
Abstract
Agriculture is an important contributor to air pollution and its health impacts, with ramifications for environmental and health inequity. A substantial fraction of these effects can be attributable to dietary changes, but the extent of such impacts remains unclear. Here we show that the PM2.5-related mortality attributable specifically to dietary changes and the associated rising agricultural emissions has a high Gini coefficient of 0.369 in China in 2010, and raises the Gini coefficient of all-cause PM2.5-related mortality from 0.189 to 0.197 with more uneven allocation among income groups, reflecting worsened health inequity and an export of pollution from richer coastal regions to poorer agricultural regions via food trade. Such mortality is associated positively with urbanization but negatively with green space and healthcare quality. Our results also provide empirical evidence for the environmental Kuznets curve hypothesis, and offer decision support for equitable clean air, food and health policies in China.
Similar content being viewed by others

Introduction
Ambient particulate matter less than 2.5 μm in diameter (PM2.5) causes a heavy global health burden, accounting for 5–9 million premature deaths worldwide every year1,2,3. The health burden is unevenly distributed across countries and regions due to various socioeconomic statuses and industrial structures4. China is a hotspot of PM2.5 pollution, contributing to a quarter of the world’s PM2.5-attributable mortality5. Uneven spatial distribution of health impacts among regions and income groups is also observed within China6,7,8. Health inequality is detrimental to social well-being, undermining socioeconomic equity9,10. It may also trigger an “environmental health poverty trap”, causing a vicious cycle of poverty and health hazards4,11.
Previous studies have found that some sociodemographic and environmental factors (e.g., urbanization, green space, medical resources, and income) have strong associations with air pollution, which might further increase the unequal health impacts of air pollution. For instance, at the individual level, people with high socioeconomic status are linked to limited air-pollution-related health impacts due to high-quality living environments and healthcare resources7. At the regional level, a more complex picture ensues: economic growth initially deteriorates air quality, but after a certain level of economic growth is reached, the opposite trend occurs12. Urbanization is reported to benefit air quality by promoting the use of cleaner energy, as urban areas typically rely more on clean energy compared to rural regions but show divergent outcomes for regions with different development levels13. While medical resources can alleviate the negative health outcomes of air pollution, they are mostly allocated to urban or high-income regions14,15. Meanwhile, urbanization can increase human exposure to air pollution due to the higher population density and PM2.5 levels in urban areas. Urban green space can improve air quality and human health via psychological relaxation, stress reduction, physical activity, fitness promotion, and ecosystem services16. However, these resources (e.g., wealth, medical, and infrastructural) are unevenly distributed, contributing to health inequality.
China has launched its toughest-ever air cleanup action to improve air quality since 2013, successfully reducing the emissions of sulfur dioxide (SO2) and nitrogen oxides (NOx)17,18,19. These measures also seek to reform the industrial structures by shifting the energy matrix from fossil fuels to renewable and clean energy sources to achieve “green growth”, which can further reduce air pollution. Public health has since benefited, with PM2.5-related mortality declining by 9% in the first two years (2013–2015)19. However, much less control efforts have been laid on the agricultural sector; e.g., agricultural ammonia (NH3) emissions are currently not rigorously controlled20. The agricultural sector contributes to 20–30% of PM2.5-attributed mortality in China, highlighting the vital role of regulating agricultural emissions in PM2.5 mitigation21. One of the key drivers of agricultural emissions is the changing food demand due to dietary changes in the country since the 1980s, characterized mainly by a rapid shift from a mostly plant-based diet toward a more meat-intensive one, with a corresponding substantial increase in per capita meat consumption, which has increased from 30–40 g to 90–140 g over 1980–20108. Animal-based diets exhibit a greater nitrogen and carbon footprint compared to plant-based diets, primarily due to the lower resource and energy conversion efficiency involved in meat production and the abundance of animal waste in livestock systems (Fig. S2)22,23. Such diet-driven changes between the 1980s and 2010s have, in turn, increased agricultural NH3 emissions by more than 60% and annual PM2.5 by up to 10 μg m–3, which is roughly 20% of the total PM2.5 increase coming from all sources over the same period8. The growing food demand in food-consuming regions, in turn, has to be mostly met by rising production of the net food-producing regions via inter-regional trade in China. The resulting food-for-pollution trade may induce environmental injustice: the net food-producing regions may suffer more pollution-related health costs arising from food production while consuming less food than the net food-consuming regions24,25,26,27. Approximately 27,000 PM2.5-related premature deaths in China were transferred from the net food-consuming regions to the other regions through inter-provincial trade of agricultural products in 201224. A recent study has also demonstrated that the net food-producing regions bear an additional burden of 22,000 PM2.5-related premature deaths owing to its food supply to other regions in 201727.
Previous studies have explored the potential driving factors of the unequal health impacts of PM2.5. For instance, disparities in socioeconomic status28, trade24, and energy consumption structure29 all contributed to the uneven allocation of PM2.5-related health impacts. However, they did not explore how dietary changes in the population may impact PM2.5-related health inequality, and how sociodemographic and environmental factors might variably modulate such impacts in different regions. To bridge this knowledge gap, we first derived the all-cause PM2.5-related mortality and PM2.5-related mortality arising from dietary changes at the city level in China in 2010 using high-resolution atmospheric model experiments8. Then, the Lorenz curve and Gini index were applied to quantify PM2.5-related health inequality. Finally, we examined the spatially heterogeneous associations between PM2.5-related mortality arising from dietary changes and various sociodemographic and environmental factors. Our work provides quantitative estimates of how dietary changes influence PM2.5-related health inequality, reveals the important drivers behind it, and offers insights for targeted, coordinated, and equitable pollution mitigation and food-system strategies in China.
