
Abstract
Background
Urinary tract infections (UTI) are the most frequently diagnosed infection in residents of long-term care and are a major risk factor for urosepsis, hospitalisation, and death. Translocation of gut pathobionts into the urinary tract is the presumed cause of most UTIs. While specific gut microbiota characteristics have been linked to UTI risk in younger adults, their relevance in aged care residents remains uncertain.
Methods
The faecal microbiome was assessed in 54 long-term aged care residents with a history of UTIs and 69 residents without a UTI history. Further comparisons were made to microbiome characteristics in 20 younger adults without UTIs. Microbiome characteristics were examined in relation to prior and subsequent UTIs, as well as antibiotic therapy.
Results
In long-term aged care residents, prior UTI history and exposure to UTI-exclusive antibiotics do not significantly affect microbiome composition or functional capacity. However, exposure to antibiotics unrelated to UTI treatment is associated with distinct microbiota compositional traits. Adjustment for dementia, incontinence, diabetes, and prior antibiotic use finds no microbiota characteristic linked to UTI development. However, prior UTI is identified as a predictor of future UTIs. Comparison with younger adults identifies greater within-participant dispersion in aged care residents, as well as lower microbiota diversity and altered microbiome functional potential.
Conclusions
No association between the gut microbiome and UTI incidence, as has been reported in younger individuals, is evident in long-term aged care residents. Considerable variability in gut microbiome characteristics, relating to high antibiotic exposure and age-related physiological and immunological factors, could mask such a relationship. However, it cannot be discounted that increased UTI risk in the elderly is independent of microbiome-mediated mechanisms.
Plain language summary
Urinary tract infections (UTIs) are common in residents of long-term aged care facilities, posing serious health risks. Harmful bacteria moving from the gut to the urinary tract is thought to cause most UTIs. It is still unclear, however, how differences in gut bacteria contribute to UTI risk in older adults. Here, we investigate the gut bacteria of aged care residents, both with and without a history of UTIs, and compare them to younger adults. While prior UTIs did not alter gut bacteria, antibiotic use did. We observed greater variability in gut bacteria among aged care residents compared to younger adults. These observations suggest that both high antibiotic exposure and age-related factors may mask any potential relationship between gut bacteria and UTI risk in this population. Understanding these factors could lead to improved UTI prevention and treatment strategies for elderly individuals.
Similar content being viewed by others

Introduction
Urinary tract infections (UTIs) are amongst the most common bacterial infections treated in hospital and community settings1 and a major contributor to antibiotic prescribing2,3. UTIs occur when bacteria, most commonly uropathogenic Escherichia coli (UPEC), proliferate in the urinary tract. If left untreated, UTIs can lead to pyelonephritis and urosepsis, which can be life-threatening4. Up to 30% of sepsis cases originate from the urinary tract, with an estimated mortality ranging from 20% to 40%5,6,7.
UTIs are a considerable concern among elderly individuals. The incidence of UTIs increases with age and represents the third leading cause of infection-related hospitalisations8,9. Moreover, older hospitalized patients ( >85 years) have a higher risk of developing uroseptic shock than younger patients ( < 65 years), which is associated with longer hospital stays and higher mortality10. UTIs represent a significant proportion of acquired infections in aged care residents, comprising over one-third of total cases9. High rates of cognitive decline, frailty, and medical comorbidities among this population not only increases the risk of UTI complications but also poses challenges for clinical assessment11,12. Consequently, empirical antibiotic therapy is often used even in the absence of confirmatory pathology or clear clinical symptoms.
The lower intestinal tract serves as a reservoir for UPEC and other UTI-causing bacteria, including other members of the Enterobacteriaceae family and some Enterococcus species4,13. The gut microbiome plays a crucial role in controlling the colonization and proliferation of pathogenic bacteria in the gut, particularly through the suppression of their growth by commensal anaerobic taxa14,15,16. Recent studies have explored this role of gut microbiome in the development of UTIs. Magruder and colleagues identified gut uropathogen abundance as an independent risk factor for the development of bacteriuria and UTI in kidney transplant recipients17. Additionally, Worby and colleagues found that lower microbial richness and a reduced prevalence of butyrate-producing bacteria were significantly associated with recurrent UTI in younger women18. However, how the microbiome influences the risk of UTI in elderly individuals, a population at high risk of both UTI and its severe complications, remains unexplored.
In this study, we test the null hypothesis that UTI risk is independent of gut microbiome characteristics. We aim to determine whether a history of UTI is associated with disruption of gut microbiome composition and functional potential, and whether specific microbiome features predict future UTI. We compare faecal microbiome characteristics of 69 age- and sex-matched aged care residents with no UTI history to those of 54 individuals who experienced UTI within 12 months of sample collection. Additionally, we examine the relationship between UTI incidence and antibiotic treatment, and assess the predictive value of prior UTI on microbiome composition, and microbiome composition on future UTI risk. Our comparison with a younger cohort reveals a substantially more dispersed stool microbiome in aged care residents, possibly due to high antibiotic exposure and age-related physiological and immunological factors. Despite these variations, antibiotics, rather than UTIs, drive gut microbiome changes. Furthermore, neither the presence of uropathogens nor specific compositional characteristics significantly link to future UTI risk. While microbiome-UTI relationships observed in younger adults are absent in our study, we acknowledge the possibility of UTI risk in the elderly being independent of microbiome-mediated mechanisms.
