
Abstract
Income inequality, a structural property of societies characterized by the unequal distribution of resources, is associated with adverse mental health outcomes during adolescence, which is a sensitive period of neurodevelopment. While previous research has explored the impact of individual-level socioeconomic factors on brain structure and function, the neurobiological mechanisms linking structural inequality to mental health disparities remain poorly understood. Here, using data from the Adolescent Brain Cognitive Development study, we investigated the associations between state-level income inequality, indexed by the Gini coefficient, and brain structure and functional connectivity in over 8,000 children aged 9–10 years (from 17 states in the USA). We analyzed whole-brain cortical thickness and surface area, and volume and region-specific measures of thickness and surface area, as well as functional connectivity within and between 12 brain networks, controlling for several individual-level and state-level confounders (for example, income, educational attainment, state-level incarceration rate and Medicaid expansion status). Mediation analyses were conducted to test whether brain metrics linked income inequality to mental health outcomes at 6-month and 18-month follow-ups. Higher income inequality was associated with reduced cortical thickness and surface area across widespread brain regions, as well as altered functional connectivity between multiple brain networks. Lower cortical volume and surface area, as well as connectivity between the default mode and dorsal attention networks, mediated the association between higher structural income inequality and greater mental health problems. Our findings reveal income inequality as a unique societal-level determinant of neurodevelopment and mental health, independent of individual socioeconomic status. Policies aimed at reducing inequality and strengthening social cohesion to mitigate its neurobiological and mental health impacts are needed.
Similar content being viewed by others

Main
Economic inequality, characterized by the unequal distribution of income and wealth in a society, is associated with mental health and wellbeing outcomes beyond the influence of household income1,2,3. This may be particularly relevant during adolescence—a dynamic period of neurodevelopment when the brain undergoes rapid maturation and many mental health disorders begin to emerge4,5. Research increasingly underscores the link between higher income inequality and a range of adverse mental health outcomes in young people, including elevated rates of depression, anxiety and behavioral disorders6,7,8,9. Inequality-related stressors may contribute to heightened mental health vulnerabilities by shaping neurodevelopmental pathways, particularly those involved in emotion regulation and social cognition. Although numerous studies have examined how individual-level income is associated with brain development10,11, few have considered the broader role of structural income inequality in brain development and mental health. Income inequality has risen worldwide in recent decades12. Investigating whether and how inequality becomes neurobiologically embedded and heightens the risk of psychopathology during adolescence could provide valuable insights. Absolute poverty—typically defined as the inability to meet basic needs and operationalized based on thresholds set by the government and/or economists—has known effects on neurobiology10. If structural inequality has similar measurable associations, addressing it may gain broader acceptance across political ideologies.
Income inequality, which refers to the disproportionate concentration of income within a small fraction of the population, can fundamentally alter the social environment and is a distinct construct from poverty. While income inequality can exacerbate poverty by concentrating resources among a small proportion of the population, it is a structural characteristic of a society that can influence mental health through unique pathways—such as increased social comparison, which is a fundamental process through which individuals evaluate themselves by comparing their attributes, abilities and achievements to those of others13, and reduced social cohesion—not captured by individual income or poverty alone1,3. Inequality fosters relative deprivation, social comparison and perceptions of limited social mobility1,3. This creates conditions that induce chronic stress, a well-established risk factor for psychopathology14. Although evidence from adolescent samples is limited, biological evidence is aligned with the idea that inequality contributes to increased stress. A study of over 19,000 individuals across four European countries found that C-reactive protein levels, a marker of inflammation, were lowest in more equal societies (for example, Switzerland) and highest in more unequal ones (for example, Portugal)15. Experimental findings are also consistent with this: Shapiro et al.16 showed that short-term exposure to inequality triggers physiological stress responses. Increased stress levels could explain the well-established links between inequality and mental health1,3,17.
Stress neurobiology research shows that chronic stress exposure is associated with neural pathways involved in emotion regulation and cognitive control18, which are relevant for mental health. Extensive research has linked low individual income to altered brain structure and function, such as reduced cortical thickness and surface area and changes in functional connectivity19,20, factors closely associated with mental health21. Importantly, the association of individual socioeconomic status (SES) with brain volume has been shown to vary across European countries, with associations being stronger in some countries than others22—potentially reflecting broader structural factors such as inequality—a hypothesis that remains untested. Apart from a study examining electrophysiological brain dynamics in adults23 and a few studies examining links of local income disparity with gray matter24,25, the role of structural income inequality in shaping brain structure and function and, crucially, behavior outcomes in youth, remains unexplored. This gap underscores the critical need to explore how income inequality may influence neurobiology and mental health, independent of individual income.
In this study, we leverage population-based data from the Adolescent Brain Cognitive Development (ABCD) study to assess associations between state-level income inequality, indexed by the Gini coefficient, and brain structure and functional connectivity in children aged 9–10 years. Specifically, we examine the associations of inequality with cortical thickness and surface area, analyzing both whole-brain and region-specific measures, as well as functional connectivity within and between 12 brain networks. Finally, we evaluated whether any implicated brain structure or connectivity metrics mediated the relationship between state-level inequality and mental health 6 and 18 months later, aiming to elucidate the pathways through which structural inequality contributes to mental health disparities. Overall, the present study aims to examine the neural mechanisms through which income inequality is associated with adolescent mental health. By examining neurobiological pathways, we aim to better understand how inequality contributes to mental health disparities and inform potential interventions.
Results
The sample consisted of 10,071 children (4,871 female; 56% non-Hispanic white; Table 1) from across 17 states in the USA (N = 8,412 for functional connectivity after excluding unusable scans). We used linear mixed-effects models to examine associations of income inequality (operationalized as the Gini coefficient) with average cortical thickness, total cortical volume, total surface area, regional cortical thickness (n = 34 variables) and surface area (n = 34 variables), and within- and between-network connectivity (n = 78 variables). Our analyses control for multiple key covariates, including participant age and sex assigned at birth, scanner model, in-scanner motion (for connectivity variables), household income-to-needs ratio, parental educational attainment, parent mental health and state-level variables including incarceration rate, Temporary Assistance for Needy Families (TANF) and Medicaid expansion status. We also accounted for the nested family structure. These covariates were included to isolate the unique contribution of structural inequality to brain and mental health outcomes. False discovery rate (FDR) corrections (PFDR < 0.05) were applied within cortical thickness, surface area and functional connectivity analyses.
Inequality and brain structure
Higher income inequality was significantly associated with lower overall cortical volume (β = −2.93, s.e.m 0.49, t = −6.04, P < 0.001), average cortical thickness (β = −1.33, s.e.m. 0.55, t = −2.41, P = 0.016) and total surface area (β = −2.99, s.e.m. 0.49, t = −6.06, P < 0.001; Fig. 1a–c). Further, higher income inequality was associated with widespread patterns of lower cortical thickness (Fig. 1d and Table 2) and surface area (Fig. 1e and Table 2) across frontal, temporal, parietal and occipital regions (n = 48 variables). For a few regions, inequality was associated with higher thickness and surface area, including for the bank of superior temporal sulcus (STS) and supramarginal thickness, and parahippocampal area. The complete model output for all associations is available in Supplementary Table 2.

