
Abstract
Theoretical models suggest that attention-deficit/hyperactivity and problematic online gaming could contribute to negative mental health outcomes, yet evidence on their interplay remains limited. Using data from 3171 adolescents in the Tokyo Teen Cohort, the present study examined the interplay of attention-deficit/hyperactivity at age 12 and problematic online gaming at age 14 associated with mental health issues at age 16. The sample consisted of 1487 girls (46.9%) and 1684 boys (53.1%). Doubly robust estimation revealed that a high degree of problematic online gaming consistently elevated the absolute and relative risks of mental health issues. The fully adjusted risk difference and risk ratio (95% confidence intervals (CIs)) were: incident depression, 7.8% (3.0%–13.1%) and 1.62 (1.25–2.05); incident anxiety, 5.7% (2.7%–8.7%) and 1.98 (1.45–2.67); incident psychotic experiences, 5.9% (2.3%–10.8%) and 1.72 (1.30–2.47); diminished well-being, 9.6% (5.1%–14.3%) and 1.54 (1.27–1.84). Higher attention-deficit/hyperactivity scores were associated with a greater degree of problematic online gaming (adjusted β per 1 SD: 0.18, 95% CI: 0.12–0.24). Causal mediation analysis—ensuring temporal plausibility, carefully adjusting for confounders, and accounting for exposure–mediator interaction—showed that problematic online gaming partially mediated the association between attention-deficit/hyperactivity and mental health issues: depressive symptoms (29.2%), anxiety (12.3%), psychotic experiences (20.6%), and diminished well-being (22.1%). The findings highlight the interplay of psychopathology, diminished inhibitory control, and addictive behaviors associated with negative consequences. Problematic online gaming may represent a modifiable mediator, warranting further intervention research to examine its potential as a treatment target.
Similar content being viewed by others

Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a prevalent neurodevelopmental condition, affecting ~8% of children and adolescents globally, with boys being twice as likely to be diagnosed as girls1. This condition imposes a substantial economic burden worldwide through healthcare costs, educational support needs, and productivity losses2. Past research suggests that ADHD is associated with mental health challenges, including depression, anxiety, psychotic experiences, and diminished well-being3,4,5,6.
Gaming disorder has been included in the International Classification of Diseases 11th Revision7, and internet gaming disorder has been included in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) as a condition for further study8. Cross-sectional studies suggested an association between problematic gaming behaviors and suicidal outcomes9,10. Also, a recent cohort study suggested a longitudinal association of offline video gaming and computer use (including computer-based gaming) with mental health issues, although residual confounding was likely11.
Theoretical frameworks may offer useful insights into how attention-deficit/hyperactivity and problematic online gaming could potentially contribute to negative mental health outcomes. Specifically, theoretical models introduced by Brand et al. and Dong et al.12,13,14 suggest that addictive behaviors may emerge via the pathway involving psychopathology and diminished inhibitory control, potentially leading to long-term adverse consequences. Attention-deficit/hyperactivity, characterized by core features of psychopathology as well as diminished inhibitory control8,15, aligns with the foundational elements of these models. Problematic online gaming, as a form of addictive behavior, may arise in response to external and internal triggers interacting with these factors. While such behaviors may provide short-term gratification, they may result in long-term negative outcomes, including worsened mental health. Fig. 1 illustrates the potential pathway, highlighting how psychopathology, diminished inhibitory control, and addictive behaviors contribute to negative mental health consequences in the context of attention-deficit/hyperactivity and problematic online gaming. Given the heterogeneous nature of problematic online gaming, it may, similar to other forms of addictive behaviors8, be associated with a range of negative mental health outcomes depending on individual vulnerabilities and contextual factors.

The psychopathological aspects of attention-deficit/hyperactivity may act as predisposing factors influencing triggers. These triggers can be further affected by the diminished inhibitory control associated with attention-deficit/hyperactivity, contributing to the development of addictive behaviors like problematic online gaming. Problematic online gaming, while providing immediate gratification, may lead to negative consequences.
Based on the theoretical models mentioned above, we hypothesized that attention-deficit/hyperactivity increases the likelihood of engaging in problematic online gaming; problematic online gaming contributes to mental health issues. Indeed, previous studies suggested the association between attention-deficit/hyperactivity and problematic online gaming16,17,18,19, as well as between problematic online gaming and negative mental health outcomes20,21,22,23. We additionally hypothesized that problematic online gaming serves as a mediator between attention-deficit/hyperactivity and these outcomes. These hypotheses are interconnected and aim to address the following:
(1) Problematic online gaming is associated with subsequent mental health issues.
(2) Attention-deficit/hyperactivity is associated with subsequent problematic online gaming.
(3) Problematic online gaming mediates the relationship between attention-deficit/hyperactivity and mental health issues, accounting for its interaction with attention-deficit/hyperactivity.
This study explores the dynamic interplay of attention-deficit/hyperactivity and problematic online gaming associated with mental health, with a particular focus on problematic online gaming as a modifiable mediator. By examining these relationships, this study aims to provide empirical support for theoretical models and inform clinical and public health strategies. We employed causal mediation analysis to investigate the mediation effect of problematic online gaming on the relationship between attention-deficit/hyperactivity and mental health issues. This approach requires several key considerations24:
(a) A clear temporal order of exposure, mediator, and outcome.
(b) Control for exposure-mediator confounding and mediator-outcome confounding, as well as exposure-outcome confounding, when evaluating natural direct and indirect effects.
(c) Consideration of exposure-mediator interaction.
Unfortunately, studies employing mediation analysis often encounter these methodological challenges, which hinder their interpretations and the applicability of their findings to real-world contexts24. This underscores the need for more rigorous causal inference approaches to provide meaningful implications. In the present study, we aimed to address all of these considerations by using three time-point data, carefully adjusting for confounding, and incorporating the exposure-mediator interaction (the interaction between attention-deficit/hyperactivity and problematic online gaming).