Methods
Aged care resident cohort
Participants were recruited and stool collected as part of the Generating evidence on Resistant bacteria in the Aged Care Environment (GRACE) study19. GRACE was a cross-sectional study in long-term aged care in metropolitan South Australia, conducted between March 2019 and March 2020. Participants were ineligible if they were in respite care, receiving palliative care, or where third-party consent was not obtained when required. The sample size calculation for GRACE was based on a permutational ANOVA (PERMANOVA) for testing the association between gut microbiome Bray-Curtis dissimilarity and antibiotic exposure. A total of 200 participants provided 86% power to detect a between group difference with a 2-sided type 1 error rate of alpha=0.05. All participants provided consent to the study through written consent themselves, or where third-party consent was required, a legal guardian or family member with power of attorney provided consent on their behalf. Consent was for use of samples to determine the relationship between microbiome composition and exposures including antimicrobial prescribing, clinical history, medications, and diet. The study was approved by the Southern Adelaide Clinical Human Research Ethics Committee (HREC/18/SAC/244).
Of 279 individuals assessed for eligibility, 137 were excluded due to a failure to obtain a stool sample, an unknown date of stool collection, catheterisation within the 24-month study period (12 months prior to, or following, stool collection), or a failure to obtain clinical data (Supplementary Fig. 1). Of the 142 individuals who were eligible to participate, 54 experienced one or more UTI during the 24-month study period. To form a “no UTI” comparator group, a subset of the 88 participants who did not experience a UTI were randomly selected (using RAND Excel function) to achieve a sex ratio that was equal to the case group. The age distribution of this comparator group, which contained 69 participants, was confirmed to be equivalent to that of the case group using the Kolmogrov-Smirnov normality test.
Participant data and UTI history
Participant data, including medication use, healthcare service utilisation (including pathology services), and comorbidities, were derived from the Pharmaceutical Benefits Scheme (PBS), Medicare Benefits Schedule (MBS), and Aged Care Funding Instrument (ACFI) assessment, respectively (Supplementary Table 1).
UTI was defined as pyuria ( >10 white blood cells per µL) and growth of >104 of a single or mixed pathogen/s, and/or prescription of a medication used exclusively in the treatment of UTIs, including trimethoprim, nitrofurantoin and/or methenamine hippurate. Other antibiotics were characterised by exposure to amoxicillin, amoxicillin/clavulanic acid, azithromycin, cefaclor, cefalexin, ceftriaxone, cefuroxime, ciprofloxacin, clarithromycin, clindamycin, doxycycline, erythromycin, flucloxacillin, metronidazole, norfloxacin, roxithromycin, and trimethoprim/sulfamethoxazole. Urosepsis was defined as bacteraemia with the same pathogen as cultured in urine culture during the same episode of care20.
Stool DNA extraction
All stool was collected and stored using Norgen Stool Nucleic Acid Collection and Preservation Tubes (Norgen Biotek, ON, Canada) as outlined in the Supplementary Methods. DNA was extracted using the Powerlyzer PowerSoil DNA Isolation Kit (Qiagen, Hilden, Germany) according to manufacturer’s specifications.
Shotgun metagenomic sequencing and bioinformatic processing
The microbiome was assessed by metagenomic sequencing using the Nextera XT DNA Library Prep Kit (Illumina, CA, USA) and sequenced on an Illumina Novaseq platform with 150 bp paired end reads as per manufacturer’s instructions. The resulting reads had a median read depth of 45.0 M reads per sample (interquartile range = 39.8–47.8 M). Metagenomic sequence data are accessible via the European Nucleotide Archive (ENA) under the accession number PRJEB51408, with sample accession numbers listed in Supplementary Data 1.
Sequences were quality-filtered using Trimmomatic (v0.39) and reads that aligned to the NCBI human reference genome (release GRCh38)21 were removed using Bowtie (v2.3.5.1)22. Microbiome taxonomic composition data were determined using MetaPhlAn (v3.0)23. Functional potential profiling of microbial communities was performed by HUMAnN (v3.0) against the MetaCyc database on all species detectable per sample with MetaPhlAn23. Along with untargeted analysis of the HUMAnN output, targeted analysis of functional pathway abundance was also performed, based on the involvement in short-chain fatty acid production (n = 22) as well as butyrogenic capacity alone (n = 7), which are hypothesised to be involved in UTI pathogenesis24.
The ‘vegan’ R package25 was used to determine alpha- and beta-diversity metrics. Alpha diversity included: species richness, Shannon’s diversity, Pielou’s evenness index, and Faith’s phylogenetic diversity, calculated from taxonomic relative abundances at the species level. Beta-diversity included Bray-Curtis dissimilarity index, calculated using square-root transformed species relative abundance data and metabolic pathway abundance data. The Bray-Curtis distance from centroid (the distance between a sample and the corresponding group centroid) was calculated from the Bray-Curtis dissimilarity index. Principal coordinate of analysis (PCoA) plots were applied to visualise compositional differences. The contribution of species to intestinal microbiome variance was determined by a correlation biplot using the ‘ape’ R package26. A correlation co-efficient cut-off of >0.25 was applied to filter for species that contribute to microbiome variance.