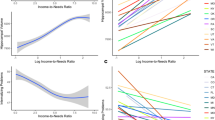
a–c, The association between Gini coefficient and average cortical thickness (a), total surface area (b) and total cortical volume (c). d,e, The t-statistic values from linear mixed-effects models for significant associations between Gini coefficient and regional cortical thickness variables (d) and surface area variables (e). Only areas with significant associations are depicted in the figure.
In sensitivity analyses, we adjusted for the average cortical thickness for thickness models and the total surface area in surface area models (Supplementary Table 4). Briefly, thickness results remained largely unchanged (22 out of 24 variables were still significant), whereas some surface area results were no longer significant (12 out of 22 variables remained significant). This suggests that inequality is associated with regional structure, over and above global effects.
Inequality and brain connectivity
Similarly, we found a significant relationship between inequality and several (n = 46) connections between and within functional networks. Higher inequality was associated with alterations in connectivity within and between networks involved in higher-order cognition and attention, such as the cingulo-opercular network (CON), dorsal attention network (DAN), default mode network (DMN), frontoparietal network (FPN) and ventral attention network (VAN). Inequality was also linked to connectivity in networks related to sensory and motor functions, including the auditory network (AN), sensorimotor network (SMN) and visual network (VN) (Fig. 2 and Table 3). The complete model output for all associations is available in Supplementary Table 3.

a, A heat map of the t-statistic values (from linear mixed models) of the relationship between Gini coefficient and significant connectivity variables after correction for multiple comparisons (n = 46). Only the bottom half of the matrix has been displayed for ease of readability. b, A chord diagram for significant connections. Red and blue chords represent positive and negative associations, respectively.
Additionally, to directly assess whether income inequality explained additional variance beyond individual-level SES, we compared models with and without the Gini coefficient for a few representative models (global brain measures and the first two significant connectivity variables). We found that including income inequality significantly improved the model fit for all brain outcomes tested and resulted in small but consistent increases in marginal R2 when the Gini coefficient was added to the models (Supplementary Table 5). This suggests that the Gini coefficient explains unique variance above individual-level SES and other covariates in the model. The main effects of parent income to needs and educational attainment are presented in Supplementary Tables 11 and 12.
Inequality, brain structure and connectivity and mental health
We then leveraged structural equation modeling, including the same covariates as the linear mixed-effects models, to test the role of the implicated brain variables as mediators of the association of inequality with total mental health problems at 6 months and 18 months later. The FDR was used to adjust for multiple comparisons within each set of analyses. Fit indices indicated acceptable to excellent fit for the structure models (root mean square error of approximation: mean 0.013, s.d. 0.004; comparative fit index: mean 0.997, s.d. 0.002; Tucker–Lewis index: mean 0.97, s.d. 0.023) and connectivity models (root mean square error of approximation: mean 0.016, s.d. 0.003; comparative fit index: mean 0.993, s.d. 0.004; Tucker–Lewis index: mean 0.93, s.d. 0.038). There was a significant total effect of inequality on mental health at the 18-month follow-up but not the 6-month follow-up (Supplementary Tables 6–10). We found a significant indirect effect for total surface area and cortical volume, and connectivity between the DAN and DMN for the association between inequality and total mental health problems at both 6 months and 18 months later. Specifically, higher inequality was associated with lower surface area and volume and higher (that is, less negative) DMN–DAN connectivity, which were in turn associated with higher mental health problems (Fig. 3 and results for 6 months provided in the Supplementary Information). These results were significant even when total mental health problems at baseline were accounted for in sensitivity analyses (see Supplementary Information for the model output).

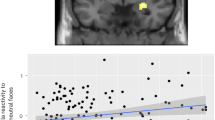
a–c, The neural mediators between income inequality and total mental health problems for total surface area (a), total cortical volume (b) and DMN to DAN connectivity (c).
Discussion
The present study provides new evidence on the neural mechanisms through which structural income inequality contributes to psychopathology. Our findings show that structural inequality is associated with measurable differences in brain structure and functional connectivity, which have implications for subsequent mental health outcomes during early adolescence. Higher income inequality was associated with reduced cortical thickness and surface area across widespread brain regions spanning all four lobes of the brain, which is in line with our whole-brain findings. The present study also revealed that structural income inequality was associated with alterations in functional connectivity within and between multiple cortical brain networks, including both higher-order cognitive and sensorimotor systems. These findings of widespread associations between inequality and brain structure and connectivity extend prior research on the impact of individual socioeconomic factors10,11,19,20,26,27,28,29,30,31,32 on brain development by highlighting the role of structural income inequality as a unique societal-level determinant that operates independently of individual-level SES. Importantly, total brain volume and surface area, as well as connectivity between the DMN and DAN, mediated links between inequality and mental health 6 months and 18 months later.
Given the evidence showing that inequality fundamentally alters the social environment—resulting in lower levels of social cohesion, trust and social capital, as well as higher levels of social comparison13—and the crucial role that social relationships play in our health and wellbeing33, it is unsurprising that inequality is associated with higher stress levels34. While not directly measured in our study, we speculate that these social changes and increased stress levels probably contribute to the profound impacts on the brain outcomes in children observed in our study. We discuss these ideas further below.
A key finding of this study is that youth living in states with higher income inequality have, on average, lower surface area and thickness across widespread regions in the brain, spanning the frontal, parietal, temporal and occipital lobes. The implicated regions support a range of functions including executive function, emotion regulation, reward processing, attention and sensory integration, socioemotional processing and visual processing35,36,37,38,39,40. Inequality was also associated with differences in functional connectivity within and between numerous functional systems involved in both sensorimotor and higher-order cognitive functions. Together, these findings indicate that income inequality may shape brain development in a diffuse and pervasive manner, potentially influencing a wide range of cognitive, emotional and behavioral outcomes in children and adolescents. Importantly, our findings are consistent with and extend prior work on individual SES showing similarly widespread associations of SES with brain structure and connectivity19,20,29 and associations between SES and a range of outcomes in children41,42,43,44. We speculate that such widespread patterns may be a consequence of inequality-related chronic stress. While both household income and inequality generate chronic stress, with potential biological consequences, they may do so via different psychosocial pathways. For instance, absolute poverty may trigger stress via material deprivation and income insecurity, while inequality may amplify status anxiety and social comparison as inequality heightens the salience of socioeconomic hierarchies, leading to increased upward social comparisons and feelings of inadequacy3,45,46. Social comparison—a psychological process through which individuals evaluate themselves relative to others13—is heightened in unequal societies where status hierarchies are more salient. This fosters upward comparison and contributes to status anxiety, a persistent worry about one’s social standing47. According to the status anxiety hypothesis, individuals in more unequal societies may experience greater stress about their social rank—even if they are not economically deprived. Supporting this, relative income (for example, income rank) is often a stronger predictor of psychological distress and life satisfaction than absolute income, particularly in high-inequality areas48,49,50,51. Experimental and observational studies have also linked higher inequality to increased materialism, status seeking and conspicuous consumption52. For children and adolescents, who are particularly sensitive to social comparison53, this may translate into a heightened preoccupation with peer status, social rejection and negative self-evaluation54, all of which lead to higher stress levels55. Growing up in the context of higher income inequality is also associated with greater victimization in adolescence56.