Methods
Participants
We used data from the Tokyo Teen Cohort, a population-based cohort with multiple time points25. The eligibility criteria were as follows: (1) adolescents born between September 2002 and August 2004, (2) living in one of three municipalities in Japan (Setagaya, Mitaka, or Chofu), and (3) written parental consent was obtained. Note that adolescents were included regardless of the degree of problematic online gaming. A random sampling via the basic resident register was conducted in these municipalities. A total of 3171 child-parent pairs participated at age 10 (November 2012 to January 2015), 3007 at age 12 (August 2014 to January 2017; follow-up rate: 94.8%), 2667 at age 14 (August 2014 to January 2017; follow-up rate: 84.1%), and 2616 at age 16 (February 2019 to September 2021; follow-up rate: 82.5%). Trained interviewers visited the participants’ homes and provided self-report questionnaires to child-parent pairs at each time point. While we used information from ages 12, 14, and 16 in the present study, all 3171 children were included in the analysis using the imputation method, as highlighted in the “Statistical analysis” section. All procedures were approved by the Institutional Review Boards of the Tokyo Metropolitan Institute of Medical Science (12-35), the University of Tokyo (10057), and the SOKENDAI (2012002). All parents provided written informed consent. This study was not pre-registered. Data on race and ethnicity were not collected.
Attention-deficit/hyperactivity
To assess attention-deficit/hyperactivity at age 12, we employed the Strengths and Difficulties Questionnaire hyperactivity/inattention subscale26, a parent-report five-item measure widely used in epidemiological studies. The subscale evaluates behaviors such as restlessness, overactivity, and difficulties in sustaining attention. Each item was rated on a three-point scale: “not true,” “somewhat true,” and “certainly true” scored as 0, 1, and 2 points, respectively. The score was calculated by summing the responses (possible range 0–10), with higher scores indicating greater levels of attention-deficit/hyperactivity. The data demonstrated acceptable internal consistency (Cronbach’s α, 0.75).
Problematic online gaming
We assessed problematic online gaming at age 14 using a self-reported measure employed in the previous study27. This measure was originally developed based on modified gambling disorder criteria, rather than the proposed internet gaming disorder criteria in the DSM-5-TR8. This measure included nine items with yes/no response options evaluating the presence of behaviors or emotions associated with addiction to online games over the past 12 months. Some items, such as those related to chasing behavior and financial reliance, may reflect constructs characteristic of gambling disorder features. Details of items can be found in Supplementary Table 1. The score was calculated by summing the responses (possible range 0–9), with higher scores indicating greater levels of problematic online gaming. For dichotomization, a cut-off of four or more symptoms was used, consistent with gambling disorder criteria rather than internet gaming disorder criteria8. The data demonstrated limited internal consistency (Cronbach’s α, 0.64), and thus the results should be interpreted with caution.
Mental health outcomes
To assess depressive symptoms at ages 12 and 16, we employed the Short Mood and Feelings Questionnaire (SMFQ), a standard 13-item self-report measure28,29, following the recommendation from the NICE guidance30. The scale evaluates depressive symptoms over the past 2 weeks. Each item had three response options: “always,” “sometimes,” and “never,” scored with 2, 1, and 0 points, respectively. Items were summed into a composite score (possible range 0–26); a greater score suggests a higher degree of depressive symptoms. The data demonstrated strong internal consistency (Cronbach’s α, 0.92).
To assess anxiety at ages 12 and 16, we utilized the Child Behavior Checklist (CBCL)31, a widely used caregiver-reported questionnaire consisting of 118 items. To mitigate the burden on participants, we selected 84 items from the CBCL for the survey. Of these, 14 items were specifically designed to assess anxiety, derived from the CBCL anxiety scale, which initially comprised 16 items. The scale evaluates anxiety symptoms over the past 6 months. Each item was evaluated on a three-point scale: “not true,” “somewhat or sometimes true,” and “very true or often true.” A total score was calculated by summing the responses for each item, with higher scores indicating a higher degree of anxiety (possible range 0–28). The data demonstrated acceptable internal consistency (Cronbach’s α, 0.78).
We assessed psychotic experiences32 at ages 12 and 16 using the Adolescent Psychotic-like Symptom Screener (APSS), an established seven-item self-report questionnaire33,34. Each item had three response options: “yes, definitely,” “maybe,” and “no, never,” scored with 1, 0.5, and 0 points, respectively. At age 12, participants were asked about lifetime experiences, while at age 16, they were asked about experiences within the past 2 years. Items were summed into a total score (possible range 0–7); a greater score suggests a higher degree of psychotic experiences. Details of items can be found in Supplementary Table 2. The data demonstrated acceptable internal consistency (Cronbach’s α, 0.71).
To assess well-being at ages 12 and 16, we employed the WHO-Five Well-Being Index (WHO-5), a standard five-item self-report questionnaire35. The WHO-5 evaluates well-being over the past 2 weeks, assessing positive aspects of mental health, such as mood, vitality, and general interest in life. Each item had six response options: “not at all,” “a little,” “somewhat,” “quite a bit,” “a lot,” and “all of the time.” A total score was calculated by summing the responses and multiplying by four (possible range 0–100), with higher scores indicating better well-being. The data demonstrated good internal consistency (Cronbach’s α, 0.81).