Quantitative PCR
Quantitative PCR (qPCR) was performed on DNA extracted from stool specimens for detection and enumeration of uropathogens (Supplementary Table 2). Enumeration of E. coli was performed using a validated Taqman Probe assay utilising KAPPA PROBE FAST ROX Low Master Mix reagents (Kapa Biosystems, Cape Town, South Africa)27. UPEC absolute abundance was determined as described28, with modifications. Briefly, 1 μL of DNA extract was added to 17.5 µL of KAPA Probe FAST (Sigma-Aldrich, Burlington, USA), 3.5 µL of each 5.0 µM primer, 5.25 µL of 7.5 µM TaqMan probe, and 4.25 µL of distilled water. All qPCRs were run in three technical replicates of 10 µL, on QuantStudio 6 Flex Real-Time PCR system (Applied Biosystems, Carlsbad, USA). Standard curves for both qPCRs were generated based on serial dilutions of ATCC strains of known concentrations of Escherichia coli (ATCC25922). The limit of quantification for E. coli and UPEC was 6.9 copies/mg stool and 54.6 copies/mg stool, respectively.
Non-elderly comparator cohort
Stool metagenomic sequencing data were compared to MetaPhlAn3 output from baseline samples from a healthy comparator group (n = 20, age range 21–57 years). Details of recruitment, sample collection and processing have been published as part of the IMPACT randomised controlled trial29. Briefly, participants were recruited between 1 February 2018 and 31 August 2018 and ethics was approved by institutional ethics committees (HREC/15/MHS/41) and registered with the Australian and New Zealand Clinical Trials Registry (ACTRN12617000278336). Additional consent was not required from participants for data comparisons.
Statistical analysis
Variance in Bray-Curtis dissimilarity between groups was determined using permutational multivariate analyses of variance (PERMANOVA) and dispersion (PERMDISP), using PRIMER-E (v7.0.21)30, with 9,999 random permutations. The contribution of bacterial species to intestinal microbiome variance was determined by multiple correlation analysis, with a significant correlation threshold at >0.25, of principal coordinates using PRIMER-E. Comparisons of alpha diversity metrics, Bray-Curtis distance from centroid, Bray-Curtis dissimilarity, and individual taxa were performed using GraphPad Prism software (v9.4.0). Normality of the datasets was determined using the Shapiro-Wilk test. Significance (p < 0.05) was determined using unpaired t-test (two-tailed) for parametric data and Mann-Whitney U test (two-tailed) for non-parametric data. Comparisons of categorical data were computed using Chi-squared test. P-values were adjusted for multiple testing using the Benjamini-Hochberg correction at a false discovery rate of 0.05. Species and functional differences between groups were assessed by linear discriminant analysis (LDA) effect size (LEfSe), where a = 0.05, LDA score = 2, and a “one versus all” test31. Species and pathways identified by LEfSe were validated by Mann-Whitney U test.
The effect of microbiome and host variables on future UTI risk was modelled by logistic regression using SAS Studio (v3.81). Host variables included prior UTI, prior antibiotic exposure, moderate-to-severe incontinence, diabetes, and dementia, and were related to future UTI in both univariate and multivariate models. Microbial variables included alpha diversity measures (Shannon’s diversity, species richness, Faith’s phylogenetic diversity, and Pielou’s evenness) and the relative abundances of gut taxa associated frailty or UTI: Faecalibacterium prausnitzii32, E. coli14,33, UPEC34, Enterobacteriaceae4, Pseudomonadota, and butyrate-producing bacterial species (Anaerostipes hadrus, Eubacterium rectale, Coprococcus catus, Faecalibacterium prausnitzii, Coprococcus eutactus, Roseburia intestinalis, Eubacterium hallii, and Roseburia inulinivorans)18. Multivariable logistic regression was used to relate these microbial variables to future UTI events, adjusting for prior UTI, prior antibiotic exposure, age, sex, moderate-to-severe incontinence, diabetes, and dementia. Odds ratios (OR) and 95% confidence intervals for the coefficients of the regression models were calculated and tested for statistical significance (p < 0.05).
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Results
Aged care cohort characteristics
One hundred and twenty-three aged care residents participated in the study, with a median age of 87.6 years (IQR 81–93 years) and 81.3% of participants being female (Table 1). Of the participants, 56.9% had a diagnosis of dementia, and 91.1% had moderate or severe incontinence. The cohort was divided into two groups: a case group of 54 individuals who experienced at least one UTI during the 24-month study period, and a comparator group of 69 age- and sex-matched individuals who did not experience UTI (Supplementary Table 1). The groups did not differ significantly in any of the assessed unmatched characteristics, except for exposure to antibiotics exclusively prescribed for UTI. Cohort characteristics were comparable to data from 142,923 permanent residents of residential aged care facilities in the Registry of Senior Australians (ROSA) (Supplementary Table 1). However, the study cohort had a higher proportion of females (81.3%, compared to 68.4% nationally) and those with severe incontinence (85.4%, compared to 77.5%).
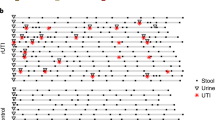
The case group experienced a total of 110 UTIs during the 24-month study period, with a median of one UTI (IQR 1–2.3) per person. Out of the 54 individuals in this group, 41 had at least one UTI in the 12 months preceding sample collection (61 UTIs in total), and 28 had at least one UTI in the 12 months following sample collection (49 UTIs in total) (Fig. 1a). Fifteen individuals experienced at least one UTI during both periods. Four individuals in the case group were hospitalised with urosepsis, with one case occurring prior to sample collection and three cases occurring after sample collection.

a Horizontal lines represent timelines for each participant (n = 54) that developed UTI over the 24-month study period. The black dotted line denotes stool sample collection (day 0). Filled circles indicate a UTI event. UTI events circled in blue represent hospitalisation with urosepsis. b The frequency of genera detected in the stool microbiome compared to their relative abundances, with core taxa identified (detected in 60% or more of individuals, with a median relative abundance of at least 0.1%). Genera are coloured according to phyla: Actinomycetota (blue), Bacteroidota (orange), Bacillota (green) and Pseudomonadota (red).