Further, inequality may also contribute to higher levels of adolescent stress indirectly. For example, ample evidence shows that inequality degrades mental health in adults1,3,17, and poor parent mental health is associated with greater family conflict and reduced parental support57, both of which may contribute to adolescent stress. Biological and experimental evidence is in line with the idea that inequality contributes to stress15,16. Experiencing chronic stress may disrupt the hypothalamic–pituitary–adrenal axis and elevate cortisol levels, norepinephrine and adrenaline58. While short-term stress responses may be protective, chronic stress places strain on the brain and other organ systems58. In the brain, chronic stress may disrupt synaptic homeostasis by impairing the balance between synapse formation and pruning, driven in part by prolonged glucocorticoid exposure59. This can lead to widespread synaptic loss and reduced synaptic density59, which may contribute to the widespread connectivity alterations in large-scale functional networks observed in the present study. Additionally, chronic stress can reduce dendritic arborization complexity, potentially driving reductions in cortical volume and thickness60,61. Further research is needed to test these pathways directly.
Income inequality not only exacerbates chronic stress but may also deprive adolescents of the protective effects of strong social ties, such as emotional support and shared resources, which may buffer these associations. For example, income inequality erodes social capital—defined as trust, networks and norms of reciprocity within communities—which is critical for fostering social cohesion and mental wellbeing62. Communities with high levels of inequality tend to experience greater segregation, reduced civic participation and weaker social networks, all of which can amplify feelings of isolation and mistrust63, contributing to the maintenance or exacerbation of chronic stress. This chronic stress may ultimately influence brain structure and function as described earlier.
Another central finding of our study is that whole-brain cortical surface area and cortical volume, and connectivity between the DMN and DAN, mediated the association between income inequality and mental health problems. These results are consistent with prior work showing that the DMN and DAN are involved in emotion regulation, and disruptions in their connectivity have been associated with various mental health disorders64,65,66. Furthermore, our findings build on prior research showing associations between reduced cortical volume and surface area and various forms of psychopathology (for example, depression, anxiety and externalizing disorders)67,68,69,70,71. Our results suggest that income inequality may contribute to these associations by shaping neurodevelopment, although further research is needed to disentangle the mechanisms underlying these links. Notably, only a small subset of brain variables associated with income inequality mediated these links, leaving the exact contribution of these neural alterations to behavioral outcomes uncertain. We speculate that it is possible such effects would be evident in outcomes not examined in the present study—such as emotion regulation and cognitive function—or over a longer developmental timespan, such as late adolescence or young adulthood.
Implications for policy and intervention
Our findings suggest that structural income inequality is associated with neurobiological differences, even after accounting for absolute income and poverty. These brain differences, in turn, help explain links to adverse mental health outcomes. As such, structural inequality should be considered a harmful social determinant with clear biological sequalae, meriting attention in efforts to improve population mental health, regardless of political ideology. In other words, addressing absolute poverty alone is likely to be inadequate and policies aimed at reducing inequality, improving social capital and cohesion, and mitigating the effects of social comparison are needed. We have discussed possible interventions in depth in a recent paper (see ref. 3 for a review). Briefly, economic reform including progressive taxation, increased social safety nets and universal healthcare are needed to alleviate the stressors that disproportionately affect children in more unequal societies3. Further, efforts to promote social capital, such as community-building initiatives and investments in public infrastructure, could mitigate the detrimental effects of inequality on mental health by fostering trust and social cohesion1,2,3. Interventions targeting status anxiety, such as programs promoting emotion regulation, social connectedness and feelings of self-worth, may help reduce the salience of social comparison among adolescents. In particular, schools could play a critical role by creating inclusive environments that minimize socioeconomic disparities and emphasize belonging and connectedness to promote mental health in young people72. Given our findings of links between structural inequality and brain structure and function, and evidence suggesting that inequality is associated with worse outcomes for everyone, even those not struggling financially2,17, such measures are urgently needed.
Limitations and future directions
Despite its strengths, this study has several limitations: (1) while the Gini coefficient we used provides a robust measure of income inequality, it did not capture other inequities, such as wealth disparities or access to healthy nutrition, that may also influence brain development. Although we relied on the Gini coefficient, other indices, such as the proportion of total income earned, Atkinson index, income ratios or the Robin Hood index may offer complementary insights73. For instance, the Theil index allows for the decomposition of inequality into between-group and within-group components74,75 (for example, between race versus within race), offering a more granular understanding of how different dimensions of inequality may relate to brain development. Future work could benefit from incorporating multiple measures of inequality to provide a more nuanced understanding of how different aspects of income distribution may differentially relate to brain outcomes. (2) Our findings are correlational. Experimental studies (for example, from behavioral economics) and longitudinal neuroimaging research, ideally grounded in causal inference frameworks, are needed to establish causal pathways. (3) While we speculate that the brain differences observed in our study may be due to the chronic stress associated with inequality, we did not measure perceived stress or biological markers of stress (for example, cortisol levels) directly. As such, any interpretations should be made with caution. Future work should test whether both self-reported and physiological indicators of stress mediate links between inequality and brain structure and function. Relatedly, stress and its neurodevelopmental consequences caused by structural factors such as inequality, and individual-level factors including poverty are not easily dissociable. (4) We chose to focus on state-level income inequality, which captures broader macrosocial factors and has been underexplored in developmental cognitive neuroscience. Future work should test the unique, distinct and joint effects of local inequality versus state inequality to better understand how different social contexts contribute to developmental outcomes76. (5) In our dataset, 21 sites span only 17 states, with 15 out of 17 states represented by a single site. This precluded us from including site as a random effect without compromising our ability to estimate state-level associations. While we controlled for scanner manufacturer and model, future research with broader geographic sampling and multiple sites per state could better disentangle site-specific variability from state-level predictors of brain structure and function. (6) The ABCD study does not include data from states with the highest poverty rates in the USA (for example, Mississippi, Louisiana and New Mexico). These findings therefore may not be generalizable to structurally disadvantaged states. However, our findings of inequality being associated with brain structure and function even in states with comparatively lower levels of poverty highlights the relevance of state-level contextual factors beyond absolute deprivation. (7) Averaging left and right hemisphere values may have masked potential hemispheric differences. This could be explored in future work with specific hypotheses. (8) This study examined whole-brain patterns and overall psychopathology and cannot comment on associations relevant for specific mental health domains. Future work should investigate more specific pathways to delineate risk and resilience mechanisms for distinct mental health domains. (9) We did not examine the role of residential segregation and homogeneity, which may influence children’s development through shared pathways with inequality such as low social capital, fragmentation, exclusion and lack of belonging76,77,78. Future work that examines the extent to which these exposures share common versus distinct pathways is needed. Further, it would also be valuable to examine whether racial homogeneity within a state or region influences the strength of the association between inequality and children’s outcomes in future work. Future research should examine the environmental and biological mechanisms linking inequality to brain structure and connectivity, such as neighborhood cohesion, prosocial behavior, parental stress, family conflict and stress pathways. Finally, while effect sizes are small, small effects can accumulate and have meaningful effects at the population level79.