Covariates
We selected covariates at age 12 based on the modified disjunctive cause criterion to adjust for potential causes of the exposure, outcome, or both, excluding instrumental variables and including covariates that acted as proxies for unmeasured variables that are common causes of both the exposure and the outcome36. The model included age, gender, body mass index37, IQ38, household income39, loneliness40,41, physical punishment38, relationships of mother, father, and friends42, neighborhood cohesion43,44, and gender nonconforming behavior42. Per analysis, we included the baseline level of each mental health condition, time spent gaming, and problematic internet use at age 12, thereby mitigating the possibility of reverse causation. Although direct information on problematic online gaming at age 12 was unavailable, the set of time spent gaming and problematic internet use was supposed to serve as a proxy45 for problematic online gaming due to its overlap, and conditioning on these variables as covariates aimed to mitigate the confounding bias caused by problematic online gaming at this age. Details on covariates are shown in Supplementary Method 1.
Statistical analysis
All analyses were performed using R 4.4.1. First, we conducted a regression analysis to evaluate the association between problematic online gaming at age 14 and mental health at age 16, namely depressive symptoms, anxiety, psychotic experiences, and well-being. We fitted three models: Model 1 was unadjusted; Model 2 adjusted for age, gender, body mass index, IQ, and household income at age 12; and Model 3 adjusted for the variables included in Model 2, loneliness, physical punishment, relationships with mother, father, and friends, neighborhood cohesion, gender nonconformity, and the baseline level of each mental health condition at age 12.
Subsequently, we applied doubly robust estimation, dichotomizing the exposure and outcomes, while adjusting for the aforementioned covariates included in Model 3. Doubly robust estimation is a causal inference approach designed to be robust to potential model misspecification46. To develop a doubly robust estimator, we first fitted propensity models to calculate inverse probability weights. Using these weights, we implemented canonical link generalized linear models. While such models do not automatically yield a doubly robust estimator, we subsequently applied standardization (the g-formula) for the average causal effects (risk difference (RD) and risk ratio (RR)) to ensure the doubly robust property. Problematic online gaming was dichotomized using a cut-off score of four (low degree: 0–3; high degree: 4–9), consistent with prior research27. Depressive symptoms were dichotomized with a cut-off score of eight on the SMFQ28, while anxiety was dichotomized with a T-score of 6547. Psychotic experiences were identified by selecting “yes, definitely” for at least one item on the APSS34. Diminished well-being was dichotomized using a cut-off score of 50 on the WHO-535.
For the doubly robust estimation, we explored effect heterogeneity across genders. To achieve this, we employed models with a product term between problematic online gaming and gender. We then computed the relative excess risk due to interaction (RERI) as an additive scale, as well as the ratio of risk ratios (RRR) as a multiplicative scale. The RERI and RRR demonstrate how the combined effects of problematic online gaming and gender influence the RR for mental health issues beyond their individual effects in both additive and multiplicative ways. The calculations for RERI and RRR are detailed in Supplementary Method 2.
To assess the robustness of the association between problematic online gaming and mental health outcomes, we conducted four sensitivity analyses. First, we performed regression analyses evaluating problematic online gaming as a dichotomous variable. Second, we conducted Poisson regression analyses, treating mental health issues as dichotomous variables. Third, for the doubly robust estimation, we analyzed E-values to estimate the degree of unmeasured confounding necessary to negate the observed associations. Fourth, we excluded loneliness from the model, considering that loneliness was assessed via the SMFQ, which was also used to examine depressive symptoms.
Next, we evaluated the association between attention-deficit/hyperactivity at age 12 and problematic online gaming at age 14. We fitted three models: Model 1 was unadjusted; Model 2 adjusted for age, gender, body mass index, IQ, and household income at age 12; and Model 3 adjusted for the variables included in Model 2, loneliness, physical punishment, relationships with mother, father, and friends, neighborhood cohesion, gender nonconformity, and the baseline level of time spent gaming and problematic internet use at age 12.
Lastly, we conducted a causal mediation analysis48 to examine the interplay of attention-deficit/hyperactivity (exposure) and problematic online gaming (mediator) associated with subsequent mental health issues (outcomes). To ascertain the clear temporal order, we used data on attention-deficit/hyperactivity at age 12, problematic online gaming at age 14, and mental health issues at age 16. To address the exposure-mediator, mediator-outcome, and exposure-outcome confounding, we adjusted for age, gender, body mass index, IQ, household income, loneliness, physical punishment, relationships with mother, father, and friends, neighborhood cohesion, gender nonconformity, as well as the baseline levels of time spent gaming, problematic internet use, and each mental health outcome condition at age 12. To capture the dynamics of mediation, we included the interaction of exposure (attention-deficit/hyperactivity) and mediator (problematic online gaming).
Addressing these key considerations, we used a two-way decomposition analysis, decomposing the total effect of attention-deficit/hyperactivity on mental health into the pure direct effect and total indirect effect49,50.
Total Effect = Pure Direct Effect + Total Indirect Effect
-
Total Effect: The total effect of a one standard deviation (SD) increase from the mean in the attention-deficit/hyperactivity score on mental health, accounting for both the pathways with and without problematic online gaming.
-
Pure Direct Effect: The effect of a 1 SD increase from the mean in the attention-deficit/hyperactivity score on mental health, fixing the problematic online gaming score to the value that an individual would take if the attention-deficit/hyperactivity score were at the mean.
-
Total Indirect Effect: The effect of changing the problematic online gaming score from the value that an individual would take if the attention-deficit/hyperactivity score were at the mean to the value that the same individual would take if the attention-deficit/hyperactivity score were increased by 1 SD, fixing the attention-deficit/hyperactivity score at the 1 SD increased value.
Note that we examined the effects for a 1 SD increase from the mean in attention-deficit/hyperactivity as a standard approach, while any two trajectories can be compared51. Proportion mediated was calculated by dividing the total indirect effect by the total effect.
Proportion Mediated = Total Indirect Effect/Total Effect
Proportion mediated represents the proportion of the total effect attributable to the causal pathway through problematic online gaming, which reflects the importance of problematic online gaming-related mechanisms in explaining the effect of attention-deficit/hyperactivity on mental health.
