
Abstract
Purpose
To determine the association between hospital and surgeon volume with the incidence of postoperative endophthalmitis.
Methods
A prospective cohort study was conducted to analyse the national health insurance claims data of those patients receiving cataract surgery in 2000 in Taiwan. A total of 108 705 patients who received cataract surgery by 1004 surgeons at 494 hospitals were followed to the end of 2002. Stepwise Cox regression was used to analyse the effects of hospital and surgeon volume of cataract surgery on postoperative endophthalmitis after adjustment for patient's age, gender, education, ophthalmic comorbidities, general comorbidities, and surgical factors including operative methods, different types of intraocular lenses, and surgeon's age.
Results
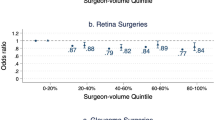
The 2-year incidence of postoperative endophthalmitis at high-volume hospitals (0.90%) was lower than low-volume hospitals (1.16%). The incidence of postoperative endophthalmitis by high-volume surgeons (0.59%) was lower than those by middle-high-volume (0.73%), middle-low-volume (0.80%), or low-volume surgeons (1.16%). After controlling for case mix, the risk of postoperative endophthalmitis of the low-volume hospitals (hazard ratio (HR)=1.39) was higher than that of the high-volume hospitals. The risk of postoperative endophthalmitis of low-volume surgeons (HR=1.67) was higher than that of the high-volume surgeons.
Conclusions
The provider volume (hospital and surgeon volume) is associated with the risk of postoperative endophthalmitis. The patients who receive cataract surgery at low-volume hospitals or by low-volume surgeons have significantly higher risk of postoperative endophthalmitis than at high-volume hospitals or by high-volume surgeons. Provider volume can be considered in further postoperative endophthalmitis study as a risk factor.
Similar content being viewed by others

Log in or create a free account to read this content
Gain free access to this article, as well as selected content from this journal and more on nature.com
or
References
American Academy of Ophthalmology. Basic and Clinical Science Course 2004/2005. Section 11: Lens and Cataract. American Academy of Ophthalmology: San Francisco, 2004/2005.
Javitt JC, Street DA, Tielsch JM, Wang Q, Kolb MM, Schien O et al. National outcomes of cataract extraction. Retinal detachment and endophthalmitis after outpatient cataract surgery. Cataract Patient Outcomes Research Team. Ophthalmology 1994; 101: 100–105.
Syam PP, Eleftheriadis H, Casswell AG, Brittain GP, McLeod BK, Liu CSC . Clinical outcome following cataract surgery in very elderly patients. Eye 2004; 18: 59–62.
Hannan EL, Racz M, Kavey RE, Quaegebeur JM, Williams R . Pediatric cardiac surgery: the effect of hospital and surgeon volume on in-hospital mortality. Pediatrics 1998; 01: 963–969.
Dardik A, Lin JW, Gordon TA, Williams GM, Perler BA . Results of elective abdominal aortic aneurysm repair in the 1990s: a population-based analysis of 2335 cases. J Vasc Surg 1999; 30: 985–995.
Hannan EL, Wu C, Ryan TJ, Bennett E, Culliford AT, Gold JP et al. Do hospital and surgeons with higher coronary artery bypass graft surgery volumes still have lower risk-adjusted mortality rate? Circulation 2003; 108: 795–801.
Smith ER, Butler WE, Barker FG . In-hospital mortality rates after ventriculoperitoneal shunt procedures in the United States, 1998–2000: relation to hospital and surgeon volume of care. J Neurosurg Spine 2004; 100: 90–97.
Losina E, Barrett J, Mahomed NN, Baron JA, Katz JN . Early failures of total hip replacement: effect of surgeon volume. Arthritis Rheum 2004; 50: 1338–1343.
Schrag D, Panageas KS, Riedel E, Hsieh L, Bach PB, Guillem JG et al. Surgeon volume compared to hospital volume as a predictor of outcome following primary colon cancer resection. J Surg Oncol 2003; 83: 68–78.
Morlet N, Li J, Semmens J, Ng J, team EPSWA . The Endophthalmitis Population Study of Western Australia (EPSWA): first report. Br J Ophthalmol 2003; 87: 574–576.
Javitt JC, Vitale S, Canner JK, Street DA, Krakauer H, McBean AM et al. National outcomes of cataract extraction: endophthalmitis following inpatient surgery. Arch Ophthalmol 1991; 109: 1085–1089.
Allardice GM, Wright EM, Peterson M, Miller JM . A statistical approach to an outbreak of endophthalmitis following cataract surgery at a hospital in the West of Scotland. J Hosp Infect 2001; 49: 23–29.
Norregaard JC, Thoning H, Bernth-Petersen P, Andersen TF, Javitt JC, Anderson GF . Risk of endophthalmitis after cataract extraction: results from the International Cataract Surgery Outcomes study. Br J Ophthalmol 1997; 81: 102–106.
Kanski JJ . Clinical Ophthalmology: A Systemic Approach, 4th edn. Butterworth-Heinemann Ltd: Stoneham, MA, 1999.
Cooper BA, Holekamp NM, Bohigian G, Thompson PA . Case control study of endophthalmitis after cataract surgery comparing scleral tunnel and clear corneal wounds. Am J Ophthalmol 2003; 136 (2): 300–305.
Menikoff JA, Speaker MG, Marmor M, Raskin EM . A case–control study of risk factors for postoperative endophthalmitis. Ophthalmology 1991; 98: 1761–1768.
Scott IU, Flynn Jr HW, Feuer W . Endophthalmitis after secondary intraocular lens implantation. A case-report study. Ophthalmology 1995; 102: 1925–1931.
Habib M, Mandal K, Bunce CV, Fraser SG . The relation of volume with outcome in phacoemulsification surgery. Br J Ophthalmol 2004; 88: 643–646.
Schein OD, Steinberg EP, Javitt JC, Cassard SD, Tielsch JM, Steinwachs DM et al. Variation in cataract surgery practice and clinical outcomes. Ophthalmology 1994; 101: 1142–1152.
Hannan EL, Kilburn H, Lindsey ML, Lewis R . Clinical versus administrative data bases for CABG surgery—does it matter? Med Care 1992; 30: 892–907.
Wei HM . Quality of claim management in healthcare organizations: a study on the consistency of ICD coding in a medical center. Institute of Hospital and Health Care Administration, National Yang-Ming University, Master's thesis, 2004.
Hannan EL, Kilburn Jr H, Bernard H, O'Donnell JF, Lukacik G, Shields EP . Coronary artery bypass surgery: the relationship between inhospital mortality rate and surgical volume after controlling for clinical risk factors. Med Care 1991; 29: 1094–1104.
Acknowledgements
The authors have no proprietary interest in any aspect of this study. This study was supported by a grant from the Bureau of National Health Insurance (DOH92-NH-1011).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Fang, YT., Chien, LN., Ng, YY. et al. Association of hospital and surgeon operation volume with the incidence of postoperative endophthalmitis: Taiwan experience. Eye 20, 900–907 (2006). https://doi.org/10.1038/sj.eye.6702045
Received:
Revised:
Accepted:
Published:
Issue date:
DOI: https://doi.org/10.1038/sj.eye.6702045
Keywords
This article is cited by
-
The effects of cement fixation on survival in elderly patients with hip hemiarthroplasty: a nationwide cohort study
BMC Musculoskeletal Disorders (2019)
-
Hospital and surgeon operation volume associated with endophthalmitis
Eye (2007)
-
Hospital cataract surgery volume and postoperative endophthalmitis
Eye (2007)