Conclusions
This study advances our understanding of how income inequality shapes child brain structure and function and mental health. Our findings highlight how structural inequality becomes biologically embedded to influence mental health. Addressing inequality at the societal level is essential to fostering environments that support healthy neurodevelopment and mental wellbeing for all children.
Methods
Participants
This study utilized data from the ABCD study (release 5.1), an ongoing large-scale, multisite, longitudinal research study from the USA. Baseline data were collected from September 2017 to August 2018. The present study used neuroimaging data from the baseline time point and self-reported mental health from 6-month (when self-reported mental health was first assessed80) and 18-month (the last time point before the COVID-19 pandemic) follow-ups. The ABCD study aims to comprehensively track psychological and neurobiological development from late childhood to late adolescence. The study is conducted across 21 research sites (from 17 states). The participating sites cover about 20% of the 9–10-year-old population in the USA. Schools within a 50-mile radius of each site—across public, charter and private institutions—were selected using probability sampling within the 21 defined catchment areas (see ref. 81 for more information). Participants took part in clinical interviews, neuroimaging sessions, neurocognitive testing and completed various surveys. Written informed consent was obtained from parents or caregivers, and children provided assent. All participant rights were safeguarded by local institutional review boards. After excluding participants based on imaging quality and missing data on covariates, 10,071 children remained in the final analysis sample for brain structure and 8,412 for functional connectivity. Detailed demographic information for the sample has been provided below.
Measures
Inequality
We focused on structural inequality at the state level, which is intended to capture broader, system-level socioeconomic stratification—the policies, norms and institutional frameworks that shape income distribution at a population level. Inequality at the state level was assessed using the Gini coefficient, one of the most widely used measures of income inequality2,34,73, making it comparable with previous research. The Gini coefficient quantifies the extent to which income distribution among individuals or households within a population deviates from perfect equality. Values range from 0 (complete equality, where everyone has the same income) to 1 (complete inequality, where one person has all the income and everyone else has none). It is typically calculated from the Lorenz curve, which plots the cumulative proportion of income earned against the cumulative proportion of the population, ranked from poorest to richest. The coefficient represents the area between the Lorenz curve and the line of perfect equality, divided by the total area under the line of perfect equality. State-level Gini coefficient values were acquired for the year 2017 from the US Census Bureau. Importantly, larger geographic units, such as states or nations, offer more consistent and robust findings on the relationship between inequality and various outcomes than inequality at a smaller geographical scale such as the neighborhood34,82. For example, Wilkinson and Pickett82 found that the proportion of analyses reporting a supportive association between income inequality and health outcomes was 83% among international studies, 73% in studies using large subnational units (for example, states) and only 45% in studies using small areas such as neighborhoods. Similarly, Hsieh and Pugh83 concluded that consistent associations between income inequality and violent crime were found in studies using national or state-level data, but not in studies using smaller geographic units34. This pattern has been echoed in later multilevel meta-analyses34,84, supporting the idea that state-level measures more reliably capture meaningful variation in inequality. Further, inequality is a relatively stable construct and can be assumed to precede neurobiological changes temporally. More importantly, brain structure and function cannot influence state-level income inequality, making reverse causality a non-issue in this context. We report associations between the state-level Gini coefficient and state-level median income and racial homogeneity (percentage white) and income-to-needs ratio (averaged for individuals in the state) in Supplementary Table 1.
Mental health
We utilized youth-reported symptoms of psychopathology on the Brief Problem Monitor, which assesses symptoms over the past week using 19 items drawn from the Child Behavior Checklist, Teacher’s Report Form and Youth Self-Report85,86. Items are rated as 0 (‘not true’), 1 (‘somewhat true’) or 2 (‘very true’) and are categorized into three domains (attention, internalizing and externalizing). We utilized the total problems raw score, which included scores on internalizing, externalizing and attention symptoms. Internal consistency in our sample was high (Cronbach’s α = 0.85), indicating good reliability. The present study used data from two time points: the 6-month (the time point at which self-reported mental health was first assessed) and 18-month follow-up (which was the last timepoint of complete data before the pandemic). This was done to examine whether brain structure and connectivity mediated associations between inequality and mental health both in the short term and over a longer period, thereby testing the robustness and persistence of any observed effects.
Race and ethnicity
Race and ethnicity data were collected through two questions: (1) “What race do you consider the child to be?” (Asian, Black or African American, white) and (2) “Is the child of Hispanic/Latino/Latina descent?” (yes or no). Responses were categorized into five groups: Asian, Hispanic, non-Hispanic Black, non-Hispanic white and multiracial/multiethnic, and this classification is used in the study’s data releases. This variable was binarized into non-Hispanic white and non-white.
Covariates
Models were adjusted for a range of theoretically motivated covariates87. The mean educational attainment of parents/caregivers (in years) was calculated by averaging the education levels of both parents/caregivers. In cases where data for both were unavailable, the information for the available parent or caregiver was used. The income-to-needs ratio was determined by dividing the median value of the household’s income band (as defined by the ABCD study) by the federal poverty line for the respective household size. Parental mental health was the (responding) parent’s total raw score on the self-reported Adult Self Report instrument of broad psychopathology. Additionally, we accounted for the average TANF benefit at the state level88,89 as low assistance for needy families can exacerbate inequality as well as increase individual-level stress, which in turn can influence neurodevelopment. Further, we covaried for incarceration rate90 (that is, the number of individuals incarcerated in the state out of every 100,000 in population), as more unequal states may have higher levels of crime, which can influence brain development and mental health, as well as Medicaid expansion (binary variable) as an indicator of whether the state had expanded Medicaid eligibility91. In sensitivity analyses for our mediation models, we accounted for parent-reported youth mental health problems (total problems subscale) based on the Child Behavior Checklist92.