Aged care cohort stool microbiota characteristics
In total, 521 bacterial species were detected in the cohort. Of these, 29 were identified as core taxa (detected in 60% or more of individuals, with a median relative abundance of at least 0.1%), representing four bacterial phyla (Actinomycetota, Bacteroidota, Bacillota and Pseudomonadota) (Fig. 1b). Sixty percent of core species (n = 19) were gram-positive, 93% (n = 27) were obligate anaerobes, and 52% (n = 15) were capable of butyrate biosynthesis.
Prior UTI as a determinant of faecal microbiome characteristics
Faecal microbiota composition in those who experienced a UTI in the 12 months prior to sample collection and those who did not was not significantly different (PERMANOVA, R2 = 0.71%, p = 0.75) (Fig. 2a). There was also no difference in the dispersion of samples between groups (PERMDISP, Pseudo-F = 0.41, p = 0.54). These findings remained unchanged when the UTI assessment period was limited to three or six months prior to sample collection (Supplementary Table 3). Assessed alpha diversity measures did not differ significantly between the two groups at any time point (all p > 0.05; see Supplementary Fig. 2).

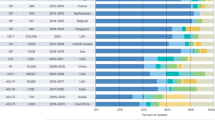
a Principal Coordinate Analysis of the gut microbiota of stool samples from residents with prior UTI (n = 41, pink) and no prior UTI (n = 69, teal). b Bacterial species that were significantly higher in prior UTI group and no prior UTI group. LDA scores were computed using linear discriminant analysis effect size (LEfSe). c Bar plot illustrating the significance and explained variance (R2) of antibiotic exposure on the gut microbiome, using PERMANOVA test on Bray-Curtis dissimilarity. Antibiotic exposures were grouped according to total antibiotics, those used exclusively for UTI treatment (trimethoprim, nitrofurantoin, methenamine hippurate), and those not used exclusively for UTI treatment. Three exposure periods were assessed (12 months, 6 months, and 3 months). *p < 0.05, **p < 0.01, ***p < 0.001.
Differential abundance analysis revealed nine species that were significantly different between those who had prior UTI and those who did not (Fig. 2b). Bifidobacterium dentium, Dorea longicatena, Amedibacillus dolichus, Lactobacillus rogosae, Olsenella profusa, Streptococcus parasanguinis, and Streptococcus salivarius were less abundant in residents with prior UTI, whereas Erysipelatoclostridium ramosum was more abundant (Fig. 2b). These species are all gram-positive and recognised members of the normal gut microbiota. All but two (S. parasanguinis, and S. salivarius) are obligate anaerobes.
Comparison of microbiome functional capacity identified no significant difference in overall pathway composition or in abundance of specific functional pathways between those who had experienced prior UTI and those who had not (Supplementary Table 4).
Gut microbiome characteristics influenced by antibiotic exposure, but not sex, age, or UTI-exclusive therapy
Antibiotic exposure in the prior 12 months was assessed according to three categories: 1) total antibiotics, 2) UTI-exclusive therapy (trimethoprim, nitrofurantoin and methenamine hippurate) and 3) other antibiotics (those not in UTI-exclusive therapy group). Total antibiotic exposure and exposure to other antibiotics both significantly explained gut microbiome composition (Fig. 2c, Supplementary Table 5). This remained true when assessment was limited to three or six months prior to sample collection (Fig. 2c, Supplementary Table 5). However, UTI-exclusive therapy was not associated with gut microbiome characteristics based on any duration of assessment period (Fig. 2c, Supplementary Table 5). Neither sex nor age was associated with gut microbiome composition, and none of the assessed variables were significantly associated with gut microbiota alpha diversity, functional capacity, or cumulative relative abundance of butyrogenic taxa (Supplementary Table 5).
Faecal microbiome characteristics were not associated with future UTI
Twenty-eight members of the aged care cohort (22.8%) experienced at least one UTI in the 12 months following sample collection. Of these, 15 (53.6%) had experienced a UTI prior to sample collection. The faecal microbiota composition of those who developed a UTI during the prospective assessment period did not differ significantly with those who did not (PERMANOVA, R2 = 0.67%, p = 0.68) (Fig. 3a), including where the assessment period was limited to three or six months post sample collection (Supplementary Table 3). None of the assessed alpha diversity metrics differed between comparator groups (all p > 0.05, Supplementary Fig. 3). No microbial factors were found to be independently associated with subsequent UTI risk through multivariable logistic regression (Fig. 3b).

a Principal Coordinate Analysis plot illustrating the gut microbiota of stool samples from residents who developed subsequent UTI (n = 28, pink) compared to those with no UTI (n = 95, teal). b Multivariable logistic regression for microbiome predictors of future UTI. c Box and whisker plot comparing cumulative relative abundances of butyrate-producing bacterial species (Mann-Whitney U test). The centre line denotes the median, the box limits denote the inter-quartile range (IQR) and whiskers extend to the limits. d Multivariable logistic regression for non-microbiome predictors of future UTI. Multivariable logistic regression models were adjusted for age, sex, dementia, moderate-severe incontinence, diabetes, any antibiotic exposure within the previous 12 months, and prior UTI incidence. Error bars indicate 95% CI. *p < 0.05.
