural environment, without undergoing an experimental prenatal exposure procedure. Both foreign languages were selected for their different speech properties compared to the native language (French). German and Hebrew are stress-timed languages, whereas French is a syllable-timed language38,39,40. Furthermore, Hebrew and German have different phonological properties. Hebrew is more similar to French in that aspect, as both languages have similar vowel repertories41. Hebrew also implies iambic patterns (i.e., word-or-phrase-final stress)38,39,42, whereas German has word-initial lexical stress, such as trochaic patterns43. All stories were told by the same multilingual female speaker, fluent in all three languages.
Within 3 days after birth, all newborns listened to the same story segments in the three languages (Figs. 1 and 2). Thus, German and Hebrew were each other’s controls, as each of the two languages was foreign, but prenatally exposed for some of the participants, and totally unfamiliar to others. The control group received no prenatal exposure to either Hebrew or German, only to French through their unilingual familial environment. Although left-hemispheric language lateralization of brain responses to the native language has not been systematically observed across studies, we expected to find stronger brain responses in left temporal areas for the native language compared to the unexposed foreign language11,25. Furthermore, we aimed to explore whether newborns exposed prenatally to a foreign language exhibited different patterns of brain responses compared to their native language and to a completely unexposed foreign language. We hypothesized that the brain responses to the native language would be more left-lateralized than the brain responses to the prenatally exposed foreign language. In turn, brain responses to the exposed foreign language would be more left-lateralized than the responses to the unexposed foreign language, but less so than that of the native language.

Timeline of recruitment, prenatal linguistic exposure according to fetal gestational age (GA) and fNIRS recording during a passive listening story task within 3 days after birth. Participants recruited after 35 weeks of GA underwent no prenatal exposure to German or Hebrew.

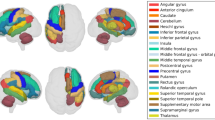
A A newborn participant with the fNIRS headgear in their crib. B Probe placement and their approximate spatial projection onto a newborn MRI brain template. Coupling of light sources (red dots) and detectors (black dots) yielded a total of 72 channels (colored lines). Colors represent the six regions of interest (ROI) subdivisions identified in the left (LH) and right (RH) hemispheres based on anatomical landmarks and 10-10 coordinates82. C Example of the experimental paradigm. The three languages were presented in blocks of three consecutive story segments of the same language (French (FR) in black, German (GE) in red, and Hebrew (HE) in blue). The order of the languages was randomized and counterbalanced across participants.
Results
Concentration changes according to language familiarity at birth
Figure 3 shows the mean oxyhemoglobin (HbO) concentration changes in response to language familiarity for each region of interest (ROI) based on the prenatal exposure condition (native, exposed, or unexposed). An increase in HbO concentration was seen for channels located in the left temporal regions in response to the native and exposed conditions (see Fig. 2B for channels and ROI distribution). In the right hemisphere, brain responses revealed a decrease of HbO concentrations in the prefrontal region in native and exposed conditions, whereas there was no significant change in HbO concentration in the unexposed condition. Note that HbR hemodynamic changes over time and statistical analyses results on HbR data are reported in Supplementary Materials (Fig. S1). Supplementary Table S1 shows hemodynamic HbR concentration mean and standard error estimates for all exposure conditions, ROIs and hemispheres.

A Topographical representation of mean HbO concentration changes according to language familiarity for the native (n = 60), exposed (n = 39) and unexposed (n = 60) language conditions. Front (F) and back (B) of topographical representation are indicated for left and right hemispheres. B HbO concentration changes for Native in blue, Exposed (German or Hebrew, depending on the prenatal linguistic group) in cyan, Unexposed (Hebrew or German, depending on the prenatal linguistic group) in green. Channels are plotted following the headgear placement shown in Fig. 2 for the left and right hemispheres. The black vertical lines indicate the onset of the stimulation period. An asterisk (*) over a region indicates significant (P < 0.05) differences between native and unexposed conditions.
The influence of prenatal experience on hemodynamic responses
A repeated measure ANOVA on the HbO concentration changes, as it is known to be more sensitive than HbR to blood oxygenation changes related to brain activity44,45, with the between-subject factor Condition (Native, Exposed, Unexposed) and the within-subject factors ROI and Hemisphere revealed a main effect of Hemisphere (F1, 156 = 18.433, P < 0.001, effect size = 0.106), a significant effect of ROI (F3.856, 152 = 4.014, P = 0.004, effect size = 0.025), and a significant triple interaction (F8.53, 153 = 2.617, P = 0.007, effect size = 0.032). Post hocs for the triple interaction are described below.
Post hoc analysis for Condition revealed no significant difference between the native and exposed condition, nor between exposed and unexposed conditions. A significant difference (P = 0.018) was found between native (0.034 ± 0.011) and unexposed language (−0.010 ± 0.011) in the temporal left region. A significant difference (P = 0.045) in the right prefrontal region was found between the native condition (−0.038 ± 0.010) and the unexposed condition (−0.004 ± 0.011) (Figs. 3 and 4).

Data of hemodynamic HbO concentration changes were plotted in box plots for the three exposure conditions and six ROIs, in the left hemisphere (left panel) and in the right hemisphere (right panel). The white diamonds show the mean of the data. Black arrows indicate significant post hoc differences between native and unexposed conditions. An asterisk (*) over a region indicates significant (P < 0.05) hemispheric differences for the native and the exposed conditions in the posterior temporal, temporo-parietal, prefrontal, and posterior frontal regions. No hemispheric differences were found for the unexposed condition. Blue arrows show significant differences between regions within the same hemisphere for the native condition. Hemodynamic HbO concentration mean and standard error estimates for all exposure conditions, ROIs, and hemispheres are available in Supplementary Table S2.