Imaging acquisition, preprocessing and connectivity data
The imaging procedures used here have been comprehensively outlined by Casey et al.93. Neuroimaging was performed following standardized protocols across multiple sites using 3T magnetic resonance imaging scanners from Siemens, Phillips or General Electric, equipped with 32-channel head coils. A high-resolution 3D T1-weighted image with 1 mm voxel size was obtained for all participants. Further, four or five 5 min resting-state scans (eyes open) were performed to ensure a minimum of 8 min of relatively low-motion data. For further details, refer to Hagler et al.94. The preprocessing was carried out by the ABCD data analysis and informatics core, utilizing a uniform pipeline (for detailed procedures and quality control, refer to Hagler et al.94). Motion correction was implemented in real-time at the Siemens and GE sites using dedicated software tools. Both automated and manual methods were employed to assess data quality, and all images were reviewed by trained professionals to detect artifacts or abnormalities. Artifact severity in the cortical reconstructions of the postprocessed images was rated on a scale from 0 to 3, with 3 indicating the highest level of artifact. Based on these ratings, technicians recommended the inclusion of only those images rated 0 for further analysis. Signal-to-noise ratios and head motion were assessed using automated tools.
FreeSurfer version 7.1.1 was used for cortical surface reconstruction and parcellation (Desikan–Killiany atlas). In this study, we focused on cortical thickness and surface area (34 variables each). Since no lateralized effects were hypothesized and prior work on individual-level environmental factors and brain structure has not yielded consistent results for lateralized effects10, values for the left and right hemispheres were averaged for the analysis. This is consistent with ours and others’ prior work on this sample19,95, and a study by Taylor et al.96 showed that SES is largely consistently associated with volume in the left and right hemisphere in the ABCD sample. Scans were excluded if they did not meet the quality control inclusion criteria outlined by the data analysis, informatics and resource center of ABCD (see release notes for details).
Functional magnetic resonance imaging time courses were projected onto FreeSurfer’s cortical surface. Using these time courses, within- and between-network connectivity (Pearson correlation) was calculated based on the Gordon parcellation scheme (36) for 12 predefined resting-state networks: AN, CON, cinguloparietal network, DAN, DMN, FPN, retrosplenial temporal network (RTN), SMN (hand (H)), SMN (mouth (M)), salience network (SN), VAN and VN. These connectivity measures were then Fisher z-transformed, resulting in 78 dependent variables, 66 between-network connectivity variables and 12 within-network connectivity variables (with within-network connectivity representing the average correlation across all pairs of regions within each network). Scans were excluded if they did not meet the quality control inclusion criteria outlined by the ABCD data analysis, informatics and resource center (see release notes for details).
Statistical analyses
To examine the effects of state-level income inequality on brain structure and functional connectivity, we conducted linear mixed-effects models (using the lme4 package in R). State-level income inequality, indexed by the Gini coefficient, was included as the main predictor, with brain structure (cortical thickness and surface area, 34 variables each) and functional connectivity (across 12 brain networks, 78 variables in total) as the dependent variables (with separate models for each outcome). We corrected for multiple comparisons using the FDR within each set of analyses for thickness, area and connectivity (PFDR < 0.05). P values were obtained using the lmerTest package. We ran three additional models for total cortical volume, total surface area and average cortical thickness. We included participant age at baseline, sex, scanner type and average framewise displacement (for connectivity measures), income-to-needs ratio at baseline, parent educational attainment at baseline and parent mental health problems at baseline as covariates to control for potential confounding factors. We additionally adjusted for TANF, incarceration rate and Medicaid expansion status (from 2016–2017) at the state level and included a random effect for family ID. All numerical variables were standardized for analyses. Semi-partial R2 values were obtained using the partR2 package in R. Given the small number of states (n = 17) and adjustments for key individual-level covariates (for example, age, sex, income-to-needs ratio, parent educational attainment and parent mental health) and site and state-level variables (for example, scanner manufacturer and model, state-level policies and cash assistance, and incarceration rates), clustering or random effects at the state or site level were deemed redundant as the included covariates adequately account for potential confounding and site-related variability. Since some covariates might arguably lie on the causal pathway from inequality to youth mental health (for example, parent mental health issues), the estimates obtained from our model are conservative. However, including this covariate adjusts for other environmental factors that may be associated with parent mental health issues—such as neglect, inconsistent caregiving and substance abuse—as well as genetic propensity to mental health problems. This approach allowed us to isolate effects associated with inequality to a greater extent. Further, to tease apart regional effects from global effects, we adjusted for average thickness (for regional thickness models) and total surface area (for regional surface area models). Model output for this additional analysis has been provided in Supplementary Table 4. Additionally, sensitivity analyses adjusting for racial homogeneity at the state-level (that is, percentage white) have been provided in Supplementary Tables 18–21.
On secondary analyses, race/ethnicity was modeled as a moderator of the association between inequality and brain structure and connectivity to account for intersectional influences. As above, we corrected for multiple comparisons using the FDR within each set of analyses for thickness, area and connectivity (PFDR < 0.05). These results have been reported and are discussed in the Supplementary Information.
For the significant variables identified in the linear mixed-effects models, we performed mediation analysis using structural equation modeling in the lavaan package in R. The analysis aimed to investigate whether brain structure or functional connectivity metrics mediated the relationship between state-level income inequality and total mental health symptoms assessed both 6 months and 18 months later. Scanner manufacturer/model, family ID (to account for family structure) and mean framewise displacement (for functional connectivity variables) were regressed out of the brain measures (that is, the mediator). All covariates (for example, sex, baseline income-to-needs ratio, baseline parental education and baseline parent psychopathology, 2016–2017 Medicaid, TANF and incarceration rate) were included as predictors in both the brain and outcome equations of the mediation models to ensure effects of interest were adjusted for these variables. Additionally, interview age at baseline was modeled in the ‘a’ path and interview age at the respective mental health assessment (either the 6-month or 18-month follow-up) was modeled as a covariate in the ‘b’ path. The structural models were not saturated and included only theoretically driven paths. To assess the significance of indirect effects, we employed a bootstrapping procedure with 5,000 resamples to obtain bias-corrected confidence intervals (CIs) and P values for the indirect pathways. As before, we corrected for multiple comparisons within each set of analyses (that is, thickness, surface area and connectivity; PFDR < 0.05). A moderated mediation model was conducted for variables where race/ethnicity moderates the association between inequality and brain variables (results reported in the Supplementary Information). In a sensitivity analysis, we tested whether results were robust to the inclusion of total mental health problems at baseline as a covariate.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The ABCD study data used in this project are publicly available (https://abcdstudy.org/). Access to the data is granted to qualified researchers via a data use agreement. For further information on how to obtain access to this dataset, visit the NIH Brain Development Cohorts data sharing platform (https://www.nbdc-datahub.org/).
Code availability
All data analyses used readily available programs (for example, open-source R code). No custom code was used.
