
Abstract
Background
Mental disorders are highly prevalent during pregnancy and are associated with unfavorable obstetrical outcomes, including maternal mortality. This study examined specific and combined associations of mental disorders with maternal morbidities.
Methods
A cross-sectional study of all delivery hospitalizations between the ages of 12–55 years was conducted using the National Inpatient Sample data from 2017. The International Classification of Diseases-10 codes were used to define exposures including depressive, anxiety, post-traumatic stress (PTSD), sleep, and bipolar disorders, and outcomes including premature rupture of membranes (PROM), hydramnios, placental disorder, cesarean delivery, fetal death, preterm birth, and postpartum hemorrhage (PPH). Survey-weighted logistic regression analysis was conducted to evaluate the associations between mental disorders and obstetric outcomes after adjusting for age, race/ethnicity, household income, primary payer, smoking, alcohol use, substance use, and obesity.
Results
The analysis of 715,810 delivery hospitalizations, representing 3,579,046 deliveries in the US demonstrates that sleep disorder is associated with PROM (OR = 1.41; 95% CI: 1.13, 1.75), placental disorder (OR = 1.56; 95% CI: 1.24, 1.95), cesarean delivery (OR = 1.50; 95% CI: 1.36, 1.65), and PPH (OR = 1.36; 95% CI: 1.10, 1.68) to a greater extent than other mental disorders. However, depressive disorder is greatly associated with hydramnios (OR = 1.16; 95% CI: 1.08, 1.25) and fetal death (OR = 1.38; 95% CI: 1.18, 1.61), while PTSD (OR = 1.40; 95% CI: 1.19, 1.64) is associated with preterm birth than other mental disorders.
Conclusions
Most mental disorders are independently associated with critical obstetric outcomes, with the extent of associations depending on specific obstetric outcomes. The study findings indicate the need for mandatory screening and management of mental health conditions in routine obstetrical care to improve maternal and child health outcomes.
Plain language summary
Preexisting mental disorders are associated with adverse maternal outcomes. However, the associations of common mental disorders and their co-occurrence with specific maternal outcomes, independent of pregnancy complications such as hypertension and diabetes, are unclear. We analyzed a large National Inpatient Sample database representing United States hospitalizations and showed that individual mental disorders and the presence of multiple mental disorders are strongly associated with multiple obstetric outcomes, independent of pregnancy complications such as hypertension and diabetes. This study indicates the need for screening and management of mental disorders during obstetrical care to improve maternal health and child outcomes.
Similar content being viewed by others

Introduction
Mental health during reproductive ages is crucial for positive maternal and child health outcomes. Mental disorders during pregnancy are noted to be the leading cause of maternal mortality and other adverse outcomes in the United States (US)1,2. Pregnant women demonstrate a high prevalence of mental disorders, particularly owing to unpleasant previous delivery experiences and birth outcomes, and unplanned pregnancies. In addition, preexisting mental disorders are likely to relapse during pregnancy owing to unanticipated obstetric outcomes such as cesarean deliveries and miscarriages3,4,5. Multiple studies have highlighted the elevated risk of new or relapse mental disorders during pregnancy6. Moreover, untreated mental illness during pregnancy may increase unhealthy behaviors with significant negative perinatal health consequences5. Although maternal morbidity and mortality have been recognized as a serious public health crisis in the US7, the role of preexisting mental disorders on perinatal outcomes has not been studied comprehensively8.
Depression is the leading mental disorder during pregnancy with an estimated incidence of 13.6–17%6. Moreover, the majority of perinatal depression starts before or during pregnancy9. Anxiety disorder (15.2%) during pregnancy also appears to be as common as depression5. Similarly, sleep disorders, especially obstructive sleep apnea (OSA) also estimated to be 5–19% during pregnancy globally10. Several studies provide the prevalence range of bipolar disorder and post-traumatic stress disorder (PTSD) during pregnancy as 5–18.8%11,12, and 3.4–6.1%13, respectively. Maternal mental disorders are likely to be associated with multiple unfavorable health outcomes due to cognitive and physiologic changes, and multisystem dysregulation2,14. Multiple studies highlighted the potential reasons for the associations between mental disorders during pregnancy and perinatal outcomes8,15,16,17,18,19,20. Specifically, these studies suggest that women with mental disorders are likely to have socioeconomic disparities, poor marital quality, lower antenatal checkup attendance, higher risky behavior, such as higher usage of tobacco and psychoactive substances, poor adherence to medical treatments, and genetic factors, leading to adverse perinatal outcomes. In addition, mental disorders affect matrix metalloproteinases, brain-derived neurotrophic factor, plasminogen activator inhibitor (PAI)−1, plasminogen activator (tPA) activity, free-protein S levels, and low intake of micronutrients, which are associated with adverse perinatal outcomes21. In fact, maternal mental health conditions may yield transgenerational effects on child and adolescent development22,23.