Results
PM2.5-related mortality rate at the city scale
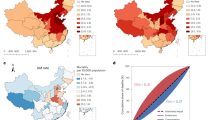
We first examined how dietary changes have worsened PM2.5-related health inequality in mainland China (referred to as China in this paper). Figure 1 shows the share of premature deaths caused by PM2.5 with (all-cause mortality: A-mortality) and without dietary changes (A–D-mortality), and dietary change-related PM2.5 (D-mortality) in the total population at the city level (359 cities) and regional level in China in 2010. The average mortality rate induced by dietary changes (D-mortality rate) is 0.66 deaths per 10000 people or ~5% of the 13.3 deaths per 10,000 people all-cause PM2.5-related mortality rate (A-mortality rate). The highest A-mortality, A–D-mortality, and D-mortality rates are all located in the central and eastern parts of China. The Moran’s I index (Z = 26, p < 0.001) for D-mortality is 0.83, higher than the 0.73 (Z = 23, p < 0.001) for A-mortality and the 0.72 (Z = 23, p < 0.001) for A–D-mortality, all reflecting high spatial autocorrelation: as the mortality of a city increases, so does that of its neighboring cities. We further applied the local indicators of spatial association (LISA) to detect the spatial clusters of the three mortality rates (Fig. S3). The hotspots of A-mortality and A–D-mortality are similar, but fewer hotspots are identified in Northeast China (NE) for A–D-mortality than for A-mortality. The hotspots of D-mortality are different: the Huang–Huai–Hai region (HHH) has the highest A-mortality and A–D-mortality, while NE has the highest D-mortality. Without the effects of dietary changes, NE and HHH are less affected by PM2.5, especially for NE (Fig. 1a, b). Although NE is a major food-producing region on a par with HHH, it rarely hosts the hotspots of agricultural NH3 emissions due to state-of-the-art agricultural machinery and management and lower air temperature30,31,32. During 1980–2010, China’s meat production surged by 5.3 times, with HHH and NE experiencing remarkable increases by 7.7 and 6.9 times, respectively33. To meet the increasing food and feed crop demand, over the same period, grain yield nearly tripled in NE, compared to a doubling in HHH, and planting area increased by 1.28 times in NE, compared to 1.09 times in HHH33. In recent decades, to support economic growth, approximately 77,200 km2 of cultivated land has been converted to built-up areas, primarily in South China (SC) and HHH34. Meanwhile, to meet the increasing food demand driven by a rising urban population and dietary shifts, an even larger area of approximately 329,400 km2 has been brought into cultivation in NE and Northwest China (NW)34. Consequently, NE is subject to more environmental burdens from dietary changes8.

a Spatial distribution of all-cause mortality rate caused by PM2.5 at the city level; b spatial distribution of PM2.5-related mortality rate without dietary changes; c spatial distribution of PM2.5-related mortality rate specifically induced by dietary changes at the city level; d the relative mortality rate (represented by: regional average/national average) at regional level. The spatial distribution of (e) agricultural and (f) food functional regions. Agricultural regions include Southwest (SW), Northwest (NW), Northeast (NE), Huang–Huai–Hai (HHH), Middle and Lower Yangtze River (MLYR), and South China (SC). Food functional regions include net food-producing region (FP), net food-consuming region (FC), and food-balanced region (i.e., regions with balanced food supply and demand, FB).
We further examined the regional disparities in mortality rates among different sub-regions, as listed from top to bottom as residents’ income increases (Fig. 1d and Fig. S4). Here, we divide China into two kinds of sub-regions: one is by agricultural regions, i.e., grouping China into six sub-regions based on agricultural endowments including land, water, and meteorological conditions35; another is by food functional regions, i.e., dividing China into three sub-regions according to their role (producer or consumer) in intra-China food trade36 (see region definitions in Fig. 1e, f and Table S1). We found that regions with middle incomes have higher levels of mortality than regions with high or low incomes. The disparities in D-mortality between high- or low-income regions and middle-income regions are more obvious than those of A-mortality and A–D-mortality. Specifically, the HHH and the net food-producing (FP) region have the highest average A-mortality rate of 15.6 deaths per 10,000 people and 15 deaths per 10,000 people, respectively, which are 1.82 times and 1.38 times as many as SC (8.57 deaths per 10,000 people) and the net food-consuming (FC) region (10.8 deaths per 10,000 people), respectively. The disparities in A–D-mortality are smaller, where the rate of 14.2 deaths per 10,000 people in FP is 1.35 times that of 10.5 deaths per 10,000 people in FC. In China’s internal food trade, the generally poorer FP produces excess food to supply the richer FC while meeting its own demand; the food demand and supply in FB, the poorest of all, are mostly balanced36. Environmental pressures induced by food demand would be partially transferred from FC to FP via food trade, possibly resulting in unequal health impacts of PM2.5; as shown above, dietary changes have widened such unequal allocation. On the other hand, developing non-agricultural sectors, including industries and services, often lead to income growth and subsequently increase the opportunity cost of agricultural production37. Therefore, the grain output of the more developed FC has decreased in the past decades, while an increase ensues in FP38, further amplifying internal food trade and the pollution transfer embodied in it.
PM2.5-related health inequality
To quantify the PM2.5-related health inequality and the subsequent inequity, we examined the Lorenz curves and Gini coefficients. The Lorenz curve here is a cumulative PM2.5-related mortality distribution curve, and the Gini coefficient is derived from this curve, with values ranging from 0 to 1. A larger deviation of the curve from the diagonal line of equitable distribution corresponds to a higher Gini coefficient, indicating higher distribution inequality. With the horizontal axis representing A-mortality, A–D-mortality, and D-mortality rates, Fig. 2a–c shows the regional health inequality. The Gini coefficient of A-mortality is 0.197, higher than the 0.189 of A–D-mortality. Given the uneven distribution of D-mortality (Gini coefficient = 0.369), the absence of dietary changes potentially enhances the equity of PM2.5-related health outcomes. Figure 2d–f shows the health inequality associated with income. The Lorenz curve is close to the equitable line in Fig. 2d, e, while Fig. 2f shows a larger difference. According to the ranking of residents’ income, five income groups with the same population size have been divided from poor to rich (see income group distribution in Fig. S5). We found that 27.4% of the 359 cities belong to the poor group, which earns 10.7% of the total income and is linked to 17.6% of A-mortality, 17.7% of A–D-mortality, and 15.3% of D-mortality in 2010. Meanwhile, 10.3% of the cities belong to the rich group, which earns 36.0% of the total income and is linked to 19.6% of A-mortality, 19.8% of A–D-mortality, and 17.0% of D-mortality. The middle-income group (including the lower middle-, middle-, and middle high-income groups) earns 53.3% of the total income and is linked to 62.8% of A-mortality, 62.5% of A–D-mortality, and 67.7% of D-mortality. The increasingly disproportionate share among the income groups in D-mortality indicates that dietary changes could increase the disparities of PM2.5-related mortality among different income groups. Compared to A-mortality, A–D-mortality distributes more evenly among income groups (Fig. S6). Although the difference between A-mortality and A–D-mortality is small, our results indicate that PM2.5-related health impacts may distribute more evenly without the effects of dietary changes.