References
Patel, V. et al. Income inequality and depression: a systematic review and meta-analysis of the association and a scoping review of mechanisms. World Psychiatry 17, 76–89 (2018).
Wilkinson, R. G. & Pickett, K. The Spirit Level: Why Equality Is Better for Everyone (Penguin, 2010).
Rakesh, D. et al. Economic inequality and mental health: causality, mechanisms, and interventions. Annu. Rev. Clin. Psychol. 21, 353–377 (2025).
Solmi, M. et al. Age at onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Mol. Psychiatry 27, 281–295 (2022).
Rakesh, D., Dehestani, N. & Whittle, S. in Encyclopedia of Adolescence 2nd edn (eds Troop-Gordon, W. & Neblett, E. W.) (Academic, 2024); https://www.sciencedirect.com/science/article/pii/B978032396023600124X
Dierckens, M. et al. National-level wealth inequality and socioeconomic inequality in adolescent mental well-being: a time series analysis of 17 countries. J. Adolesc. Health 66, S21–S28 (2020).
Pabayo, R., Dunn, E. C., Gilman, S. E., Kawachi, I. & Molnar, B. E. Income inequality within urban settings and depressive symptoms among adolescents. J. Epidemiol. Community Health 70, 997–1003 (2016).
Elgar, F. J., Gariépy, G., Torsheim, T. & Currie, C. Early-life income inequality and adolescent health and well-being. Soc. Sci. Med. 174, 197–208 (2017).
Farmer, G., MacDonald, S. W., Yamamoto, S. S., Wilkes, C. & Pabayo, R. Neighbourhood income inequality and general psychopathology at 3-years of age. J. Can. Acad. Child Adolesc. Psychiatry 31, 135 (2022).
Rakesh, D. & Whittle, S. Socioeconomic status and the developing brain—a systematic review of neuroimaging findings in youth. Neurosci. Biobehav. Rev. 130, 379–407 (2021).
Rakesh, D., Whittle, S., Sheridan, M. A. & McLaughlin, K. A. Childhood socioeconomic status and the pace of structural neurodevelopment: accelerated, delayed, or simply different? Trends Cogn. Sci. 27, 833–851 (2023).
Horowitz, J. M., Igielnik, R. & Kochhar, R. Trends in income and wealth inequality. Pew Research Center https://www.pewresearch.org/social-trends/2020/01/09/trends-in-income-and-wealth-inequality/ (2020).
Wilkinson, R. & Pickett, K. The enemy between us: the psychological and social costs of inequality. Eur. J. Soc. Psychol. 47, 11–24 (2017).
Lupien, S. J., Juster, R.-P., Raymond, C. & Marin, M.-F. The effects of chronic stress on the human brain: from neurotoxicity, to vulnerability, to opportunity. Front. Neuroendocrinol. 49, 91–105 (2018).
Layte, R. et al. A comparative analysis of the status anxiety hypothesis of socio-economic inequalities in health based on 18,349 individuals in four countries and five cohort studies. Sci. Rep. 9, 796 (2019).
Shapiro, M. S., Rylant, R., de Lima, A., Vidaurri, A. & van de Werfhorst, H. Playing a rigged game: inequality’s effect on physiological stress responses. Physiol. Behav. 180, 60–69 (2017).
Wilkinson, R. & Pickett, K. The Inner Level: How More Equal Societies Reduce Stress, Restore Sanity and Improve Everyone’s Well-Being (Penguin, 2018).
McEwen, B. S. Allostasis and allostatic load: Implications for neuropsychopharmacology. Neuropsychopharmacology 22, 108–124 (2000).
Rakesh, D., Zalesky, A. & Whittle, S. Assessment of parent income and education, neighborhood disadvantage, and child brain structure. JAMA Netw. Open 5, e2226208 (2022).
Rakesh, D., Zalesky, A. & Whittle, S. Similar but distinct—effects of different socioeconomic indicators on resting state functional connectivity: findings from the Adolescent Brain Cognitive Development (ABCD) study. Dev. Cogn. Neurosci. 51, 101005 (2021).
Whittle, S., Zhang, L. & Rakesh, D. Environmental and neurodevelopmental contributors to youth mental illness. Neuropsychopharmacology 50, 201–210 (2024).
Walhovd, K. B. et al. Education and income show heterogeneous relationships to lifespan brain and cognitive differences across European and US cohorts. Cereb. Cortex 32, 839–854 (2021).
Baez, S. et al. Structural inequality and temporal brain dynamics across diverse samples. Clin. Transl. Med. 14, e70032 (2024).
Vargas, T. G., Damme, K. S. F. & Mittal, V. A. Differentiating distinct and converging neural correlates of types of systemic environmental exposures. Hum. Brain Mapp. 43, 2232–2248 (2022).
Parker, N. et al. Income inequality, gene expression, and brain maturation during adolescence. Sci. Rep. 7, 7397 (2017).
Farah, M. J. Socioeconomic status and the brain: prospects for neuroscience-informed policy. Nat. Rev. Neurosci. 19, 428–438 (2018).
Farah, M. J. The neuroscience of socioeconomic status: correlates, causes, and consequences. Neuron 96, 56–71 (2017).
Rakesh, D., Seguin, C., Zalesky, A., Cropley, V. & Whittle, S. Associations between neighborhood disadvantage, resting-state functional connectivity, and behavior in the adolescent brain cognitive development study: the moderating role of positive family and school environments. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 6, 877–886 (2021).
Sripada, C. et al. Socioeconomic resources are associated with distributed alterations of the brain’s intrinsic functional architecture in youth. Dev. Cogn. Neurosci. 58, 101164 (2022).
Rakesh, D., Sadikova, E. & McLaughlin, K. A. Associations among socioeconomic disadvantage, longitudinal changes in within-network connectivity, and academic outcomes in the ABCD study. Dev. Cogn. Neurosci. 74, 101587 (2025).
Jednoróg, K. et al. The influence of socioeconomic status on children’s brain structure. PLoS ONE 7, e42486 (2012).
Noble, K. G. et al. Family income, parental education and brain structure in children and adolescents. Nat. Neurosci. 18, 773–778 (2015).
Cohen, S. Social relationships and health. Am. Psychol. 59, 676–684 (2004).
Pickett, K. E. & Wilkinson, R. G. Income inequality and health: a causal review. Soc. Sci. Med. 128, 316–326 (2015).
Alvarez, J. A. & Emory, E. Executive function and the frontal lobes: a meta-analytic review. Neuropsychol. Rev. 16, 17–42 (2006).
Stuss, D. T. Functions of the frontal lobes: relation to executive functions. J. Int. Neuropsychol. Soc. 17, 759–765 (2011).
Grill-Spector, K. & Malach, R. The human visual cortex. Annu. Rev. Neurosci. 27, 649–677 (2004).
Pozzi, E., Vijayakumar, N., Rakesh, D. & Whittle, S. Neural correlates of emotion regulation in adolescents and emerging adults: a meta-analytic study. Biol. Psychiatry 89, 194–204 (2021).