Studies evaluated the association of mental disorders with adverse maternal outcomes and reported a strong association with morbidity such as preeclampsia and gestational diabetes, as well as obstetric outcomes including cesarean section, preterm delivery, and postpartum hemorrhage (PPH)5,8. However, studies evaluating the association between mental disorders and adverse maternal outcomes are confined to limited obstetrical outcomes or composite mental disorders and obstetrical outcomes14,24,25,26. Moreover, these previous studies showed the link between mental disorders with obstetrical outcomes without adjusting for preeclampsia and gestational diabetes, and thus were unable to demonstrate if mental disorders associate with obstetrical outcomes independent of preeclampsia and gestational diabetes. In addition, the individual or joint evaluation of preexisting mental disorders on multiple obstetric outcomes independent of canonical comorbid conditions such as preeclampsia and gestational diabetes has not been studied, particularly in samples without a history of diabetes and hypertension.
We sought to evaluate the associations between preexisting mental disorders and maternal morbidities in the US. Specifically, we aimed (a) to evaluate the extent of association between individual mental disorders with maternal morbidities, and (b) to evaluate the relationship between a number of mental disorders with maternal morbidities. We hypothesized that different mental disorders are associated with maternal health outcomes differently, independent of canonical risk factors such as preeclampsia and gestational diabetes, and a certain number of mental conditions are markedly associated with specific maternal health outcomes.
Using the analysis of 715,810 delivery hospitalizations, representing 3,579,046 deliveries in the US, we show that most mental disorders, including depression, anxiety, sleep, PTSD, and bipolar disorders, are independently associated with critical obstetric outcomes. Moreover, we identify that the extent of the associations between mental disorders and obstetric outcomes depends on the type of obstetric outcomes. The presence of three or more mental disorders is markedly associated with adverse maternal health outcomes, indicating mandatory screening and management of all considered mental illnesses during obstetrical care.
Methods
Study population
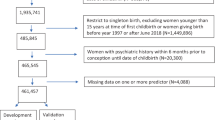
We conducted a retrospective cross-sectional study by extracting delivery hospitalizations from the National Inpatient Sample (NIS) database from the year 2017. The NIS is a publicly available all-payer inpatient healthcare database designed to produce US regional and national estimates of inpatient outcomes, resources, and costs. The NIS database is part of family databases developed through a Federal-State-Industry partnership by the Agency for Healthcare Research and Quality (AHRQ) for the Healthcare Cost and Utilization Project (HCUP). To access the specific NIS database, the database needs to be purchased from the website https://hcup-us.ahrq.gov/nisoverview.jsp. Our study did not require participant consent or Institutional Review Board (IRB) approval since NIS, 2017 includes the de-identified datasets from the International Classification of Diseases, 10th Revision (ICD-10) codes from participating hospitals27. An additional IRB approval was not needed for this study. The NIS extracts all clinical and nonclinical data elements for each hospital stay. Since NIS collects all administrative claim codes, those used for billing, all mental disorder diagnoses from previous health records are carried to the delivery hospitalization. Only those who were not assessed for a mental health diagnosis or assigned a different code that does not affect reimbursement are missed or misclassified in the NIS database. Our study included all delivery hospitalizations of women aged 12–55 years. The delivery codes included in our study capture more than 95% of deliveries28. We excluded hospitalizations with procedure codes of abortions, miscarriages, pregnancy with abortive outcomes, ectopic or abdominal pregnancy and related complications, spontaneous or unspecified abortions, termination with other complications, ovarian pregnancy without intrauterine pregnancy, cesarean delivery without indication, preexisting hypertension, and diabetes. However, we validated our findings by including preexisting hypertension and diabetes records in a sensitivity analysis.
Exposure-mental health conditions
We abstracted five common mental disorders, including depressive disorder, anxiety disorder, PTSD, sleep disorder, and bipolar disorder, using the ICD-10 codes (Supplementary Table 1). ICD codes for mental disorder diagnoses are based on claim codes made by physicians. Mental disorder diagnoses were mostly made prior to hospitalization for deliveries. The ICD codes used to ascertain these mental disorders appropriately estimate the burden of these conditions in the US. Although we considered all validated administrative codes that contain all diagnoses, the database may still underrepresent diagnoses owing to variation in coding practices that do not affect reimbursement.
Obstetric outcomes
The study outcomes were major adverse obstetric events during deliveries, including cesarean delivery, preterm birth, PPH, premature rupture of membranes (PROM), placental disorder, and fetal death/stillbirth. These outcomes were defined using the ICD-10 and are provided in the supplementary file (Supplementary Table 1). Like the diagnosis of mental disorders, the diagnoses of perinatal outcomes were also based on claim codes. The perinatal outcomes were given at the time of hospitalization for deliveries. Although we considered all validated administrative codes that contain all diagnoses, a lack of validation and underrepresentation of perinatal outcomes may occur in the NIS database.