a, d Lorenz curves for all-cause PM2.5-related premature deaths (A-mortality); b, e Lorenz curves for PM2.5-related premature deaths without the effects of dietary changes (A–D-mortality); c, f Lorenz curves for PM2.5-related premature deaths specifically attributable to dietary changes (D-mortality). The horizontal axis is sorted according to a–c mortality rate and d–f per capita income. The diagonal is the absolute equitable line. The tables in d–f give the average mortality rate of five income groups for A-mortality and D-mortality, respectively.
As for the mortality rates of different income groups (Fig. 2), we found that middle-income regions tend to have higher values than low- and high-income regions. The middle-income regions suffer more air pollution, especially the middle high-income group. Comparable evidence has also been shown in previous studies in China via household surveys28 and on a global scale39, potentially linked to the rapid industrial expansion in middle-income regions. In China, industries are relocating from cities in high-income regions to cities in middle-income regions40, accompanied by a corresponding shift in pollution hotspots. On the other hand, the limited potential for developing manufacturing and agriculture in cities with low incomes (e.g., cities in Tibet and Qinghai) lead to cleaner air and less PM2.5-related mortality. The levels of air pollution are closely related to the regional industrial structure and economic growth. Middle-income regions, where manufacturing serves as the major industry, bear the heaviest air pollution burdens. Within these middle-income regions of China, a lot of areas (e.g., HHH and NE) also have high levels of agricultural production. Conversely, in low-income regions, economic activities are more limited, leading to relatively better air quality. This pattern aligns with the assumption of the environmental Kuznets curve (EKC), a concept we will explore further in the subsequent section.
Factors influencing PM2.5-related mortality induced by dietary changes
We applied multiscale geographically weighted regression (MGWR) and ordinary least-squares (OLS) models to examine the associations between A-mortality, D-mortality and sociodemographic, environmental factors. The dependent variables are D-mortality rates and A-mortality rates; independent variables include the urbanization rate, green space, medical resources, and income. All models include the same covariates (e.g., cropland ratio, building ratio, temperature, precipitation, relative humidity, road density, primary sector GDP per capita, secondary sector GDP per capita, share of primary sector in total GDP, population, and agricultural machinery). Due to missing data for the western regions of China (e.g., Tibet, Qinghai, and Xinjiang), only 306 cities (covering 96.8% of the population and 90.3% of total income) were considered. MGWR performs better than OLS: the R2 of MGWR models are 0.865 and 0.961for A-mortality and D-mortality, respectively, much higher than the 0.596 and 0.574 of OLS models (see MGWR and OLS results in Tables S2–S4, and Fig. S7). Figure 3 shows the profiles of the estimated local coefficients, and Figure S8 presents the spatial distribution of these coefficients. First, urbanization is positively correlated with D-mortality over the country, but this association weakens as income increases (Fig. 3a). However, we found an opposite association between the urbanization rate and A-mortality (Fig. 3e). Urbanization refers to the population migration from rural to urban areas; it is usually accompanied by dietary changes. Since urban residents tend to have more meat- and emission-intensive diets, urbanization would increase food demand and agricultural emissions in China41. Therefore, dietary changes combined with urbanization would induce more air pollution and subsequent health impacts. Urbanization is also often accompanied by a transition in energy consumption structure. Urban residents generally utilize cleaner energy structures with less solid fuel (biomass and coal combustion) and more liquefied petroleum gas and electricity than rural residents13. Such a transition compensates for people’s increased exposure to PM2.5 due to higher population density, ultimately allowing urbanization to mitigate PM2.5-related health impacts at a population level13.

a–d represent estimated coefficients of D-mortality on urbanization rate, green space, medical resources, and residents’ income. e–h are the same as a–d but for A-mortality. The Box–Whisker from the top to the bottom in the boxplot are upper limit, 75th percentile, median, 25th percentile, and lower limit. Points outside the upper and lower limits are outliers.
Green space has negative associations with both D-mortality and A-mortality (Fig. 3b, f). Green space has been shown to reduce the health impacts of air pollution by cleaning air, enhancing physical activities, and reducing mental stress16. However, our result further demonstrates that the benefit of greenspace is only valid in middle- to high- income regions, and the estimated coefficients become stronger as income increases (Fig. S8a, b). The availability of medical resources has a negative association with D-mortality (Fig. 3c), which becomes stronger as income decreases, with the low-income regions having the highest estimated coefficients. Low-income regions are also poor in healthcare resources; the health benefits of investing more healthcare resources there are likely to be greater. However, our result does not reveal any mitigation effects of medical resources on A-mortality (Fig. 3g). Similar results have also been reported in previous studies, which showed that PM2.5-related mortality can be mitigated by medical resources only in several capital cities and high-income cities, as many residents tend to visit regional center cities (e.g., provincial capitals) for healthcare42,43.
Figure 3d, h shows the mixed effects of income on D-mortality and A-mortality. Specifically, income has a positive association with D-mortality and A-mortality in low-income regions such as western China, but has a negative association in eastern China (Fig. S8h, i). Figure 4 further presents the clear inverted U-shape curves, fitted to a quadratic function, of income with D-mortality and A-mortality: economic growth initially leads to increasing mortality, but after a certain level of economic growth (turning point), the relationship is reversed. The association between economic development and PM2.5-related health impacts hypothesized by the environmental Kuznets curve (EKC) is thus clearly observed in China. The turning point of EKC comes earlier in D-mortality (at an income of 16,700 CNY per capita) than in A-mortality (17,300 CNY per capita), implying that fewer regions have crossed the turning point of A-mortality than D-mortality (Fig. S8h, i). According to EKC, as the economy of a region grows and as its industrial focus gradually shifts from the primary sectors (e.g., agriculture) via the secondary sectors (e.g., manufacturing) toward the service sectors, and the turning point often occurs during the final transition toward services44. As D-mortality is mostly associated with agriculture, the turning point may happen as soon as the industrial focus shifts away from agriculture.

The fitting equations are inserted in the figure: yA and yD represent A-mortality and D-mortality, respectively.