Post hoc analysis on Hemisphere revealed a left-greater-than-right response for the native language condition in the temporo-parietal (L = 0.014 ± 0.011 > R = −0.031 ± 0.012; P = 0.004), prefrontal (L = 0.028 ± 0.009 > R = -0.038 ± 0.010; P < 0.001) and posterior frontal (L = 0.015 ± 0.009 > R = −0.014 ± 0.009; P = 0.032) regions. The exposed condition also showed a significant left hemispheric dominance in the posterior temporal (L = 0.023 ± 0.014 > R = −0.048 ± 0.014; P < 0.001), temporo-parietal (L = 0.001 ± 0.014 > R = −0.047 ± 0.014; P = 0.013) and posterior frontal (L = 0.022 ± 0.011 > R = −0.012 ± 0.011; P = 0.042) regions. No significant hemispheric difference was found in the unexposed condition.
Post hoc analysis on ROI showed that, in the native condition, the hemodynamic concentration change in the left temporal region (0.034 ± 0.011, P = 0.002) was higher than in the left posterior temporal region (−0.017 ± 0.012). In the right hemisphere, concentration measures in the temporal region (0.017 ± 0.011) were significantly higher than in the posterior temporal (−0.034 ± 0.011; P < 0.001), temporo-parietal (−0.031 ± 0.012; P = 0.011), and prefrontal (−0.038 ± 0.010; P = 0.007) regions. Furthermore, the inferior frontal region (0.011 ± 0.011; P = 0.001) showed significantly higher hemodynamic concentration change than the prefrontal region (−0.038 ± 0.010). None of the post hoc analyses on ROI was significant for the exposed and unexposed conditions.
It is noteworthy that correlational analyses between the amount of prenatal exposure and the amplitude of the HbO concentrations revealed no significant correlation (P < 0.05) in any ROI for both hemispheres, and for each language familiarity condition. Although the goal of the present study was to investigate the impact of language familiarity on brain responses at birth, Supplementary Table S3 reports the means and standard errors for native (French) and foreign (Hebrew and German) languages, irrespective of prenatal exposure, as well as the interaction effects between conditions. Table S4 show the means and standard errors for German and Hebrew, regardless of the prenatal exposure groups. Both tables have been included in the Supplementary Materials as it may be of interest to readers studying bilingualism or the neural processing of different languages.
Discussion
The current study aimed to better understand how the linguistic environment influences brain responses at birth and to investigate the impact of language familiarity on newborns’ brain responses. To do so, fetuses from monolingual French-speaking families were recruited. A subset of fetuses was exposed in utero to linguistic stimuli in their native language (French) and a foreign language (German or Hebrew) during the last month of pregnancy. The same linguistic stimuli were presented in the three languages to all newborns in the first days following birth, while their brain responses were recorded using fNIRS. Data collected at birth were then analyzed according to exposure conditions to the speech stimuli; native, prenatally exposed, and unexposed languages. A control group only listened to French in utero through their natural environment, without undergoing an experimental prenatal exposure procedure. Therefore, their data were only analyzed as part of the native condition (when listening to French) or unexposed condition (when listening to Hebrew and German).
A key finding of our study is that the experimental manipulation of fetuses’ prenatal linguistic experience through a short but repetitive exposure to a new language triggered a similar response in the left temporal region than that of the native language at birth. Our results provide evidence that even brief prenatal exposure to a foreign language could make it recognizable to neonates, leading to brain activation patterns similar to those observed when listening to their native language. The brain responses to the prenatally exposed foreign language were not significantly different from the responses to the native language. However, significant differences in brain responses were found between the native and the unexposed foreign language conditions (Fig. 4). Studies have reported that near-term fetuses can perceive speech during the last weeks of gestation and show differentiated responses toward familiar voices18,19,20. The stronger brain responses found in the left temporal region when listening to the native and the prenatally exposed foreign languages compared to the unexposed foreign language may indicate prenatal learning. As the left hemisphere is known to be predominantly recruited in speech memory and learning in newborns46,47,48, it is possible that prenatal learning of the native and exposed stories occurred in utero.
Furthermore, a decrease in HbO concentrations in the right prefrontal region was significantly greater in the native condition than in the unexposed condition. Although difficult to interpret, this finding might be associated with a form of recognition for the native language. In another fNIRS study comparing 3-month-old infants’ brain responses to a habituated syllable /ba/ and a novel syllable /pa/, it was found that the temporal regions were activated in response to the familiar, repetitive syllable. In contrast, prefrontal activation was observed when infants listened to a novel syllable49. The authors suggested that the prefrontal cortex is involved in the perception of invariance and novelty in the infant’s environment. In comparison, our results show a decrease in HbO concentrations in the right prefrontal region when neonates listened to their native language, compared to when they listened to an unexposed foreign language. Habituation is considered to be a basic form of memory and learning50. While our study was not designed to assess brain responses to habituated stimuli, these findings may be explained by the possibility that the right prefrontal cortex is involved in a form of recognition or prenatal learning of phonemes belonging to the newborns’ native language.
No differences were reported between brain responses in the native condition and the exposed condition. These results suggest that brief prenatal exposure to a foreign language leads to a pattern of brain activation that is no longer significantly different from the brain response to the native language. Overall, it supports the hypothesis that prenatal exposure leads to the recruitment of brain networks that are similar, or at least do not differ from those activated by the native language.