Covariates
The covariates considered in this study were age (12–18, 19–35, 36–45 and 45–55 years), race/ethnicity (white, black, Hispanic, Asian/Pacific Islander, Native American, and other/missing), household income quartile (1st, 2nd, 3rd, 4th, and missing), primary payer (Medicare, Medicaid, private insurance, self-pay, no charge, and others/missing), smoking (no and yes), alcohol (no and yes), obesity (no and yes), and substance use (no and yes). Furthermore, preeclampsia (no and yes) and gestational diabetes (no and yes) were also adjusted in the models, along with all other covariates adjusted in the primary models, to validate the results for each primary outcome. In an additional sensitivity analysis, we included preexisting hypertension and diabetes records based on the ICD-10 codes.
Statistics and reproducibility
Appropriate sampling weight was applied in accordance with the Healthcare Cost and Utilization Project (HCUP)-NIS protocol. Data were summarized with appropriate descriptive statistics, including mean with standard deviation (SD) or frequencies with percentages. The association between each mental disorder with each obstetric outcome was evaluated using unadjusted and adjusted survey-weighted logistic regression analyses. Accordingly, the considered covariates, including age, race/ethnicity, household income, primary payer, smoking, alcohol use, substance use, and obesity, were adjusted in the primary analyses as per the study objective29. In the unadjusted analysis, only one exposure was included in the analysis for each outcome, whereas each exposure was adjusted with all considered covariates in the adjusted analysis for each outcome. The results of logistic regression were summarized with odds ratio (OR) and 95% confidence interval (CI). We also evaluated the association between adverse obstetric outcomes and the simultaneous presence of any psychiatric conditions (no disorder, one disorder, two disorders, and three or more disorders) using survey-weighted logistic regression analyses. To examine the combined evaluations of all mental disorders with each obstetric outcome, we developed adjusted models by including all mental disorders simultaneously in the logistic regression analyses. Prior to analyzing the joint evaluation of all mental disorders, Cramer’s V association coefficient was computed to determine the collinearity between mental disorders. The results of these logistic models were further validated by risk ratio (RR) estimation using survey-weighted Poisson regression analyses30. We further conducted multiple logistic regression models after additionally adjusting for gestational diabetes and preeclampsia to validate all the findings obtained from the primary adjusted models. Although we excluded all preexisting hypertension and diabetes from the primary analyses, we further validated the results of the primary analyses using survey-weighted logistic regression models by including all hypertension and diabetes cases and adjusting for all covariates, including hypertension, diabetes, and other covariates. Stata 17.0 version was used for the data management and statistical analyses. Owing to multiple outcomes, the primary findings were confirmed at 1% alpha after adjusting for multiple comparisons. All other findings were considered statistically significant at a p-value less than 0.05 of alpha. We followed statistical analysis and methods in biomedical research (SAMBR) checklists30 and constructed statistical analysis as per the guidance resources29.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Results
Baseline characteristics
We observed 715,810 unweighted delivery hospitalizations in the National Inpatient Sample (NIS) dataset, representing 3,579,046 deliveries in the US. The mean (SD) age was 28.7 (5.8) years, with a majority in the age group of 19–35 years (84.2%). The majority of the deliveries were for non-Hispanic whites (52.5%), followed by non-Hispanic blacks (17.3%) and Hispanics (17.9%). Most hospitalizations had household income in the first quartile (27.6%) and second quartile (25.4%). The primary payers were private (50.9%) or Medicaid (43.1%). Among comorbidities and risk factors, preeclampsia (10.9%), gestational diabetes (7.6%), substance use (5.9%), and smoking (5.3%) were most frequently observed (Table 1). The major mental diagnoses were anxiety disorder (3.7%), depressive disorder (3.1%), bipolar disorder (0.7%), PTSD (0.3%), and sleep disorder (0.2%). The most prevalent maternal illnesses during pregnancy were hydramnios (4.1%), followed by PROM (2.7%), and placental disorder (2.6%). 31.5% of these hospitalizations resulted in cesarean delivery. The most common obstetric outcomes were preterm birth (4.6%) and PPH (3.6%), while fetal death was observed in only 0.7% (Table 2). The prevalence of maternal morbidities was found to be 1–2% higher in records having mental disorders compared to those without mental disorders (Supplementary Table 2).