Posner, M. I. & Petersen, S. E. The attention system of the human brain. Annu. Rev. Neurosci. 13, 25–42 (1990).
Olson, I. R., Plotzker, A. & Ezzyat, Y. The enigmatic temporal pole: a review of findings on social and emotional processing. Brain 130, 1718–1731 (2007).
Rakesh, D., Lee, P. A., Gaikwad, A. & McLaughlin, K. A. Annual research review: associations of socioeconomic status with cognitive function, language ability, and academic achievement in youth: a systematic review of mechanisms and protective factors. J. Child Psychol. Psychiatry 66, 417–439 (2025).
Lawson, G. M., Hook, C. J. & Farah, M. J. A meta-analysis of the relationship between socioeconomic status and executive function performance among children. Dev. Sci. 21, e12529 (2018).
Bradley, R. H. & Corwyn, R. F. Socioeconomic status and child development. Annu. Rev. Psychol. 53, 371–399 (2002).
Reiss, F. Socioeconomic inequalities and mental health problems in children and adolescents: a systematic review. Soc. Sci. Med. 90, 24–31 (2013).
Cheung, F. & Lucas, R. E. Income inequality is associated with stronger social comparison effects: the effect of relative income on life satisfaction. J. Pers. Soc. Psychol. 110, 332–341 (2016).
Walasek, L. & Brown, G. D. A. Income inequality and status seeking: searching for positional goods in unequal US states. Psychol. Sci. 26, 527–533 (2015).
Delhey, J., Schneickert, C. & Steckermeier, L. C. Sociocultural inequalities and status anxiety: redirecting the Spirit Level Theory. Int. J. Comp. Sociol. 58, 215–240 (2017).
Wood, A. M., Boyce, C. J., Moore, S. C. & Brown, G. D. A. An evolutionary based social rank explanation of why low income predicts mental distress: a 17 year cohort study of 30,000 people. J. Affect. Disord. 136, 882–888 (2012).
Osafo Hounkpatin, H., Wood, A. M., Brown, G. D. A. & Dunn, G. Why does income relate to depressive symptoms? Testing the income rank hypothesis longitudinally. Soc. Indic. Res. 124, 637–655 (2015).
Boyce, C. J., Brown, G. D. A. & Moore, S. C. Money and happiness: rank of income, not income, affects life satisfaction. Psychol. Sci. 21, 471–475 (2010).
Boyce, W. T., Sokolowski, M. B. & Robinson, G. E. Toward a new biology of social adversity. Proc. Natl Acad. Sci. USA 109, 17143–17148 (2012).
Pybus, K., Power, M., Pickett, K. E. & Wilkinson, R. Income inequality, status consumption and status anxiety: an exploratory review of implications for sustainability and directions for future research. Soc. Sci. Humanit. Open 6, 100353 (2022).
Harter, S. The Construction of the Self, Second Edition: Developmental and Sociocultural Foundations (Guilford Publications, 2015).
Wang, J.-L., Wang, H.-Z., Gaskin, J. & Hawk, S. The mediating roles of upward social comparison and self-esteem and the moderating role of social comparison orientation in the association between social networking site usage and subjective well-being. Front. Psychol. 8, 233971 (2017).
He, D., Shen, X. & Liu, Q.-Q. The relationship between upward social comparison on SNSs and excessive smartphone use: a moderated mediation analysis. Child. Youth Serv. Rev. 116, 105232 (2020).
Elgar, F. J. et al. Association of early-life exposure to income inequality with bullying in adolescence in 40 countries. JAMA Pediatrics 173, e191181 (2019).
Van Loon, L. M. A., Van de Ven, M. O. M., Van Doesum, K. T. M., Witteman, C. L. M. & Hosman, C. M. H. The relation between parental mental illness and adolescent mental health: the role of family factors. J. Child. Fam. Stud. 23, 1201–1214 (2014).
Shonkoff, J. P. et al. The lifelong effects of early childhood adversity and toxic stress. Pediatrics 129, e232–e246 (2012).
Hall, B. S., Moda, R. N. & Liston, C. Glucocorticoid mechanisms of functional connectivity changes in stress-related neuropsychiatric disorders. Neurobiol. Stress 1, 174–183 (2015).
Eiland, L. & Romeo, R. D. Stress and the developing adolescent brain. Neuroscience 249, 162–171 (2013).
Liston, C. & Gan, W.-B. Glucocorticoids are critical regulators of dendritic spine development and plasticity in vivo. Proc. Natl Acad. Sci. USA 108, 16074–16079 (2011).
Ehsan, A., Klaas, H. S., Bastianen, A. & Spini, D. Social capital and health: a systematic review of systematic reviews. SSM Popul. Health 8, 100425 (2019).
Kawachi, I., Kennedy, B. P., Lochner, K. & Prothrow-Stith, D. Social capital, income inequality, and mortality. Am. J. Public Health 87, 1491–1498 (1997).
Owens, M. M. et al. Investigation of psychiatric and neuropsychological correlates of default mode network and dorsal attention network anticorrelation in children. Cereb. Cortex 30, 6083–6096 (2020).
Jirsaraie, R. J. et al. Mapping the neurodevelopmental predictors of psychopathology. Mol. Psychiatry 30, 478–488 (2024).
Xu, Z., Zhao, W., Wang, H., Tian, Y. & Lei, X. Functional connectivity between dorsal attention and default mode networks mediates subjective sleep duration and depression in young females. J. Affect. Disord. 325, 386–391 (2023).
van Tol, M.-J. et al. Regional brain volume in depression and anxiety disorders. Arch. Gen. Psychiatry 67, 1002–1011 (2010).
Romer, A. L., Ren, B. & Pizzagalli, D. A. Brain structure relations with psychopathology trajectories in the ABCD study. J. Am. Acad. Child Adolesc. Psychiatry 62, 895–907 (2023).
Shen, X. et al. Brain structural associations with depression in a large early adolescent sample (the ABCD study). EClinicalMedicine 42, 101204 (2021).
Shad, M. U., Muddasani, S. & Rao, U. Gray matter differences between healthy and depressed adolescents: a voxel-based morphometry study. J. Child Adolesc. Psychopharmacol. 22, 190–197 (2012).
Li, Q., Whittle, S. & Rakesh, D. (2025). Longitudinal associations between greenspace exposure, structural brain development, and mental health and academic performance during early adolescence. Biol. Psychiatry https://doi.org/10.1016/j.biopsych.2025.03.026 (2025).
Raniti, M., Rakesh, D., Patton, G. C. & Sawyer, S. M. The role of school connectedness in the prevention of youth depression and anxiety: a systematic review with youth consultation. BMC Public Health 22, 2152 (2022).
Maio, F. G. D. Income inequality measures. J. Epidemiol. Community Health 61, 849–852 (2007).