Our results also showed that language processing at birth engages a fronto-temporal network, with distinctive response patterns across hemispheres and regions based on language familiarity. Significant differences in brain activation between homologous regions were present only in native and exposed conditions (Fig. 4). Our findings suggest that an early left hemispheric specialization is already present within the first few hours after birth, encompassing not only the native language but also other languages to which fetuses were regularly, although relatively briefly, exposed during the latter stages of pregnancy. The current hemispheric asymmetry found in our study concurs with findings from others highlighting a structural and functional left lateralization to native speech at birth and during early postnatal development8,11,48,51,52. Not only do these results support previous work showing that brain responses to native language are already left lateralized at birth11,25, they also suggest that left hemispheric lateralization of language processing at birth can occur even as a result of relatively brief prenatal input. Therefore, brief prenatal exposure to linguistic stimuli could modify newborns’ language brain networks. Although our results are in line with those observed by other groups, it is important to note that some studies have also found that listening to the native language activated bilateral fronto-temporal brain regions6,7. These contrasting results could be in part explained by the lack of systematization across methods, smaller sample sizes, the fact that brain activation in response to one foreign language was compared to the native language, and that native languages varied across studies (Japanese, French, and English)6,7,11,25.
The present study has certain limitations that should be recognized. First, our relatively small sample size limits the level of detection to a medium-sized effect, while hundreds of participants would be required to detect small-sized effects. Sample size also precluded us from comparing brain responses to each foreign language in exposed and unexposed conditions. Moreover, as some participants were recruited after 35 weeks of gestational age and were not prenatally exposed to a foreign language, we have a smaller sample size in the exposed condition compared to the unexposed and native conditions. This could have had an impact on our results, as some small effects might have been observed if we would have had equivalent sample sizes for all conditions. To assess the impact of including participants who did not receive prenatal exposure, a repeated measure ANOVA with the between-subject factor Condition (Native, Exposed, Unexposed), and the within-subject factors ROI and Hemisphere was conducted only with participants that had received prenatal exposure. Results are presented in the Supplementary Table S5 and followed the same pattern as those obtained with the full sample.
In the native condition, participants had different levels of exposure to the French linguistic stimuli. Some had heard French only through natural environment in utero, whereas others were in addition exposed to the French stimuli through the experimental procedure of the study. This differential procedure could have had an impact on brain responses at birth. To assess these possible differences between data, a repeated measure ANOVA was performed by comparing both French native subgroups (those with no experimental prenatal exposure vs. those who were exposed prenatally to the French linguistic stimuli), and no significant differences in HbO concentration changes were found between groups (see Supplementary Table S5). Considering those results and that all children were naturally exposed to French in the womb as both their parents were monolingual French speakers, all participants were included in the native condition to obtain optimal statistical power.
Although further research is necessary to better understand how prenatal linguistic exposure impacts brain responses to languages at birth, our findings demonstrate that even a short period of exposure in utero to an unfamiliar foreign language can influence speech processing at birth. Language familiarity seems to play a role in shaping language networks during early perinatal development. This study is in line with previous findings about left-hemispheric lateralization for native language processing shortly after birth and adds insights into the neural basis of language development.
Materials and methods
Experimental design
This study is part of a longitudinal project which aims to investigate the developmental trajectories of language brain networks in young children. To do so, healthy infants were followed from birth to three years of age and underwent developmental assessments as well as fNIRS recording during rest and a passive story listening task at different time points. In the current study, only fNIRS data acquired at birth during the passive story listening task were used to assess the impact of prenatal exposure to linguistic stimuli on brain responses in newborns.
Participants
Seventy-seven healthy pregnant people and their future newborns were recruited during the third trimester of pregnancy at one of their antenatal visits to the obstetrical and gynecology clinic at Sainte-Justine University Hospital. Inclusion criteria were being from French-speaking parents and having a unilingual familial context, as assessed by a self-reported questionnaire filled out by the parents. Exclusion criteria were specific major events during gestation or birth history (e.g., intrauterine growth delay, severe infection disease during gestation including HIV, toxoplamosis, herpes, and tuberculosis, birth <37 weeks of gestation, birth weight <2500 g, APGAR at 1 min ≤7) and identification of a genetic, congenital, or neurologic condition known to affect neurodevelopment. Newborns’ eligibility was reassessed after birth by reviewing their medical records. They were excluded if suspected of having an auditory deficit or if their health condition required a stay at the neonatal intensive care unit. As part of the Quebec Newborn Hearing Screening Program, all newborns received an otoacoustic emissions (OAE) test in both ears and auditory brainstem responses in cases of suspected hearing loss. The study was approved by the Research Ethics Committee of Sainte-Justine University Hospital. Informed written consent was obtained from all parents. All ethical regulations relevant to human research participants were followed.
An a priori power analysis was conducted using G power version 3.1.9.753 to obtain 80% power and detect a medium effect size (f = 0.25). A significance criterion of α = 0.05 as used in the case where there was no correlation among repeated measures, and a non-sphericity correction epsilon = 0.8 was applied. In this case, the power analysis showed repeated measures ANOVA required a minimal sample size of 36. From all 77 recruited participants, 17 were excluded due to one or more of the following reasons: neonatal complications (N = 9), cancellation of the laboratory visits after birth due to the Covid pandemic (N = 5), withdrawal of their participation after delivery (N = 2) and incomplete data due to a technical problem during the fNIRS recording (N = 1). Data from the remaining 60 newborns were subsequently analyzed.