Conclusions and discussion
Over the past decades, the rapid urbanization and economic growth in China have been accompanied by massive energy consumption, which has led to heavy PM2.5 pollution and its associated health burdens. Yet, the extent of economic development varies vastly in space, leading to different levels of income, PM2.5 levels, and PM2.5-related health impacts in different regions45,46. Diverging patterns of development among regions have also increased inter-regional trade, which entails a corresponding transfer of air pollution. The less developed interior regions produce primarily energy-intensive and emission-intensive goods, and on average supply them to the coastal regions or export them to other countries47. Although this has helped the more developed coastal regions improve air quality and reduce PM2.5-related health burdens there, it has generated more air pollution in the less developed regions47, leading to PM2.5-related environmental and health inequity. Furthermore, urbanization and economic growth have also substantially modified people’s dietary patterns, mostly in the form of a widespread shift from a plant-based diet to a more meat-intensive diet over the past half-century, especially in the richer coastal regions. Our previous work has shown that such a shift, driven largely by the rising demand for animal products, has increased agricultural emissions and worsened PM2.5-related health impacts8. The increasing food demand from the more developed, net food-consuming regions is satisfied via trade by the supply from the net food-producing regions, which are often less developed48. Diets determine nutrient intake and thus affect health equity. Several studies have suggested that the availability, quality, and affordability of food are intimately linked to health equity. For instance, reductions in food prices have been found to substantially enhance health equity49. A global study suggested that although food system transformation has bolstered food accessibility, it has no discernible effects on health equity50. However, previous studies have mostly focused on health equity from the perspective of nutritional inequality, whereas the impacts of dietary changes on environmental and health inequity have been largely unquantified.
We examined the impacts of dietary shifts on PM2.5 levels via changing agricultural NH3 emissions. Figure S9 provides the effects of dietary changes on NH3 emissions between 1980 and 2010. Over this period, agricultural NH3 emissions rose from 6.4 Tg to 12.1 Tg, with ~70% attributable to dietary changes and ~30% to population growth. Dietary change-induced NH3 emissions exhibit obvious disparities across China. Notably, the largest increase occurred in HHH (1.34 Tg), followed by NE (0.81 Tg). Among food functional regions, FP experienced the most substantial impact, contributing to 79% of the rise in emissions. This unequal distribution of emissions leads to a disparate distribution of air pollution. A recent study has also verified that the air pollution related-health burden from China’s food system exhibits obvious inequality in the distribution across food supply and demand side, different regions, and income groups27. Dietary changes have heightened our food demand, consequently amplifying such inequality. Our results indicate that dietary changes could alter the distribution of PM2.5-related health impacts. The PM2.5-related mortality rate attributable to dietary changes (D-mortality) shows a clear spatial clustering, with a higher spatial autocorrelation than the all-cause PM2.5-related mortality rate with (A-mortality) and without the effects of dietary changes (A–D-mortality). The hotspot of A-mortality and D-mortality also differs, situated in the HHH and NE region, respectively. The D-mortality rate in NE is estimated as 1.26 deaths per 10,000 people, much higher than 0.66 deaths per 10,000 people of the national average. Such a result demonstrates that NE, an important food production region, is the most affected by dietary change-related air pollution. We further used the Gini index to quantify the unequal distribution of mortality: A-mortality has a higher Gini index and is thus associated with higher health inequality than A–D-mortality. The Lorenz curves further indicate that the disparities in A-mortality among different income groups are more prominent than those in A–D-mortality, reflecting the worsening potential of PM2.5-related health inequality by dietary changes via their impacts on agricultural emissions.
Spatially, the uneven distribution of agricultural endowments (e.g., water or arable land) in China has contributed to inequitable agricultural production51. According to agricultural statistics33, the grain output of the less developed FP regions has increased from 69% of the national total in 1980 to 75% in 2010. The proportion of national meat production attributable to FP remained stable at approximately 68% during 1980–2010, while FC experienced a decline in its share from 16% in 1980 to 12% in 2010. Yet, the high food demand from the more developed FC regions burdens the food systems disproportionately, leading to more agricultural emissions and PM2.5-related health impacts in FP regions. Thus, dietary changes ultimately amplify PM2.5-related health inequity via uneven agricultural production and consumption in China. Such an amplification should be taken into account when policy makers formulate measures to reduce social inequity embedded within the food and environmental systems. At large, environmental pollution and food security are highly intertwined, and we suggest that an integrated approach addressing them synergistically is necessary to achieve sustainable development and a more equitable society.
Certain environmental and sociodemographic factors can modulate the health impacts induced by PM2.5. Our findings imply that A-mortality and D-mortality have close and spatially heterogeneous relationships with urbanization rate, green space, medical resources, and residents’ income. Moreover, our results provide empirical evidence for the EKC hypothesis. This does not imply that tackling environmental degradation simply requires economic growth. Previous studies have indeed proposed and empirically verified the pollution haven hypothesis52: pollution is unlikely to be eliminated as income grows, as it tends to be transferred to other regions where environmental regulations are lax, either within a given country or internationally. In China, many of the manufacturing industries have already moved from the high-income eastern coastal regions to the middle-income interior parts of China40, accompanied by a transfer of pollution to these regions53. Similarly, food production in the more developed FC regions has also shifted toward the middle-income FP regions (e.g., HHH and NE), and to a lesser extent toward the even poorer FB regions (e.g., NW including Xinjiang, Gansu, and the western parts of Inner Mongolia) despite lower land productivity and higher natural risks34,38. Coupled with the rising food demand from FC regions, the environmental costs and inequity arising from the shifts of food production may be underestimated.
Our study has several limitations regarding data collection and model application. First, although MGWR was applied to reduce the impacts of the common problems in aggregated data, such as the modifiable areal unit problem (MAUP)54,55, our results might still be affected by MAUP, namely, that research outcomes might differ due to the use of areal units of different spatial scales (e.g., city level or county level). Second, due to data limitation, only 306 cities were analyzed in our statistical models. However, these 306 cities already account for 98.6% and 99.7% of A-mortality and D-mortality, respectively, so our major findings and conclusions should not be affected. Third, the mortality estimation has uncertainties resulting from the Global Burden of Disease (GBD) and global exposure mortality model (GEMM)1. GEMM is based on global cohort studies and may introduce biases when applied to China due to disparities in PM2.5 components, toxicities, and healthcare levels. For instance, ammonium is mainly derived from agriculture, second only to organic carbon in toxicity, and its effects have strong spatial heterogeneity56. Moreover, we only considered D-mortality arising from agricultural NH3 emissions, but nitrogen oxides (NOx) are also generated from agriculture and can worsen PM2.5 pollution. For these reasons, the PM2.5-related health impacts and inequity arising from dietary changes may be underestimated. Regarding the dietary change-related NH3 emissions, we assumed that the dietary structure of residents is the same nationwide to calculate the emission changes caused by dietary changes from 1980 to 2010, because no region-specific data on dietary composition are available. Variations in diets across different regions could introduce additional uncertainty in the estimates of corresponding NH3 emissions in production, but this is mitigated by the assumption of free inter-provincial food trade8. The simulated PM2.5 is also constrained by the limitations is computing resources and input data to a resolution of 0.1° × 0.1°, which is inadequate to support the analysis of distribution between urban and rural areas within the same grid cell.