Functional analysis identified 22 pathways associated with SCFA biosynthesis in the study cohort metagenome, including seven associated with butyrate biosynthesis. None of these pathways were differentially abundant in individuals who developed UTI following sample collection compared with those who did not (Supplementary Table 6). No association was identified between cumulative butyrogenic pathway abundance and any aspect of antibiotic exposure (Supplementary Table 5), and no intergroup differences in the cumulative relative abundance of butyrogenic taxa were identified (Fig. 3c).
While UPEC was detected in 42 members of the study cohort (34.1%), carriage rate did not differ significantly between comparator groups (39.3% vs 32.6%). Where detected, the absolute UPEC abundance also did not differ between groups (Supplementary Fig. 4a), nor did the carriage frequency, relative abundance, and absolute abundance of E. coli (Supplementary Fig. 4b, c).
Prior UTI is associated with future UTI
Of the assessed UTI risk factors (prior UTI, dementia, moderate-severe incontinence, diabetes, and any antibiotic exposure) only prior UTI (up to 12 months prior to sample collection) was associated with the development of subsequent UTI (OR 3.52, 95% CI 1.19–10.34, p = 0.023) (Fig. 3d). This relationship remained significant when limited to UTI incidence in the six months preceding sample collection (OR 2.94, 95% CI 1.01–8.58, p = 0.048). Limiting UTI incidence to at least 2 cases in the 12 months prior to sample collection, however, found no significant relationship with the likelihood of subsequent UTI (OR 2.54, 95% CI 0.54–11.89, p = 0.24).
Given that 23 participants (18.7%) died in the 12 months following sample collection, sensitivity analysis was performed on those who completed the study period (n = 100). This analysis identified the same relationship between the microbiome and future UTI risk (Supplementary Fig. 5a–f) and exposures/co-morbidities and future UTI risk (Supplementary Fig. 5g) as reported for the wider cohort.
Aged care residents exhibit greater microbiome variance than younger healthy adults
Associations between features of the gut microbiota and UTI risk have been reported in younger populations. Comparison of the microbiome characteristics of the aged care resident study cohort to those of a non-elderly cohort (mean age 39.3 ± 12.6) identified significant differences in variance (PERMANOVA, R2 = 5.4%, p < 0.0001) and dispersion (PERMDISP, Pseudo-F = 63.3, p < 0.0001) (Fig. 4a). Bray-Curtis distance from centroid was significantly higher in the aged care cohort compared to the younger comparator group (Fig. 4b). Eight species were identified within aged care residents as contributing significantly to the observed variation in microbial community composition, including Collinsella aerofaciens, Bifidobacterium adolescentis, Anaerostipes hadrus, Faecalibacterium prausnitzii, Methanobrevibacter smithii, Ruminococcus gnavus, Eubacterium rectale and Blautia wexlerae (Supplementary Data 2). Intergroup differences in microbiome composition (Supplementary Data 3) included significantly higher levels of Bacteroidota in older individuals, and Bacillota in the younger cohort. The gut microbiota of aged care residents was also significantly less diverse (p < 0.01, Fig. 4c), had lower levels of butyrate-producing taxa than the comparator group (p < 0.0001, Fig. 4d), and showed significant differences in microbial functional capacity (PERMANOVA, R2 = 89.5%, p < 0.0001; Supplementary Fig. 6).

a Principal Coordinate Analysis plot illustrating the intestinal microbiota of stool samples from aged care residents (n = 123, pink) and the non-elderly cohort (n = 20, grey). b Box and whisker plot comparing Bray-Curtis (BC) dissimilarity distance from centroid. c Box and whisker plot comparing species richness (Mann-Whitney U test). d Box and whisker plot comparing cumulative relative abundance of butyrate-producing species (Mann-Whitney U test). The box centre lines denote the median, the box limits denote the inter-quartile range (IQR), and whiskers extend to the limits. **p < 0.01, ****p < 0.0001
Discussion
There are several models that could explain relationships between disruption of intestinal microbiology and increased UTI risk. These include the gut microbiome influencing UTI risk by serving as a reservoir for uropathogens4, or by influencing systemic immune regulation18, or UTIs and associated therapies influencing intestinal microbiology, including through exposure to antibiotics. Alternatively, associations between UTIs and altered gut microbiota might simply reflect shared independent risk factors. Through the assessment of multiple cohorts, and inclusion of variables that may affect the association between the gut microbiome and UTIs, we were able to explore such relationships. We focused particularly on individuals living in long-term aged care, who are known to be at high risk of UTI and associated complications. Our findings suggest that antibiotics, rather than UTIs, are associated with gut microbiome changes. Moreover, neither the presence of uropathogens nor specific compositional characteristics are significantly linked to future UTI risk. The stool microbiome of aged care residents was found to be substantially more dispersed than that of non-elderly individuals, potentially explaining the absence of microbiome-UTI relationships that have been reported for younger adults previously.
Our finding that the detection of intestinal uropathogens was not associated with UTI is consistent with those of Worby et al., who investigated intestinal microbiology in women with a history of recurrent UTI18. However, other studies have linked the detection of intestinal uropathogens to UTIs35,36,37,38,39. Longitudinal genomic analysis of urine and stool isolates from women with UTIs by both Thanert and colleagues and by Chen and colleagues, for example, both suggested that the gut may be the source of uropathogens in most cases39. However, both studies also report marked individual variance in the pattern of gut colonisation, with the detection and abundance of uropathogens varying considerably preceding and between episodes of infection, suggesting that colonisation of the gut by uropathogens is not sufficient to explain UTI risk by itself.