Among these participants, 39 participants recruited at 35 weeks of GA or less were randomly assigned to one of the prenatal linguistic exposure groups: German (N = 20) or Hebrew (N = 19), to balance prenatal linguistic exposure and to control variability due to language phonetics. In addition to participants who received prenatal exposure, an additional 21 participants were recruited after 35 weeks of GA and were not exposed prenatally to linguistic stimuli through an experimental procedure. They listened to French in utero through their natural environment. Therefore, their data were analyzed as part of the native condition (when listening to French) or unexposed condition (when listening to Hebrew and German).
Demographic and clinical variables were collected from medical records and parental questionnaires. No statistically significant differences regarding medical and sociodemographic variables were found across groups (see Table 1 for a description of the sample).
Stimuli
One multilingual female fluent in French, German, and Hebrew recorded all three versions of the children’s story as to avoid variability that could be influenced by use of different speakers. She read the stories using infant-directed speech. Each language version included 18 blocks total, with a mean duration of 15.1 ± 0.1 s. Mean intensity of all blocks was normalized, and 3-s fade-in and fade-out (starting and ending at 60% of mean intensity) were applied using Audacity 2.2.1. To create a continuous 5-min story for each version of the prenatal exposure, all 18 blocks of the same language were juxtaposed together with 0.8 s pauses in between. The same stimuli were used for prenatal exposure and fNIRS testing at birth.
For each stimulus block, mean pitch, maximal and standard deviation of the fundamental frequencies (f0) were extracted using Praat v.6.1.32, and the number of syllables was initially counted by a native speaker and then further validated by a second independent listener27,54. To estimate pitch variability within each block, a normalized metric (i.e., standard deviation f0 relative to mean f0) was further computed55. Table 2 shows the main acoustic proprieties across the three language conditions.
Procedure
Prenatal linguistic exposure
Starting at the 35th week of GA, fetuses in the prenatal groups (N = 39: 20 German; 19 Hebrew) were exposed daily to two versions of the same children’s story: one in their native language (French) and the other in a foreign language (German or Hebrew, based on their subgroup). This gestational period was selected as an orientation response to complex speech stimuli has been previously observed in fetuses of this age, unlike in younger fetuses18,19,20. Participants recruited after 35 weeks of GA (N = 21) were exposed to none of those stimuli during gestation.
All pregnant people doing prenatal exposition were given an audio kit containing headphones and a portable audio player (Sony MDRZX110). They were all instructed to complete one prenatal exposure session daily up to delivery, at least once every other day. They kept a diary to track the number of completed daily sessions and the surrounding conditions revealing an adequate exposure for all participants (mean exposure 25.3 ± 8.8 sessions). No participants had to be excluded because of a lack of prenatal exposure. For each session, the pregnant mothers were instructed to place the headphones on their abdomen approximately at the level of their belly button. Each prenatal exposure session lasted 20 minutes, during which a native (French) and foreign (German or Hebrew, based on the participant’s subgroup) version of the 5-min story was presented twice in alternation. The starting language was counterbalanced across participants. The volume had been previously calibrated to 90 dB in the laboratory to compensate for sound attenuation through maternal tissues, resulting in an ~60 dB SPL in utero, which posed no risk to fetal auditory development56,57,58. At that sound level, participants could hear the languages through the headphones placed on their abdomen and may have been able to guess which foreign language they had been assigned to. Pregnant participants were asked to complete the sessions in a quiet environment, free from surrounding conversations or other verbal or auditory interference (e.g., no television with the sound on, listening to music, or speaking during the session).
Neonatal fNIRS recording
All newborns underwent an fNIRS recording within their first three days of life before being discharged from the postpartum unit at Sainte-Justine University Hospital. Age at recording ranged between 10 and 78 h after birth (mean age at testing: 30.3 h ± 14.1).
The entire testing session, including fNIRS installation and data acquisition during the passive story listening task and at rest lasted 60 min or less. During the session, newborns were comfortably asleep on their backs, either in their hospital crib or on a cushion placed on their parents’ lap (Fig. 2A). To control for the behavioral state of the participants, all recordings took place while the newborns were in a quiet state of sleep. A pediatric nurse was always present to ensure participants’ well-being and to make sure that the newborns were adequately positioned to hear the stimuli with their head centered between the two speakers and no objects or cushion close to the ears. All newborns passively listened to the children’s story in each of the three languages, i.e., French, German, and Hebrew.
Stimuli were delivered through two speakers placed bilaterally at 70 cm from the newborns’ heads, with the intensity reaching ~70 dB SPL as measured by a sound meter. The stories were presented using a block design paradigm, consisting of 18 blocks for each language condition. The 15 s stimulation blocks were followed by silent interstimulus intervals lasting between 23 and 27 s(Fig. 2C), resulting in an approximate total duration of 36 min. The paradigm presentation order was similar to that described in ref. 11 and consisted of three consecutive blocks from one language. The stimulus presentation order for French, German, and Hebrew was counterbalanced between participants.