Policy implications
Environmental justice posits that all individuals merit equal safeguarding from environmental pollution. Disparities in air pollution exposure exist globally among communities and regions, resulting in health inequality. Implementing targeted intervention strategies can effectively mitigate the health impacts and disparities arising from air pollution. For example, the Climate and Economic Justice Screening Tool (CEJST) policy, launched by the US, aims to identify disadvantaged areas in environmental pollution and prioritize providing policy and financial support to these areas to alleviate environmental pollution57. Based on our analysis of the factors driving PM2.5-related mortality, urban green space plays a pivotal role in mitigating the health effects of air pollution, thus promoting equitable access to green space within cities is particularly meaningful. Notably, our findings indicate that urban green space have a pronounced effect in the eastern regions of China (more developed regions) characterized by higher urbanization compared to the western regions. Hence, the planning of green space should be a focal point in the future urbanization process of the western regions. In addition, the judicious allocation of resources and industries is vital, encompassing more equitable distribution of medical resources and management of pollution-intensive industries. Particularly in rapidly developing regions, strengthening environmental regulations concurrently with industrial transfer and expansion is crucial for avoiding the challenges of “control pollution after development”.
The persistent disparities in pollution distribution within China’s food systems could be exacerbated by agricultural intensification, driven by a growing spatial mismatch between producers and consumers. Hence, designing policies for balancing agricultural production, pollution abatement, and equitable distribution is an urgent pursuit. In the short term, rectifying this unequal distribution proves challenging. First, economic measures to compensate the disproportionate health impacts borne by farmers and agricultural regions should be implemented. Additionally, reducing pollutant emissions from the food systems requires immediate actions. Mitigating food loss and waste and promoting planetary health diet on the demand side, coupled with structuring an efficient food supply chain, can substantially alleviate the environmental footprints of the food systems. Enhancing agricultural production efficiency through technologies such as mechanization, automation, and moderate-scale operations can not only boost yields but also curb pollutant emissions. In the long term, achieving a transformative shift in the food systems mandates prioritizing rational spatial planning for agricultural activities. Relocating crop cultivation based on local conditions can unlock production potential while ensuring reduced and more even pollutant distribution. Moreover, arranging vegetable and meat production near consumers can stabilize the food supply and mitigate pollution disparities effectively. This approach, known as the “Vegetable Basket Plan”, has been implemented by the Chinese government across many regions58.
To reverse the heavy haze pollution problems, the Chinese government has targeted the energy and transportation sectors and launched a series of clean air actions, which have successfully reduced the emissions various pollutants including NOx and SO217, lessening the issue of polluting industries being transferred to poorer parts of China and the inequity therein59. However, the inequity embedded within the food systems and their pollution remains unresolved, and is possibly worsening. Therefore, another challenge is that policy makers need to recognize the roles of agricultural management in air pollution control, especially for agricultural nitrogen emissions. In 2023, China announced new clean air actions, which included agricultural NH3 as a target for the first time60. Specific targets have been assigned only to the Beijing-Tianjin-Hebei region, with a goal of 5% reduction by 2025 compared to 2020 levels. Greater efforts are still much needed to mitigate air pollutant emissions from the food systems. A sustainable food system ensures food security and nutrition for all without compromising the economic, social and environmental foundations required to sustain the well-being of present and future generations61, and is essential to help society achieve multiple sustainable development goals (SDGs), most prominently SDG2 “Zero Hunger”, SDG3 “Good Health and Well-being”, SDG13 “Climate Action”, and SDG1 “No Poverty”. The importance of food system transformation in addressing SDG10 “Reduced Inequalities”, especially with an emphasis on food consumption and transition toward “planetarily healthy diets”, has long been overlooked, and our findings point specifically to such importance.
Materials and methods
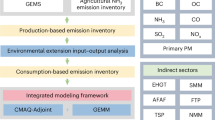
Study framework and datasets
Our previous work has estimated the PM2.5-related mortality in China to be 1.83 million deaths in 2010, 5% of which could be attributable to dietary changes8. Such mortality is highly unevenly distributed across space and income groups; thus to better understand this distribution, here we divided China into six agricultural sub-regions based on the characteristics of agricultural production35, i.e., Huang–Huai–Hai (HHH), Middle and Lower Yangtze River (MLYR), Northeast (NE), Northwest (NW), Southwest (SW), and South China (SC). According to agricultural endowments and their roles in the intra-China food trade, three food functional sub-regions have also been grouped: a net food-producing region (FP) produces food to meet local and non-local demand; a net food-consuming region (FC) cannot achieve self-sufficient food supply and needs to import food from elsewhere; a food-balanced (FB) region means that the local food supply can satisfy the demand but with no surplus for export. The boundaries for these sub-regions in China can be found in Fig. 1e, f. The food functional sub-region classification by the Chinese government in 2003 was intended to enhance China’s grain production by concentrating resources in FP36. Two decades of investments have made FP the main contributor to grain production and meat production, responsible for 78% and 66% of domestic grain and meat production, respectively, exemplifying its substantial roles in the agricultural sector. Multi-source datasets were integrated to quantify PM2.5-related health inequality and contribution of major drivers to PM2.5-related mortality at the city level in 2010. We employed Moran’s I to explore the spatial patterns of gridded PM2.5-related mortality data and then aggregated premature deaths at the city level. We further obtained several environmental and sociodemographic factors from national statistical data (https://data.stats.gov.cn/english/) and city statistical yearbooks62, including urbanization rate, green space, medical resources, income, urban–rural income gap, cropland ratio, building ratio, temperature, precipitation, relative humidity, road density, primary sector GDP per capita, secondary sector GDP per capita, share of primary sector in total GDP, population, and agricultural machinery. The data of 306 cities in China were used in this study, and the data profile can be found in Table S5.