Unadjusted and adjusted associations of each of the mental conditions with obstetric outcomes in delivery hospitalizations
Most mental disorders were associated with adverse obstetric outcomes in unadjusted analyses (Supplementary Table 3). In the adjusted analysis after controlling for age, race/ethnicity, household income, primary payer, smoking, alcohol use, substance use, and obesity, all the mental disorders including PTSD (OR = 1.66; 95% CI: 1.35, 2.03), sleep disorder (OR = 1.61; 95% CI: 1.29, 2.00), anxiety disorder (OR = 1.49; 95% CI: 1.40, 1.59), depressive disorder (OR = 1.49; 95% CI: 1.39, 1.59), and bipolar disorder (OR = 1.38; 95% CI: 1.21, 1.58) were associated with PROM. Similarly, most mental disorders including PTSD (OR = 1.52; 95% CI: 1.26, 1.83), sleep disorder (OR = 1.48; 95% CI: 1.20, 1.83), anxiety disorder (OR = 1.34; 95% CI: 1.26, 1.43), depression disorder (OR = 1.32; 95%CI:1.24, 1.41), and bipolar disorder (OR = 1.20; 95% CI: 1.04, 1.38) were associated with PPH in adjusted analyses. PTSD (OR = 1.69; 95% CI: 1.44, 1.98), bipolar disorder (OR = 1.39; 95% CI: 1.25, 1.55), anxiety disorder (OR = 1.38; 95% CI: 1.30, 1.46), and depressive disorder (OR = 1.28; 95% CI: 1.20, 1.36) were also strongly associated with preterm birth. Cesarean delivery was strongly associated with sleep disorder (OR = 1.55; 95% CI: 1.40, 1.70), followed by anxiety disorder (OR = 1.18; 95% CI: 1.15, 1.22) and bipolar disorder (OR = 1.09; 95% CI: 1.02, 1.16). Placental disorder was also strongly associated with sleep disorder (OR = 1.68; 95% CI: 1.35, 2.11), followed by anxiety disorder (OR = 1.34; 95% CI: 1.24, 1.44), and depressive disorder (OR = 1.25; 95% CI: 1.16, 1.35) but not with bipolar disorder. Depressive and anxiety disorders were markedly associated with fetal death (OR = 1.46; 95% CI: 1.27, 1.68; OR = 1.29; 95% CI: 1.13, 1.48) as well as hydramnios (OR = 1.21; 95% CI: 1.14, 1.30; OR = 1.19; 95% CI: 1.12, 1.26), respectively (Fig. 1). The relative risk models yielded similar effect sizes for all these associations. Moreover, these associations remained significant even after correcting for multiple comparisons (Supplementary Table 4).

a Adjusted association of each mental disorder with each obstetric outcome after adjusting for age, race/ethnicity, household income, primary payer, smoking, alcohol use, substance use, and obesity. b Adjusted association of all mental disorders with each obstetric outcome after adjusting for other mental disorders, age, race/ethnicity, household income, primary payer, smoking, alcohol use, substance use, and obesity. OR odds ratio, CI confidence interval, PROM premature rupture of membranes, PPH postpartum hemorrhage, PTSD post-traumatic stress disorder.
Unadjusted and adjusted associations with the number of mental disorders with obstetric outcomes in delivery hospitalizations
Compared to no mental disorders, the presence of a mental disorder was consistently associated with all obstetric outcomes including PROM (OR = 1.42; 95% CI: 1.34, 1.51), PPH (OR = 1.34; 95% CI: 1.26, 1.41), fetal death (OR = 1.33; 95% CI: 1.17, 1.51), preterm birth (OR = 1.26; 95% CI: 1.19, 1.32), placental disorder (OR = 1.24; 95% CI: 1.16, 1.33) and hydramnios (OR = 1.17; 95% CI: 1.10, 1.23) after adjusting for age, race/ethnicity, household income, primary payer, smoking, alcohol use, substance use, and obesity. However, the presence of at least three mental disorders was markedly associated with PROM, fetal death, preterm birth, PPH, and placental disorder, with an effect size of 1.5 or higher (Table 3). Only depression and anxiety were likely to co-occur moderately (Supplementary Table 5). In simultaneous evaluation of all mental disorders, sleep disorder was associated with PROM (OR = 1.41; 95% CI: 1.13, 1.75), placental disorder (OR = 1.56; 95% CI: 1.24, 1.95), cesarean delivery (OR = 1.50; 95% CI: 1.36, 1.65), and PPH (OR = 1.36; 95% CI: 1.10, 1.68) to a greater extent than other psychiatric disorders. However, the depressive disorder was associated with hydramnios (OR = 1.16; 95% CI: 1.08, 1.25) and fetal death (OR = 1.38; 95% CI: 1.18, 1.61 while PTSD (OR = 1.40; 95% CI: 1.19, 1.64) was associated with preterm birth to a greater extent than other mental disorders (Fig. 1). Consistencies in findings for evaluating the relationship in different adjusted models, including each mental disorder with each obstetric outcome, and all mental disorders with each obstetric outcome, indicated no issue of collinearity (Fig. 1).
Adjusted association of each of the mental conditions with obstetric outcomes in delivery hospitalizations, adjusting for preeclampsia and gestational diabetes
After adjusting for age, race/ethnicity, household income, primary payer, smoking, alcohol use, substance use, obesity, preeclampsia, and gestational diabetes, PTSD and sleep disorder were strongly associated with PROM (OR = 1.68, 95%CI: 1.37, 2.06; OR = 1.63, 95% CI: 1.31, 2.03) and PPH (OR = 1.47, 95% CI: 1.21, 1.77; OR = 1.37, 95% CI: 1.11, 1.69), independent of preeclampsia and gestational diabetes. In addition, PTSD remained strongly associated with preterm birth (OR = 1.65; 95% CI: 1.41, 1.93) while sleep disorder was markedly associated with placental disorder (OR = 1.64; 95% CI: 1.31, 2.05) even after additionally adjusting for preeclampsia and gestational diabetes. In addition, anxiety and depression were mostly associated with all perinatal outcomes, independent of preeclampsia and gestational diabetes (Table 4). The association between the number of mental disorders and obstetric outcomes remained consistent in models with additionally adjusted covariates (Supplementary Table 6). The associations between all mental disorders and perinatal outcomes were unchanged with or without additionally adjusting for preeclampsia and gestational diabetes (Supplementary Table 7). After including all preexisting diabetes and hypertension (N = 740,828), the association between each mental disorder and each outcome remained unchanged even after additionally adjusting for all hypertension and all diabetes, along with other covariates (Supplementary Table 8).