fNIRS data acquisition was performed using a continuous-wave NIRScout system (NIRx Medical Technologies, Germany) equipped with 16 detectors and 16 sources of 760 nm and 850 nm wavelengths, and a sampling rate of 7.8 Hz. The montage included 72 channels with an approximate 2–5 cm source-detector separation. In children, a source-detector distance of 2–2.5 cm is enough to obtain a depth of 1.5–2 cm59. It has been shown that a too short distance (<2 cm) between sources and detectors only records hemodynamic changes in superficial tissues, whereas at a too long distance (i.e., more than 5 cm), not enough photons reach the detector60. Detectors and sources were held in place by a flexible headgear (Easycap GmbH, Germany). The positioning of the headgear was standardized across newborns based on their head circumference, nasion-inion distance, and left and right preauricular points as reference markers. The probes were positioned to symmetrically cover six cortical regions in both hemispheres: prefrontal, inferior frontal, posterior frontal, temporal, posterior temporal and temporo-parietal (Fig. 2B). Following the procedure outlined in ref. 61, spatial localization of each probe relative to fiducial points (nasion, inion, left and right preauricular) was digitized on a newborn head model using the Polaris stereotaxic system (Northern Digital Inc., Canada) and Brainsight Frameless 39 software (Rogue Research Inc., Canada). It was then co-registered onto a newborn structural MRI template62 and visualized using the 3DMTG interface from the LIONirs toolbox63. Anatomical registration was further validated according to the international 10-10 system64. This procedure allowed the estimation of the underlying cerebral regions associated with each channel and regions of interest (ROIs), making them comparable to those in other infant studies, while accounting for variations in probe placement5,46,65,66. The pediatric nurse also ensured that the headgear remained stable in case of fussiness and newborns’ movements (e.g., sucking, startles) were filmed to validate movement artifact identification in offline analyses.
Preprocessing
fNIRS data processing was performed using the LIONirs toolbox63 embedded in the SPM12 toolbox67 and ran under Matlab R2021b (MathWorks, United States). First, the data were visually inspected to ensure the signal quality (e.g., no large-scale signal aberrations, presence of a heartbeat). The use of trial rejection exclusively to address motion artifacts has been discouraged in the fNIRS literature, including studies involving infants, as it reduces the number of valid trials and impacts the accuracy of the hemodynamic response function (HRF) recovery68,69. When possible, artifacts were corrected using target principal component analysis (PCA) and parallel factor analysis (PARAFAC)70,71. If excessive movement artifacts (>15%) occurred during the stimulation periods and shortly before or after (i.e., 5 s), the trial was rejected30. Overall, 20% of the trials were rejected across all participants because of excessive movement artifacts. Only channels showing the presence of cardiac frequency were used for further analysis as it is an indicator of the signal’s quality63,72.
To account for physiological confounds, we first applied a fourth-order Butterworth low-pass filter with a cut-off frequency of 0.2 Hz to eliminate high-frequency noise (e.g., respiration and heartbeat). Data were then converted to optical density changes and transformed into relative concentration changes of HbO and HbR using the modified Beer-Lambert law, along with an age-appropriate differential pathlength factor (DPF)73 (DPF at 760 nm = 5.286; DPF at 850 nm = 4.224). A General Linear Model (GLM) approach was used to estimate task-evoked hemodynamic response function (HRF)74 related to the HbO concentration changes, since it is known to be more sensitive than HbR to blood oxygenation changes related to brain activity44,45. Using GLM, the regression coefficient associated with physiological noise using the combination of all channels was computed75, and physiological responses were subtracted from the HRF time course average76. Regions of interest (ROI) were assigned according to their anatomical localization (Fig. 2B). In order to statistically assess ROI differences across language and prenatal exposition conditions for each participant, channels located within the same ROI were further averaged together to obtain the mean HbO concentration change for each ROI. Mean ROI concentration changes for each language condition and each participant were then exported for subsequent statistical analysis.
Statistical analysis
A winsorizing method was applied to ensure an automatic control of outliers using a threshold of 10 and 90% percentiles77. Kormogorov–Smirnov tests confirmed that all variables were normally distributed78,79. Variances were homogeneous as assessed by Levene’s test for equality of variance. Mauchy’s spherical assumptions were not respected, therefore the Greenhouse-Geisser correction was applied80. A repeated measure ANOVA was performed using within-subject factors ROI (Prefrontal, Inferior frontal, Posterior frontal, Temporal, Posterior temporal, Temporo-parietal) and Hemisphere (LH, RH), and between-subjects factor Condition (Native, Exposed, Unexposed). Figure 5 explains how participants’ data recorded at birth were split into three language familiarity conditions (Native, Exposed, Unexposed). Post hoc tests with Bonferroni correction were applied to further investigate significant interactions (IBM SPSS Statistics for Windows, version 27.0. Armonk, NY: IBM Corp). Pearson correlational analyses were also performed for each language familiarity condition and ROI, for both hemispheres, between HbO concentration and the amount of exposure for participants who had received prenatal exposure. The amount of exposure for each participant was calculated by turning the number of prenatal exposure sessions reported by their parent into percentages.

Participants’ fNIRS data were split into three language familiarity conditions (Native in blue, Exposed in cyan, Unexposed in green) according to prenatal exposure conditions (Prenatal exposure (German), Prenatal exposure (Hebrew), No prenatal exposure) and language of story.
Statistics and reproducibility
Details of the experiment as well as preprocessing of fNIRS data are available in the Materials and methods section “Experimental design”. We performed a repeated measure ANOVA in SPSS, using a significance criterion of 0.05, followed by post hoc tests with Bonferroni correction.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The data supporting the findings of this study are available as a supplementary Excel data sheet.
References
Byers-Heinlein, K. & Fennell, C. T. Perceptual narrowing in the context of increased variation: insights from bilingual infants. Dev. Psychobiol. 56, 274–291 (2014).
Hervé, P.-Y., Zago, L., Petit, L., Mazoyer, B. & Tzourio-Mazoyer, N. Revisiting human hemispheric specialization with neuroimaging. Trends Cogn. Sci. 17, 69–80 (2013).
Kuhl, P. K. Brain mechanisms in early language acquisition. Neuron 67, 713–727 (2010).