For valid inference of natural direct and indirect effects, four assumptions must hold48:
(A) No exposure-outcome confounding after the adjustments.
(B) No mediator-outcome confounding after the adjustments.
(C) No exposure-mediator confounding after the adjustments.
(D) No mediator-outcome confounders influenced by exposure.
While these assumptions are unverifiable, we sought to account for potential confounding as thoroughly as possible, as described above. As a sensitivity analysis for the mediation effect, we excluded loneliness from the model, considering that loneliness was assessed via the SMFQ, which was also used to examine depressive symptoms.
For regression analyses involving continuous outcomes, data distribution was assumed to be normal, but this was not formally tested. Missing data were handled via random forest imputation52. All analyses were stratified by gender. β is reported per 1 SD increase in the exposure; its magnitude depends on each outcome’s scale and is not comparable across outcomes. Confidence intervals (CIs) were calculated using the standard error for regression analysis, the percentile bootstrap approach for the doubly robust estimation, and the delta method for the mediation analysis.
Results
Baseline characteristics
Table 1 summarizes the baseline characteristics of the study population at age 12, comparing participants with and without attention-deficit/hyperactivity data. The mean age was 12.2 years (SD, 0.28). The sample consisted of 1487 girls (46.9%) and 1684 boys (53.1%). Participants missing attention-deficit/hyperactivity data appeared more likely to be male, had a higher degree of depressive symptoms and psychotic experiences, a lower degree of anxiety and well-being, and a higher degree of problematic internet use. Other characteristics appeared similar. The interpretation of these differences should be considered carefully, as the group missing attention-deficit/hyperactivity data had substantially higher rates of missing data across most variables (frequently exceeding 90%) compared to those with attention-deficit/hyperactivity data (typically 15–20%).
Association between problematic online gaming and mental health
Gender-specific scores for problematic online gaming at age 14 and mental health outcomes at age 16 are shown in Supplementary Table 3. First, we conducted regression analysis to examine the association between problematic online gaming at age 14 and mental health at age 16 (Table 2 and Supplementary Fig. 1.) In Model 3 (the fully adjusted model), higher problematic online gaming scores were associated with all mental health outcomes: a higher degree of depressive symptoms (β: 0.91, 95% CI: 0.73–1.08, p < 0.001), a higher degree of anxiety (β: 0.44, 95% CI: 0.34–0.54, p < 0.001), a higher degree of psychotic experiences (β: 0.09, 95% CI: 0.06–0.11, p < 0.001), and a lower degree of well-being (β: –3.24, 95% CI: −3.95 to −2.53, p < 0.001). These associations were consistently demonstrated across genders and across Model 1 to Model 3.
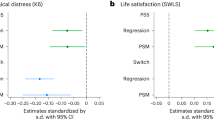
Subsequently, we applied doubly robust estimation to further investigate these associations (Fig. 2 and Supplementary Table 4)46. A high degree of problematic online gaming was consistently associated with both increased absolute and relative risks across mental health outcomes. The fully adjusted RD and RR (95% CIs) were as follows: incident depression, 7.8% (3.0%–13.1%) and 1.62 (1.25–2.05); incident anxiety, 5.7% (2.7%–8.7%) and 1.98 (1.45–2.67); incident psychotic experiences, 5.9% (2.3%–10.8%) and 1.72 (1.30–2.47); diminished well-being, 9.6% (5.1%–14.3%) and 1.54 (1.27–1.84).

A Risk difference; B risk ratio. Mental health issues at age 16 were compared between high and low problematic online gaming groups at age 14, adjusting for a wide range of covariates (see “Methods” section). To develop a doubly robust estimator, we first fitted propensity models to calculate inverse probability weights. Using these weights, we implemented canonical link generalized linear models. While such models do not automatically yield a doubly robust estimator, we subsequently applied standardization (the g-formula) for the average causal effects to ensure the doubly robust property.
For the doubly robust estimation, we explored the interaction between problematic online gaming and gender. Both genders showed elevated risks (Fig. 2 and Supplementary Table 4). Significant additive interaction was shown for incident depression (RERI: 1.21, 95% CI: 0.11–2.55), suggesting the absolute risk increase was larger in girls (Supplementary Table 5). On the other hand, no significant additive interaction was found for other outcomes. None of the outcomes showed significant multiplicative interaction.
We conducted four sensitivity analyses to assess the robustness of the association between problematic online gaming and subsequent mental health issues. First, we performed regression analyses evaluating problematic online gaming as a dichotomous variable and found significant associations with all mental health outcomes (Supplementary Table 6). Second, we conducted Poisson regression analyses, treating mental health issues as dichotomous variables, and observed significantly increased risks for all outcomes (Supplementary Table 7). Third, we examined the E-values for the doubly robust estimation and found that substantial unmeasured confounding would be required to explain away the observed estimates (E-values for point estimates: 2.62 for incident depression, 3.37 for incident anxiety, 2.82 for incident psychotic experiences, and 2.45 for diminished well-being) (Supplementary Table 8). Fourth, we excluded loneliness from the model and found that the findings remained consistent (Supplementary Table 9). Gender-stratified sensitivity analyses showed patterns consistent with our main findings.
Association between attention-deficit/hyperactivity and problematic online gaming
Next, we evaluated the association between attention-deficit/hyperactivity at age 12 and problematic online gaming at age 14 (Supplementary Fig. 2 and Supplementary Table 10). Gender-specific scores for attention-deficit/hyperactivity at age 12 are shown in Supplementary Table 3. In Model 3 (the fully adjusted model), higher attention-deficit/hyperactivity scores were associated with a greater degree of problematic online gaming (adjusted β per 1 SD: 0.18, 95% CI: 0.12–0.24, p < 0.001). These associations were consistently demonstrated across genders and across Model 1 to Model 3. As a sensitivity analysis, we analyzed problematic online gaming in a dichotomous manner and found that attention-deficit/hyperactivity remained significantly associated with a high degree of problematic online gaming (Supplementary Table 9).