Discussion
Among all psychiatric conditions, anxiety disorder was consistently associated with all obstetric outcomes. Similarly, depressive disorder was also found to be consistently associated with all maternal morbidities except for cesarean delivery. PTSD was associated with preterm birth to a greater extent than any other mental disorder. PROM and PPH were markedly associated with PTSD and sleep disorders. Cesarean delivery and placental disorder were greatly associated with sleep disorder, while fetal death and hydramnios were strongly associated with depressive disorder. These findings demonstrate that various mental disorders are associated with obstetric outcomes differently. We also found that delivery hospitalizations with three or more mental disorders had higher odds of observing adverse maternal health outcomes. Our study highlights that routine screening for mental illnesses and their proper management during pregnancy is highly needed for improving maternal health and birth outcomes.
Based on composite analysis, we can infer that having a sleep disorder is a critical factor associated with cesarean delivery and maternal illnesses during pregnancy. Similar to our findings, several studies identified an increased risk of PROM associated with poor sleep quality after adjusting for other canonical factors31. Further, a meta-analysis32 demonstrated that OSA during pregnancy is highly associated with an increased risk of preterm birth and cesarean delivery. Although there is no data for sleep disorder and placental disorder, a small-sized study33 validates our findings by demonstrating that OSA and its severity are associated with placenta weight and neonatal weight, which may be mediated by placental leptin levels. Our study identified PTSD as one of the strongest factors for preterm birth and PROM outcomes. Several studies confirmed our findings that PTSD during pregnancy elevates the risk of preterm birth34. A longitudinal study conducted by Yonkers et al.35 observed that increases in PTSD symptoms are associated with an increased risk of preterm birth. However, they identified that women with both PTSD and depression have the highest risk of preterm birth. Another small study confirmed the association between PTSD and PROM36. Like our study, depression and anxiety have been associated with adverse maternal and pregnancy outcomes, including fetal death or stillbirth37,38. The majority of prior studies demonstrated the relationship between mental disorders and adverse maternal and pregnancy outcomes, possibly by linking them to preeclampsia and comorbid depression14,32,36,39. However, we found the association between mental disorders and adverse maternal health outcomes independent of preeclampsia, gestational diabetes, obesity, smoking, and substance use, indicating a direct association between mental disorders and obstetric outcomes. Moreover, in our study, the simultaneous presence of any three mental disorders had 1.5–2-fold higher odds of obstetric outcomes compared to no disorders, indicating the importance of screening all these mental disorders during pregnancy and reproductive screening. In contrast, a few studies only delineated the adjusted association of the presence of at least one mental disorder on the risk of adverse maternal health outcomes14,25. These studies estimated a 1.07–1.5 times higher risk of adverse maternal outcomes associated with mental disorders.
The underlying mechanisms between mental disorders and maternal morbidities are not fully understood and may be bidirectional2. Mental disorders are known to affect the pregnancy environment through the endocrine, central nervous, and immune systems. Maternal stressors affect the hypothalamic-pituitary-adrenal (HPA) axis and inflammatory responses, which affect maternal health and fetal growth22. Psychiatric stressors alter neuroendocrine disturbance, which increases maternal HPA axis activity and placental secretion of corticotropin-releasing hormone mediated by cortisol. Catecholamines typically surge during the later trimester, followed by a decline in the postnatal period40,41,42,43,44. In addition, mental disorders may also affect lifestyle behaviors, including nutrition, sleep behavior, physical activity, and substance use. These behaviors then have a bidirectional effect on the central nervous and endocrine systems, leading to adverse obstetric outcomes14. In addition, an interplay between social determinants of health, prior mother’s own unpleasant experiences, and untreated mental disorders may further aggravate unfavorable maternal health outcomes2,45. Early childhood trauma and prenatal stress in both parents can induce epigenetic changes that can yield deleterious transgenerational effects22.