Wang, D., Buckner, R. L. & Liu, H. Functional specialization in the human brain estimated by intrinsic hemispheric interaction. J. Neurosci. 34, 12341–12352 (2014).
Gervain, J., Macagno, F., Cogoi, S., PeñA, M. & Mehler, J. The neonate brain detects speech structure. Proc. Natl. Acad. Sci. USA 105, 14222–14227 (2008).
May, L., Byers-Heinlein, K., Gervain, J. & Werker, J. F. Language and the newborn brain: does prenatal language experience shape the neonate neural response to speech? Front. Psychol. 2, 222 (2011).
May, L., Gervain, J., Carreiras, M. & Werker, J. F. The specificity of the neural response to speech at birth. Dev. Sci. 21, e12564 (2018).
Peña, M. et al. Sounds and silence: an optical topography study of language recognition at birth. Proc. Natl. Acad. Sci. USA 100, 11702–11705 (2003).
Perani, D. et al. Neural language networks at birth. Proc. Natl. Acad. Sci. USA 108, 16056–16061 (2011).
Saito, Y. et al. The function of the frontal lobe in neonates for response to a prosodic voice. Early Hum. Dev. 83, 225–230 (2007).
Vannasing, P. et al. Distinct hemispheric specializations for native and non-native languages in one-day-old newborns identified by fNIRS. Neuropsychologia 84, 63–69 (2016).
Dehaene-Lambertz, G., Hertz-Pannier, L. & Dubois, J. Nature and nurture in language acquisition: anatomical and functional brain-imaging studies in infants. Trends Neurosci. 29, 367–373 (2006).
Graven, S. N. & Browne, J. V. Auditory development in the fetus and infant. Newborn Infant Nurs. 8, 187–193 (2008).
Ghio, M., Cara, C. & Tettamanti, M. The prenatal brain readiness for speech processing: a review on foetal development of auditory and primordial language networks. Neurosci. Biobehav. Rev. 128, 709–719 (2021).
E. Partanen & P. Virtala, Prenatal sensory development. in The Cambridge Encyclopedia of Child Development 2nd edn (eds Hopkins B., Geangu E. & Linkenauger S.) 231–224 (Cambridge University Press, 2017).
Busnel, M. C., Granier-Deferre, C. & Lecanuet, J. P. Fetal audition. Ann. N. Y. Acad. Sci. 662, 118–134 (1992).
Querleu, D., Renard, X., Versyp, F., Paris-Delrue, L. & Crèpin, G. Fetal hearing. Eur. J. Obstet. Gynecol. Reprod. Biol. 28, 191–212 (1988).
Kisilevsky, B. S. et al. Effects of experience on fetal voice recognition. Psychol. Sci. 14, 220–224 (2003).
Kisilevsky, B. S. et al. Fetal sensitivity to properties of maternal speech and language. Infant Behav. Dev. 32, 59–71 (2009).
Krueger, C. & Garvan, C. Emergence and retention of learning in early fetal development. Infant Behav. Dev. 37, 162–173 (2014).
Byers-Heinlein, K., Burns, T. C. & Werker, J. F. The roots of bilingualism in newborns. Psychol. Sci. 21, 343–348 (2010).
Moon, C., Cooper, R. P. & Fifer, W. P. Two-day-olds prefer their native language. Infant Behav. Dev. 16, 495–500 (1993).
Beauchemin, M. et al. Mother and stranger: an electrophysiological study of voice processing in newborns. Cereb. Cortex. 21, 1705–1711 (2011).
Uchida-Ota, M. et al. Maternal speech shapes the cerebral frontotemporal network in neonates: a hemodynamic functional connectivity study. Dev. Cogn. Neurosci. 39, 100701 (2019).
Sato, H. et al. Cerebral hemodynamics in newborn infants exposed to speech sounds: a whole-head optical topography study. Hum. Brain Mapp. 33, 2092–2103 (2012).
Mariani, B. et al. Prenatal experience with language shapes the brain. Sci. Adv. 9, eadj3524 (2023).
Arvaniti, A. & Rodriquez, T. The role of rhythm class, speaking rate, and F0 in language discrimination. Lab. Phon. 4, 7–38 (2013).
Partanen, E. et al. Learning-induced neural plasticity of speech processing before birth. Proc. Natl. Acad. Sci. USA 110, 15145–15150 (2013).
Partanen, E., Kujala, T., Tervaniemi, M. & Huotilainen, M. Prenatal music exposure induces long-term neural effects. PLoS ONE 8, e78946 (2013).
Paquette, N. et al. Developmental patterns of expressive language hemispheric lateralization in children, adolescents and adults using functional near-infrared spectroscopy. Neuropsychologia 68, 117–125 (2015).
Gallagher, A., Tremblay, J. & Vannasing, P. Language mapping in children using resting-state functional connectivity: comparison with a task-based approach. J. Biomed. Opt. 21, 125006 (2016).
Chen, W.-L. et al. Functional near-infrared apectroscopy and its clinical application in the field of neuroscience: advances and future directions. Front. Neurosci. 14, 1–15 (2020).
Gratton, G. et al. Fast and localized event-related optical signals (EROS) in the human occipital cortex: comparisons with the visual evoked potential and fMRI. NeuroImage 6, 168–180 (1997).
Hu, Z., Liu, G., Dong, Q. & Niu, H. Applications of resting-state fNIRS in the developing brain: a review from the connectome perspective. Front. Neurosci. 14, 476 (2020).
Watanabe, E. et al. Non-invasive assessment of language dominance with near-infrared spectroscopic mapping. Neurosci. Lett. 256, 49–52 (1998).