Causal mediation analysis
Lastly, we conducted a causal mediation analysis, addressing critical methodological considerations outlined in Table 3. Fig. 3 shows the causal diagram representing the mediation effect of problematic online gaming at age 14 on the relationship between attention-deficit/hyperactivity at age 12 and mental health outcomes at age 16. Fig. 4 and Table 4 summarize the results for mediation effects. Significant total indirect effects were observed across all mental health outcomes: depressive symptoms (β: 0.08, 95% CI: 0.04–0.11, p < 0.001), anxiety (β: 0.04, 95% CI: 0.02–0.06, p < 0.001), psychotic experiences (β: 0.01, 95% CI: 0.01–0.02, p < 0.001), and diminished well-being (β: 0.28, 95% CI: 0.14–0.41, p < 0.001). The proportion mediated was 29.2% for depressive symptoms, 12.3% for anxiety, 20.6% for psychotic experiences, and 22.1% for diminished well-being. Gender-stratified analyses showed that the mediation effects were pronounced in both girls and boys. As a sensitivity analysis, we excluded loneliness from the adjustment model and found that the results did not substantially change (Supplementary Fig. 3 and Supplementary Table 12).

To capture the dynamics of mediation, we accounted for the interaction of exposure (attention-deficit/hyperactivity) and mediator (problematic online gaming).

Bars represent the proportion of the total effect of attention-deficit/hyperactivity at age 12 on mental health issues at age 16 that is attributable to the causal pathway through problematic online gaming at age 14. This reflects the importance of problematic online gaming–related mechanisms in explaining the effect of attention-deficit/hyperactivity on mental health issues.
Discussion
This study provides evidence supporting our three hypotheses: (1) problematic online gaming is associated with subsequent mental health issues, (2) attention-deficit/hyperactivity is associated with subsequent problematic online gaming, and (3) problematic online gaming mediates the relationship between attention-deficit/hyperactivity and mental health issues. A high degree of problematic online gaming showed 5%–10% absolute risk increases and 1.5–2-fold relative risk increases. These findings are consistent with previous studies showing that problematic online gaming was associated with later mental health issues 20,21,22,23. The results were robust in multiple sensitivity analyses. Although we found no significant multiplicative interaction, possibly due to limited statistical power, the absolute risk increase in depression was larger in girls. These findings align with our previous study53, which showed a greater impact of problematic internet use on depression in girls. While the reason for the gender-specific results on depression is beyond the scope of this paper, Japanese men are reportedly more likely than women to own and play gaming consoles and tend to spend more time playing video games54. Some platforms are more commonly linked to solitary play, whereas others are often used in in-person social contexts54. These differences might be related to heterogeneous patterns of online gaming across genders.
Our findings indicated that attention-deficit/hyperactivity was significantly associated with subsequent problematic online gaming, consistent with previous studies16,17,18,19. Problematic online gaming, in turn, mediated the relationship between attention-deficit/hyperactivity and adverse mental health outcomes. In accordance with the theoretical model12,13, the psychopathological aspects of attention-deficit/hyperactivity may act as predisposing factors influencing triggers. These triggers can be further affected by the diminished inhibitory control associated with attention-deficit/hyperactivity, contributing to the development of addictive behaviors like problematic online gaming. Problematic online gaming, while providing immediate gratification, may lead to negative consequences. To address key methodological considerations, we utilized three time-point data at ages 12, 14, and 16, ensuring a clear temporal order among exposure, mediator, and outcome, which allowed us to establish the directionality of these relationships. We also accounted for confounding factors as comprehensively as possible to enhance the robustness of our findings. Furthermore, our model addressed the interaction between attention-deficit/hyperactivity and problematic online gaming, thereby capturing the dynamics of mediation that are likely to exist in real-world settings. By addressing these key considerations, our findings provide robust empirical support for the existing theoretical models, emphasizing the complex role of psychopathology, diminished inhibitory control, and addictive behavior in leading to long-term negative outcomes. Pharmacological treatment for attention-deficit/hyperactivity is generally effective and widely used55, but it does not necessarily normalize symptoms56, i.e., the symptoms could remain only partially modifiable. In such cases, problematic online gaming may represent a modifiable mediator57. Further intervention study is warranted to examine its potential as a treatment target.
This study builds on and complements prior research emphasizing the positive aspects of gaming, such as fostering social connections and emotional regulation. A recent study employing a robust causal inference approach demonstrated a positive effect of gaming on mental health54. On the other hand, this study also highlighted the heterogeneity of these effects; for instance, the benefits diminished with longer gaming durations, and some early teens using platforms like the PlayStation 5 did not experience positive impacts. Thus, we believe our findings complement the authors’ study by showing that there are populations experiencing the negative impacts of gaming, depending on how they engage with it.