The mechanisms by which the wider gut microbiome might contribute to UTI risk remain poorly understood. Worby et al. reported that reductions in lower bacterial diversity and butyrogenic commensal taxa were associated with UTI risk18. However, as noted by the authors, antibiotic exposure was higher in their recurrent UTI cohort compared to the control group, potentially contributing to observed differences in microbiome characteristics. In other contexts, such as in haematological stem cell transplant recipients, pathobiont overgrowth in the gut has been linked to the subsequent development of bacteraemia37. Similarly, Magruder et al. reported a higher relative abundance of uropathogens, including E. coli and Enterococcus sp, in the gut microbiota of kidney transplant patients with bacteriuria compared to controls14. However, the role of pathobiont overgrowth in bacterial translocation is less clear in immunocompetent populations who have not undergone chemotherapy or interventions that compromise the gut epithelial barrier.
In our study of long-term aged care residents, we identified a significant association between prior antibiotic use and gut microbiome perturbation. However, when we limited analysis to therapies used exclusively for UTI (including trimethoprim, nitrofurantoin, and methenamine hippurate), no association with microbiome disruption was observed. While this finding is not entirely surprising, given that these UTI treatments have minimal impact on anaerobic gut commensals compared to other antibiotics40,41, it underscores the importance of judicious antibiotic selection in avoiding microbiome disruption42. Moreover, it suggests that prior antimicrobial therapy, and not prior UTI in itself, drives the microbiome perturbation in this population.
We also observed a significant difference in the stool microbiome between elderly aged care residents and a younger adult cohort, characterised by higher within-participant dispersion and lower diversity in the former. These findings are consistent with well-described changes in the gut microbiome in later life43,44. Elderly individuals tend to exhibit more variable microbiota composition, with reduced stability in response to lifestyle perturbations43,45. The relative abundance of keystone commensal taxa and species that are important mediators of host physiology, such as Faecalibacterium prausnitzii, also tend to decline in later life32, resulting in a decrease in microbial capacity for synthesis of important physiological regulators like butyrate32,46. These ageing-associated alterations in gut microbiome characteristics likely reflect changes in both physiology and external exposures, including antibiotics and wider polypharmacy47. The contribution of these factors to the gut microbiome may therefore explain why this aged care population do not show the same association between the gut microbiome and UTIs as reported previously in a younger population18.
Alternatively, the disrupted microbiome evident in aged care residents might represent a common risk factor for UTI acquisition across this cohort, via the mechanisms hypothesised by Worby et al.18. For example, compared to healthy controls, the gut microbiome of aged care residents featured a low diversity and low capacity for butyrate production, characteristics that align with those described by Worby et al. in those with recurrent UTI18. It cannot be discounted that the gut microbiome of aged care residents predisposes to UTI risk, with other, non-microbiome variables influencing whether UTI develops. Our analysis of predictors of UTI identified prior UTI as the only variable associated with future UTI, given that the cohort arms were age- and sex-matched.
Our study had limitations that should be considered. First, defining UTIs in the elderly is challenging. As older individuals may have difficulty communicating symptoms, infection is less clearly associated with clinical markers, such as fever, and the principal indicator of potential UTI may include confusion or behavioural disturbance. Therefore, the extent to which all assigned UTIs represent symptomatic infections is uncertain. We therefore defined UTI based on antibiotic use and pathology results, rather than clinical symptoms. Second, we observed considerable inter-individual variation in the gut microbiome of this elderly population, which may reflect the high variability in diet, polypharmacy, and comorbidities in this population. This heterogeneity reduces our ability to identify potential specific UTI-microbiome relationships. Notably, our cohort characteristics align with those of 142,923 permanent residents of residential aged care facilities in the Registry of Senior Australians (ROSA), with the exceptions of the proportion of females and prevalence of severe incontinence. Given that severe incontinence is more prevalent in older women48, its higher prevalence in our aged care cohort was anticipated due to the greater proportion of females. Third, we aimed to investigate the relationship between the gut microbiome and any prior or future UTI; we did not assess the relationship with severity or frequency of UTIs. As only four cohort participants had a UTI that was complicated by bacteraemia, while only ten had ≥3 UTIs in 12 months (the definition of recurrent UTI49), we had limited power to explore these relationships. Additional studies with larger sample sizes or a more targeted elderly population are required to specifically determine whether stool microbiome features are indicative of UTI risk, severity, or frequency. However, undertaking such studies presents considerable challenges, given the need to recruit participants from a population where over half of individuals have dementia, long-term assessment is necessary, and both stool samples and prescribing data must be accessed.
Given the high burden of UTI in elderly populations, better understanding the potential influence of the gut microbiome on UTI risk for this population is critically important. Our study highlights that microbiome-UTI associations found in younger populations18 do not extend to elderly aged care cohorts, a finding that is potentially explained by the high degree of gut microbiome variance in elderly individuals. However, despite this inter-personal variation, we identified antibiotics, particularly those prescribed for non-UTI indications, as a major influence on gut microbiome characteristics in the elderly. Determining the clinical significance of this relationship to UTI and to wider health outcomes must now be a research priority.
Data availability
Metagenomic sequence data for the GRACE study are accessible from the European Nucleotide Archive under the accession number PRJEB51408, with sample accession numbers listed in Supplementary Data 1. Sequence data for the non-elderly comparator cohort are accessible from the Sequence Read Archive (SRA) under BioProject accession number PRJNA680665. Source data for all figures are available in Supplementary Data 2-5. The principal coordinates detailing the contribution of bacterial species to microbiome variance in aged care residents are provided in Supplementary Data 6. The list of 127 bacterial species that differed significantly between aged-care residents and non-elderly individuals can be found in Supplementary Data 7. All other data is available upon reasonable request from the corresponding author.