Hillman, E. M. C. Coupling mechanism and significance of the BOLD signal: a status report. Annu. Rev. Neurosci. 37, 161–181 (2014).
Biswal, B., Zerrin Yetkin, F., Haughton, V. M. & Hyde, J. S. Functional connectivity in the motor cortex of resting human brain using echo-planar MRI. Magn. Reson. Med. 34, 537–541 (1995).
Nazzi, T., Iakimova, G., Bertoncini, J., Frédonie, S. & Alcantara, C. Early segmentation of fluent speech by infants acquiring French: emerging evidence for crosslinguistic differences. J. Mem. Lang. 54, 283–299 (2006).
Segal, O., Keren-Portnoy, T. & Vihman, M. Infant recognition of Hebrew vocalic word patterns. Infancy 20, 208–236 (2015).
Segal, O., Nir-Sagiv, B., Kishon-Rabin, L. & Ravid, D. Prosodic patterns in Hebrew child-directed speech. J. Child. Lang. 36, 629–656 (2009).
Ravid, D. & Shlesinger, Y. Vowel reduction in modern Hebrew: traces of the past and current variation. Folia Linguist 35, 371–398 (2001).
Bijeljac-Babic, R., Serres, J., Höhle, B. & Nazzi, T. Effect of bilingualism on lexical stress pattern discrimination in French-learning infants. PLoS ONE 7, e30843 (2012).
Höhle, B., Bijeljac-Babic, R., Herold, B., Weissenborn, J. & Nazzi, T. Language specific prosodic preferences during the first half year of life: evidence from German and French infants. Infant Behav. Dev. 32, 262–274 (2009).
Homae, F., Watanabe, H., Nakano, T. & Taga, G. Prosodic processing in the developing brain. Neurosci. Res. 59, 29–39 (2007).
Zhang, Y., Brooks, D. H., Franceschini, M. F. & Boas, D. A. Eigenvector-based spatial filtering for reduction of physiological interference in diffuse optical imaging. J. Biomed. Opt. 10, 011014 (2005).
Benavides-Varela, S. et al. Brain regions and functional interactions supporting early word recognition in the face of input variability. Proc. Natl. Acad. Sci. USA 114, 7588–7593 (2017).
Bouchon, C., Nazzi, T. & Gervain, J. Hemispheric asymmetries in repetition enhancement and suppression effects in the newborn brain. PLoS ONE 10, e0140160 (2015).
Minagawa-Kawai, Y., Cristià, A. & Dupoux, E. Cerebral lateralization and early speech acquisition: a developmental scenario. Dev. Cogn. Neurosci. 1, 217–232 (2011).
Nakano, T., Watanabe, H., Homae, F. & Taga, G. Prefrontal cortical involvement in young infants’ analysis of novelty. Cereb. Cortex. 19, 455–463 (2009).
Thompson, R. F. & Spencer, W. A. Habituation: a model phenomenon for the study of neuronal substrates of behavior. Psychol. Rev. 73, 16–43 (1966).
Dehaene-Lambertz, G. et al. Language or music, mother or Mozart? Structural and environmental influences on infants’ language networks. Brain Lang. 114, 53–65 (2010).
Minagawa-Kawai, Y. et al. Optical brain imaging reveals general auditory and language-specific processing in early infant development. Cereb. Cortex. 21, 254–261 (2011).
Faul, F., Erdfelder, E., Lang, A.-G. & Buchner, A. G. *Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 39, 175–191 (2007).
Boersma, R., Podesva, J. & Sharma, D. Acoustic analysis. in Research Methods in Linguistics 375–396 (Cambridge University Press, 2014).
Zimmerer, F., Jügler, J., Andreeva, B., Möbius, B. & Trouvain, J. Too cautious to vary more? A comparison of pitch variation in native and non-native productions of French and German speakers. In Proc. 7th Speech Prosody Conference (PLOS (Public Library of Science), 2014).
Arulkumaran, S. et al. In-utero sound levels when vibroacoustic stimulation is applied to the maternal abdomen: an assessment of the possibility of cochlea damage in the fetus. Br. J. Obstet. Gynaecol. 99, 43–45 (1992).
Granier-Deferre, C., Bassereau, S., Ribeiro, A., Jacquet, A.-Y. & Decasper, A. J. A melodic contour repeatedly experienced by human near-term fetuses elicits a profound cardiac reaction one month after birth. PLoS ONE 6, e17304 (2011).
Granier-Deferre, C., Ribeiro, A., Jacquet, A.-Y. & Bassereau, S. Near-term fetuses process temporal features of speech. Dev. Sci. 14, 336–352 (2011).
Pinti, P., Tachtsidis, I., Burgess, P. W. & Hamilton, A. F. de C. Non-invasive optical imaging of brain function with fNIRS: current status and way forward. in Encyclopedia of the Human Brain 2nd edn, 96–120 (Elsevier, 2025).
Tremblay, J. et al. Comparison of source localization techniques in diffuse optical tomography for fNIRS application using a realistic head model. Biomed. Opt. Express 9, 2994–3016 (2018).
Lloyd-Fox, S. et al. Coregistering functional near-infrared spectroscopy with underlying cortical areas in infants. Neurophotonics. 1, 025006 (2014).
Kazemi, K., Moghaddam, H. A., Grebe, R., Gondry-Jouet, C. & Wallois, F. A neonatal atlas template for spatial normalization of whole-brain magnetic resonance images of newborns: preliminary results. NeuroImage 37, 463–473 (2007).