In our previous work we robustly estimated dietary change-related agricultural NH3 emissions, which served as input to a high-resolution air quality model to simulate the corresponding PM2.5 changes8. Here, the PM2.5-related health burdens were projected at the grid cell level based on the concentration–response functions, and then, the gridded data of mortality was aggregated at the city level in China for further analysis of inequality and driving factors. The Lorenz curve and Gini coefficient were applied to quantify spatial and income group disparities. Statistical models are employed to analyze the relationships between mortality rate and various driving factors. The methodological framework is summarized in Fig. S1.
PM2.5 concentrations and associated mortality rates
The gridded PM2.5-related mortality datasets were from our previous work with detailed description therein8. In brief, we employed the GEOS-Chem chemical transport model to simulate PM2.5 concentrations in year 2010 using an agricultural NH3 emission inventory generated by a crop-specific and livestock-specific NH3 emission model for China63, as well as various other inventories for other atmospheric species. Simulated concentrations were bias-corrected using the Data Integration Model for Air Quality (DIMAQ)64 at 0.1° × 0.1° resolution. To obtain PM2.5-related mortality driven by dietary changes alone, we first utilized actual agricultural activity data from 2010 to generate agricultural NH3 emissions and simulate PM2.5 levels for 2010 (denoted as [S1]). Then, we considered a counterfactual scenario, where Chinese residents maintained their dietary patterns in early 1980s, to generate agricultural NH3 emissions in accordance with early-1980s diets and simulate PM2.5 accordingly (denoted as [S2]), keeping all other conditions the same as [S1]. The all-cause PM2.5 concentrations with and without dietary changes were thus the PM2.5 concentrations from [S1] and [S2], respectively, and dietary change-related PM2.5 is the PM2.5 from [S1] minus that from [S2].
We then applied the concentration–response functions of the global exposure mortality model (GEMM)1 to the simulated PM2.5 concentrations to obtain the all-cause PM2.5-related mortality with (A-mortality) and without (A–D-mortality) dietary changes, and PM2.5-related mortality caused by dietary changes (D-mortality) across the country. The GEMM model first estimates the relative risk (RR) of different annual PM2.5 levels, and then RR is combined with the baseline mortality rate of PM2.5-related disease (γ) and population (P) to project mortality (M):
Where z is the PM2.5 concentration; zcf represents the theoretical counterfactual PM2.5 concentration; α, β, μ, and v are the fitting parameters from GEMM1.
Lorenz curves and Gini coefficients
We applied the Lorenz curve and the Gini coefficient to quantify PM2.5-related health inequality. Lorenz first proposed the Lorenz curve to evaluate income inequality among the population65, which has since also been widely used in fields of energy and resource use66,67. In the context of health risk here, the vertical axis represents the cumulative share of PM2.5-related mortality, while the horizontal axis stands for the cumulative share of people (ranked by mortality rate or income status). This curve helps us identify the distribution of PM2.5-related mortality in different population groups. The greater the deviation of the Lorenz curve from the absolute equitable line (diagonal line), the higher the inequality. Based on the Lorenz curve, the Gini coefficient is a numerical representation of this inequality, calculated as:
where M is the PM2.5-related mortality rate (ratio of annual premature deaths to total population); Mi and Mj represent the mortality rate of the city i and j; M̅ stands for the average mortality rate for all cities; n is the total number of cities.
Selected environmental and sociodemographic factors
We selected 16 potential driving factors in three major aspects. Urban green space refers to the proportion of green space in the urban built-up area derived from the city statistical yearbooks of China. The cropland and building area ratios are the cropland and built-up ratio to the total area of a city. These three indicators are expected to represent landscape features. Meteorological factors include annual averages of temperature, precipitation, and relative humidity for cities. Variables related to socioeconomic activities include the following. The urbanization rate is the population urbanization rate calculated as the ratio of the urban population to the total population of a city. Road density describes the local accessibility (either to hospitals or to transport facilities), calculated as the road length per unit area. The primary sector GDP per capita and secondary sector GDP per capita are the gross domestic product (GDP) of the primary (e.g., agriculture) and secondary (e.g., manufacturing) sectors per capita. These two factors and the share of the primary sector in total GDP is expected to represent the local industrial structure. Agricultural machinery is calculated as the power consumption of agricultural machinery per 10,000 CNY of agricultural output. The larger the value, the higher the degree of agricultural mechanization. Medical resources are represented by the number of medical beds each city has. Residents’ income is the disposable income (net income) per capita. The urban–rural income gap is the ratio of urban residents’ per capita income to rural residents’ per capita income. All these socioeconomic indicators were derived from the city statistical yearbooks of China. The description of indicators can also be found in Table S6.
Statistical models
Multiscale geographically weighted regression (MGWR) is an advanced version of geographically weighted regression (GWR). It is a local regression model that allows all objects to have their local coefficients of explanatory variables. Each explanatory variable may operate at a different spatial scale (bandwidth)68. We employed MGWR to address the spatial effects of influencing factors on PM2.5-related mortality. The regression formula of MGWR is as follows:
where i and j represent different cities and explanatory variables, respectively; bwj refers to the bandwidth of the jth variable, which is determined by a backfitting algorithm. Within bandwidth, the weight of cities in regression is decided by a spatial kernel function. The closer they are, the more impact they have. βbwj indicates the jth coefficient; xij indicates the jth explanatory variable in region i; εi is the random error. We also applied an ordinary least-squares (OLS) model as a comparison, and its general form is shown in Eq. (3). The goodness-of-fit measures, Akaike Information Criterion (AIC) and R2, were employed to assess the fitting performance. In the statistical analysis, the dependent variables are the all-cause PM2.5-related mortality rate (A-mortality) or the PM2.5-related mortality rate attributable to dietary changes (D-mortality), while the independent variables include urbanization rate, greenspace, medical resources, and income. All models have the same control variables (i.e., the other environmental and sociodemographic variables listed above).
Data availability
The source data for all figures and results in this paper are available at ref. 69.
Code availability
The codes for creating figures in this paper are available at ref. 69.
References
Burnett, R. et al. Global estimates of mortality associated with longterm exposure to outdoor fine particulate matter. Proc. Natl Acad. Sci. USA 115, 9592–9597 (2018).
Bu, X. et al. Global PM2.5-attributable health burden from 1990 to 2017: Estimates from the Global Burden of disease study 2017. Environ. Res. 197, 111123 (2021).
Yin, H. et al. Population ageing and deaths attributable to ambient PM2·5 pollution: a global analysis of economic cost. Lancet Planet. Health 5, e356–e367 (2021).