References
Yang, X. et al. Disease burden and long-term trends of urinary tract infections: a worldwide report. Front Public Health 10, 888205 (2022).
Britt, H. et al. General practice activity in Australia 2015–16. (Sydney University Press, 2016).
National Centre for Antimicrobial Stewardship and Australian Commission on Safety and Quality in Health Care. (ACSQHC, Sydney, 2021).
Flores-Mireles, A. L., Walker, J. N., Caparon, M. & Hultgren, S. J. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 13, 269–284 (2015).
Burrell, A. R., McLaws, M.-L., Fullick, M., Sullivan, R. B. & Sindhusake, D. SEPSIS KILLS: early intervention saves lives. Med J. Aust. 204, 73–73 (2016).
Choi, M. H., Kim, D., Park, Y. & Jeong, S. H. Impact of urinary tract infection-causative microorganisms on the progression to bloodstream infection: A propensity score-matched analysis. J. Infect. 85, 513–518 (2022).
Levy, M. M. et al. Outcomes of the Surviving Sepsis Campaign in intensive care units in the USA and Europe: a prospective cohort study. Lancet Infect. Dis. 12, 919–924 (2012).
Haas, L. E. M., van Dillen, L. S., de Lange, D. W., van Dijk, D. & Hamaker, M. E. Outcome of very old patients admitted to the ICU for sepsis: A systematic review. Eur. Geriatr. Med 8, 446–453 (2017).
Rowe, T. A. & Juthani-Mehta, M. Urinary tract infection in older adults. Aging health 9, https://doi.org/10.2217/ahe.13.38 (2013).
Hsiao, C. Y. et al. Risk factors for uroseptic shock in hospitalized patients aged over 80 years with urinary tract infection. Ann. Transl. Med. 8, 477 (2020).
Rowe, T. A. et al. Reliability of nonlocalizing signs and symptoms as indicators of the presence of infection in nursing-home residents. Infect. Control Hosp. Epidemiol. 43, 417–426 (2022).
Tocut, M., Zohar, I., Schwartz, O., Yossepowitch, O. & Maor, Y. Short- and long-term mortality in patients with urosepsis caused by Escherichia coli susceptible and resistant to 3rd generation cephalosporins. BMC Infect. Dis. 22, 571 (2022).
Foxman, B., Barlow, R., D’Arcy, H., Gillespie, B. & Sobel, J. D. Urinary tract infection: self-reported incidence and associated costs. Ann. Epidemiol. 10, 509–515 (2000).
Magruder, M. et al. Gut commensal microbiota and decreased risk for Enterobacteriaceae bacteriuria and urinary tract infection. Gut Microbes 12, 1805281 (2020).
Littman, D. R. & Pamer, E. G. Role of the commensal microbiota in normal and pathogenic host immune responses. Cell Host Microbe 10, 311–323 (2011).
Sorbara, M. T. et al. Inhibiting antibiotic-resistant Enterobacteriaceae by microbiota-mediated intracellular acidification. J. Exp. Med 216, 84–98 (2019).
Magruder, M. et al. Gut uropathogen abundance is a risk factor for development of bacteriuria and urinary tract infection. Nat. Commun. 10, 5521 (2019).
Worby, C. J. et al. Longitudinal multi-omics analyses link gut microbiome dysbiosis with recurrent urinary tract infections in women. Nat. Microbiol 7, 630–639 (2022).
Carpenter, L. et al. Cohort profile: GRACE – a residential aged care cohort examining factors influencing antimicrobial resistance carriage. BMC Geriatr. 23, 521 (2023).
Dreger, N. M., Degener, S., Ahmad-Nejad, P., Wöbker, G. & Roth, S. Urosepsis–etiology, diagnosis, and treatment. Dtsch Arztebl Int 112, 837–847 (2015). quiz 848.
Bolger, A. M., Lohse, M. & Usadel, B. Trimmomatic: a flexible trimmer for Illumina sequence data. Bioinformatics 30, 2114–2120 (2014).
Langmead, B. & Salzberg, S. L. Fast gapped-read alignment with Bowtie 2. Nat. Methods 9, 357–359 (2012).
Beghini, F. et al. Integrating taxonomic, functional, and strain-level profiling of diverse microbial communities with bioBakery 3. Elife 10, https://doi.org/10.7554/eLife.65088 (2021).
Caspi, R. et al. The MetaCyc database of metabolic pathways and enzymes. Nucleic Acids Res 46, D633–D639 (2017).
Oksanen, J. et al. vegan community ecology package version 2.6-2 April 2022. (2022).
Paradis, E. et al. ape: Analyses of Phylogenetics and Evolution version 5.7-1. (2023).
Huijsdens, X. W. et al. Quantification of bacteria adherent to gastrointestinal mucosa by real-time PCR. J. Clin. Microbiol 40, 4423–4427 (2002).
Enderle, J. L., Miller, A. L. & Pyles, R. B. Quantification of bacterial uropathogens in preclinical samples using real-time PCR assays. Curr. Microbiol 68, 220–226 (2014).
Burr, L. D. et al. Assessment of long-term macrolide exposure on the oropharyngeal microbiome and macrolide resistance in healthy adults and consequences for onward transmission of resistance. Antimicrob. Agents Chemother. 66, e0224621 (2022).