Tremblay, J. et al. LIONirs: flexible Matlab toolbox for fNIRS data analysis. J. Neurosci. Methods 370, 109487 (2022).
Kabdebon, C. et al. Anatomical correlations of the international 10–20 sensor placement system in infants. NeuroImage 99, 342–356 (2014).
Abboub, N., Nazzi, T. & Gervain, J. Prosodic grouping at birth. Brain. Lang. 162, 46–59 (2016).
Mercure, E. et al. Language experience impacts brain activation for spoken and signed language in infancy: insights from unimodal and bimodal bilinguals. Neurobiol. Lang. 1, 9–32 (2020).
Penny, W. D., Friston, K. J., Ashburner, J. T., Kiebel, S. J. & Nichols, T. E. Statistical parametric mapping: the analysis of functional brain images (Elsevier, 2011).
Brigadoi, S. et al. Motion artifacts in functional near-infrared spectroscopy: a comparison of motion correction techniques applied to real cognitive data. NeuroImage 85, 181–191 (2014).
Di Lorenzo, R. et al. Recommendations for motion correction of infant fNIRS data applicable to multiple data sets and acquisition systems. NeuroImage 200, 511–527 (2019).
Hüsser, A. et al. Parallel factor analysis for multidimensional decomposition of functional near-infrared spectroscopy data. Neurophotonics 9, 045004 (2022).
Yücel, M. A., Selb, J., Cooper, R. J. & Boas, D. A. Targeted principle component analysis: a new motion artifact correction approach for near-infrared spectroscopy. J. Innov. Opt. Health Sci. 07, 1350066 (2014).
Pollonini, L. et al. Auditory cortex activation to natural speech and simulated cochlear implant speech measured with functional near-infrared spectroscopy. Hear. Res. 309, 84–93 (2014).
Scholkmann, F. & Wolf, M. General equation for the differential pathlength factor of the frontal human head depending on wavelength and age. J. Biomed. Opt. 18, 105004 (2013).
Glover, G. H. Deconvolution of impulse response in event-related BOLD fMRI1. NeuroImage 9, 416–429 (1999).
Gervain, J. et al. Near-infrared spectroscopy: a report from the McDonnell infant methodology consortium. Dev. Cogn. Neurosci. 1, 22–46 (2011).
Saager, R. B. & Berger, A. J. Measurement of layer-like hemodynamic trends in scalp and cortex: implications for physiological baseline suppression in functional near-infrared spectroscopy. J. Biomed. Opt. 13, 034017 (2008).
Ruppert, D. Trimming and Winsorization. in Wiley StatsRef: Statistics Reference Online (Wiley, 2014).
Feng, C. et al. Log-transformation and its implications for data analysis. Shanghai Arch. Psychiatry 26, 105–109 (2014).
Mishra, P. et al. Descriptive statistics and normality tests for statistical data. Ann. Card. Anaesth. 22, 67 (2019).
Landau, S. & Everitt, B. S. A Handbook of Statistical Analyses Using SPSS. (Chapman and Hall/CRC, 2003).
Boyd, M. A socioeconomic scale for Canada: measuring occupational status from the census. Can. Rev. Sociol. 45, 51–91 (2008).
Nuwer, M. R. et al. IFCN standards for digital recording of clinical EEG. Electroencephalogr. Clin. Neurophysiol. 106, 259–261 (1998).
Acknowledgements
We are grateful to the study participants and their families. We would like to thank the Mother-Child Postpartum Unity of Sainte Justine University Hospital and the Sainte-Justine Foundation for their help on the project, as well as Lise-Angela Ouellet, Sophie Perreault, Guylaine Aubé, Hélène Gagnon, Pauline Lebret, Sarah Kraimeche, Ioana Medeleine Constantin, Clémence Noiseux, Jacqueline Trieu, and Florence Ménard for their support in the project recruitment and data collection. We would also like to acknowledge that this work has been supported by a Natural Sciences and Engineering Research Council of Canada (NSERC) Discovery Grant RGPIN-2020-05029 (A.G.), a Canada Research Chair in Child Neuropsychology and Brain Imaging 950-232661 (A.G.), a NSERC scholarship (L.C.D. & A.R.), a Canadian Institutes of Health Research scholarship (L.C.D.), a Fonds de Recherche du Québec—Santé/Nature et Technologie scholarship (L.C.D. & A.R.), as well as a Sainte-Justine University Hospital Foundation scholarship (A.R.).
Author information
Authors and Affiliations
Contributions
Anne Gallagher, Phetsamone Vannasing, and Laura Caron-Desrochers designed the experiment, Catherine Taillefer and Isabelle Boucoiran helped with recruitment in the Mother-Child Postpartum Unity of Sainte Justine University Hospital, Laura Caron-Desrochers, Natacha Paquette, Phetsamone Vannasing, Julie Tremblay, and Laurence Petitpas conducted the experiment, Andréanne René, Julie Tremblay and Laura Caron-Desrochers analyzed the data, Andréanne René, Laura Caron-Desrochers, Solène Fourdain and Kassandra Roger wrote the paper, and Anne Gallagher, Natacha Paquette, and Judit Gervain edited the paper.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Communications Biology thanks Evelyne Mercure, Neelima Wagley and the other anonymous reviewer(s) for their contribution to the peer review of this work. Primary handling editor: Jasmine Pan.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
René, A., Caron-Desrochers, L., Tremblay, J. et al. Prenatal linguistic exposure shapes language brain responses at birth. Commun Biol 8, 1155 (2025). https://doi.org/10.1038/s42003-025-08594-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s42003-025-08594-8