Yang, H., Huang, X., Westervelt, D. M., Horowitz, L. & Peng, W. Socio-demographic factors shaping the future global health burden from air pollution. Nat. Sustain. 6, 58–68 (2022).
Cohen, A. J. et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015. Lancet 389, 1907–1918 (2017).
Azimi, M., Feng, F. & Zhou, C. Air pollution inequality and health inequality in China: An empirical study. Environ. Sci. Pollut. Res. 26, 11962–11974 (2019).
Yang, T. & Liu, W. Does air pollution affect public health and health inequality? Empirical evidence from China. J. Clean. Prod. 203, 43–52 (2018).
Liu, X. et al. Dietary shifts can reduce premature deaths related to particulate matter pollution in China. Nat. Food 2, 997–1004 (2021).
Braveman, P. Health disparities and health equity: Concepts and measurement. Annu. Rev. Public Health 27, 167–194 (2006).
Bartley, M. Health inequality: an introduction to concepts, theories and methods. J. Epidemiol. Community Health 59, 711 (2005).
Jiang, X., Fu, W. & Li, G. Can the improvement of living environment stimulate urban Innovation?—Analysis of high-quality innovative talents and foreign direct investment spillover effect mechanism. J. Clean. Prod. 255, 120212 (2020).
Zhang, Z., Shao, C., Guan, Y. & Xue, C. Socioeconomic factors and regional differences of PM2.5 health risks in China. J. Environ. Manag. 251, 109564 (2019).
Shen, H. et al. Urbanization-induced population migration has reduced ambient PM2.5 concentrations in China. Sci. Adv. 3, 1–13 (2017).
Dong, E. et al. Differences in regional distribution and inequality in health-resource allocation at hospital and primary health centre levels: a longitudinal study in Shanghai, China. BMJ Open 10, e035635 (2020).
Zhang, T., Xu, Y., Ren, J., Sun, L. & Liu, C. Inequality in the distribution of health resources and health services in China: hospitals versus primary care institutions. Int. J. Equity Health 16, 42 (2017).
Braubach, M. et al. Effects of Urban Green Space on Environmental Health, Equity and Resilience. 187–205 https://doi.org/10.1007/978-3-319-56091-5_11 (2017).
Zhang, Q. et al. Drivers of improved PM2.5 air quality in China from 2013 to 2017. Proc. Natl Acad. Sci. USA 116, 24463–24469 (2019).
Geng, G. et al. Drivers of PM2.5 air pollution deaths in China 2002–2017. Nat. Geosci. 14, 645–650 (2021).
Zheng, Y. et al. Air quality improvements and health benefits from China’s clean air action since 2013. Environ. Res. Lett. 12, 114020 (2017).
Wu, Y. et al. PM2.5 pollution is substantially affected by ammonia emissions in China. Environ. Pollut. 218, 86–94 (2016).
Zheng, H. et al. Transition in source contributions of PM2.5 exposure and associated premature mortality in China during 2005–2015. Environ. Int. 132, 105111 (2019).
Springmann, M. et al. The global and regional air quality impacts of dietary change. Nat. Commun. 14, 6227 (2023).
Sun, Z. et al. Dietary change in high-income nations alone can lead to substantial double climate dividend. Nat. Food 3, 29–37 (2022).
Zhao, H. et al. Imbalanced transfer of trade-related air pollution mortality in China. Environ. Res. Lett. 15, 094009 (2020).
Oita, A. et al. Substantial nitrogen pollution embedded in international trade. Nat. Geosci. 9, 111–115 (2016).
Dalin, C. & Rodríguez-Iturbe, I. Environmental impacts of food trade via resource use and greenhouse gas emissions. Environ. Res. Lett. 11, 035012 (2016).
Zheng, L. et al. Health burden from food systems is highly unequal across income groups. Nat. Food 5, 251–261 (2024).
Jiao, K., Xu, M. & Liu, M. Health status and air pollution related socioeconomic concerns in urban China. Int. J. Equity Health 17, 18 (2018).
Zhao, H. et al. Inequality of household consumption and air pollution-related deaths in China. Nat. Commun. 10, 4337 (2019).
Kong, L. et al. Improved inversion of monthly ammonia emissions in china based on the Chinese Ammonia Monitoring Network and Ensemble Kalman Filter. Environ. Sci. Technol. 53, 12529–12538 (2019).
Zhang, L., Zhang, X., Gao, Q. & Yan, L. Nitrogen application effect on maize yield, NH3, and N2O emissions in Northeast China by meta-analysis. Agronomy 13, 1479 (2023).
Wang, C. et al. An empirical model to estimate ammonia emission from cropland fertilization in China. Environ. Pollut. 288, 117982 (2021).
NBSC. National Bureau of Statistics of China. http://www.stats.gov.cn/english/ (2023).
Li, Y., Li, X., Tan, M., Wang, X. & Xin, L. The impact of cultivated land spatial shift on food crop production in China, 1990–2010. L. Degrad. Dev 29, 1652–1659 (2018).
Wang, C. et al. Ammonia emissions from croplands decrease with farm size in China. Environ. Sci. Technol. 56, 9915–9923 (2022).
The division of grain production sub-regions need to be improved. https://www.moa.gov.cn/ztzl/ymksn/jjrbbd/202308/t20230803_6433429.htm.
Chen, Y. & Li, X. Spatial-temporal characteristics and influencing factors of grain yield change in China. Agric. Eng. 29, 1–10 (2013).
Wang, J., Zhang, Z. & Liu, Y. Spatial shifts in grain production increases in China and implications for food security. Land Use Policy 74, 204–213 (2018).
Rentschler, J. & Leonova, N. Global air pollution exposure and poverty. Nat. Commun. 14, 4432 (2023).
Liu, Y. & Dong, F. How industrial transfer processes impact on haze pollution in China: An analysis from the perspective of spatial effects. Int. J. Environ. Res. Public Health 16, 423 (2019).
Cui, S. et al. A hybrid method for quantifying China’s nitrogen footprint during urbanisation from 1990 to 2009. Environ. Int. 97, 137–145 (2016).
Bei di, D., Lei, D. & Jinhua, C. Differences of PM2. 5 health risks and influencing factors in different types of cities. China Popul. Environ. 31, 90–100 (2021).
Xia, F., Xing, J., Xu, J. & Pan, X. The short-term impact of air pollution on medical expenditures: evidence from Beijing. J. Environ. Econ. Manag. 114, 102680 (2022).