Hero, R. E. & Levy, M. E. The racial structure of inequality: consequences for welfare policy in the United States. Soc. Sci. Q. 99, 459–472 (2018).
Hero, R. E. & Levy, M. E. The racial structure of economic inequality in the United States: understanding change and continuity in an era of “great divergence”. Soc. Sci. Q. 97, 491–505 (2016).
Vargas, T., Conley, R. E. & Mittal, V. A. Chronic stress, structural exposures and neurobiological mechanisms: a stimulation, discrepancy and deprivation model of psychosis. Int. Rev. Neurobiol. 152, 41–69 (2020).
Erdem, Ö., Prins, R. G., Voorham, T. A. J. J., van Lenthe, F. J. & Burdorf, A. Structural neighbourhood conditions, social cohesion and psychological distress in the Netherlands. Eur. J. Public Health 25, 995–1001 (2015).
Emerson, S. D., Minh, A. & Guhn, M. Ethnic density of regions and psychiatric disorders among ethnic minority individuals. Int. J. Soc. Psychiatry 64, 130–144 (2018).
Funder, D. C. & Ozer, D. J. Evaluating effect size in psychological research: sense and nonsense. Adv. Methods Pract. Psychol. Sci. 2, 156–168 (2019).
Barch, D. M. et al. Demographic and mental health assessments in the adolescent brain and cognitive development study: updates and age-related trajectories. Dev. Cogn. Neurosci. 52, 101031 (2021).
Garavan, H. et al. Recruiting the ABCD sample: design considerations and procedures. Dev. Cogn. Neurosci. 32, 16–22 (2018).
Wilkinson, R. G. & Pickett, K. E. Income inequality and population health: a review and explanation of the evidence. Soc. Sci. Med. 62, 1768–1784 (2006).
Hsieh, C.-C. & Pugh, M. D. Poverty, income inequality, and violent crime: a meta-analysis of recent aggregate data studies. Crim. Justice Rev. 18, 182–202 (1993).
Kondo, N. et al. Income inequality and health: the role of population size, inequality threshold, period effects and lag effects. J. Epidemiol. Community Health 66, e11 (2012).
Achenbach, T. M., McConaughy, S. H., Ivanova, M. Y. & Rescorla, L. A. Manual for the ASEBA Brief Problem Monitor for Ages 6–18 (ASEBA)
Achenbach, T. M. & Rescorla, L. Manual for the ASEBA School-Age Forms and Profiles: An Integrated System of Multi-Informant Assessment (ASEBA, 2001).
Saragosa-Harris, N. M. et al. A practical guide for researchers and reviewers using the ABCD study and other large longitudinal datasets. Dev. Cogn. Neurosci. 55, 101115 (2022).
Increases in TANF cash benefit levels are critical to help families meet rising costs. Center on Budget and Policy Priorities https://www.cbpp.org/research/income-security/increases-in-tanf-cash-benefit-levels-are-critical-to-help-families-meet-0 (2014).
Weissman, D. G., Hatzenbuehler, M. L., Cikara, M., Barch, D. M. & McLaughlin, K. A. State-level macro-economic factors moderate the association of low income with brain structure and mental health in US children. Nat. Commun. 14, 2085 (2023).
Maruschak, L. Correctional populations in the United States, 2017−2018. https://bjs.ojp.gov/library/publications/correctional-populations-unitedstates-2017-2018 (2020).
Data.Medicaid.gov. Centers for Medicare and Medicaid Services. https://data.medicaid.gov/ (2021).
Achenbach, T. M. in Encyclopedia of Clinical Neuropsychology (Springer, 2018); https://doi.org/10.1007/978-3-319-56782-2_1529-3
Casey, B. J. et al. The Adolescent Brain Cognitive Development (ABCD) study: imaging acquisition across 21 sites. Dev. Cogn. Neurosci. 32, 43–54 (2018).
Hagler, D. J. et al. Image processing and analysis methods for the Adolescent Brain Cognitive Development study. Neuroimage 202, 116091 (2019).
Hackman, D. A. et al. Association of local variation in neighborhood disadvantage in metropolitan areas with youth neurocognition and brain structure. JAMA Pediatrics 175, e210426 (2021).
Taylor, R. L., Cooper, S. R., Jackson, J. J. & Barch, D. M. Assessment of neighborhood poverty, cognitive function, and prefrontal and hippocampal volumes in children. JAMA Netw. Open 3, e2023774 (2020).
Acknowledgements
D.R. acknowledges support from a Young Investigator Grant from the Brain and Behaviour Research Foundation (no. 32908) and a New Investigator Research Grant from the UKRI Medical Research Council (no. MR/Z506667/1). T.V. acknowledges funding from the National Institute of Mental Health (NIMH) (no. R37-MH119194-05S2). Data used in the preparation of this article were obtained from the ABCD study (https://abcdstudy.org) held in the NIMH Data Archive. This is a multisite, longitudinal study designed to recruit more than 11,000 children ages 9–10 years old and follow them over 10 years into early adulthood. The ABCD study is supported by the National Institutes of Health and additional federal partners under award numbers U01DA041048, U01DA050989, U01DA051016, U01DA041022, U01DA051018, U01DA051037, U01DA050987, U01DA041174, U01DA041106, U01DA041117, U01DA041028, U01DA041134, U01DA050988, U01DA051039, U01DA041156, U01DA041025, U01DA041120, U01DA051038, U01DA041148, U01DA041093, U01DA041089, U24DA041123 and U24DA041147. A full list of supporters is available at https://abcdstudy.org/federal-partners.html. A listing of participating sites and a complete listing of the study investigators can be found at https://abcdstudy.org/consortium_members/. ABCD consortium investigators designed and implemented the study and/or provided data but did not necessarily participate in the analysis or writing of this report. The views expressed in this paper are those of the authors and do not necessarily reflect the official views of the National Institutes of Health, the Department of Health and Human Services, the US federal government or ABCD consortium investigators.
Author information
Authors and Affiliations
Contributions
D.R. conceptualized the study and research design, conducted analyses and wrote and revised the first and subsequent drafts of the paper. D.I.T. and T.V. consulted on the analysis plan and provided additional feedback on the paper. K.E.P. and V.P. provided feedback on the analysis plan, critical feedback on the paper and expert guidance and support. All authors approved the final version before submission. All authors have read and agreed to the published version of the paper.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Mental Health thanks Pilyoung Kim, Genevieve Patterson, Xueyi Shen and the other, anonymous reviewer(s) for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary Information
Supplementary Tables 1–23, Figs. 1 and 2, rationale and Discussion.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rakesh, D., Tsomokos, D.I., Vargas, T. et al. Macroeconomic income inequality, brain structure and function, and mental health. Nat. Mental Health 3, 1318–1330 (2025). https://doi.org/10.1038/s44220-025-00508-1
Received:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s44220-025-00508-1