Although the prevalence of mental disorders is much higher than the canonical risk factors, such as preeclampsia and gestational diabetes, more than 75% of women do not get screening or treatment for mental disorders9,46. Even the majority of women diagnosed with mental disorders do not receive referrals or get treatment4. The American College of Obstetricians and Gynecologists and the American Psychiatric Association recommend regular screening for mental disorders during pregnancy14. Sadly, many physicians do not follow the recommended guidelines. Therefore, the current obstetric management mostly pertains to lifestyle management, focusing on preeclampsia and gestational diabetes. Approximately 23% of preventable maternal mortality is likely to occur due to maternal mental disorders47. The transgenerational effects and long-term adverse effects on offspring growth have been linked with maternal mental disorders22,23. Considering the prevalent condition of mental disorders during and before pregnancy and their long-term devastating effects on maternal and child health, it is essential to adopt strategies for improving maternal and child health care. The implementation strategies may include (a) mandatory mental health screening by maternal health care providers through recruitment of specialized reproductive psychiatrists (b) capacity building and training of obstetricians for screening maternal psychiatric conditions (c) adaptation of interdisciplinary collaborative care model (d) adaptation of outreach, education, navigation, access, referral, and follow up intervention programs for early screening and management of reproductive psychiatric health and wellbeing, and (e) reducing social determinants of health barriers for mental health and obstetrical care2,45,46.
The study has limitations that are inherent in administrative databases, such as coding errors and misclassification. The NIS datasets record inpatient hospitalizations and diagnoses at discharge but do not longitudinally follow to track post-discharge events, which may falsely lead to an underestimation of complications and adverse outcomes. It is also difficult to ascertain the exact time (prenatal or perinatal) when a mental disorder was diagnosed in a pregnant woman hospitalized for delivery, although most mental diagnoses are likely to be made prior to delivery hospitalization. The database also lacks pertinent details about antidepressants, antipsychotics, mood stabilizer medication, and illicit substances used by the patients, which independently may influence the severity of the comorbidity as well as outcomes. The cross-sectional design of the dataset also limits prove causation. Owing to the cross-sectional design, the time of mental disorder diagnosis was unclear, leading to uncertainty in evaluating the effect of mental disorders on perinatal outcomes. Although mental disorders during women’s reproductive years are underscreened, underdiagnosed, and untreated14 and are associated with adverse perinatal outcomes as confirmed in our study, our study cannot infer whether we should screen for mental disorders before they enter reproductive age or before they plan the pregnancy, or during initial pregnancy trimesters or throughout pregnancy due to a cross-sectional design. Lastly, there is marked heterogeneity in defining comorbidities and complications between centers, further amplified by variations in coding due to misinterpretation of hospital records and patient documentation or data entry errors. Residual confounding may still be present in this analysis even after adjusting for several covariates. For example, genetic risk factors for mental illnesses may further confound the relationship between mental disorders and maternal health outcomes. Studies have suggested that individuals with genetic risk factors are more susceptible to adverse maternal health outcomes48,49,50,51. The mental disorders are possibly underrepresented in our study, mostly owing to the underscreening of mental disorders, which is likely to occur in any retrospective research on mental health, as mental disorders are often underdiagnosed. Considering the large sample size and use of the validated codes that capture all mental diagnoses, our study robustly and reliably provides the critical associations between mental disorders and perinatal outcomes. Our study addresses an important topic in improving obstetrical care through the management of mental health conditions. Our study not only determined the association between individual mental disorders with a comprehensive set of obstetric outcomes but also evaluated whether a specific mental disorder is associated with an obstetric outcome independent of preeclampsia, gestational diabetes, and obesity in records without preexisting diabetes and hypertension.
Conclusion
We found that most mental disorders were independently associated with critical obstetric outcomes. However, the extent of the association depends on the type of obstetric outcomes. The presence of three or more mental disorders is markedly associated with adverse maternal health outcomes, indicating mandatory screening and management of all considered mental illnesses in obstetrical care, particularly during pregnancy, to prevent their adverse consequences on maternal health and child outcomes. Effective implementation strategies are essential through collaborative, multidisciplinary approaches and policy support models to improve maternal mental health screening and management in obstetrics care for improving overall maternal and child health outcomes. Moreover, current gaps in understanding the pathophysiology and long-term impacts warrant comprehensive longitudinal studies to elucidate and expand our knowledge to improve prevention and management strategies, finally reducing maternal morbidity and optimizing pregnancy outcomes.
Data availability
The database used in this study can be purchased from the HCUP-Agency for Healthcare Research and Quality (AHRQ) website (https://hcup-us.ahrq.gov/nisoverview.jsp). The analytic dataset generated from NIS and related statistical codes may be obtained from the corresponding author upon reasonable request. The data used for generating Fig. 1 is provided in Supplementary Data 1.
References
Organization W. H. O. Mental Health Aspects of Women’s Reproductive Health: A Global Review of the Literature (WHO, 2009).
Wisner, K. L., Murphy, C. & Thomas, M. M. Prioritizing maternal mental health in addressing morbidity and mortality. JAMA Psychiatry 81, 521–526 (2024).
Lin, S. C., Tyus, N., Maloney, M., Ohri, B. & Sripipatana, A. Mental health status among women of reproductive age from underserved communities in the United States and the associations between depression and physical health. A cross-sectional study. PLoS ONE 15, e0231243 (2020).
Johnson, P. J., Jou, J. & Upchurch, D. M. Health care disparities among U.S. women of reproductive age by level of psychological distress. J. Womens Health 28, 1286–1294 (2019).
Abdelhafez, M. A. et al. Psychiatric illness and pregnancy: a literature review. Heliyon 9, e20958 (2023).