Limitations
This study has several limitations. First, despite the longitudinal design and the rich confounder adjustment, the possibility of residual confounding remains. Valid inference in causal mediation analysis relies on no-confounding assumptions (see the “Methods” section), but these assumptions are unverifiable. Specifically, we used the set of time spent gaming and problematic internet use as a proxy for problematic online gaming at age 12; however, it is unverifiable whether adjusting for this set was sufficient to account for the baseline level of problematic online gaming. Second, the potential for measurement bias exists, particularly with self-reported measures, which might not accurately capture the actual pathology as a clinical interview would. Also, the standardized measures used in this study were not formally validated in Japanese, which could further contribute to measurement bias. Moreover, the problematic online gaming measure demonstrated limited internal consistency, which warrants caution when interpreting the findings. Third, we lacked data on potentially important factors, e.g., substance use58 and physical injuries59,60. Also, we evaluated physical punishment as a proxy for adverse childhood experiences61,62 but did not consider other stressful or traumatic exposures, such as emotional neglect. Fourth, the transportability of our findings may be limited; the sample, predominantly of Asian ethnicity from the highly urbanized city, may not represent rural or diverse racial demographics well. Lastly, the effect of problematic online gaming could be better corroborated using the framework of target trial emulation. This framework can mitigate the influence of biases such as immortal time bias caused by the misalignment of the start of follow-up, eligibility, and treatment assignment (in this case, the initiation of problematic online gaming)63. For example, future studies should focus on the initiation of problematic online gaming rather than problematic online gaming at a particular time point, in the same way as randomized controlled trials examine the initiation of treatment. Achieving this would require consistent and frequent recording of measurements over time.
This study advances our understanding of the interplay of attention-deficit/hyperactivity and problematic online gaming associated with negative mental health outcomes, supporting existing theoretical models. Clinicians and educators should focus on identifying and addressing early signs of problematic online gaming. Problematic online gaming may represent a modifiable mediator, warranting further intervention research to examine its potential as a treatment target.
Data availability
The dataset containing the numerical estimates used to generate Fig. 2 (risk differences and risk ratios with 95% confidence intervals) is available on Zenodo: https://doi.org/10.5281/zenodo.1576092664. Data described in the manuscript will be made available upon request pending application and approval.
Code availability
The code used in this study is archived on Zenodo: https://doi.org/10.5281/zenodo.1576084165. This version corresponds to the GitHub repository at https://github.com/ZuiCNarita/DR-and-CMA250122 and reflects the analyses reported in the manuscript.
References
Ayano, G., Demelash, S., Gizachew, Y., Tsegay, L. & Alati, R. The global prevalence of attention deficit hyperactivity disorder in children and adolescents: an umbrella review of meta-analyses. J. Affect. Disord. 339, 860–866 (2023).
Doshi, J. A. et al. Economic impact of childhood and adult attention-deficit/hyperactivity disorder in the United States. J. Am. Acad. Child Adolesc. Psychiatry 51, 990–1002.e2 (2012).
Riglin, L. et al. ADHD and depression: investigating a causal explanation. Psychol. Med. 51, 1890–1897 (2021).
Quenneville, A. F. et al. Anxiety disorders in adult ADHD: A frequent comorbidity and a risk factor for externalizing problems. Psychiatry Res. 310, 114423 (2022).
Stickley, A., Shirama, A. & Sumiyoshi, T. Are attention-deficit/hyperactivity disorder symptoms associated with negative health outcomes in individuals with psychotic experiences? Findings from a cross-sectional study in Japan. Front. Psychiatry 14, 1133779 (2023).
Peasgood, T. et al. The impact of ADHD on the health and well-being of ADHD children and their siblings. Eur. Child Adolesc. Psychiatry 25, 1217–1231 (2016).
World Health Organization. International Classification of Diseases 11th Revision (ICD-11). https://icd.who.int/en (2022).
American Psychiatric Association. Diagnostic And Statistical Manual Of Mental Disorders, Fifth Edition, Text Revision (American Psychiatric Association, 2022).
Lin, I.-H. et al. The association between suicidality and Internet addiction and activities in Taiwanese adolescents. Compr. Psychiatry 55, 504–510 (2014).
Rikkers, W., Lawrence, D., Hafekost, J. & Zubrick, S. R. Internet use and electronic gaming by children and adolescents with emotional and behavioural problems in Australia—results from the second Child and Adolescent Survey of Mental Health and Wellbeing. BMC Public Health 16, 399 (2016).
Paquin, V. et al. Trajectories of adolescent media use and their associations with psychotic experiences. JAMA Psychiatryhttps://doi.org/10.1001/jamapsychiatry.2024.0384 (2024).
Brand, M. et al. The Interaction of Person-Affect-Cognition-Execution (I-PACE) model for addictive behaviors: update, generalization to addictive behaviors beyond internet-use disorders, and specification of the process character of addictive behaviors. Neurosci. Biobehav. Rev. 104, 1–10 (2019).
Brand, M., Young, K. S., Laier, C., Wölfling, K. & Potenza, M. N. Integrating psychological and neurobiological considerations regarding the development and maintenance of specific Internet-use disorders: an Interaction of Person-Affect-Cognition-Execution (I-PACE) model. Neurosci. Biobehav. Rev. 71, 252–266 (2016).
Dong, G. & Potenza, M. N. Risk-taking and risky decision-making in Internet gaming disorder: implications regarding online gaming in the setting of negative consequences. J. Psychiatr. Res. 73, 1–8 (2016).
Pang, T., Yang, L., Liu, Y. & Chang, S. The trajectory of attention deficit hyperactivity disorder symptoms and its dynamic relationship with inhibitory control. J. Child Psychol. Psychiatry https://doi.org/10.1111/jcpp.14112 (2025).
Lee, J., Bae, S., Kim, B. N. & Han, D. H. Impact of attention-deficit/hyperactivity disorder comorbidity on longitudinal course in Internet gaming disorder: a 3-year clinical cohort study. J. Child Psychol. Psychiatry 62, 1110–1119 (2021).
Marmet, S., Studer, J., Grazioli, V. S. & Gmel, G. Bidirectional associations between Self-reported gaming disorder and Adult attention deficit hyperactivity disorder: evidence from a sample of young Swiss men. Front. Psychiatry 9, 649 (2018).
Wang, J.-L., Yin, X.-Q., Wang, H.-Z., King, D. L. & Rost, D. H. The longitudinal associations between internet addiction and ADHD symptoms among adolescents. J. Behav. Addict. 13, 191–204 (2024).