Clarke, K. & Gorley, R. Getting started with PRIMER v7. Primer-E Ltd., Plymouth 93 (2015).
Segata, N. et al. Metagenomic biomarker discovery and explanation. Genome Biol. 12, R60 (2011).
Jackson, M. A. et al. Signatures of early frailty in the gut microbiota. Genome Med. 8, 8 (2016).
Lim, L. & Bennett, N. Improving management of urinary tract infections in residential aged care facilities. AJGP 51, 551–557 (2022).
Shah, C., Baral, R., Bartaula, B. & Shrestha, L. B. Virulence factors of uropathogenic Escherichia coli (UPEC) and correlation with antimicrobial resistance. BMC Microbiol. 19, 204 (2019).
Bidet, P. et al. Comparative genomic analysis of ESBL-producing Escherichia coli from faecal carriage and febrile urinary tract infection in children: a prospective multicentre study. JAC Antimicrob. Resist. 4, dlac056 (2022).
Jantunen, M. E., Saxén, H., Lukinmaa, S., Ala-Houhala, M. & Siitonen, A. Genomic identity of pyelonephritogenic Escherichia coli isolated from blood, urine and faeces of children with urosepsis. J. Med. Microbiol. 50, 650–652 (2001).
Taur, Y. et al. Intestinal domination and the risk of bacteremia in patients undergoing allogeneic hematopoietic stem cell transplantation. Clin. Infect. Dis. 55, 905–914 (2012).
Chen, S. L. et al. Genomic diversity and fitness of E. coli strains recovered from the intestinal and urinary tracts of women with recurrent urinary tract infection. Sci. Transl. Med. 5, 184ra160–184ra160 (2013).
Thänert, R. et al. Comparative genomics of antibiotic-resistant uropathogens implicates three routes for recurrence of urinary tract infections. mBio 10, https://doi.org/10.1128/mBio.01977-19 (2019).
Brook, I., Wexler, H. M. & Goldstein, E. J. Antianaerobic antimicrobials: spectrum and susceptibility testing. Clin. Microbiol Rev. 26, 526–546 (2013).
Stewardson, A. J. et al. Collateral damage from oral ciprofloxacin versus nitrofurantoin in outpatients with urinary tract infections: a culture-free analysis of gut microbiota. Clin. Microbiol. Infect. 21, 344.e341–311 (2015).
Papanicolas, L. E., Warner, M., Wesselingh, S. L. & Rogers, G. B. Protect commensal gut bacteria to improve antimicrobial stewardship. Clin. Microbiol Infect. 26, 814–815 (2020).
Claesson, M. J. et al. Composition, variability, and temporal stability of the intestinal microbiota of the elderly. Proc. Natl Acad. Sci. USA 108, 4586–4591 (2011).
Wilmanski, T. et al. Gut microbiome pattern reflects healthy ageing and predicts survival in humans. Nat. Metab. 3, 274–286 (2021).
Biagi, E. et al. Through ageing, and beyond: gut microbiota and inflammatory status in seniors and centenarians. PLoS ONE 5, e10667 (2010).
Claesson, M. J. et al. Gut microbiota composition correlates with diet and health in the elderly. Nature 488, 178–184 (2012).
Nagata, N. et al. Population-level Metagenomics Uncovers Distinct Effects of Multiple Medications on the Human Gut Microbiome. Gastroenterology 163, 1038–1052 (2022).
Chang, H. J., Lynm, C. & Glass, R. M. Urinary Incontinence in Older Women. JAMA 303, 2208–2208 (2010).
Aydin, A., Ahmed, K., Zaman, I., Khan, M. S. & Dasgupta, P. Recurrent urinary tract infections in women. Int Urogynecol J. 26, 795–804 (2015).
Acknowledgements
This research was supported by an Australian Medical Research Future Fund (MRFF) grant from the Australian Department of Health (GNT1152268). G.B.R. discloses support for the research of this work from National Health and Medical Research Council (NHMRC) Senior Research Fellowship (GNT119378) and a Matthew Flinders Professorial Fellowship. M.I. discloses support for the research of this work from The Hospital Research Foundation Mid-Career Fellowship (MCF-27-2019) and NHMRC Investigator Grant (GNT119378). D.J.L. discloses support for the research of this work from an EMBL Australia Group Leader Award. S.L.T. discloses support for the research of this work from an NHMRC Emerging Leadership grant (GNT2008625).
Author information
Authors and Affiliations
Consortia
Contributions
Study design was undertaken by G.B.R. Data analysis was undertaken by S.J.M., L.C., S.L.T., & J.M.C. The manuscript was drafted by S.J.M., L.E.P., S.L.T., S.L.W., A.P.S. & G.B.R. All authors and the GRACE investigator group (E.F., D.G., D.J.L., C.W., L.E.X.L., M.C., & M.I.) provided intellectual input to the manuscript. The final manuscript was read and approved by all authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests. The Australian Department of Health reviewed the study proposal, but did not play a role in study design, data collection, analysis, interpretation, or manuscript writing.
Peer review
Peer review information
Communications Medicine thanks Cheng-Yen Kao and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Miller, S.J., Carpenter, L., Taylor, S.L. et al. Intestinal microbiology and urinary tract infection associated risk in long-term aged care residents. Commun Med 4, 164 (2024). https://doi.org/10.1038/s43856-024-00583-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s43856-024-00583-y
This article is cited by
-
Metatranscriptomics-based metabolic modeling of patient-specific urinary microbiome during infection
npj Biofilms and Microbiomes (2025)