Carter, D. & Kostaras, X. Psychiatric disorders in pregnancy. B. C. Med. J. 47, 96 (2005).
Gingrey, J. P. Maternal mortality: a US public health crisis. Am. J. Public Health 110, 462–464 (2020).
Runkle, J. D., Risley, K., Roy, M. & Sugg, M. M. Association between perinatal mental health and pregnancy and neonatal complications: a retrospective birth cohort study. Womens Health Issues 33, 289–299 (2023).
Wisner, K. L. et al. Onset timing, thoughts of self-harm, and diagnoses in postpartum women with screen-positive depression findings. JAMA Psychiatry 70, 490–498 (2013).
Kember, A. J., Elangainesan, P., Ferraro, Z. M., Jones, C. & Hobson, S. R. Common sleep disorders in pregnancy: a review. Front. Med.10, 1235252 (2023).
Rusner, M., Berg, M. & Begley, C. Bipolar disorder in pregnancy and childbirth: a systematic review of outcomes. BMC Pregnancy Childbirth 16, 331 (2016).
Masters, G. A. et al. Positive screening rates for bipolar disorder in pregnant and postpartum women and associated risk factors. Gen. Hosp. Psychiatry 61, 53–59 (2019).
Yildiz, P. D., Ayers, S. & Phillips, L. The prevalence of posttraumatic stress disorder in pregnancy and after birth: A systematic review and meta-analysis. J. Affect. Disord. 208, 634–645 (2017).
Logue, T. C. et al. Trends in and complications associated with mental health condition diagnoses during delivery hospitalizations. Am. J. Obstet. Gynecol. 226, 405.e401–405.e416 (2022).
Sudziute, K. et al. Pre-existingmental health disorders affect pregnancy and neonatal outcomes: a retrospectivecohort study. BMC Pregnancy Childbirth 20, 419 (2020).
Misgana, T. et al. Association between antenatal common mental disorders symptoms, and adverse obstetric and perinatal outcomes: a community-based prospective cohort study in Eastern Ethiopia. J. Affect. Disord. 355, 31–39 (2024).
Mongan, D. et al. Prevalence of self-reported mental disorders in pregnancy and associations with adverse neonatal outcomes: a population-based cross-sectional study. BMC Pregnancy Childbirth 19, 412 (2019).
Rejno, G. et al. Maternal anxiety, depression and asthma and adverse pregnancy outcomes - a population based study. Sci. Rep. 9, 13101 (2019).
Boden, R. et al. Risks of adverse pregnancy and birth outcomes in women treated or not treated with mood stabilisers for bipolar disorder: population based cohort study. BMJ 345, e7085 (2012).
Alipour, Z., Kheirabadi, G. R., Kazemi, A. & Fooladi, M. The most important risk factors affecting mental health during pregnancy: a systematic review. East. Mediterr. Health J. 24, 549–559 (2018).
Schofield, Z., Enye, S. & Kapoor, D. Pre-existing mental health disorders and pregnancy. Obstet. Gynaecol. Reprod. Med. 32, 83-87 (2022).
Coussons-Read, M. E. Effects of prenatal stress on pregnancy and human development: mechanisms and pathways. Obstet. Med. 6, 52–57 (2013).
Rogers, A. et al. Association between maternal perinatal depression and anxiety and child and adolescent development: a meta-analysis. JAMA Pediatr. 174, 1082–1092 (2020).
McKee, K. et al. Perinatal mood and anxiety disorders, serious mental illness, and delivery-related health outcomes, United States, 2006-2015. BMC Womens Health 20, 150 (2020).
Heun-Johnson, H. et al. Association between maternal serious mental illness and adverse birth outcomes. J. Perinatol. 39, 737–745 (2019).
Blackman, A. et al. Severe maternal morbidity and mental health hospitalizations or emergency department visits. JAMA Netw. Open 7, e247983 (2024).
Dwivedi, A. K., Vishwakarma, D., Dubey, P. & Reddy, S. Association of polycystic ovary syndrome with cardiovascular disease among female hospitalizations in the United States. Eur. J. Endocrinol. 188, 555–563 (2023).
Clapp, M. A., James, K. E. & Friedman, A. M. Identification of delivery encounters using international classification of diseases, tenth revision, diagnosis and procedure codes. Obstet. Gynecol. 136, 765–767 (2020).
Dwivedi, A. K. How to write statistical analysis section in medical research. J. Investig. Med. 70, 1759–1770 (2022).
Dwivedi, A. K. & Shukla, R. Evidence-based statistical analysis and methods in biomedical research (SAMBR) checklists according to design features. Cancer Rep. 3, e1211 (2020).
Du, M. et al. Maternal sleep quality during early pregnancy, risk factors and its impact on pregnancy outcomes: a prospective cohort study. Sleep Med. 79, 11–18 (2021).
Xu, T., Feng, Y., Peng, H., Guo, D. & Li, T. Obstructive sleep apnea and the risk of perinatal outcomes: a meta-analysis of cohort studies. Sci. Rep. 4, 6982 (2014).