Koncz, P. et al. The emerging evidence on the association between symptoms of ADHD and gaming disorder: A systematic review and meta-analysis. Clin. Psychol. Rev. 106, 102343 (2023).
Wright, M. F. & Wachs, S. Problematic online gaming, subjective health complaints, and depression among adolescent gamers from the United States: the role of console-gaming aggression. J. Child. Media 16, 451–460 (2022).
Wartberg, L., Kriston, L., Zieglmeier, M., Lincoln, T. & Kammerl, R. A longitudinal study on psychosocial causes and consequences of Internet gaming disorder in adolescence. Psychol. Med. 49, 287–294 (2019).
Chen, C.-Y. et al. The relationship between children’s problematic Internet-related behaviors and psychological distress during the onset of the COVID-19 pandemic: a longitudinal study. J. Addict. Med. 16, e73–e80 (2022).
Chen, I.-H. et al. Problematic internet-related behaviors mediate the associations between levels of internet engagement and distress among schoolchildren during COVID-19 lockdown: a longitudinal structural equation modeling study. J. Behav. Addict. 10, 135–148 (2021).
Narita, Z. C., Miyashita, M., Furukawa, T. A. & Nishida, A. Key considerations in mediation analysis for psychiatric research. JAMA Psychiatry https://doi.org/10.1001/jamapsychiatry.2025.0566 (2025).
Ando, S. et al. Cohort Profile: The Tokyo Teen Cohort study (TTC). Int. J. Epidemiol. 48, 1414–1414g (2019).
Goodman, R. Psychometric properties of the strengths and difficulties questionnaire. J. Am. Acad. Child Adolesc. Psychiatry 40, 1337–1345 (2001).
Ide, S. et al. Adolescent problem gaming and loot box purchasing in video games: cross-sectional observational study using population-based cohort data. JMIR Serious Games 9, e23886 (2021).
Angold, A., Costello, E. J., Messer, S. C. & Pickles, A. Development of a short questionnaire for use in epidemiological studies of depression in children and adolescents. Int. J. Methods Psychiatr. Res. 5, 237–249 (1995).
Sharp, C., Goodyer, I. M. & Croudace, T. J. The Short Mood and Feelings Questionnaire (SMFQ): a unidimensional item response theory and categorical data factor analysis of self-report ratings from a community sample of 7-through 11-year-old children. J. Abnorm. Child Psychol. 34, 379–391 (2006).
National Institute for Health and Care Excellence. Depression in children and young people: identification and management [NICE guideline NG134]. London: NICE; 2019.
Itani, T. Standardization of the Japanese version of the Child Behavior Checklist/4-18. Psychiatr. Neurol. Pediatr. Jpn. 41, 243–252 (2001).
Narita, Z. C. Bias against psychotic experiences in peer review. Psychiatry Res. 350, 116549 (2025).
Laurens, K. R. et al. Community screening for psychotic-like experiences and other putative antecedents of schizophrenia in children aged 9-12 years. Schizophr. Res. 90, 130–146 (2007).
Kelleher, I., Harley, M., Murtagh, A. & Cannon, M. Are screening instruments valid for psychotic-like experiences? A validation study of screening questions for psychotic-like experiences using in-depth clinical interview. Schizophr. Bull. 37, 362–369 (2011).
Topp, C. W., Østergaard, S. D., Søndergaard, S. & Bech, P. The WHO-5 Well-Being Index: a systematic review of the literature. Psychother. Psychosom. 84, 167–176 (2015).
VanderWeele, T. J. Principles of confounder selection. Eur. J. Epidemiol. 34, 211–219 (2019).
Jung, S. J. et al. Association between body size, weight change and depression: systematic review and meta-analysis. Br. J. Psychiatry 211, 14–21 (2017).
Edwards, V. J., Holden, G. W., Felitti, V. J. & Anda, R. F. Relationship between multiple forms of childhood maltreatment and adult mental health in community respondents: results from the adverse childhood experiences study. Am. J. Psychiatry 160, 1453–1460 (2003).
Sareen, J., Afifi, T. O., McMillan, K. A. & Asmundson, G. J. G. Relationship between household income and mental disorders: findings from a population-based longitudinal study. Arch. Gen. Psychiatry 68, 419–427 (2011).
Narita, Z., Stickley, A. & DeVylder, J. Loneliness and psychotic experiences in a general population sample. Schizophr. Res. 218, 146–150 (2020).
Narita, Z. et al. Loneliness and psychotic experiences among US university students: findings from the Healthy Minds Study 2020. Psychiatry Res. 308, 114362 (2021).
Narita, Z. et al. Uncovering associations between gender nonconformity, psychosocial factors, and mental health in adolescents: a birth cohort study. Psychol. Med. 54, 921–930 (2024).
Narita, Z. et al. Neighborhood change and psychotic experiences in a general population sample. Schizophr. Res. 216, 316–321 (2020).
Fedina, L. et al. Moderating effects of perceived neighborhood factors on intimate partner violence, psychological distress, and suicide risk. J. Interpers. Violence 36, 10546–10563 (2021).
Hernán, M. & Robins, J. Causal Inference: What If. 257–275 (Chapman & Hall/CRC, 2020).
Gabriel, E. E. et al. Inverse probability of treatment weighting with generalized linear outcome models for doubly robust estimation. Stat. Med. 43, 534–547 (2024).
Funabiki, Y. & Murai, T. Standardization of the ASEBA Child Behavior Checklist (CBCL: Ages 6-18) in Japan. Jpn. J. Child Adolesc. Psychiatry Relat. Fields 58, 175–184 (2017).
VanderWeele, T. J. Explanation in Causal Inference: Methods for Mediation and Interaction (Oxford University Press, 2015).