Kaika, D. & Zervas, E. The Environmental Kuznets Curve (EKC) theory—Part A: concept, causes and the CO2 emissions case. Energy Policy 62, 1392–1402 (2013).
Lu, D., Xu, J., Yang, D. & Zhao, J. Spatio-temporal variation and influence factors of PM2.5 concentrations in China from 1998 to 2014. Atmos. Pollut. Res. 8, 1151–1159 (2017).
Wang, S., Zhou, C., Wang, Z., Feng, K. & Hubacek, K. The characteristics and drivers of fine particulate matter (PM2.5) distribution in China. J. Clean. Prod. 142, 1800–1809 (2017).
Wang, H. et al. Trade-driven relocation of air pollution and health impacts in China. Nat. Commun. 8, 738 (2017).
Wu, S. et al. Virtual land, water, and carbon flow in the inter-province trade of staple crops in China. Resour. Conserv. Recycl. 136, 179–186 (2018).
Lee, A., Patay, D., Herron, L.-M., Parnell Harrison, E. & Lewis, M. Affordability of current, and healthy, more equitable, sustainable diets by area of socioeconomic disadvantage and remoteness in Queensland: insights into food choice. Int. J. Equity Health 20, 153 (2021).
Ambikapathi, R. et al. Global food systems transitions have enabled affordable diets but had less favourable outcomes for nutrition, environmental health, inclusion and equity. Nat. Food 3, 764–779 (2022).
Zhu, X., Li, Y., Li, M., Pan, Y. & Shi, P. Agricultural irrigation in China. J. Soil Water Conserv. 68, 147A–154A (2013).
Eskeland, G. S. & Harrison, A. E. Moving to greener pastures? Multinationals and the pollution haven hypothesis. J. Dev. Econ. 70, 1–23 (2003).
Liao, H., Yang, L., Dai, S. & Van Assche, A. Outward FDI, industrial structure upgrading and domestic employment: empirical evidence from the Chinese economy and the belt and road initiative. J. Asian Econ. 74, 101303 (2021).
Fotheringham, A. S. & Sachdeva, M. Scale and local modeling: new perspectives on the modifiable areal unit problem and Simpson’s paradox. J. Geogr. Syst. 24, 475–499 (2022).
Mansour, S., Al Kindi, A., Al-Said, A., Al-Said, A. & Atkinson, P. Sociodemographic determinants of COVID-19 incidence rates in Oman: Geospatial modelling using multiscale geographically weighted regression (MGWR). Sustain. Cities Soc. 65, 102627 (2021).
Yang, J. et al. Fine particulate matter constituents and cause-specific mortality in China: A nationwide modelling study. Environ. Int. 143, 105927 (2020).
Wang, Y. et al. Air quality policy should quantify effects on disparities. Science 381, 272–274 (2023).
Bai, Z. et al. Relocate 10 billion livestock to reduce harmful nitrogen pollution exposure for 90% of China’s population. Nat. Food 3, 152–160 (2022).
Shi, S. et al. Evolution in disparity of PM2.5 pollution in China. Eco-Env. Health 2, 257–263 (2023).
Council. Action Plan for Continuous Improvement of Air Quality. https://www.gov.cn/zhengce/content/202312/content_6919000.htm (2023).
Nguyen, H. Sustainable food systems: Concept and framework. Food Agric. Organ. United Nations Rome, Italy (2018).
National Bureau of Statistics of China. China City Statistical Yearbook 2011. (China Statistics Press, 2011).
Zhang, L. et al. Agricultural ammonia emissions in China: Reconciling bottom-up and top-down estimates. Atmos. Chem. Phys. 18, 339–355 (2018).
Shaddick, G. et al. Data Integration for the Assessment of Population Exposure to Ambient Air Pollution for Global Burden of Disease Assessment. Environ. Sci. Technol. 52, 9069–9078 (2018).
Gastwirth, J. L. The Estimation of the Lorenz Curve and Gini Index. Rev. Econ. Stat. 54, 306 (1972).
Wang, Q. et al. Examining energy inequality under the rapid residential energy transition in China through household surveys. Nat. Energy 8, 251–263 (2023).
Chen, B. et al. Contrasting inequality in human exposure to greenspace between cities of Global North and Global South. Nat. Commun. 13, 4636 (2022).
Fotheringham, A. S., Yang, W. & Kang, W. Multiscale Geographically Weighted Regression (MGWR). Ann. Am. Assoc. Geogr. 107, 1247–1265 (2017).
Luo, B. The source data and ploting codes for ‘Dietary changes are associated with an increase in air pollution-related health and environmental inequity in China’ published in communications earth & environment. https://doi.org/10.6084/m9.figshare.28079171.v1 (2024).
Acknowledgements
This work was supported by the General Research Fund from the Hong Kong Research Grants Council (RGC) (reference No. 14307722) granted to APKT. It was also supported by other grants from the RGC (General Research Fund, reference No. 14605920 14611621, 14606922, and 14603724; Collaborative Research Fund, reference No. C4023-20GF; Research Matching Grants, reference No. 8601219, 8601242, 3110151), a grant from the Research Committee on Research Sustainability of Major Research Grants Council Funding Schemes (reference No. 3133235) of The Chinese University of Hong Kong (CUHK), and a grant from the Vice-Chancellor's One-off Discretionary Fund (Smart and Sustainable Cities: City of Commons) (4930787) of CUHK. J.W.H. is supported by an RGC Postdoctoral Fellowship awarded by the Research Grants Council of Hong Kong (reference No. PDFS2425-4H01).
Author information
Authors and Affiliations
Contributions
A.P.K.T. and M.P.K. conceived the study and supervised the writing of the paper. B.L. designed the study, conducted model simulations, analyzed the results, and wrote the paper draft. J.W.H. designed the study, analyzed the results, and revised the draft. X.Y.L. provided and analyzed PM2.5-related mortality datasets.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Communications Earth & Environment thanks Lianming Zheng, Ciro Bustillo-LeCompte and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Primary Handling Editors: Paula Prist and Martina Grecequet. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Luo, B., Huang, J., Liu, X. et al. Dietary changes are associated with an increase in air pollution-related health and environmental inequity in China. Commun Earth Environ 6, 79 (2025). https://doi.org/10.1038/s43247-025-02050-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s43247-025-02050-5
This article is cited by
-
Reactive Nitrogen from Agriculture: A Review of Emissions, Air Quality, and Climate Impacts
Current Pollution Reports (2025)