Kidron, D., Bar-Lev, Y., Tsarfaty, I., Many, A. & Tauman, R. The effect of maternal obstructive sleep apnea on the placenta. Sleep 42, zsz072 (2019).
Urato, A. C. Posttraumatic stress disorder and risk of spontaneous preterm birth. Obstet. Gynecol. 125, 988–989 (2015).
Yonkers, K. A. et al. Pregnant women with posttraumatic stress disorder and risk of preterm birth. JAMA Psychiatry 71, 897–904 (2014).
Stramrood, C. A. et al. Posttraumatic stress disorder following preeclampsia and PPROM: a prospective study with 15 months follow-up. Reprod. Sci. 18, 645–653 (2011).
Dayan, J. et al. Role of anxiety and depression in the onset of spontaneous preterm labor. Am. J. Epidemiol. 155, 293–301 (2002).
Biaggi, A., Conroy, S., Pawlby, S. & Pariante, C. M. Identifying the women at risk of antenatal anxiety and depression: a systematic review. J. Affect. Disord. 191, 62–77 (2016).
Qiu, C., Williams, M. A., Calderon-Margalit, R., Cripe, S. M. & Sorensen, T. K. Preeclampsia risk in relation to maternal mood and anxiety disorders diagnosed before or during early pregnancy. Am. J. Hypertens. 22, 397–402 (2009).
Chrousos, G. P., Torpy, D. J. & Gold, P. W. Interactions between the hypothalamic-pituitary-adrenal axis and the female reproductive system: clinical implications. Ann. Intern. Med. 129, 229–240 (1998).
Smith, R. et al. Mood changes, obstetric experience and alterations in plasma cortisol, beta-endorphin and corticotrophin releasing hormone during pregnancy and the puerperium. J. Psychosom. Res. 34, 53–69 (1990).
Holzman, C. et al. Maternal catecholamine levels in midpregnancy and risk of preterm delivery. Am. J. Epidemiol. 170, 1014–1024 (2009).
Sandman, C. A., Wadhwa, P. D., Chicz-DeMet, A., Dunkel-Schetter, C. & Porto, M. Maternal stress, HPA activity, and fetal/infant outcome. Ann. N. Y. Acad. Sci. 814, 266–275 (1997).
Stetler, C. & Miller, G. E. Depression and hypothalamic-pituitary-adrenal activation: a quantitative summary of four decades of research. Psychosom. Med. 73, 114–126 (2011).
Chauhan, A. & Potdar, J. Maternal mental health during pregnancy: a critical review. Cureus 14, e30656 (2022).
Vesga-Lopez, O. et al. Psychiatric disorders in pregnant and postpartum women in the United States. Arch. Gen. Psychiatry 65, 805–815 (2008).
Centers for Disease Control and Prevention. Pregnancy-Related Deaths: Data from Maternal Mortality Review Committees in 36 US States, 2017–2019, CDC (accessed May 28, 2024).
Jami, E. S., Hammerschlag, A. R., Bartels, M. & Middeldorp, C. M. Parental characteristics and offspring mental health and related outcomes: a systematic review of genetically informative literature. Transl. Psychiatry 11, 197 (2021).
Suvisaari, J. M. et al. Obstetric complications as risk factors for schizophrenia spectrum psychoses in offspring of mothers with psychotic disorder. Schizophr. Bull. 39, 1056–1066 (2013).
Ratanatharathorn, A., Chibnik, L. B., Koenen, K. C., Weisskopf, M. G. & Roberts, A. L. Association of maternal polygenic risk scores for mental illness with perinatal risk factors for offspring mental illness. Sci. Adv. 8, eabn3740 (2022).
Judd, F. et al. Adverse obstetric and neonatal outcomes in women with severe mental illness: to what extent can they be prevented? Schizophr. Res. 157, 305–309 (2014).
Acknowledgements
We appreciate the efforts of all researchers who are involved and participate in maintaining the Healthcare Cost and Utilization Project (HCUP) -NIS datasets. We also thank all participating hospitals and their subjects in the NIS studies. We appreciate the department’s postdoctoral fellows for their constructive input on preliminary data analysis.
Author information
Authors and Affiliations
Contributions
A.K.D. has full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. P.D., S.Y.R. and A.K.D. conceived the study and design. P.D., K.S., and A.K.D. were involved in data acquisition, analysis, or interpretation of data, and drafting of the manuscript. P.D., S.L.M., P.M.T. and A.K.D. provided administrative, technical, and material support. A.K.D conducted all the statistical analyses. S.Y.R., S.L.M., P.M.T., and A.K.D. provided supervision throughout the study. All authors were involved in the critical revision of the manuscript for important intellectual content.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Communications Medicine thanks Marius Lahti-Pulkkinen and the other anonymous reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Dubey, P., Dwivedi, A.K., Sharma, K. et al. Associations of mental disorders with maternal health outcomes. Commun Med 5, 350 (2025). https://doi.org/10.1038/s43856-025-01062-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s43856-025-01062-8