Yazawa, A. et al. Early childhood adversity and late-life depressive symptoms: unpacking mediation and interaction by adult socioeconomic status. Soc. Psychiatry Psychiatr. Epidemiol. 57, 1147–1156 (2022).
VanderWeele, T. J. A unification of mediation and interaction: a 4-way decomposition. Epidemiology 25, 749–761 (2014).
VanderWeele, T. J. & Tchetgen Tchetgen, E. J. Mediation analysis with time varying exposures and mediators. J. R. Stat. Soc. Ser. B Stat. Methodol. 79, 917–938 (2017).
Stekhoven, D. J. & Bühlmann, P. MissForest-non-parametric missing value imputation for mixed-type data. Bioinformatics 28, 112–118 (2012).
Narita, Z. et al. Association of problematic internet use with psychotic experiences and depression in adolescents: a cohort study. Schizophr. Bull. https://doi.org/10.1093/schbul/sbae089 (2024).
Egami, H., Rahman, M. S., Yamamoto, T., Egami, C. & Wakabayashi, T. Causal effect of video gaming on mental well-being in Japan 2020-2022. Nat. Hum. Behav. 8, 1943–1956 (2024).
Mechler, K., Banaschewski, T., Hohmann, S. & Häge, A. Evidence-based pharmacological treatment options for ADHD in children and adolescents. Pharmacol. Ther. 230, 107940 (2022).
Shaw, M. et al. A systematic review and analysis of long-term outcomes in attention deficit hyperactivity disorder: effects of treatment and non-treatment. BMC Med. 10, 99 (2012).
Stevens, M. W. R., King, D. L., Dorstyn, D. & Delfabbro, P. H. Cognitive-behavioral therapy for Internet gaming disorder: a systematic review and meta-analysis. Clin. Psychol. Psychother. 26, 191–203 (2019).
Matheson, S. L., Laurie, M. & Laurens, K. R. Substance use and psychotic-like experiences in young people: a systematic review and meta-analysis. Psychol. Med. 53, 305–319 (2023).
Stickley, A. et al. Psychotic experiences and accidents, injuries, and poisonings among adults in the United States. Psychiatry Res. 282, 112610 (2019).
Stickley, A. et al. Physical injury and psychotic experiences in 48 low- and middle-income countries. Psychol. Med. 50, 2751–2758 (2020).
Stickley, A. et al. Childhood physical neglect and psychotic experiences: findings from the National Comorbidity Survey Replication. Early Interv. Psychiatry 15, 256–262 (2021).
Stickley, A. et al. Childhood neglect and suicidal behavior: findings from the National Comorbidity Survey Replication. Child Abuse Negl. 103, 104400 (2020).
Narita, Z. C. & Furukawa, T. A. Misuse of prediction models in psychiatric research. Lancet Psychiatry https://doi.org/10.1016/S2215-0366(24)00352-3 (2024).
Narita, Z. C. Dataset for figures in COMMSPSYCHOL-25-0086A. Zenodo, https://doi.org/10.5281/ZENODO.15760926 (2025).
Narita, Z. C. ZuiCNarita/DR-and-CMA250122: initial release for Zenodo. Zenodo, https://doi.org/10.5281/ZENODO.15760841 (2025).
Acknowledgements
This project was funded by Japan Society for the Promotion of Science (JP20H01777, JP20H03951, JP21H05171, JP21H05173, JP21H05174, JP21K10487, JP22H05211, JP23H03174, JP23H05472, JP24H00666, JP24H00917, JP25K20564, and JP24K16821), UTokyo Institute for Diversity and Adaptation of Human Mind (UTIDAHM), the International Research Center for Neurointelligence (WPI-IRCN) at the University of Tokyo Institutes for Advanced Study (UTIAS), the Japan Science and Technology Agency (JPMJPF2105), and the Ministry of Health Labour and Welfare (23AB1002). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
Zui C. Narita analyzed the data and wrote the initial draft of the manuscript. Syudo Yamasaki, Mitsuhiro Miyashita, and Satoshi Yamaguchi contributed to data curation. Shuntaro Ando, Jordan DeVylder, Toshiaki A. Furukawa, Kiyoto Kasai, and Atsushi Nishida provided supervision and conceptual input. Gemma Knowles and Daniel Stanyon contributed to the interpretation of findings. All authors reviewed, revised, and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
T.A.F. reports personal fees from Boehringer-Ingelheim, Daiichi Sankyo, DT Axis, Micron, Shionogi, SONY, and UpToDate, and a grant from DT Axis and Shionogi, outside the submitted work. In addition, T.A.F. has a patent 7448125 and a pending patent 2022-082495, and has licensed intellectual properties for Kokoro-app to Mitsubishi-Tanabe. K.K. reports grants from Teijin, Takeda, Lily, Otsuka, Daiichi Sankyo, Shionogi, Tanabe-Mitsubishi, and Sumitomo; and personal fees from Sumitomo, Meiji-Seika, Ricoh, Fuji-film Wako, Takeda, Otsuka, and Astellas outside the submitted work. The other authors declared no conflicts of interest.
Ethical approval
All procedures were approved by the Institutional Review Boards of the Tokyo Metropolitan Institute of Medical Science (12-35), the University of Tokyo (10057), and the SOKENDAI (2012002). All parents provided written informed consent.
Peer review
Peer review information
Communications Psychology thanks Patrik Koncz, Antonio Mendoza Diaz, and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Primary Handling Editors: Troby Ka-Yan Lui. [A peer review file is available].
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Narita, Z.C., DeVylder, J., Knowles, G. et al. Problematic online gaming mediates the association between attention-deficit/hyperactivity and subsequent mental health issues in adolescents. Commun Psychol 3, 117 (2025). https://doi.org/10.1038/s44271-025-00296-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s44271-025-00296-5
